Introduction
Acute cerebral hemorrhage is a type of primary
non-traumatic intracerebral hemorrhage, accounting for 15–20% of
all strokes, and the mortality rate is as high as approximately
30%. To date, no specific treatment method has been developed to
effectively reduce mortality of acute cerebral hemorrhage (1). The morbidity of cerebral hemorrhage is
twice that of ischemic cerebrovascular disease (2), and the 30-day mortality is as high as
41% (3). Studies have indicated that
peripheral blood leukocytes are associated with the prognosis of
patients with cerebral hemorrhage. Leukocytes have an important
role in the secondary damage caused by inflammatory reactions after
intracerebral hemorrhage (4), which
are associated with early neurologic impairment in patients with
cerebral hemorrhage (5). In a mouse
model of intracerebral hemorrhage, it has been demonstrated that
peripheral blood mononuclear cells significantly aggregate at the
hemorrhage site compared with other types of inflammatory cell
(6). Matrix metalloproteinases
(MMPs) are considered as important inflammatory mediators (7), and neutrophils are the major source of
MMP9 (8). Previous studies have
indicated that peripheral blood leukocytes are associated with
inflammatory reactions in acute cerebral hemorrhage. However, the
mechanism of the inflammatory response after intracerebral
hemorrhage has not been fully elucidated.
Gastrointestinal bleeding caused by Cushing ulcer is
one of the complications of acute cerebral hemorrhage, with a
morbidity of 48.3% and a mortality of as high as 87.9%. Therefore,
identifying and preventing gastrointestinal hemorrhage in patients
with cerebral hemorrhage may effectively reduce the mortality rate.
Previous studies have indicated that NLR and PLR are closely linked
to the degree of severity and prognosis of inflammation-associated
diseases, including malignant tumors and acute pancreatitis
(9,10). Based on clinical data and preliminary
observations, our group determined that the neutrophil count (NEU)
has a certain value in identifying patients with acute cerebral
hemorrhage combined with gastrointestinal hemorrhage. The present
study aimed to explore the clinical significance of NLR and PLR in
the diagnosis and prognosis of acute cerebral hemorrhage.
Patients and methods
Subjects
A total of 335 patients with acute cerebral
hemorrhage diagnosed by clinical examinations and cranial computed
tomography (CT) at the First People's Hospital of Wujiang District
(Suzhou, China) between January 2012 and January 2017 were
selected. The cohort comprised 181 male patients and 154 female
patients with an age range of 32–87 years (median age, 60 years).
All enrolled patients were admitted due to acute cerebral
hemorrhage. Among them, 86 patients who experienced
gastrointestinal hemorrhage were selected as the observation group
and the remaining 249 were selected as a negative control group.
The diagnostic criteria for gastrointestinal hemorrhage were as
follows: Bloody or brown vomitus or gastric tube drainage, or
positive occult blood test; tarry stool or melena or positive fecal
occult blood test. In all cases, gastrointestinal hemorrhage
occurred within 2 weeks of acute cerebral hemorrhage. Exclusion
criteria included admission at 24 h after the onset, history of
blood transfusion within 3 months, comorbidity of hematological
diseases, tumors, severe dysfunctions of liver and kidney,
endocrine or digestive system diseases, and various autoimmune
diseases, as well as taking of immunosuppressants, a history of
acute infection or antibiotic medication in last 3 weeks, and a
history of stroke. The present study was approved by the ethics
committee of the First People's Hospital of Wujiang District
(Suzhou, China). Written informed consent was obtained from all
participants prior to the study.
Collection of basic
characteristics
Peripheral blood samples of all subjects were
collected within 24 h after admission and every 2 days since after.
The NEU, white blood cell count (WBC), platelet count (PLT), NLR
and PLR of each subject were recorded. Furthermore, sex, age, blood
pressure, the site of cerebral hemorrhage and the volume of
bleeding, the Glasgow Coma Scale (GCS) score and presence of
hematosepsis were also recorded.
Statistical analysis
SPSS 22.0 statistical software (IBM Corp.) was used
for data analysis. Measurement data were expressed as the mean ±
standard deviation. Student's t-test or the Chi-squared test were
used to compare differences between the two groups. Kaplan-Meier
analysis was performed to draw the survival curves and the log-rank
test was utilized to assess differences in survival between the
groups. Univariate Cox hazard analysis and stepwise multivariate
Cox hazard analysis were performed to identify independent risk
factors of acute cerebral hemorrhage combined with gastrointestinal
hemorrhage. P<0.05 was considered to indicate statistical
significance.
Results
Basic characteristics of the
subjects
A total of 355 patients with acute cerebral
hemorrhage combined with gastrointestinal hemorrhage diagnosed by
clinical examinations and cranial CT at our hospital between
January 2012 and January 2017 were selected for inclusion. Based on
the presence of the complication of gastrointestinal hemorrhage, 86
subjects were assigned to the observation group and the 249
remaining subjects were enrolled in the negative control group.
Sex, age, blood pressure, the site of cerebral hemorrhage, the
amount of bleeding, GCS score and presence of hematosepsis were
recorded and compared between the two groups. The specific
information of the subjects is listed in Table I. There was no significant difference
in sex, age and blood pressure between the two groups, while the
observation group had a higher GCS score, volume of cerebral
hemorrhage and rate of hematosepsis.
 | Table I.Baseline clinicopathological
characteristics of the patients. |
Table I.
Baseline clinicopathological
characteristics of the patients.
| Parameter | Observation group
(n=86) | Control group
(n=249) | P-value |
|---|
| Sex |
|
| 0.713 |
| Male | 45 (52.3) | 136 (54.6) |
|
|
Female | 41 (47.7) | 113 (45.4) |
|
| Age (years) | 59.3±6.2 | 61.8±5.3 | 0.697 |
| Blood pressure
(mmHg) |
|
| 0.543 |
|
>180/100 | 68 (79.1) | 189 (75.9) |
|
|
<180/100 | 18 (20.9) | 60 (24.1) |
|
| Cerebral hemorrhage
(ml) |
|
>30 | 53 (61.6) | 111 (44.6) | 0.006 |
|
<30 | 33 (38.4) | 138 (55.4) |
|
| Location |
|
| 0.183 |
|
Brainstem | 7 (8.1) | 16 (6.4) |
|
|
Cerebellum | 11 (12.8) | 36 (14.4) |
|
| Lobe | 10 (11.6) | 37 (14.9) |
|
| Basal
ganglia | 38 (44.2) | 108 (43.4) |
|
|
Thalamus | 20 (23.3) | 52 (20.9) |
|
| GCS score | 6.13±2.68 | 10.69±3.67 | 0.002 |
| Hematosepsis | 21 (24.4) | 30 (12.0) | 0.005 |
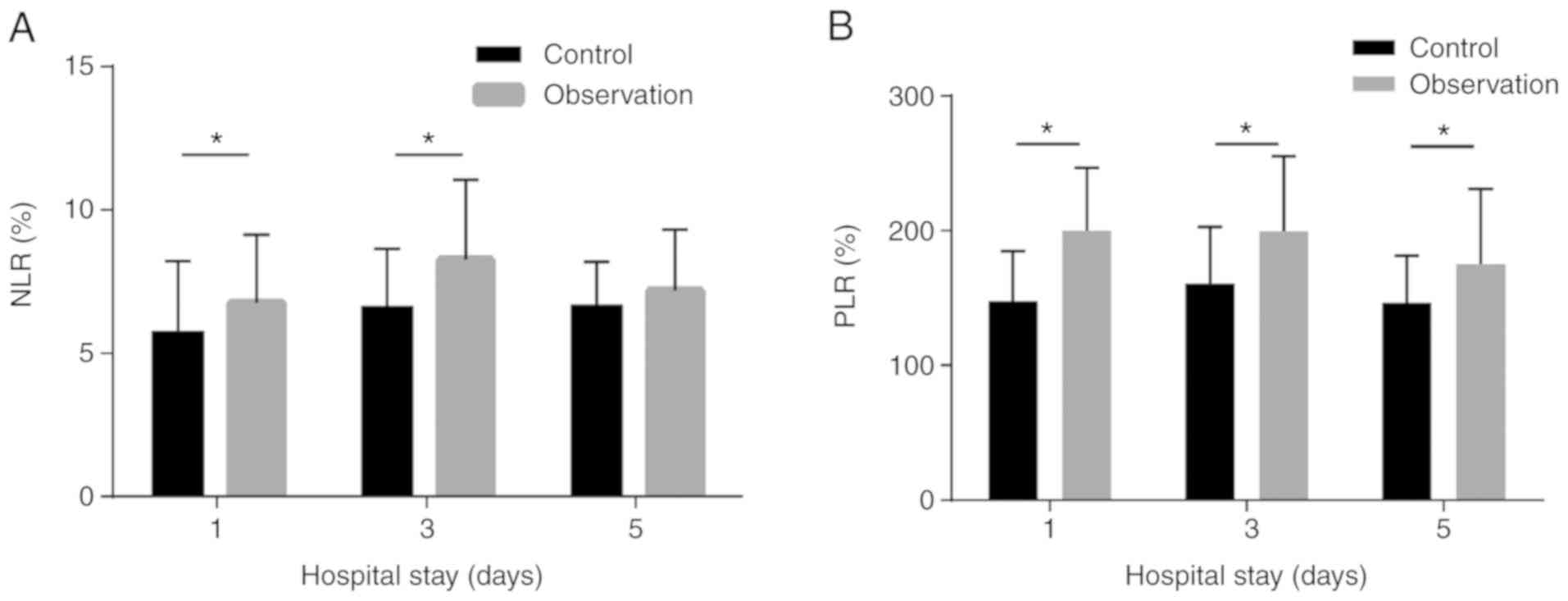
Comparisons of NLR and PLR
Within 5 days of admission, the NLR and PLR were
markedly higher in the observation group than those in the negative
control group. In particular, there were significant differences in
the NLR on the 1st and 3rd day after admission between the two
groups (all P<0.05). However, on the 5th day, no significant
difference in NLR was observed. Furthermore, significant
differences in the PLR on the 1st, 3rd and 5rd day after admission
were identified between the two groups (all P<0.05; Fig. 1).
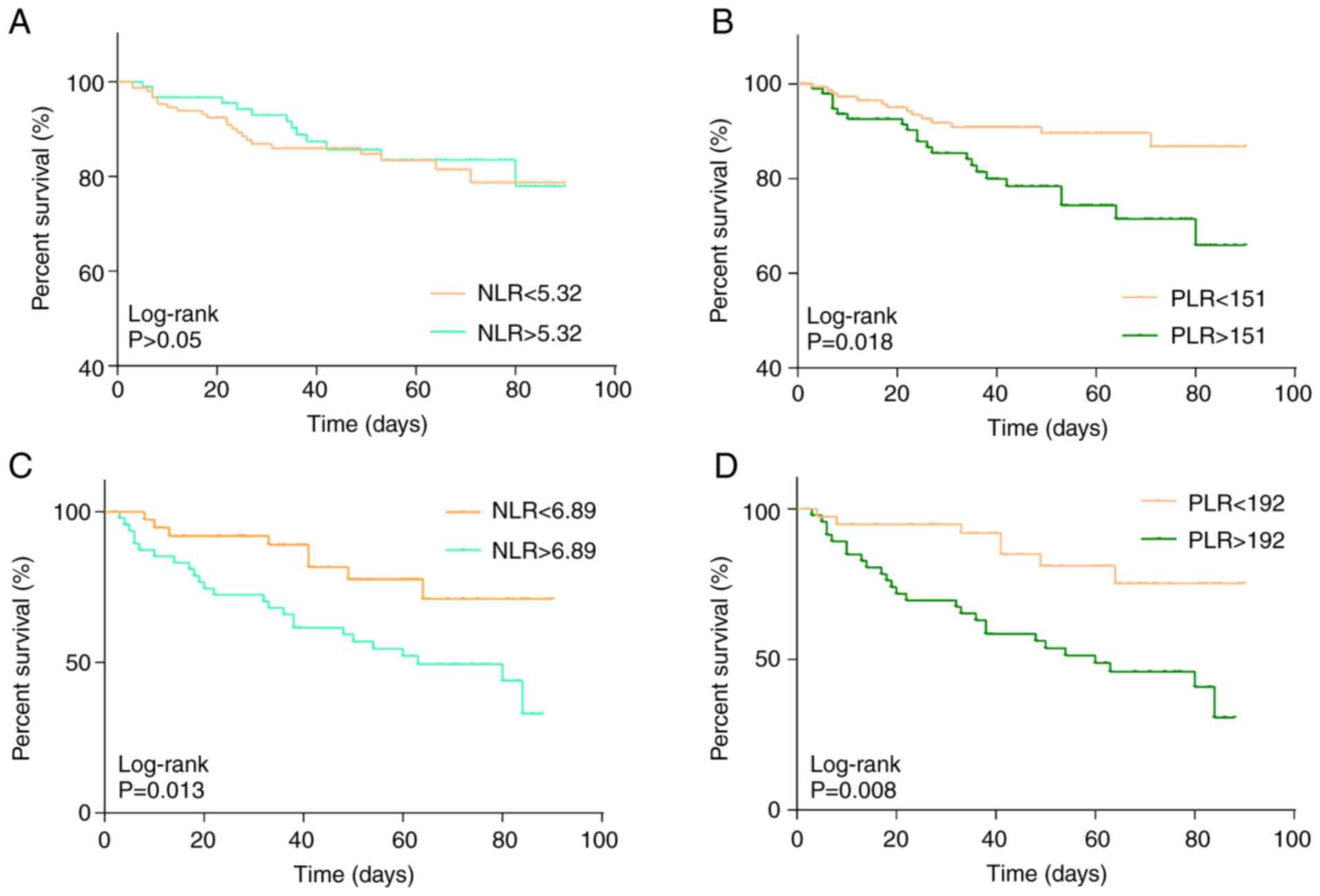
Effects of NLR and PLR on overall
survival
The NLR and PLR of each subject with acute cerebral
hemorrhage were determined on the first day of admission and the
influence of these ratios at baseline on the 90-day survival rate
was assessed. The NLR and PLR in the observation group were
5.32±1.02 and 151.20±6.35, respectively, while they were 6.89±1.93
and 192.76±8.26 in the control group, respectively. Kaplan-Meier
analysis was then performed to assess the effect of an NLR or PLR
above/below the above-mentioned mean values used as a cutoff on
overall survival in each of the two groups over 90 days (Fig. 2). The results indicated that the NLR
and PLR in the observation group were negatively associated with
the overall survival of patients with acute cerebral hemorrhage and
the survival rates of the low NLR or PLR groups were significantly
higher than that of the high NLR or PLR group (P<0.05; Fig. 2C and D). However, no significant
association between NLR and overall survival was observed in the
control group (Fig. 2A). The PLR in
the control group was negatively associated with overall survival
(P<0.05; Fig. 2B).
Multivariate logistic regression
analysis
To determine factors that are independent predictors
of gastrointestinal hemorrhage in patients with acute cerebral
hemorrhage, multivariate logistic regression analysis was
performed. A blood pressure of >180/100 mmHg, cerebral
hemorrhage >30 ml, lower GCS score, hematosepsis and the site of
cerebral hemorrhage were considered as independent variables
(P<0.05; Table II), while
gastrointestinal hemorrhage in patients with acute cerebral
hemorrhage was taken as the dependent variable. The results
suggested that cerebral hemorrhage >30 ml, lower GCS score and
hematosepsis were independent predictors of gastrointestinal
hemorrhage in patients with cerebral hemorrhage (P<0.05;
Table III).
| Table II.Univariate analysis of risk factors of
gastrointestinal hemorrhage in patients with acute cerebral
hemorrhage. |
Table II.
Univariate analysis of risk factors of
gastrointestinal hemorrhage in patients with acute cerebral
hemorrhage.
| Factor | HR | 95% CI | P-value |
|---|
| Sex |
| Male | 1 | Reference |
|
|
Female | 1.13 | 0.91–1.29 | 0.526 |
| Age (years) |
|
<60 | 1 | Reference |
|
|
>60 | 1.18 | 0.87–1.32 | 0.379 |
| Blood pressure
(mmHg) |
|
<180/100 | 1 | Reference |
|
|
>180/100 | 1.33 | 0.92–1.47 | 0.023 |
| Cerebral hemorrhage
(ml) |
|
<30 | 1 | Reference |
|
|
>30 | 1.38 | 1.26–1.49 | 0.004 |
| Location |
|
Brainstem | 1 | Reference |
|
|
Cerebellum | 0.85 | 0.62–1.23 | 0.042 |
| Lobe | 0.76 | 0.56–1.25 | 0.031 |
| Basal
ganglia | 0.89 | 0.65–1.08 | 0.035 |
|
Thalamus | 0.82 | 0.64–1.25 | 0.039 |
| GCS score |
|
>8 | 1 | Reference |
|
|
<8 | 1.43 | 1.28–1.67 | 0.017 |
| Septicemia |
| No | 1 | Reference |
|
|
Yes | 2.87 | 2.52–3.06 | <0.001 |
| Table III.Multivariate logistic regression
analysis of risk factors of gastrointestinal hemorrhage in patients
with acute cerebral hemorrhage. |
Table III.
Multivariate logistic regression
analysis of risk factors of gastrointestinal hemorrhage in patients
with acute cerebral hemorrhage.
| Factor | B | SE | Wald | OR | 95% CI | P-value |
|---|
| Cerebral hemorrhage
>30 ml | 0.879 | 0.336 | 7.235 | 1.268 | 1.004–1.210 | 0.001 |
| GCS score
<8 | 1.874 | 0.635 | 11.736 | 1.392 | 0.120–2.102 | 0.004 |
| Hematosepsis | 1.774 | 0.235 | 13.645 | 3.125 | 1.268–7.495 | 0.007 |
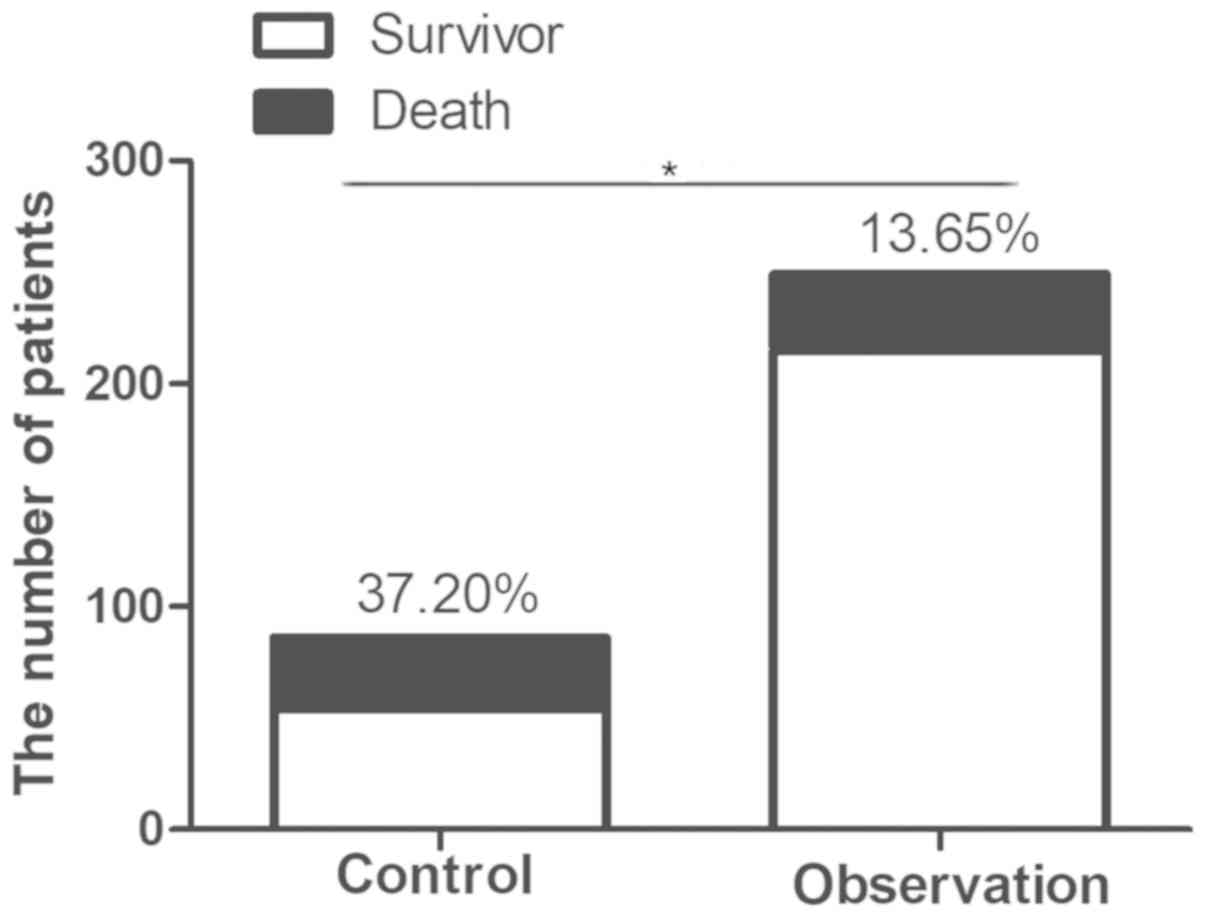
Prognostic analysis
Among the 86 patients with acute cerebral hemorrhage
combined with gastrointestinal hemorrhage, 32 patients died,
resulting in a mortality rate of 37.20%. In the negative control
group without gastrointestinal hemorrhage, 34 mortalities occurred
among the 249 cerebral hemorrhage patients, and the mortality rate
in this group was 13.65%. A significant difference in mortality was
identified between the two groups (P<0.05; Fig. 3).
Discussion
Immune inflammatory response after cerebral
hemorrhage is a complex pathophysiological process, and cerebral
edema and inflammatory reactions are crucial factors in promoting
the disease condition of cerebral hemorrhage. Inflammatory reaction
was previously considered to be the result of a stress response. It
has been reported that the hyperacute inflammatory reaction in
response to cerebral hemorrhage exerts a protective effect on
promoting hemostasis and reducing hematoma expansion (11). A series of pathophysiological
processes have been indicated to be involved in cerebral
hemorrhage. Inflammation around the hematoma has an important
influence on the degree of neurological impairment, which manifests
as aggregation of neutrophils, macrophages or monocytes, and
activation of microglia (12).
Gastrointestinal hemorrhage is a serious
complication of acute stroke and traumatic brain injury. Peptic
ulcers resulting from intracranial lesions are called Cushing
ulcers (13). With the improvement
of clinical diagnosis and treatment, the incidence of
gastrointestinal hemorrhage has markedly decreased (14,15).
Wijdicks et al (15) reported
that the incidence of stroke complicated with gastrointestinal
hemorrhage was 0.80% in stroke patients. Chen et al
(16) determined that 20.5% of
elderly patients with acute stroke experienced gastrointestinal
hemorrhage as a complication.
Previous studies on the prognosis of acute
spontaneous cerebral hemorrhage mainly focused on the association
between the leukocyte count and inflammatory reaction (17). Elevation of WBC in the acute phase of
cerebral hemorrhage has been indicated to be positively associated
with neurological impairment and 3-month mortality. However, the
number of WBC is susceptible to interference from various factors
such as diets, drugs and the endocrine system. Imtiaz et al
(18) demonstrated that lymphocytes
may protect endothelial cells and alleviating the inflammatory
response. Imbalance of neutrophils and lymphocytes exaggerates the
inflammatory response. The NLR is an indicator of the inflammatory
state of the body, with a higher NLR indicating a more severe
inflammatory response. Utilization of the NLR as an indicator of
inflammation has numerous advantages, including easy accessibility
and low cost. Gokhan et al (19) reported that the NEU and NLR in
patients with acute cerebral hemorrhage were higher than those in
controls. They also suggested that NLR was significant for
evaluating the severity of acute cerebral hemorrhage, which was
consistent with the study by Lattanzi et al (20). The NLR and PLR have a higher
sensitivity and reliability for prognosis in patients with cerebral
hemorrhage compared with those of NEU and WBC.
Through these in-depth studies, the association
between PLR and the prognostic significance of cerebrovascular
disease has been recognized. Altintas et al (21) analyzed 57 patients who were treated
by endovascular therapy after acute ischemic stroke. Their results
indicated that the PLR was able to reflect an in vivo
inflammatory state prior to thrombosis. Elevation of PLR was
associated with poor vascular recanalization after treatment with
endovascular therapy and poor prognosis over 3 months. Tao et
al (22) analyzed the
pre-operative routine blood test results of 247 patients with
subarachnoid hemorrhage and revealed that an elevated PLR was
associated with neurological impairment within 90 days after the
onset of subarachnoid hemorrhage.
Based on the previous studies, it may be speculated
that the NLR and PLR are associated with cerebral hemorrhage
combined with gastrointestinal hemorrhage. In the present study,
patients were assigned to an observation group and a negative
control group depending on whether they experienced
gastrointestinal hemorrhage after cerebral hemorrhage. It was
revealed that the NLR and PLR in the observation group were higher
than those in the control group. The occurrence time of
gastrointestinal hemorrhage is generally 1–2 weeks after acute
cerebral hemorrhage (16).
Similarly, the occurrence time of gastrointestinal hemorrhage in
the observation group of the present study was 1–2 weeks after
cerebral hemorrhage. Since the blood was collected on the 1st, 3rd
and 5th days of hospitalization, it may be speculated that the
elevation of NLR and PLR is involved in the occurrence of
gastrointestinal hemorrhage. The NLR and PLR in the observation
group were negatively associated with overall survival, whereas
only the PLR in the negative control group was identified to be
negatively associated with overall survival. The present results
were similar to those of previous studies (19,20,22).
Future studies by our group, we will aim at further investigating
the association between the NLR and PLR and mortality in the two
groups. Furthermore, logistic regression analysis indicated that
cerebral hemorrhage >30 ml, lower GCS score and hematosepsis
were independent risk factors of gastrointestinal hemorrhage in
patients with acute cerebral hemorrhage. Therefore,
gastrointestinal hemorrhage should be closely monitored in patients
with cerebral hemorrhage, particularly in those with the above risk
factors. The present results provide further information for the
prediction of gastrointestinal hemorrhage after acute cerebral
hemorrhage, which may have important significance for the timely
diagnosis and treatment of cerebral hemorrhage combined with
gastrointestinal hemorrhage. However, the present study was
retrospective and the sample size was relatively small. In the
future, more samples should be included and multicenter randomized
controlled trials should be performed to validate the conclusions
of the present study.
In conclusion, elevations of the NLR and PLR were
associated with gastrointestinal hemorrhage in patients with acute
cerebral hemorrhage. A higher NLR and PLR were negatively
associated with overall survival and prognosis. Furthermore,
cerebral hemorrhage >30 ml, lower GCS score and hematosepsis
were independent risk factors of gastrointestinal hemorrhage in
patients with acute cerebral hemorrhage.
Acknowledgements
Not applicable.
Funding
The current study was supported by Suzhou Science
and Education Xingwei Youth Science and Technology Project (grant
no. KJXW2017075), Nantong University-level Natural Science Research
Fund Project (grant no. 17ZYZ34) and Wujiang First People's
Hospital Research Fund Project (grant nos. hospital201708 and
hospital201907).
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
YZo and YZh designed the study and performed the
experiments. YZo, WZ and CH collected the data, WZ and CH analyzed
the data, and YZo and YZh prepared the manuscript. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the ethics committee of
the First People's Hospital of Wujiang District (Suzhou, China).
Written informed consent was obtained from all participants prior
to the study.
Patient consent for publication
The patients or their guardians provided written
informed consent for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Santoni M, Andrikou K, Sotte V, Bittoni A,
Lanese A, Pellei C, Piva F, Conti A, Nabissi M, Santoni G and
Cascinu S: Toll like receptors and pancreatic diseases: From a
pathogenetic mechanism to a therapeutic target. Cancer Treat Rev.
41:569–576. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
O'Neill LA: The interleukin-1
receptor/Toll-like receptor superfamily: 10 years of progress.
Immunol Rev. 226:10–18. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kawai T and Akira S: The role of
pattern-recognition receptors in innate immunity: Update on
toll-like receptors. Nat Immunol. 11:373–384. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kong Y and Le Y: Toll-like receptors in
inflammation of the central nervous system. Int Immunopharmacol.
11:1407–1414. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Abdi J, Engels F, Garssen J and Redegeld
F: The role of toll-like receptor mediated signalling in the
pathogenesis of multiple myeloma. Crit Rev Oncol Hematol.
80:225–240. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hammond MD, Taylor RA, Mullen MT, Ai Y,
Aguila HL, Mack M, Kasner SE, McCullough LD and Sansing LH:
CCR2+ Ly6C(hi) inflammatory monocyte recruitment
exacerbates acute disability following intracerebral hemorrhage. J
Neurosci. 34:3901–3909. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang J and Dore S: Inflammation after
intracerebral hemorrhage. J Cereb Blood Flow Metab. 27:894–908.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Atkinson JJ and Senior RM: Matrix
metalloproteinase-9 in lung remodeling. Am J Respir Cell Mol Biol.
28:12–24. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tian XC, Liu XL, Zeng FR, Chen Z and Wu
DH: Platelet-to-lymphocyte ratio acts as an independent risk factor
for patients with hepatitis B virus-related hepatocellular
carcinoma who received transarterial chemoembolization. Eur Rev Med
Pharmacol Sci. 20:2302–2309. 2016.PubMed/NCBI
|
|
10
|
Suppiah A, Malde D, Arab T, Hamed M,
Allgar V, Smith AM and Morris-Stiff G: The prognostic value of the
neutrophil-lymphocyte ratio (NLR) in acute pancreatitis:
Identification of an optimal NLR. J Gastrointest Surg. 17:675–681.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Morotti A, Phuah CL, Anderson CD, Jessel
MJ, Schwab K, Ayres AM, Pezzini A, Padovani A, Gurol ME,
Viswanathan A, et al: Leukocyte count and intracerebral hemorrhage
expansion. Stroke. 47:1473–1478. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gong C, Hoff JT and Keep RF: Acute
inflammatory reaction following experimental intracerebral
hemorrhage in rat. Brain Res. 871:57–65. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wijdicks EF: Cushing's ulcer: The eponym
and his own. Neurosurgery. 68:1695–1698. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Crooks CJ, Card TR and West J: Excess
long-term mortality following non-variceal upper gastrointestinal
bleeding: A population-based cohort study. PLoS Med.
10:e10014372013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wijdicks EF, Fulgham JR and Batts KP:
Gastrointestinal bleeding in stroke. Stroke. 25:2146–2148. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chen CM, Hsu HC, Chuang YW, Chang CH, Lin
CH and Hong CZ: Study on factors affecting the occurrence of upper
gastrointestinal bleeding in elderly acute stroke patients
undergoing rehabilitation. J Nutr Health Aging. 15:632–636. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Agnihotri S, Czap A, Staff I, Fortunato G
and McCullough LD: Peripheral leukocyte counts and outcomes after
intracerebral hemorrhage. J Neuroinflammation. 8:1602011.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Imtiaz F, Shafique K, Mirza SS, Ayoob Z,
Vart P and Rao S: Neutrophil lymphocyte ratio as a measure of
systemic inflammation in prevalent chronic diseases in asian
population. Int Arch Med. 5:22012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gokhan S, Ozhasenekler A, Mansur DH, Akil
E, Ustundag M and Orak M: Neutrophil lymphocyte ratios in stroke
subtypes and transient ischemic attack. Eur Rev Med Pharmacol Sci.
17:653–657. 2013.PubMed/NCBI
|
|
20
|
Lattanzi S, Cagnetti C, Provinciali L and
Silvestrini M: Neutrophil-to-lymphocyte ratio predicts the outcome
of acute intracerebral hemorrhage. Stroke. 47:1654–1657. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Altintas O, Altintas MO, Tasal A,
Kucukdagli OT and Asil T: The relationship of
platelet-to-lymphocyte ratio with clinical outcome and final
infarct core in acute ischemic stroke patients who have undergone
endovascular therapy. Neurol Res. 38:759–765. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tao C, Wang J, Hu X, Ma J, Li H and You C:
Clinical value of neutrophil to lymphocyte and platelet to
lymphocyte ratio after aneurysmal subarachnoid hemorrhage.
Neurocrit Care. 26:393–401. 2017. View Article : Google Scholar : PubMed/NCBI
|