Introduction
Tubo-ovarian abscess (TOA) is a well-known
life-threatening complication of pelvic inflammatory disease (PID),
and occurs in 10–15% of females affected by PID (1). Every year, ~70,000 females, accounting
for 1/3 of females hospitalized with PID, are treated for TOA in
the USA (2). In TOA, abscess and
tissue necrosis form in the fallopian tubes and/or ovaries, which
significantly reduces the pregnancy rate (2), which has become an important clinical
issue. It is generally thought that TOA is mainly caused by
infection of the lower genital tract, as well as direct spread of
infection from the diverticulum, appendix and intestinal tract
(3). The common pathogenic bacteria
of TOA include Bacteroides, E. coli and Peptococcus
(4).
With the development of antibiotics, TOA and pelvic
abscesses are now treated by broad-spectrum antibiotics as the
first-line treatment, and the success rate of treatment is 34–88%
(1,5), while the failure rate of antibiotic
therapy is higher in patients with larger abscesses (6). Surgical treatment is also necessary if
patients exhibit no clinical response after antibiotic therapy for
at least 72 h or ruptured abscess. Compared with patients who
underwent antibiotic therapy in combination with image-guided
drainage, part of the patients who received antibiotic therapy
alone required image-guided drainage or surgical treatment
eventually (5,7,8). There
are still no standardized guidelines as to when either antibiotic
therapy, drainage or surgery is the most suitable primary option
for patients with TOA or pelvic abscess. The risk factors for
antibiotic therapy failure and ideal subsequent clinical treatment
strategies are worthy of further investigation. Risk factors for
adverse clinical prognosis are various among previous studies;
however, they generally comprise parameters including abscess
diameter, initial inflammatory biomarkers, age and smoking status
(9,10).
In recent years, aggressive surgical treatment has
been considered to be required in a proportion of patients with
TOA. In particular, the development of minimally invasive
techniques has greatly advanced the surgical treatment of TOA
(11). However, whether patients
benefit from early laparoscopic surgery remains controversial
(12). The present study aimed to
retrospectively analyze patients diagnosed with TOA or pelvic
abscess to further explore whether early laparoscopic treatment
provides a benefit.
Materials and methods
Study design and patients
The present study was a retrospective study of
patients who were initially diagnosed with TOA or pelvic abscess at
the Department of Gynecology, Xuzhou City Hospital of Traditional
Chinese Medicine (Xuzhou, China) between April 2014 and June 2015.
The inclusion criteria were as follows: i) Symptoms of infection,
including fever and pelvic pain; ii) ultrasound or magnetic
resonance imaging (MRI) examination revealed a pelvic mass ≥3 cm;
iii) cervical motion tenderness, uterine tenderness or adnexal
tenderness, abdominal tenderness, and peritoneal signs, including
rebound tenderness and guarding on physical examination. The
clinical and imaging diagnostic standards were according to the
sexually transmitted diseases treatment guidelines (13). Patients with combined malignant
diseases were excluded from the present study.
Grouping
After definite diagnosis, all patients were informed
of the treatment management options, including conservative
antibiotic therapy, early laparoscopic treatment and late
laparoscopic treatment), and they freely selected one of the
therapeutic methods after consulting with the doctors. According to
the guidelines (13), conservative
treatment failure was defined as patients receiving conservative
treatment with little or no clinical response (oral temperature
≥38°C, no decrease in abscess diameter and pelvic pain) after 72 h
of antibiotic treatment. Patients who failed to respond to the
antibiotic regimen were given laparoscopic treatment and those who
completed initial antibiotic treatment but with recurrence during
follow-up also received laparoscopic treatment.
Treatment strategies
During laparoscopy, patients received general
anesthesia and were placed in a lithotomy position. All surgical
procedures were performed by two surgeons, who had >10 years of
relevant surgical experience. Patients in the early laparoscopic
treatment group received immediate surgical treatment. Patients in
the conservative treatment group received levofloxacin 500 mg
intravenously (i.v.) once daily or cefuroxime 1,500 mg i.v. twice
daily plus metronidazole 500 mg i.v. three times daily for 72 h, as
recommended by the Chinese Medical Association (14). The effects of the conservative
treatment were evaluated based on symptoms, serum white blood cell
(WBC) count, and abscess size (which was determined on ultrasound
or MRI). Patients who responded to the antibiotic treatment
continued this treatment to a total of 10–14 days. Conservative
treatment failure was defined as patients who received conservative
treatment with little or no clinical response (oral temperature
≥38°C, no decrease in abscess diameter, and pelvic pain) after 72 h
of antibiotic treatment (13).
Patients who failed to respond to the antibiotic regimen were
subjected to laparoscopic treatment and those who completed the
initial antibiotic treatment but with recurrence during follow-up
also received laparoscopic treatment.
Follow-up
All patients were invited for follow-up visits by
gynecological examination and ultrasound examination at the 3rd,
6th, 12th and 24th month after treatment at the outpatient clinic.
Thereafter, patients were followed up by telephone every 6–12
months for two years. All follow-ups were performed by the same
gynecologist. All patients were required to provide their own
telephone number and the number of a contact person to be used
during active follow-up, and none of the patients was lost to
follow-up within 2 years.
Data collection
Data from the medical records of the patients,
including age, para, aborta, number of dilation and curettage
procedures, caesarean delivery, smoking status, serum C-reactive
protein (CRP) levels, serum WBC count, body temperature, abscess
diameter, menopause, smoking status, presence of an intrauterine
device (IUD), duration of IUD placement and previous pelvic
operation, were collected. The association between these variables
and the clinical prognosis of patients with TOA and pelvic abscess
were evaluated. The location of abscesses, different operation
types, operation time, blood loss volume, duration of temperature
≥38°C, length of hospitalization and isolated microorganisms were
also recorded in patients who underwent laparoscopic treatment.
Bacterial culture of pyogenic fluids and drug sensitivity tests
were performed for all patients who received laparoscopic
treatment.
Statistical analysis
The distribution of continuous data was assessed
using the Kolmogorov-Smirnov test. Normally distributed continuous
data were expressed as the mean ± standard deviation and compared
using the Student's t-test. Non-normally distributed data were
presented as median (range) and analyzed with the Mann-Whitney
U-test. Categorical data were presented as a proportion and
analyzed with the chi-squared test or Fisher's exact test, as
appropriate. Receiver operating characteristics (ROC) curve
analysis was used to identify the cut-off value of abscess size for
antibiotic treatment failure. Multivariate logistic regression
model was used to explore the association between clinical
variables and antibiotic therapy failure in the conservative
treatment group. All statistical analyses were performed using the
SPSS 19.0 software (IBM Corp.). P<0.05 was considered to
indicate statistical significance.
Results
Patient characteristics
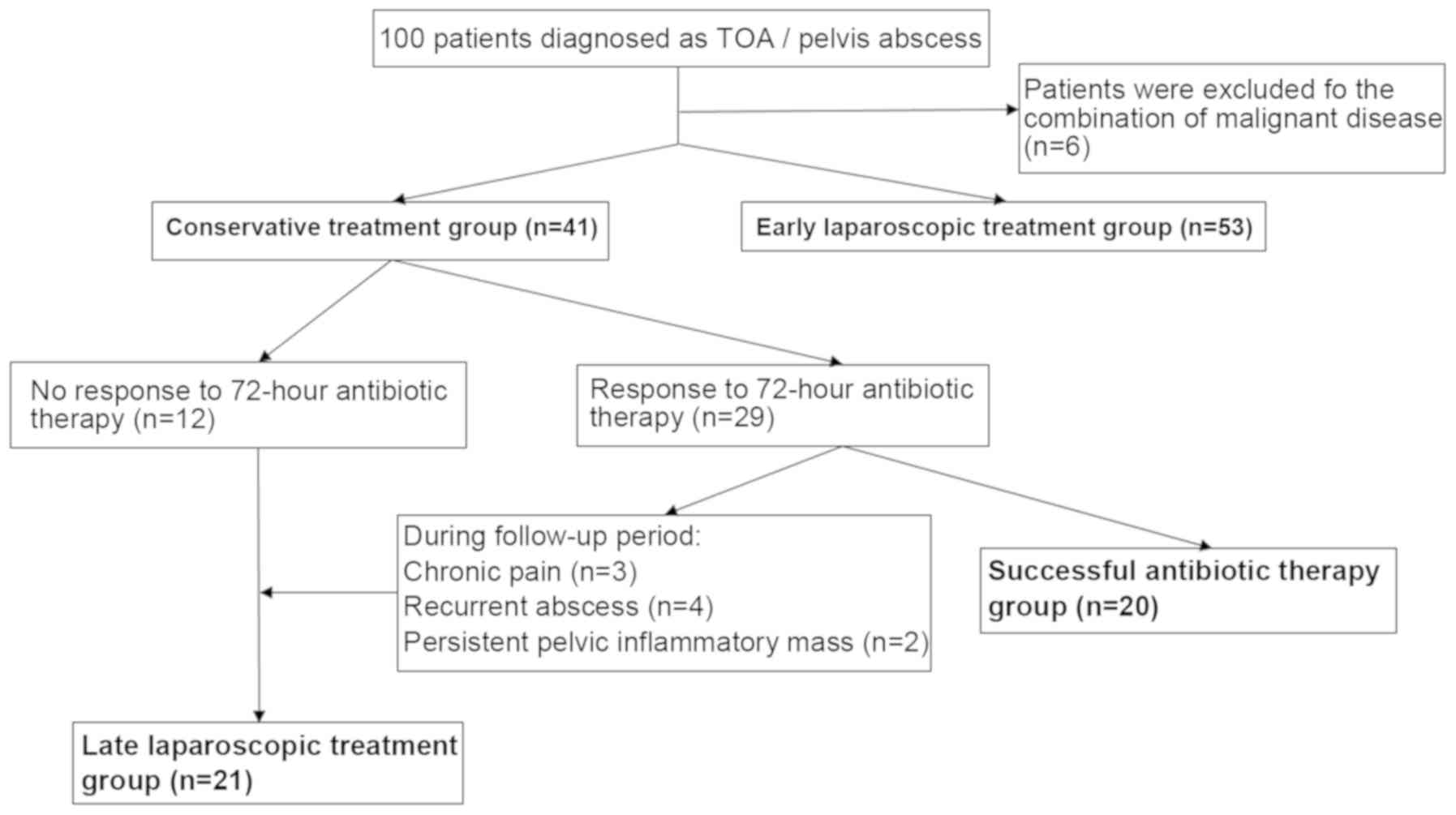
A total of 100 patients initially diagnosed with TOA
or pelvic abscess were included in the present study. Of these, six
cases (including three menopausal females) were excluded due to
malignant diseases. Eventually, the data of 94 patients were
analyzed. The mean age of the patients was 41 years (range, 26–60
years). A total of 53 patients opted for early laparoscopic
treatment within 6–12 h of diagnosis (early laparoscopic treatment
group), while 41 patients received conservative antibiotic therapy
(conservative treatment group). Among the patients receiving
antibiotic therapy, 29 cases were responsive to the 72 h
conservative therapy, of which 9 patients received late
laparoscopic therapy due to chronic pain (n=3), recurrent abscess
(n=4) and persistent pelvic inflammatory mass (n=2). Therefore, 20
patients achieved successful antibiotic therapy (successful
antibiotic therapy group). Furthermore, 12 patients failed to
respond to the antibiotic therapy within 72 h, and they received
late laparoscopic therapy. Thus, a total of 21 patients underwent
late laparoscopic therapy (late laparoscopic treatment group). The
flow chart of the study is presented in Fig. 1. The baseline characteristics of
patients in the early laparoscopic treatment group and conservative
treatment group are listed in Table
I. The duration of elevated temperature >38°C and length of
hospitalization were significantly longer in the conservative
treatment group than those in the early laparoscopic treatment
group (all P<0.001). Regarding the other documented variables,
no significant differences were observed between the two groups
(all P>0.05). The patients were followed up for 32.5±4.2 and
33.8±3.4 months in the early laparoscopic treatment group and
conservative treatment group, respectively, and the difference was
not statistically significant (P=0.101).
 | Table I.Comparison of patients'
characteristics between early laparoscopic treatment group and
conservative treatment group. |
Table I.
Comparison of patients'
characteristics between early laparoscopic treatment group and
conservative treatment group.
| Variables | Early laparoscopic
treatment group (n=53) | Conservative
treatment group (n=41) | P-value |
|---|
| Age (years) | 39.2 (25–56) | 38.5 (24–58) | 0.876 |
|
20–29 | 8 (15.1) | 6 (14.6) | 0.823 |
|
30–39 | 20 (37.7) | 18 (43.9) |
|
|
≥40 | 25 (47.2) | 17 (41.5) |
|
| Gravidity |
|
| 0.953 |
| ≤2 | 21 (39.6) | 16 (39.0) |
|
|
>2 | 32 (60.4) | 25 (61.0) |
|
| Parity |
|
| 0.958 |
| ≤1 | 48 (90.6) | 37 (90.2) |
|
|
>1 | 5 (9.4) | 4 (9.8) |
|
| Times of
abortion | 2.1±1.5 | 2.3±1.5 | 0.523 |
| Menopause | 2 (3.8) | 1 (2.4) | 0.999 |
| Presence of an
IUD | 27 (50.9) | 23 (56.1) | 0.619 |
| Duration of IUD
presence (years) | 7.5±5.2 | 8.3±6.7 | 0.529 |
| Smoking | 11 (20.6) | 7 (17.1) | 0.999 |
| Bilaterality | 19 (35.8) | 15 (36.6) | 0.941 |
| Diameter of the
abscess (cm) | 6.0±1.7 | 5.7±2.1 | 0.458 |
| WBC count
(×109 cells/mm3) | 17.3±2.8 | 16.9±3.0 | 0.511 |
| CRP (mg/dl) | 132.5±26.8 | 127.6±32.7 | 0.438 |
| Body temperature
(°C) | 38.6±0.7 | 38.8±0.5 | 0.11 |
| Previous pelvic
operation | 21 (39.6) | 13 (31.7) | 0.428 |
|
Appendectomy | 4 | 2 |
|
|
Cesarean section | 11 | 8 |
|
| Tubal
ligation | 3 | 2 |
|
| Ovarian
cystectomy | 2 | 1 |
|
|
Hysteromyomectomy | 1 | 0 |
|
| Previous pelvic
inflammation history | 9 (17.0) | 6 (14.6) | 0.758 |
| Length of
hospitalization (days) | 6.8±1.5 | 10.5±2.5 | <0.001 |
| Duration of body
temperature ≥38°C (days) | 2.2±0.3 | 3.2±0.8 | <0.001 |
| Follow-up
(months) | 32.5±4.2 | 33.8±3.4 | 0.101 |
Comparison of the clinical
characteristics between the late laparoscopic group and successful
antibiotic treatment group
Of all the patients who underwent conservative
antibiotic treatment, 21 (51.2%) received laparoscopic exploration
(late laparoscopic treatment group), including 12 cases lacking a
response to antibiotics (no reduced mass size or persistent fever
after 72 h), two patients with persistent pelvic inflammatory mass
(one in the third month and one in the fifth month, respectively),
three cases with chronic pain (persisting until the fourth month in
two patients and until the sixth month in one patient) and four
cases with recurrent abscess (one in the third month, two in the
fifth month and one in the sixth month). All of them received
laparoscopic exploration between 3 days and 6 months after
initiation of antibiotic treatment. The abscess size of the
patients in the late laparoscopic treatment group was significantly
larger than that in the successful antibiotic therapy group
(6.2±1.8 cm vs. 4.8±1.4 cm, P=0.008).
Diagnosis, surgical details and
vaginal culture results of the patients who received early and late
laparoscopic treatment
Regarding the specific diagnosis, the patients in
the early laparoscopic treatment group comprised 19 cases (35.8%)
of TOA, 26 cases (49.1%) of pyosalpinx, 4 cases (7.5%) of pelvic
abscess, 2 cases (3.8%) of appendicitis and 2 cases (3.8%) of
endometriosis cyst rupture complicated with infection, while the
late laparoscopic treatment group included 12 cases (57.1%) of TOA
and 9 cases (42.9%) of pyosalpinx. The types of surgeries did not
demonstrate significant difference between the two groups. No organ
injury was observed in either group. The results of vaginal
cultures indicated that 34 patients in the early laparoscopic
treatment group and 11 patients in the late laparoscopic treatment
group were positive. A higher proportion of bilateral adhesion was
observed in the late laparoscopic group (35.8% vs. 61.9%, P=0.041).
The results are provided in Table
II.
| Table II.Diagnosis, surgical details and
vaginal culture results of the patients who underwent laparoscopic
surgery. |
Table II.
Diagnosis, surgical details and
vaginal culture results of the patients who underwent laparoscopic
surgery.
| Item | Early laparoscopic
group (n=53) | Late laparoscopic
group (n=21) | P-value |
|---|
| Diagnosis |
|
| 0.395 |
|
Tubo-ovarian abscess | 19 | 12 |
|
|
Pyosalpinx | 26 | 9 |
|
| Pelvic
abscess | 4 | – |
|
|
Endometriosis cyst | 2 | – |
|
|
Appendicular abscess | 2 | – |
|
| Operation |
|
| 0.419 |
|
Salpingectomy | 22 | 8 |
|
| Simple
salpingo-oophorectomy | 17 | 10 |
|
|
Fallopian tube incision
drainage | 5 | 2 |
|
| Pus
cavity incision drainage | 5 |
|
|
| Ovarian
cystectomy | 2 |
|
|
|
Appendicectomy | 2 |
|
|
|
Hysterectomy and simple
salpingo-oophorectomy | 0 | 1 |
|
| Positive vaginal
culture |
|
|
|
|
Escherichia
coli | 24 | 7 | 0.348 |
|
Peptostreptococci | 8 | 4 | 0.731 |
|
Baumannii | 2 | 0 | 0.999 |
| Bilaterality | 19 (35.8) | 13 (61.9) | 0.041 |
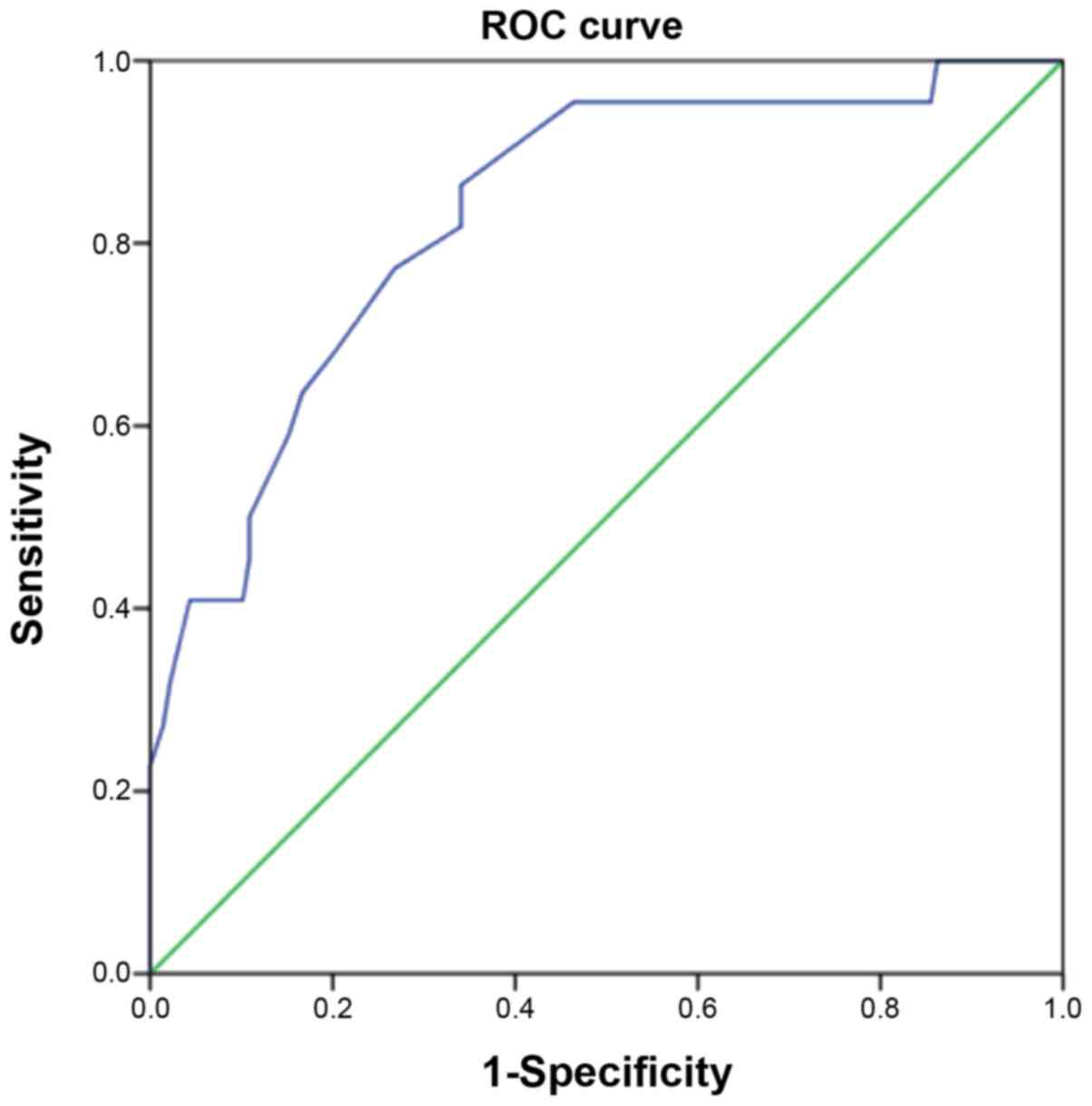
Risk factors of antibiotic
failure
ROC curve analysis was performed to determine the
best cut-off value of abscess diameter in order to further explore
the risk of antibiotic failure. The area under the curve was 0.862
(95% CI: 0.742–0.923), and an abscess diameter of 5.5 cm was
obtained as the cut-off of antibiotic failure (Fig. 2). The sensitivity, specificity,
positive predictive value and negative predictive value of
antibiotic failure were 81, 85, 85 and 81%, respectively, and the
Youden index was 0.66. Multivariate regression analysis was
performed to investigate the independent risk factors for failure
of antibiotic therapy (Table III).
Age, diameter of the abscess, serum WBC count, serum CRP, presence
of an IUD, smoking status, bilaterality, menopause, caesarean
delivery and previous pelvic inflammation were considered as
dependent variants. The results suggested that only abscess
diameter ≥5.5 cm was an independent risk factor of parenteral
antibiotic therapy failure [odds ratio (OR) = 5.742; 95%CI:
2.025–16.182, P=0.001].
| Table III.Multivariate logistic regression
model for clinical characteristics affecting antibiotic therapy
failure in conservative treatment group. |
Table III.
Multivariate logistic regression
model for clinical characteristics affecting antibiotic therapy
failure in conservative treatment group.
|
| Univariate
regression analysis | Multivariate
regression analysis |
|---|
|
|
|
|
|---|
| Factor | OR | 95%CI | P-value | OR | 95%CI | P-value |
|---|
| Age (years) | 1.326 | 0.830–2.119 | 0.238 | 1.215 | 0.785–1.880 | 0.382 |
| Diameter of the
abscess ≥5.5 cm | 4.274 | 1.813–10.075 | <0.001 | 5.724 | 2.025–16.182 | 0.001 |
| WBC count
(×109 cells/mm3) | 1.534 | 0.546–4.311 | 0.417 | 1.581 | 0.658–3.800 | 0.306 |
| CRP >50
mg/dl | 0.914 | 0.556–1.503 | 0.723 | 0.875 | 0.502–1.526 | 0.638 |
| Presence of
intrauterine device | 1.725 | 0.667–4.464 | 0.261 | 1.291 | 0.763–2.184 | 0.341 |
| Smoking status | 1.391 | 0.632–3.060 | 0.412 | 1.615 | 0.555–4.699 | 0.379 |
| Caesarean
delivery | 0.968 | 0.877–1.069 | 0.520 | 0.768 | 0.361–1.633 | 0.493 |
| Previous pelvic
inflammation | 1.530 | 0.777–3.014 | 0.219 | 1.135 | 0.905–1.423 | 0.273 |
| Bilaterality | 1.467 | 0.982–2.191 | 0.061 | 2.026 | 0.921–4.455 | 0.079 |
| Menopause | 1.216 | 0.427–3.461 | 0.714 | 1.187 | 0.535–2.632 | 0.673 |
Discussion
In the present study, the clinical value of early
laparoscopic treatment for TOA and pelvic abscess was investigated.
The results demonstrated that patients may benefit from early
laparoscopic treatment. An abscess diameter of >5.5 cm was a
significant factor associated with failure of antibiotic treatment
for pelvic abscess. The present study also suggested that patients
in the early laparoscopic group achieved more rapid recovery.
Compared with the patients in the conservative treatment group, the
duration of body temperature ≥38°C and length of hospitalization
were reduced in the early laparoscopic treatment group.
Furthermore, a relatively shorter operation time and reduced blood
loss volume were observed in patients of the early laparoscopic
treatment group. These significant differences may be associated
with less severe adhesions in the early laparoscopic treatment
group. A previous study indicated that antibiotic therapy resulted
in prolonged time of exposure of the adnexa around purulent
material (15).
It is generally recognized that the TOA and pelvic
abscess may be attributed to ascending bacterial infection from the
lower genital tract, causing abscess formation in the fallopian
tubes, uterus and peritoneal cavity (16). TOA formation may lead to severe
complications, including TOA rupture, if not treated without delay.
Commonly detected bacteria from abscess aspiration or cavities are
E. coli, Bacteriodes fragilis, Bacteriodes species,
Peptostreptococcus, Peptococcus, and aerobic
Streptococcus (17,18). As the first-line medical treatment
for TOA and pelvic abscess treatment, i.v. broad-spectrum
antibiotics covering N. gonorrhoeae, C. trachomatis and
anaerobic bacteria is recommended (13,19).
However, in patients diagnosed with TOA and pelvic abscess,
antibiotic therapy has been reported to have a failure rate of
12–76% (20,21). Surgical treatments are necessary when
patients exhibit no response or persistent mass after standard
antibiotic therapy for 48–72 h. A study by Topcu et al
(9) suggested that 79.8% (87/109) of
patients who were managed surgically or discharged after 7 days of
antibiotic therapy had a poor prognosis. The results of the present
study indicated that 51.2% (21/41) of patients in the conservative
treatment group finally received late laparoscopic surgery due to
the poor response to antibiotics or chronic pain, persistent pelvic
inflammatory mass or abscess recurrence.
The potential benefit of early laparoscopic
treatment for patients with TOA or pelvic abscess has remained
controversial. Immediate laparoscopic treatment was recommended by
Roberts and Dockery (22), since it
achieved a response rate of 90–100% as opposed to 20–87% in
patients with conservative therapy comprising broad-spectrum
antibiotics. A previous study also demonstrated that, compared with
surgical intervention, the recurrence rate of TOA in patients who
received antibiotic therapy was higher (23). For patients with TOA and pelvic
abscess, the widely-recognized risk factor for surgical treatment
after antibiotic therapy failure is abscess size, which may be
considered an objective predictive parameter (9,24–26). In
these studies, only an abscess diameter of ≥5-6.5 cm (lower limit)
was considered a significant risk factor for poor response to
antibiotic therapy. This may be due to the limited penetration of
antibiotics into the abscess cavity (14,27). The
present study identified an abscess diameter of ≥5.5 cm as the
independent risk factor of parenteral antibiotic therapy failure
(OR=5.742; 95%CI: 2.025–16.182, P=0.001), with 81% sensitivity and
85% specificity.
Menopause is a surgical indication, as in
post-menopausal females, TOA and pelvic abscess may accompany a
malignant tumor (19,28). Protopapas et al (29) reported a malignancy rate of 8/17
(47%) in post-menopausal patients with TOA and 1/76 (1.3%) in
pre-menopausal patients. In the population of the present study, 7
post-menopausal patients were diagnosed with pelvic abscess, 3 of
which (42.9%) were combined with malignant tumor. However, other
studies reported inconsistent results, including a Norwegian study
that observed no elevated malignancy risk in post-menopausal
patients and only 1 case among 16 post-menopausal patients was
diagnosed with pelvic malignancy (30).
In patients who desire to maintain fertility, early
laparoscopic treatment should also be considered. An extensive
review of the published literature and MEDLINE was performed to
investigate reasonable management options for TOA patients. Rates
of responders, pregnancies and complications associated with
various management strategies were compared (2). For patients with no suspected rupture,
the pregnancy rates were 4–15% when treated with antibiotic therapy
alone; however, the pregnancy rate reached 32–63% if treated with
antibiotics in combination with laparoscopic drainage within 24 h.
The reason for this higher pregnancy rate in patients treated by
antibiotics in combination with immediate laparoscopic drainage may
be associated with less adhesion around uterine adnexa, and this
was also verified in a population of patients who underwent
second-look laparoscopy (2).
Unfortunately, the number of available studies on pregnancy
outcomes after different treatments for TOA and pelvic abscess is
small. While the pregnancy rate was not assessed in the present
study, it indicated that more cases of bilateral adhesion were
present in the late laparoscopic group.
Previous studies have investigated the risk factors
of TOA and its poor outcomes, and the potential factors associated
with high risk of failure of conservative treatment included age
(10,31,32),
parity (4,24,31),
high levels of serum inflammatory biomarkers, e.g. WBC and CRP
(8,10,25,31) and
smoking status (10). On the
contrary, the results of other studies indicated that age, levels
of WBC and CRP, gravida, parity, body temperature and smoking
status were not associated with antibiotic therapy failure
(9,27). The present study also demonstrated
that there were no obvious differences in age, serum inflammatory
biomarker levels, body temperature, presence of IUD, smoking
status, caesarean delivery and previous pelvic inflammation between
the late laparoscopic treatment group and the successful antibiotic
therapy group. Certain studies reported that patients diagnosed
with endometrial cyst concomitant with TOA tended to exhibit a poor
response to therapeutic efficacy of antibiotics and a higher rate
of late surgical treatment than those diagnosed as simple pelvic
abscess (33,34). However, these results were not
consistent with those of another study, which suggested that
endometrial cysts did not influence the antibiotic treatment
(27). Thus, the risk factors
influencing antibiotic therapy failure in TOA patients require
further exploration.
Abscess tissues may be easily sampled for exact
diagnosis through laparoscopic exploration. In the present study,
the positive rate of pus bacterial culture was 60.8% (45/74). The
commonly detected bacteria were Escherichia coli and
Peptostreptococci, which was consistent with the results of
a previous study (35). Appendicitis
may be another differential diagnosis for patients with suspected
TOA or pelvic abscess, which gynecologists should be aware of
(36). In the present study, two
cases of appendicitis abscess and two cases of endometriosis cyst
rupture were included, and the patients received appendectomy and
ovarian cystectomy, respectively.
The surrounding tissues, including bowel, omentum
majus, uterus or bladder, may adhere tightly to the abdominal wall,
and these tissues may become fragile due to the presence of
inflammation. However, the reported occurrence rate of bowel
injuries during laparoscopic surgery is relatively low (0.13%),
which may also be repaired by laparotomy exploration (37). No bowel, bladder or urethral injury
was observed in the patients of the present study. In those
patients who had PID or a history of abdominal surgery, the first
trocar was placed 4 cm above the umbilicus in order to avoid
potential bowel adhesion. Furthermore, in recent years, MRI has
been able to clearly display the organs adhering to the abdominal
wall prior to surgery (38). In the
present study, extensive adhesion of the intestinal canal prior to
laparoscopic treatment was observed in four patients; the puncture
point was located in the right upper quadrant and the adhesion was
verified under direct vision.
The present study was not without any limitations.
First, the sample size of the patients was limited and this was
only a single-center study. The results require further
verification in a multi-center study with a larger number of
patients. Furthermore, the study design was retrospective with
inherent bias, and data collection may not have been sufficient to
include all relevant information, including late recurrence and
late complications. Finally, the follow-up period was relatively
short and the data collection and comparisons of pregnancy rate and
fertility problems between conservative therapy and early
laparoscopic groups were not performed and evaluated.
In conclusion, early laparoscopic treatment may be
associated with better clinical prognosis than conservative
treatment and late laparoscopy for patients with TOA or pelvic
abscess, particularly for those with an abscess diameter of ≥5.5
cm.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The dataset supporting the results of the present
study are included within the article.
Authors' contributions
HZ conceived and supervised the study; XJ, KZ and HZ
performed the experiments; XJ, MS, MS and HY analyzed the data; XJ
and KZ wrote the manuscript; HZ and KZ revised the manuscript. All
authors reviewed the results and approved the final version of the
manuscript.
Ethics approval and consent to
participate
This study was approved by the clinical ethics
committee of Xuzhou City Hospital of Traditional Chinese Medicine
(Xuzhou, China; no. 20140305) and individual informed consent was
waived for retrospective analysis.
Patient consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing
interests.
References
|
1
|
McNeeley SG, Hendrix SL, Mazzoni MM, Kmak
DC and Ransom SB: Medically sound, cost-effective treatment for
pelvic inflammatory disease and tuboovarian abscess. Am J Obstet
Gynecol. 178:1272–1278. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rosen M, Breitkopf D and Waud K:
Tubo-ovarian abscess management options for women who desire
fertility. Obstet Gynecol Surv. 64:681–689. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zeger W and Holt K: Gynecologic
infections. Emerg Med Clin North Am. 21:631–648. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kuo CF, Tsai SY, Liu TC, Lin CC, Liu CP
and Lee CM: Clinical characteristics and treatment outcomes of
patients with tubo-ovarian abscess at a tertiary care hospital in
Northern Taiwan. J Microbiol Immunol Infect. 45:58–64. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Goharkhay N, Verma U and Maggiorotto F:
Comparison of CT- or ultrasound-guided drainage with concomitant
intravenous antibiotics vs. intravenous antibiotics alone in the
management of tubo-ovarian abscesses. Ultrasound Obstet Gynecol.
29:65–69. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
6
|
Reed SD, Landers DV and Sweet RL:
Antibiotic treatment of tuboovarian abscess: Comparison of
broad-spectrum beta-lactam agents versus clindamycin-containing
regimens. Am J Obstet Gynecol. 164:1556–1562. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
To J, Aldape D, Frost A, Goldberg GL,
Levie M and Chudnoff S: Image-guided drainage versus
antibiotic-only treatment of pelvic abscesses: Short-term and
long-term outcomes. Fertil Steril. 102:1155–1159. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Farid H, Lau TC, Karmon AE and Styer AK:
Clinical characteristics associated with antibiotic treatment
failure for tuboovarian abscesses. Infect Dis Obstet Gynecol.
2016:51202932016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Topcu HO, Kokanali K, Güzel AI, Tokmak A,
Erkılınç S, Ümit C and Doğanay M: Risk factors for adverse clinical
outcomes in patients with tubo-ovarian abscess. J Obstet Gynaecol.
35:699–702. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Akkurt MÖ, Yalcin SE, Akkurt I, Tatar B,
Yavuz A, Yalçın Y, Akgül MA and Kayıkçıoğlu F: The evaluation of
risk factors for failed response to conservative treatment in
tubo-ovarian abscesses. J Turk Ger Gynecol Assoc. 16:226–230. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Silva F, Castro J, Godinho C, Gonçalves J,
Ramalho G and Valente F: Minimally invasive approach of
tubo-ovarian abscesses. Rev Bras Ginecol Obstet. 37:115–118. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Brun JL, Graesslin O, Fauconnier A, Verdon
R, Agostini A, Bourret A, Derniaux E, Garbin O, Huchon C, Lamy C,
et al: Updated French guidelines for diagnosis and management of
pelvic inflammatory disease. Int J Gynaecol Obstet. 134:121–125.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Workowski K and Bolan G; Centers for
Disease Control and Prevention, : Sexually transmitted diseases
treatment guidelines, 2015. MMWR Recomm Rep. 64:1–137.
2015.PubMed/NCBI
|
|
14
|
Chu L, Ma H, Liang J, Li L, Shen A, Wang
J, Li H and Tong X: Effectiveness and adverse events of early
laparoscopic therapy versus conservative treatment for tubo-ovarian
or pelvic abscess: A single-center retrospective cohort study.
Gynecol Obstet Invest. 1–9. Jan 4–2019.(Epub ahead of print).
|
|
15
|
Henry-Suchet J, Soler A and Loffredo V:
Laparoscopic treatment of tuboovarian abscesses. J Reprod Med.
29:579–582. 1984.PubMed/NCBI
|
|
16
|
Granberg S, Gjelland K and Ekerhovd E: The
management of pelvic abscess. Best Pract Res Clin Obstet Gynaecol.
23:667–678. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jaiyeoba O, Lazenby G and Soper D:
Recommendations and rationale for the treatment of pelvic
inflammatory disease. Expert Rev Anti Infect Ther. 9:61–70. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wiesenfeld HC and Sweet RL: Progress in
the management of tuboovarian abscesses. Clin Obstet Gynecol.
36:433–444. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bevan CD, Johal BJ, Mumtaz G, Ridgway GL
and Siddle NC: Clinical, laparoscopic and microbiological findings
in acute salpingitis: Report on a United Kingdom cohort. Br J
Obstet Gynaecol. 102:407–414. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Peipert JF, Ness RB, Blume J, Soper DE,
Holley R, Randall H, Sweet RL, Sondheimer SJ, Hendrix SL, Amortegui
A, et al: Clinical predictors of endometritis in women with
symptoms and signs of pelvic inflammatory disease. Am J Obstet
Gynecol. 184:856–864. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gaitán H, Angel E, Diaz R, Parada A,
Sanchez L and Vargas C: Accuracy of five different diagnostic
techniques in mild-to-moderate pelvic inflammatory disease. Infect
Dis Obstet Gynecol. 10:171–180. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Roberts W and Dockery JL: Operative and
conservative treatment of tubo-ovarian abscess due to pelvic
inflammatory disease. South Med J. 77:860–863. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Dewitt J, Reining A, Allsworth JE and
Peipert JF: Tuboovarian abscesses: Is size associated with duration
of hospitalization & complications? Obstet Gynecol Int.
2010:8470412010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kinay T, Unlubilgin E, Cirik DA,
Kayikcioglu F, Akgul MA and Dolen I: The value of ultrasonographic
tubo-ovarian abscess morphology in predicting whether patients will
require surgical treatment. Int J Gynaecol Obstet. 135:77–81. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Güngördük K, Guzel E, Asicioğlu O,
Yildirim G, Ataser G, Ark C, Gulova SS and Uzuncakmak C: Experience
of tubo-ovarian abscess in western Turkey. Int J Gynaecol Obstet.
124:45–50. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chappell CA and Wiesenfeld HC:
Pathogenesis, diagnosis, and management of severe pelvic
inflammatory disease and tuboovarian abscess. Clin Obstet Gynecol.
55:893–903. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mizushima T, Yoshida H, Ohi Y, Ishikawa M
and Hirahara F: Evaluating the risk factors for developing
resistance to parenteral therapy for tubo-ovarian abscess: A
case-control study. J Obstet Gynaecol Res. 39:1019–1023. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Workowski KA and Berman S; Centers for
Disease Control and Prevention (CDC), : Sexually transmitted
diseases treatment guidelines, 2010. MMWR Recomm Rep. 59:1–110.
2010.PubMed/NCBI
|
|
29
|
Protopapas AG, Diakomanolis ES, Milingos
SD, Rodolakis AJ, Markaki SN, Vlachos GD, Papadopoulos DE and
Michalas SP: Tubo-ovarian abscesses in postmenopausal women:
Gynecological malignancy until proven otherwise? Eur J Obstet
Gynecol Reprod Biol. 114:203–209. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gjelland K, Ekerhovd E and Granberg S:
Transvaginal ultrasound-guided aspiration for treatment of
tubo-ovarian abscess: A study of 302 cases. Am J Obstet Gynecol.
193:1323–1330. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Greenstein Y, Shah AJ, Vragovic O, Cabral
H, Soto-Wright V, Borgatta L and Kuohung W: Tuboovarian abscess.
Factors associated with operative intervention after failed
antibiotic therapy. J Reprod Med. 58:101–106. 2013.PubMed/NCBI
|
|
32
|
Halperin R, Levinson O, Yaron M, Bukovsky
I and Schneider D: Tubo-ovarian abscess in older women: Is the
woman's age a risk factor for failed response to conservative
treatment? Gynecol Obstet Invest. 55:211–215. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Liu YT, Shi HH, Yu X, Wang S, Fan QB and
Liu HY: Clinical analysis of pelvic abscess with endometriosis.
Zhonghua Fu Chan Ke Za Zhi. 52:164–167. 2017.(In Chinese).
PubMed/NCBI
|
|
34
|
Villette C, Bourret A, Santulli P, Gayet
V, Chapron C and de Ziegler D: Risks of tubo-ovarian abscess in
cases of endometrioma and assisted reproductive technologies are
both under- and overreported. Fertil Steril. 106:410–415. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Landers DV and Sweet RL: Tubo-ovarian
abscess: Contemporary approach to management. Rev Infect Dis.
5:876–884. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hiller N, Fux T, Finkelstein A, Mezeh H
and Simanovsky N: CT differentiation between tubo-ovarian and
appendiceal origin of right lower quadrant abscess: CT, clinical,
and laboratory correlation. Emerg Radiol. 23:133–139. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
van der Voort M, Heijnsdijk EA and Gouma
DJ: Bowel injury as a complication of laparoscopy. Br J Surg.
91:1253–1258. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ghonge NP and Ghonge SD: Computed
tomography and magnetic resonance imaging in the evaluation of
pelvic peritoneal adhesions: What radiologists need to know? Indian
J Radiol Imaging. 24:149–155. 2014. View Article : Google Scholar : PubMed/NCBI
|