Introduction
Septic arthritis of the hip joint may occur in
adults with a debilitating disease or sepsis at other bodily sites,
but the most common cause of a hip joint infection in the adult
population is the incidence of a previous surgical procedure (such
as an internal fixation of a fracture or the debridement of a
lesion, excluding a hip arthroplasty) (1). This kind of disease is often persistent
and recalcitrant. Due to the existence of articular cartilage
damage and chronic osteomyelitis, the infection may transform into
chronic septic arthritis (2,3) and has a high debridement failure rate
(4), which is difficult to cure and
is a challenge for orthopedists.
A Girdlestone surgery involves the complete removal
of a lesion via a head and neck incision, as well as a thorough
debridement, which is more effective in treating chronic septic
arthritis of the hip compared with the general debridement surgery
(5). Subsequently, a complete hip
arthroplasty can be performed following the infection is
effectively controlled. However, patients usually appear with
shortened extremities, arthralgia, and other symptoms after the
two-stage surgery due to a soft tissue contracture, which seriously
affects their quality of life (6,7).
Usually, a surgical program including the removal of
a prosthesis, a complete debridement, an implantation of an
antibiotic cement spacer, and a subsequent total hip arthroplasty
(THA) is effective for treating a periprosthetic joint infection
(PJI) (7–10). Previous studies have adopted a
similar staging surgical program (the incision of the head and neck
combined with the implantation of a cement spacer) for treating
refractory or chronic septic arthritides of the hip, which can
maintain the length and function of the lower limbs and can prevent
a muscle contracture prior to the stage II THA, thereby achieving
excellent results (1,11–14).
Nevertheless, all of the previous studies focused only on the
outcomes of using a bone cement spacer in patients receiving a
staging hip arthroplasty but did not compare the outcomes in
patients receiving a THA after the Girdlestone procedure alone.
Thus, these studies did not obtain direct evidence that proved the
advantages of the spacer method over the Girdlestone surgery.
The present study aims to explore the midterm
(followed-up for at least 1 year) efficacy of a two-stage THA in
treating chronic septic arthritis of the hip, as well as to compare
the outcomes between patients who received and did not receive a
cement spacer after the incision of the femoral head and neck.
Materials and methods
Patient selection
Adult patients with chronic hip infections, who had
each received a staging complete hip arthroplasty between January
2010 and January 2016 in the First Affiliated Hospital of Fujian
Medical University, were retrospectively analyzed. These patients
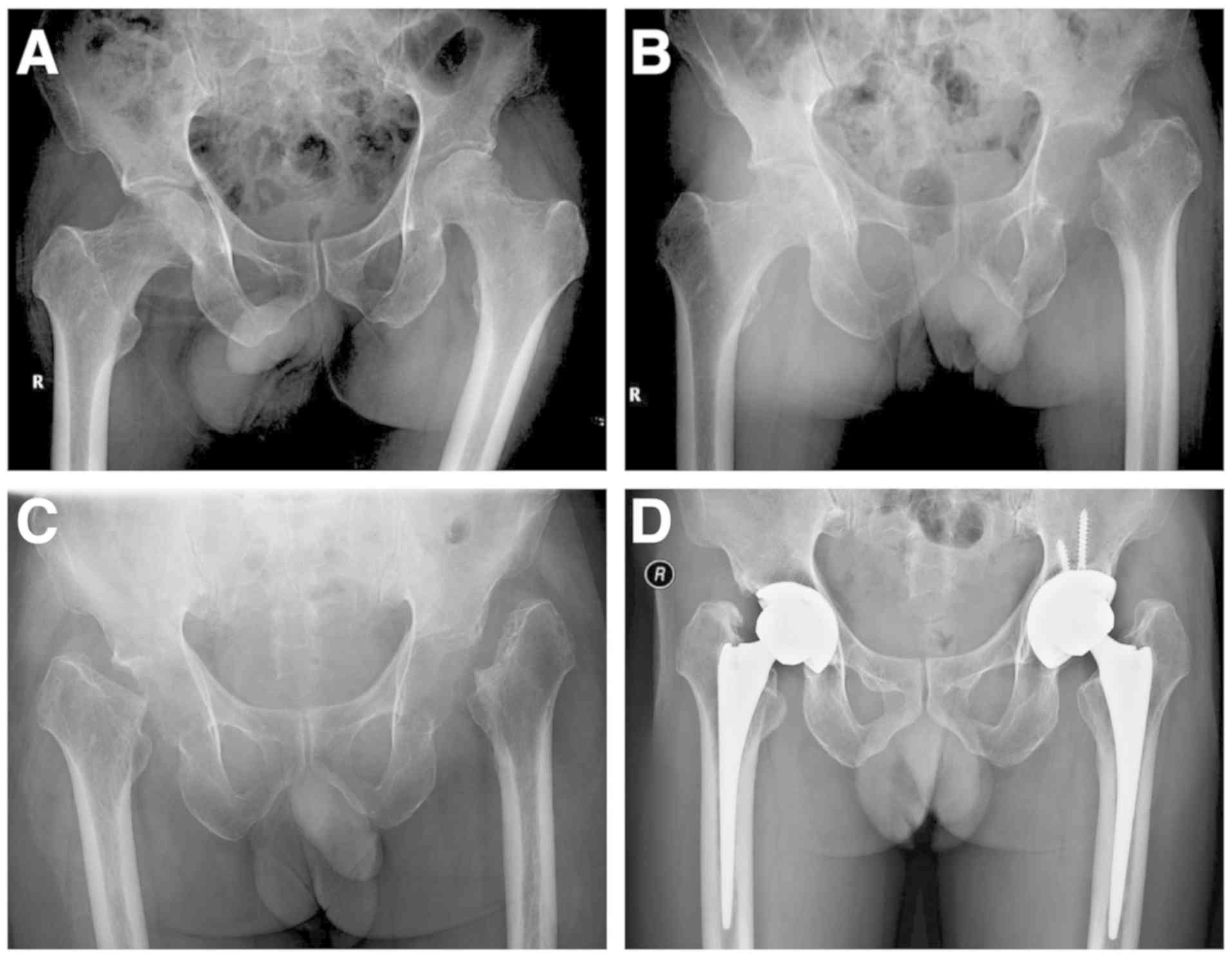
were initially diagnosed according to their disease history,
clinical manifestations (local erythema, tenderness, exudation and
pain) and imaging performances like disappearance of joint space
and femoral head damage (Fig. 1A).
All patients underwent a preoperative joint cavity puncture, as
well as an intraoperative joint fluid and tissue culture. The
inclusion criteria were as follows: i) A chronic sinus connected to
the joint cavity; ii) the presence of pus in the joint puncture or
pus and destruction of femoral head during the surgery; iii)
increased (>20 mg/l) serum C-reactive protein (CRP)
concentrations (detected using a Modular automated protein
analyzer; IMMAGE800; Beckman Coulter, Inc., Brea, CA, USA) and
positive frozen sections during the stage I surgery (numbers of
white blood cells per high-power field >5); and iv) cultures of
the joint punctures or intraoperative specimens yielding positive
results. A positive result was considered when at least one culture
yielded a strict pathogen (Staphylococcus aureus, Pseudomonas
aeruginosa, Enterobacteriaceae and anaerobes) or when
two cultures yielded a strain that was a skin commensal (including
coagulase-negative staphylococci or Propionibacterium acnes)
(15–17). The exclusion criteria were as
follows: i) Patients with infections after a THA and ii) patients
with incomplete clinical and laboratory information. Additionally,
the following data of the patients were preoperatively collected:
Cause of disease, causative organisms, comorbidities, CRP and
erythrocyte sedimentation rate (ESR; detected using an Automatic
ESR analyzer; Monitor-100; Vital, Puteaux, France).
Surgical procedures
All surgeries were performed using the same
approaches and procedures as described below and by the same
experienced surgeon. The stage I surgery was performed as follows:
An incision was made at the posterolateral region of the hip joint.
The purulent fluid was sucked out and sent for bacterial culture
and drug sensitivity examinations. Subsequently, the articular
capsule was cut open to fully expose the hip joint (the internal
fixture was taken out, if present) and was followed by the removal
of the destroyed head and neck of the femur. Subsequently, the
proximal femur was unreamed to prevent inflammation from the
reaming to the medullary cavity. The purulent pus, inflammatory
tissue, detached articular surface, and scar tissue were removed.
For the Girdlestone alone group, the incision was closed after the
drainage tube was placed (Fig. 1B and
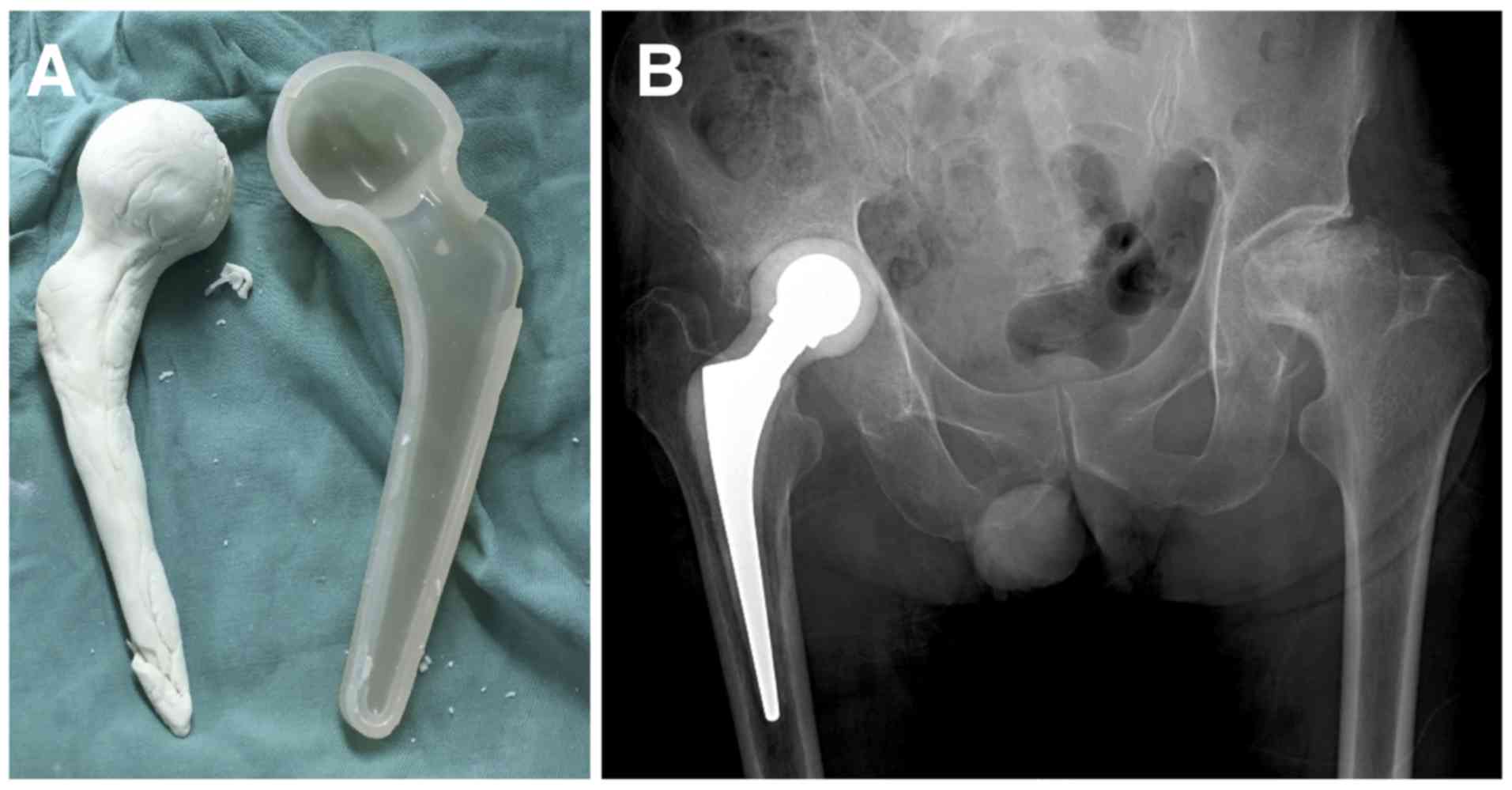
C). For the cement spacer group, after debridement, 8 g
vancomycin (Lilly, Indianapolis, IN, USA) was mixed with 80 g of
bone cement (Refobacin; Zimmer Biomet, Warsaw, IN, USA), which was
used to wrap two 4 mm Kirschner wire (Fig. 2B) or cement prostheses (Fig. 3) composed of a 28 mm femoral head, a
32 mm femoral neck and a 105 mm femoral stem (CM-CZ; AKMedical,
Beijing, China) to make a spacer that matched the acetabular and
femoral medullary cavities. The spacer was then implanted into the
hip joint, which could help to maintain the normal eccentricity and
tension of the gluteus medius. Finally, the incision was sutured
after the drainage tube was fixed. After the surgery, the drainage
tube was retained until a clear drainage fluid was observed and the
drainage fluid volume was >20 ml in both groups. The selection
of antibiotics was based on the preoperative or intraoperative
cultures and the drug sensitivity results, while vancomycin was
applied in patients without culture results. The courses of
intravenous and oral administration of antibiotics depended on the
clinical symptoms as well as the CRP decline. After the patients
received intravenous antibiotics (Table
II) for 2–4 weeks, they were switched to oral antibiotics,
which included 0.6 g levofloxacin (Daiichi Sankyo Co., Ltd., Tokyo,
Japan) once per day and 0.3 g rifampicin (Chengdu Tiantaishan
Pharmaceutical Co., Ltd., Chengdu, China) twice per day for 1–2
months. The affected limbs were allowed to gradually perform
flexion and extension activities, as well as partial loading.
 | Table II.Pathogen and stage I surgery. |
Table II.
Pathogen and stage I surgery.
| Case | Type of stage 1
surgery | Pathogen | Antibiotics
administration after stage 1 (IV) | Length of
antibiotic therapy after stage 1 (weeks) | Interval to normal
CRP (weeks) | Interval to THA
(months) |
|---|
| 1 | Girdlestone | Burkholderia
pseudomallei | Meropenem
Ceftazidime | L-24 | L-12 | L-12 |
|
|
|
|
| R-10 | R-7 | R-9.5 |
| 2 | Girdlestone | Stenotrophomonas
maltophilia | Meropenem | 12 | 12 | 33 |
| 3 | Girdlestone | Escherichia
coli | Levofloxacin | 8 | 6 | 69 |
| 4 | Girdlestone | MRSA | Vancomycin | 6 | 5 | 24 |
| 5 | Spacer | Enterobacter
cloacae | Meropenem | 6 | 4 | 3 |
| 6 | Spacer |
Corynebacterium | Vancomycin
meropenem Cefoperazone | 8 | 6 | 5.5 |
| 7 | Spacer | Negative | Vancomycin
moxifloxacin | 8 | 4 | 4.5 |
| 8 | Spacer | Streptococcus | Vancomycin
levofloxacin | 8 | 4 | 3 |
| 9 | Spacer | MSSA | Vancomycin
cefuroxime | 6 | 4 | 4 |
| 10 | Spacer | Negative | Vancomycin
levofloxacin | 12 | 12 | 3 |
| 11 | Spacer | MRSA |
Vancomycinlinezolid | 12 | 10 | 3 |
| 12 | Spacer | MSSA | Vancomycin | 6 | 3 | 4 |
| 13 | Spacer | MSSA | Vancomycin | 6 | 5 | 6 |
Indications for stage II surgery
When movement of the hip did not incur obvious pain
and the soft tissue did not appear to be swollen, patients
underwent a CRP and ESR review a total of three times, with each
review occurring once every week and yielding normal results. The
stage II surgery was conducted using the original approach. The
antibiotic bone cement spacer was removed, followed by an
intra-articular scar clearance and debridement. The patients in
both groups underwent THA using bioprosthesis (Johnson &
Johnson Services, Inc., New Brunswick, NJ, USA).
Evaluation indicators
Patients were assessed in terms of Harris hip scores
(18) before the stage I surgery,
between the two surgeries, and within the follow-up period
(12.0–62.0 months; mean duration, 24.2±3.8 months) after the last
surgery. The complications after the stage I surgery, the time of
antibiotic applications after the stage I surgery, the interval
between the stage I and stage II surgeries, the operation times,
and the operative hemorrhage of the stage II surgery were recorded
and the lengths of the lower extremities were postoperatively
compared. In addition, the patients were reviewed using the
inflammatory indicators (ESR and CRP) once every 3 months within
the follow-up period, in order to monitor the recurrences of
disease.
Statistical analyses
All of the data are presented as the mean ± standard
error of the mean. A Mann-Whitney U test was performed to evaluate
the differences between the Girdlestone alone group and the
Girdlestone + cement spacer group for all of the indicators
analyzed. The statistical significance threshold was set at
P=0.05.
Results
Analysis of included cases
According to the inclusion criteria, 16 patients
were eligible for the present study. Among these patients, three
patients with incomplete clinical data were excluded. Therefore, a
total of 13 patients (14 hip joints, with one case of a bilateral
infection) were enrolled in the study, including 8 men and 5 women,
mean age 59.3±4.3 years; range 19–79 years. The present study
included 7 cases (8 hip joints) of primary hip infections, 5 cases
of infections after the internal fixation of the hip fracture (4
cases were femoral neck fractures and one case was an acetabular
fracture), and one case of a chronic infection after the focal
cleaning of osteonecrosis of the femoral head. All of the patients
complained of symptoms for >2 months (Table I). Ten patients had pain and swelling
at the affected site, and two patients had pain symptoms and a
sinus connected with the articular cavity. The symptoms of these
patients lasted for 60–125 days (mean: 82.7±7.5 days) before the
first surgery. Nine patients had a history of antibiotic use before
the first surgery, while certain patients underwent incision
drainages (cases 1, 3, 5, and 7) with no improvement in clinical
manifestations (Table I). Beside the
cases that were negative for the presence of bacterial cultures,
half of the bacterial cultures of the two groups were comprised of
gram-negative bacteria, which were different from the commonly
found staphylococci and other positive cocci in PJI cases. On the
basis of the bacterial culture results, the patients in both groups
were given antibiotics, out of which two cases of negative cultures
were given a combination of vancomycin and quinolones
(levofloxacin; cases 7 and 10; Table
II).
| Table I.Patient data (preoperative). |
Table I.
Patient data (preoperative).
| Case | Age (years)/Sex | Cause of
presentation | Duration of symptom
(days) | Joint | Etiology | Comorbidities | Previous treatment
for infection |
|---|
| 1 | 59/M | Pain, sinus | L-60; R-35 | Bilateral | Primary | Syphilis,
osteoporosis | I&D,
Cefradine |
| 2 | 54/M | Pain | 106 | Left | Primary | Gout | Aspiration |
| 3 | 61/M | Pain, sinus | 120 | Right | Femoral neck
fracture ORIF | Eczema | I&D,
Cefdinir |
| 4 | 67/M | Pain | 125 | Right | Primary | NIDDM | None |
| 5 | 62/M | Pain | 71 | Left | Acetabula fracture
ORIF | Arterial
hypertension, NIDDM | I&D,
Moxifloxacin |
| 6 | 52/M | Sinus | 63 | Right | AVN focal
cleaning | Cirrhosis | Cefradine |
| 7 | 55/M | Pain, sinus | 61 | Right | Femoral neck
fracture ORIF | None | I&D,
Cefradine |
| 8 | 77/F | Pain | 64 | Right | Femoral neck
fracture ORIF | Arterial
hypertension, NIDDM, PD | Cefdinir |
| 9 | 49/F | Pain | 123 | Left | Primary | None | Cefradine |
| 10 | 75/F | Pain | 100 | Right | Primary | None | Cefradine |
| 11 | 79/F | Pain | 60 | Left | Primary | None | None |
| 12 | 62/M | Pain | 90 | Right | Primary | NIDDM | None |
| 13 | 19/F | Pain | 80 | Right | Femoral neck
fracture ORIF | None | Cefradine |
Pathogen and stage I surgery
For the stage I surgery, 4 patients (5 hips)
underwent the resection of the head and neck (cases 1–4, hereafter
referred to as the Girdlestone alone group), and 9 patients (9
hips) underwent the resection of the head and neck combined with
the implantation of a bone cement spacer (cases 5–13, hereafter
referred to as the spacer group). In the Girdlestone alone group,
the highly pathogenic Burkholderia cepacia was cultured in
one case (case 1, Fig. 1), which did
not show significant complications after the stage I surgery but
required a longer time duration for controlling the infection. One
case had an incision sinus and infection recurrence after the
surgery (case 3, Escherichia coli) and required a
re-debridement and an extended anti-infective treatment. Another
case had pneumonia, poor wound healing and other complications, and
underwent a re-debridement (case 2, Stenotrophomonas
maltophilia). The infection and complications in these three
cases were under control and CRP levels were restored to a normal
level after the stage I surgery in a mean of 8.4±1.5 weeks (range,
5–12 weeks). Among the patients undergoing a spacer implantation,
two cases had complications. One case had a pneumonia and type I
respiratory failure after the stage I surgery and was healed after
treatment and underwent the stage II surgery successfully (case 6
with Corynebacterium). Another case had a spacer fracture
after walking with weight loading at 3 months after the surgery and
underwent the stage II surgery soon after (case 7). The mean time
for CRP levels of the patients to decline to the normal level after
the stage I surgery was 5.8±1.0 weeks (range 4–12 weeks), which was
a shorter time period than that of the Girdlestone alone group.
However, this difference was statistically insignificant.
Additionally, two cases of the Girdlestone alone group who
underwent a debridement after the stage I surgery suffered from
poor wound healing again after the stage II surgery (cases 2 and 3)
and were healed after receiving a debridement. However, all the
patients in the spacer group were well healed. Signs of infection
recurrence were not found in both groups until the end of the
follow-up periods (Table II).
Comparison of stage II surgery and
postoperative implications in two groups
After the stage I surgery, the patients in the
Girdlestone alone and spacer groups were given antibiotics for
120±3.2 weeks and 8.0±0.8 weeks, respectively, but this difference
in antibiotic treatment times was statistically insignificant. The
mean time interval between the two surgeries was 4.0±0.4 months in
the spacer group, which was a significantly shorter time interval
than that in the Girdlestone alone group (29.5±10.7 months,
P<0.01, Table II). The stage II
arthroplasty was more difficult to perform in the Girdlestone alone
group. The mean operation time was longer (124.0±13.6 vs. 105.6±7.9
min) and the incidence of a hemorrhage was increased more in the
Girdlestone alone group (501.0±100.8 vs. 322.2±55.4 ml), but these
differences were statistically insignificant. The Girdlestone alone
group showed a more marked leg-length discrepancy after the stage
II THA than the spacer group (2.8±0.6 vs. 0.8±0.2 cm, P<0.01;
Table III).
| Table III.Patient data (stage II surgery and
postoperative implications). |
Table III.
Patient data (stage II surgery and
postoperative implications).
| Case | Operative
hemorrhage of THA (ml) | Duration of THA
operation (min) | Leg-length
discrepancy after THA (cm) | Preoperative hip
score | Interim hip
score | Final hip
score | Complication
between stages | Complication after
prosthesis implantation | Follow-up
(months) |
|---|
| 1 | L-200 | L-90 | L-2.0 | L-54 | L-74 | L-82 |
|
| 62 |
|
| R-400 | R-120 | R-2.2 | R-52 | R-72 | R-81 |
|
|
|
| 2 | 500 | 150 | 2.2 | 51 | 75 | 84 | Pneumonia,
hematosepsis, poor wound healing | Poor wound
healing | 27 |
| 3 | 600 | 100 | 5.0 | 49 | 66 | 83 | Recurrence of
infection, poor wound healing | Poor wound
healing | 24 |
| 4 | 805 | 160 | 3.0 |
| 65 | 78 |
|
| 12 |
| 5 | 250 | 90 | 1.1 | 47 | 85 | 90 |
|
| 24 |
| 6 | 600 | 105 | 2.0 | 48 | 79 | 89 | Pneumonia, type-I
respiratory failure |
| 28 |
| 7 | 200 | 70 | 1.0 | 53 | 85 | 93 |
|
| 36 |
| 8 | 300 | 80 | 0.8 | 30 | 90 | 91 | Spacer
fracture |
| 30 |
| 9 | 200 | 147 | 0.7 | 45 | 91 | 84 |
|
| 16 |
| 10 | 150 | 115 | 0 | 35 | 75 | 78 |
|
| 17 |
| 11 | 500 | 116 | 1 | 42 | 79 | 94 |
|
| 13 |
| 12 | 500 | 127 | 0 | 20 | 95 | 93 |
|
| 14 |
| 13 | 200 | 100 | 0.5 | 25 | 88 | 88 |
|
| 12 |
All patients were followed up for >12 months
after the stage II surgery (12.0–62.0 months), with a mean of
24.2±3.8 months (Girdlestone alone group: 31.3±10.8 months; spacer
group: 21.1±2.9 months). No cases had an infection recurrence or
emerging infection surrounding the prosthesis, and no cases had
prosthesis loosening, a dislocation, or a fracture around the
prosthesis during the follow-up periods. The mean Harris scores
before the surgery were comparable between the two groups (47.8±2.5
vs. 40.7±3.1; Table IV). The Harris
scores after the stage I replacement were 70.4±2.1 vs. 85.2±2.2 in
the Girdlestone alone group and spacer group, respectively, which
showed significant differences (P<0.01). At the last follow-up,
the Harris score in the spacer group was also improved than that in
the Girdlestone alone group (81.6±1.1 vs. 88.9±1.7, P<0.01;
Table IV).
| Table IV.Comparison of the two surgical
procedures. |
Table IV.
Comparison of the two surgical
procedures.
| Surgical type | Operative
hemorrhage of THA (ml) | Duration of THA
operation (min) | Leg-length
discrepancy after THA (cm) | Preoperative Harris
hip score | Interim Harris hip
score | Final Harris hip
score |
|---|
| Girdlestone
alone | 501.0±100.8 | 124.0±13.6 | 2.8±0.6 | 47.8±2.5 | 70.4±2.1 | 81.6±1.1 |
| Girdlestone +
spacer | 322.2±55.4 | 105.6±7.9 | 0.8±0.2 | 40.7±3.1 | 85.2±2.2 | 88.9±1.7 |
| P-value | 0.1658 | 0.2812 | 0.0015 | 0.1783 | 0.0020 | 0.0175 |
Discussion
The present study evaluated the midterm efficacy of
a staged complete hip arthroplasty in treating the refractory
septic arthritis of the hip. The comparison of the results from the
follow-up in patients undergoing different surgical procedures
showed that the application of an antibiotic cement spacer in
addition to a head and neck resection could better control the
infection. It could also maintain the limb length more effectively,
thus providing more favorable conditions for the stage II complete
hip arthroplasty, compared with the head and neck resection
alone.
Previous literature has reported the unsatisfactory
efficacy of a head and neck resection (19). It is generally believed that the
joint is unstable, shortened, and often painful after the surgery.
Additionally, it is not guaranteed that there is a complete and
thorough debridement (20,21). Rittmeister et al (19) reported 39 cases that underwent a head
and neck resection of the hip joint and observed 67% incidence of
complications and a repair rate of 44%. Charlton et al
(22) found that the lower limb was
shortened by an average of 30.5 mm after two resections of the head
and neck; of these, 39 and 11.4% of the patients had a claudication
and a dislocation after the stage II surgery, respectively.
The application of a spacer following a head and
neck resection has been reported, wherein the spacer can be
prefabricated or made by the surgeons during the surgery. Romanò
et al (13) applied a
prefabricated spacer made of gentamicin antibiotic loaded bone
cement in 19 patients (20 hips). The authors found that hip
arthroplasty was successfully implemented in all of the hips after
a mean of 22 weeks, and only 1 case had infection recurrence during
an average follow-up period of 56 months (13). Huang et al (23) used a variety of antibiotic bone
cements to treat 14 cases (15 hips) with refractory septic hips and
found an uncontrolled infection in only 1 case; no
spacer-associated complications were observed. Among the 14 cases
reported by Fleck et al (12), two died of other diseases, and two
did not undergo the stage II surgery, while no case showed any sign
of an infection recurrence. Shen et al (14) has questioned the traditional spacer
method, they believed that an infection following hip trauma
surgery was different from that of an infection following an
arthroplasty. Since the infection might only involve the
intra-articular soft tissue, cartilage, and subchondral bone, but
not the proximal femur, the spacer with a femoral stem may lead to
the involvement of the femoral medullary cavity and the spread of
the infection. Thus, a spacer that does not need to be placed into
the medullary cavity was used, and no infection recurrence and
spacer associated complications were found during an average
follow-up period of 39.6 months. Nonetheless, this kind of spacer
could not achieve an axial and rotational stability that was
similar to that of the traditional spacer; thus, this spacer had a
higher risk of mechanical loosening and dislocation. Therefore, the
conventional spacer was still adopted in the present study.
Two surgical methods were successfully used in the
present study. It was found that, although the resection of the
femoral head and neck could achieve a complete debridement, two
patients had postoperative infection recurrences and poor wound
healing, which greatly prolonged the time of antibiotic use and the
interval between the two surgeries. The patients also suffered from
shortened limbs and obvious dysfunctions, which may have led to
great difficulties in the stage II hip arthroplasty. This may be
because systemic medications did not help to achieve an effective
concentration locally in patients with a poor blood supply, which
led to a higher likelihood of an infection recurrence. Hsieh et
al (24) used antibiotic beads
locally after the Girdlestone surgery for treating a septic hip and
achieved an improvement in the control of infection. For the
implantation of an antibiotic bone cement spacer based on the stage
I head and neck resection, a local release of antibiotics helped in
controlling the infection and shortened the time of systemic
application of the antibiotics. At the same time, the spacer was
able to maintain the lengths and ranges of motion of the limbs
(25,26). It was not necessary to loosen the
scar tissue during the stage II surgery, which resulted in a lower
degree of operative hemorrhage and a shortened operation time.
Additionally, the postoperative limbs were shortened by no more
than 1 cm, the function was fully recovered, and no joint
dislocation was reported during the follow-up. The spacer, which
constructed using the bone cement prosthesis, is simple and
inexpensive, has improved mechanical stability (compared with the
Kirschner wire as the skeleton), and enables patients to walk with
weight loading in an earlier time period following surgery, thus
making it conducive for a functional recovery. This was therefore
used instead of Kirschner wire in the later phase.
The selection of the implant in the stage II surgery
is still controversial (27).
Theoretically, the loss of bone mass in the septic hip is less than
that in the infection following a THA, which is beneficial to the
fixation of the biological prosthesis. A cementless bioprosthesis
has been reported to have a good efficacy in treating an infection
following a THA (28,29). In addition, the use of a cement
prosthesis has been reported to be insignificantly associated with
an infection recurrence (27,30,31).
Therefore, it is believed that a cementless prosthesis is a good
choice for the stage II surgery for a septic hip. A bio-prosthesis
was implemented in the stage II arthroplasty in most patients in
this study. The results showed that the stability was immediately
achieved during the surgery, no signs of loosening of the
prosthesis were reported during the follow-up, and infections were
well controlled in the patients. Other concerns in this study are
the type and duration of antibiotic use. A systemic application of
antibiotics is needed to not only control the primary foci but also
prevent the hematogenous spread and infection metastasis. Despite
reports that a short term application of intravenous antibiotics
can also achieve the same effect as that of a long term application
after spacer therapy for a refractory septic hip (23,32),
retrospective studies exist that only have a small number of cases
and insufficient evidence. The bacterial cultures in this study
revealed mostly gram-negative bacteria. Because of insufficient
data showing the ideal doses and duration of antibiotic use, the
patients were given intravenous antibiotics for at least 4 weeks
after the stage I surgery, and the extended application was
determined according to the changes in the inflammatory
indicators.
The strengths of the present study were as follows:
(1) All the patients received
follow-ups; (2) all the surgical
procedures were performed by the same surgeon in a standard manner;
and (3) two surgical methods were
compared. Since the patients were selected at different
time-points, those patients receiving treatment after an
improvement in the prosthesis and surgical techniques may show
higher efficacy (a spacer was used in the late phase), which was
the limitations of the present study. Nevertheless, this was
unlikely to affect the credibility of the results as the use of the
spacer significantly reduced the duration of antibiotic use,
improved the function of the hip joints during the surgery, and
maintained the lengths of the lower limbs. This, thereby simplified
the stage II surgery, achieving improved final clinical efficacy.
These effects showed a significant difference between the two
groups. Evidently, this study included a small number of samples
and hence further statistical analysis could not be performed.
Furthermore, this was a retrospective study, in which patients were
not randomly grouped and received follow-ups for a relatively short
time. Therefore, further studies, with more patients and a
long-term follow-up period are needed to provide more convincing
comparative data. In conclusion, the present study found that a
staging arthroplasty was conducive for a complete debridement in
treating a chronic septic hip. The implantation of a bone cement
spacer containing antibiotics in the stage I surgery could
effectively control infection, avoid a joint contracture caused by
a head and neck resection, reduce the risk of an infection
recurrence between the two stages of the surgery. It could also
effectively maintain the lengths of the lower limbs, simplify the
stage II complete hip arthroplasty, and reduce an operative
hemorrhage. Thus, it was a more effective method for treating a
chronic septic hip arthritis.
Acknowledgements
Not applicable.
Funding
The current study was funded by Fujian Youth Talents
General Training Program (grant no. 2014-ZQN-JC-19) and the Key
Clinical Specialty Discipline Construction Program of Fujian, P.R.C
and the Key Clinical Discipline of Fujian Medical University (grant
no. XK201106).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WZ designed the current study. WL, XF, CZ and YX
accumulated the data. WL, ZH, ZY and XF analysed the data. WL and
XF drafted the manuscript. All authors read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee and
Institutional Review Board of The First Affiliated Hospital of
Fujian Medical University (committee's reference number: [2014]
047). Informed consent was obtained from each patient before the
data was collected.
Patient consent for publication
Consents regarding individual details, images,
findings of physical examination and data of the surgery details
were obtained from all patients.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AVN
|
Avascular necrosis
|
|
CRP
|
C-reactive protein
|
|
ESR
|
erythrocyte sedimentation rate
|
|
F
|
female
|
|
I&D
|
incision and debridement
|
|
M
|
male
|
|
NIDDM
|
noninsulin-dependent diabetes
mellitus
|
|
ORIF
|
open reduction internal fixation
|
|
PJI
|
Periprosthetic Joint Infection
|
|
THA
|
total hip arthroplasty
|
References
|
1
|
Diwanji SR, Kong IK, Park YH, Cho SG, Song
EK and Yoon TR: Two-stage reconstruction of infected hip joints. J
Arthroplasty. 23:656–661. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Souza Miyahara Hd, Helito CP, Oliva GB,
Aita PC, Croci AT and Vicente JR: Clinical and epidemiological
characteristics of septic arthritis of the hip, 2006 to 2012, a
seven-year review. Clinics (Sao Paulo). 69:464–468. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Vukasinović Z, Spasovski D, Cobeljić G and
Zivković Z: Septic arthritis of the hip in infancy-diagnostic and
therapeutic possibilities. Srp Arh Celok Lek. 134:77–81. 2006.(In
Serbian). PubMed/NCBI
|
|
4
|
Stutz G, Kuster MS, Kleinstück F and
Gächter A: Arthroscopic management of septic arthritis: Stages of
infection and results. Knee Surg Sport Traumatol Arthrosc.
8:270–274. 2000. View Article : Google Scholar
|
|
5
|
Harrison MH: Robert Jones, Gathorne
Girdlestone and excision arthroplasty of the hip. J Bone Joint Surg
Br. 87:13062005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Malcolm TL, Gad BV, Elsharkawy KA and
Higuera CA: Complication, survival, and reoperation rates following
girdlestone resection arthroplasty. J Arthroplasty. 30:1183–1186.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cui Q, Mihalko WM, Shields JS, Ries M and
Saleh KJ: Antibiotic-impregnated cement spacers for the treatment
of infection associated with total hip or knee arthroplasty. J Bone
Joint Surg Am. 89:871–882. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Assmann G, Kasch R, Maher CG, Hofer A,
Barz T, Merk H and Flessa S: Comparison of health care costs
between aseptic and two stage septic hip revision. J Arthroplasty.
29:1925–1931. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim YS, Bae KC, Cho CH, Lee KJ, Sohn ES
and Kim BS: Two-stage revision using a modified articulating spacer
in infected total knee arthroplasty. Knee Surg Relat Res.
25:180–185. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sandiford NA, Duncan CP, Garbuz DS and
Masri BA: Two stage management of the infected total hip
arthroplasty. Hip Int. 25:308–315. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Anagnostakos K, Duchow L and Koch K:
Two-stage protocol and spacer implantation in the treatment of
destructive septic arthritis of the hip joint. Arch Orthop Trauma
Surg. 136:899–906. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fleck EE, Spangehl MJ, Rapuri VR and
Beauchamp CP: An articulating antibiotic spacer controls infection
and improves pain and function in a degenerative septic hip. Clin
Orthop Relat Res. 469:3055–3064. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Romanò CL, Romanò D, Meani E, Logoluso N
and Drago L: Two-stage revision surgery with preformed spacers and
cementless implants for septic hip arthritis: A prospective,
non-randomized cohort study. BMC Infect Dis. 11:1292011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shen H, Wang QJ, Zhang XL and Jiang Y:
Novel articulating medullary-sparing spacer for the treatment of
infectious hip arthritis. Orthopedics. 36:e404–e408. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Osmon DR, Berbari EF, Berendt AR, Lew D,
Zimmerli W, Steckelberg JM, Rao N, Hanssen A and Wilson WR;
Infectious Diseases Society of America, : Diagnosis and management
of prosthetic joint infection: Clinical practice guidelines by the
infectious diseases Society of America. Clin Infect Dis. 56:e1–e25.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mirra JM, Amstutz HC, Matos M and Gold R:
The pathology of the joint tissues and its clinical relevance in
prosthesis failure. Clin Orthop Relat Res. 221–240. 1976.PubMed/NCBI
|
|
17
|
Spangehl MJ, Masri BA, O'Connell JX and
Duncan CP: Prospective analysis of preoperative and intraoperative
investigations for the diagnosis of infection at the sites of two
hundred and two revision total hip arthroplasties. J Bone Joint
Surg Am. 81:672–683. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mahomed NN, Arndt DC, McGrory BJ and
Harris WH: The Harris hip score: Comparison of patient self-report
with surgeon assessment. J Arthroplasty. 16:575–580. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rittmeister M, Müller M, Starker M and
Hailer NP: Functional results following Girdlestone arthroplasty. Z
Orthop Ihre Grenzgeb. 141:665–671. 2003.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fenelon GC, Von Foerster G and Engelbrecht
E: Disarticulation of the hip as a result of failed arthroplasty. A
series of 11 cases. J Bone Joint Surg Br. 62-B:441–446. 1980.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Petty W and Goldsmith S: Resection
arthroplasty following infected total hip arthroplasty. J Bone
Joint Surg Am. 62:889–896. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Charlton WP, Hozack WJ, Teloken MA, Rao R
and Bissett GA: Complications associated with reimplantation after
girdlestone arthroplasty. Clin Orthop Relat Res. 119–126. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Huang TW, Huang KC, Lee PC, Tai CL and
Hsieh PH: Encouraging outcomes of staged, uncemented arthroplasty
with short-term antibiotic therapy for treatment of recalcitrant
septic arthritis of the native hip. J Trauma. 68:965–969.
2010.PubMed/NCBI
|
|
24
|
Hsieh PH, Chang YH, Chen SH and Shih CH:
Staged arthroplasty as salvage procedure for deep hip infection
following intertrochanteric fracture. Int Orthop. 30:228–232. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Romanò CL, Romanò D, Logoluso N and Meani
E: Long-stem versus short-stem preformed antibiotic-loaded cement
spacers for two-stage revision of infected total hip arthroplasty.
Hip Int. 20:26–33. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Regis D, Sandri A, Rizzo A and Bartolozzi
P: A preformed temporary antibiotic-loaded cement spacer for the
treatment of destructive septic hip arthritis: A case report. Int J
Infect Dis. 14:e259–e261. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ganzoury IE and Eid AS: Two-stage
arthroplasty using functional temporary prosthesis to treat
infected arthroplasty and septic arthritis of the hip. J Orthop. 12
(Suppl 1):S86–S93. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fink B, Grossmann A, Fuerst M, Schäfer P
and Frommelt L: Two-stage cementless revision of infected hip
endoprostheses. Clin Orthop Relat Res. 467:1848–1858. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Masri BA, Panagiotopoulos KP, Greidanus
NV, Garbuz DS and Duncan CP: Cementless two-stage exchange
arthroplasty for infection after total hip arthroplasty. J
Arthroplasty. 22:72–78. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Fehring TK, Odum S, Calton TF and Mason
JB: Articulating versus static spacers in revision total knee
arthroplasty for sepsis. The ranawat award. Clin Orthop Relat Res.
9–16. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sanchez-Sotelo J, Berry DJ, Hanssen AD and
Cabanela ME: Midterm to long-term followup of staged reimplantation
for infected hip arthroplasty. Clin Orthop Relat Res. 467:219–224.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Rutz E and Spoerri M: Septic arthritis of
the paediatric hip-A review of current diagnostic approaches and
therapeutic concepts. Acta Orthop Belg. 79:123–134. 2013.PubMed/NCBI
|