Introduction
Human personality and its connections to various
somatic disorders represents a research subject that has recently
been drawing attention and is a reoccurring theme in many clinical
trials. The skin is closely related to the mind and is considered
as the ‘organ of expression’ of the human body. However, this
correlation can be thought of in a different way as well; through
its visibility, any major lesion from the skin can bring emotional,
psychological and/or social changes. We mention the association
between anxiety or depression and acne vulgaris, psoriasis
or bullous pemphigoid (1,2), the link between lifestyle factors and
atopic dermatitis (3) or the
association between stress hormones and cutaneous
pathophysiological processes, such as melanoma (4–6). In
addition, at molecular level, high levels of oxidative stress
parameters were found in psoriasis (7).
Thus, a new concept, psychodermatology, is a concept
that focuses on the diagnosis and treatment of psychiatric
disorders associated with cutaneous manifestations, as well as
combating social isolation associated with such disorders (8).
Health is defined as the state of complete physical,
mental and social well-being, not just the absence of disease or
infirmity (World Health Organization 2006, www.who.int). Thus, health is linked to the quality of
life and is referred to as ‘health-related quality of life (HRQL)’.
It is an increasingly common term used in clinical practice to
assess the impact of various illnesses on patients' quality of
life.
According to the American Psychiatric Association
(www.psychiatry.org), personality
disorders define those types of mental disorders in which thinking,
feeling and behavior follow a rigid, unhealthy pattern, deviated
from the cultural norms of society.
One of the personality traits, neuroticism, appears
to be correlated with a wide range of cardiovascular events, such
as higher levels of blood pressure or atherosclerosis (9). Even more, the British Health and
Lifestyle Survey concluded that neuroticism is associated with a
higher mortality risk in coronary heart diseases (10).
An interesting report utilizing the General Practice
Research Database found that risk factors for CVD occurred more
frequently in psoriasis patients compared with the general
population (11). Because
cardiovascular disease (specifically hypertension and heart
failure) and skin diseases (psoriasis) are associated with
psychological changes (12), we
hypothesize that HRQL in those patients is influenced by some
characteristics of personality. The aim of this study was to
investigate if personality traits may add some differences between
the two groups and influence the course of the diseases.
Patients and methods
Participants
This was a cross-sectional and comparative study,
performed among patients attending their scheduled follow-up visit
to the psoriasis care unit and cardiovascular unit at Iași
University Hospital (Iași, Romania). The present study was approved
by the Clinical Research Ethics Committee of The Clinical Emergency
County Hospital ‘Sf. Spiridon’ (Iași, Romania) and the Ethics
Committee of University of Medicine and Pharmacy ‘Gr. T. Popa’
(Iași, Romania). Written informed consent was obtained from each
patient prior to publication. The participation in the study was
voluntary. The patients (n=63): 35 patients with psoriasis (PSO
group) and 28 patients with cardiovascular diseases (CV group) were
enrolled from March 2017 to December 2017; they provided their
written informed consent to participate in this study. Regarding
the procedure to collect data, simple random sampling technique was
used to select the participants. They were informed about the
purpose of the study and also that their responses will be used in
a scientific study. The tests were performed in a separate room and
the inclusion criteria were: a diagnosis of moderate to severe
plaque-type psoriasis/hypertension or cardiac failure for at least
one year and an age of over 18 years.
The exclusion criteria consisted of the diagnosis of
other important diseases (neoplasia, psychiatric disorders),
pregnancy, lactating women, under 18 years of age. In addition, for
the PSO group, any systemic treatment and any cardiovascular
diseases constituted further exclusion criteria. No patients with
the inability to understand the questions in the questionnaire were
included. In total, 66 patients were excluded, 44 due to exclusion
criteria, 20 who refused to participate and 2 due to incomplete
data from questionnaires.
Measures
The SF-36 questionnaire, developed by New England
Medical Center in the Medical Outcomes Study, contains 36 items
that assess the physical and mental health of the subject. This
questionnaire has been used, so far, to evaluate HRQL in patients
diagnosed with glaucoma, asthma, chronic obstructive
bronchopneumonia, allergic rhinitis, spinal trauma, morbid obesity
and psoriasis. SF-36 improves the information obtained from the
questionnaires referring strictly to the medical condition and
offers a wider perspective on the impact of a certain disease on
the quality of life (13–16).
The Eysenck test contains questions on how the
patient acts, behaves or experiences certain feelings. Thus, this
test can detect the patient's ability to respond truthfully,
highlighting as well his/her tendency to be introverted or
extroverted. The Eysenck test was used in clinical trials that
highlighted neurotic changes, but it was also used in detecting
changes in personality in dermatological conditions, such as
acne vulgaris, as well as in other conditions, including
insomnia or coronary artery disease (17–19).
Because temperament and personality traits have both
universal and regional characteristics, we have also chosen to use
the questionnaire of the Profile of Emotional Distress (PED), a
specific tool designed for the Romanian population (20). This questionnaire was designed to
assess the subjective dimension of functional negative emotions,
dysfunctional negative emotions and positive emotions. The basic
idea of this model is that at the root of emotional and behavioral
problems there are dysfunctional and irrational beliefs about
oneself, the world and life. The scale includes 39 items and allows
the calculation of a general distress score, a negative emotion
score, a positive emotion score, and scores for ‘worry’, ‘anxiety’
and ‘depression’ (dysfunctional). In this study, we calculated the
general score of distress and the score of dysfunctional negative
emotions.
Statistical analysis
Data was loaded and processed using statistical
functions in SPSS 18.0 (PASW statistics). The Skewness/Kurtosis
test (>-2 P-value <2) was utilized to test the normality of
the set of values used to examine a continuous variable. The ANOVA
test was used to analyze the dispersion of the dependent variable,
intra- and intergroup. After applying the ANOVA test, Bonferroni
(post-hoc Bonferroni) correction was performed. This correction
reduces the type I error rate when testing multiple hypotheses.
When calculating the significant difference between two or more
groups, based on the distribution of the value series, the
significance threshold of 95% was applied to the quantitative
tests: Student's t-test, paired samples t-test and Chi-square test.
In addition, the Kruskall-Wallis test was used to compare ordinal
variables from three or more groups, but it was used for
specific/predictive balance plotting at the ROC curve, which served
as a prognostic factor. P<0.05 was considered to indicate a
statistically significant difference.
Results
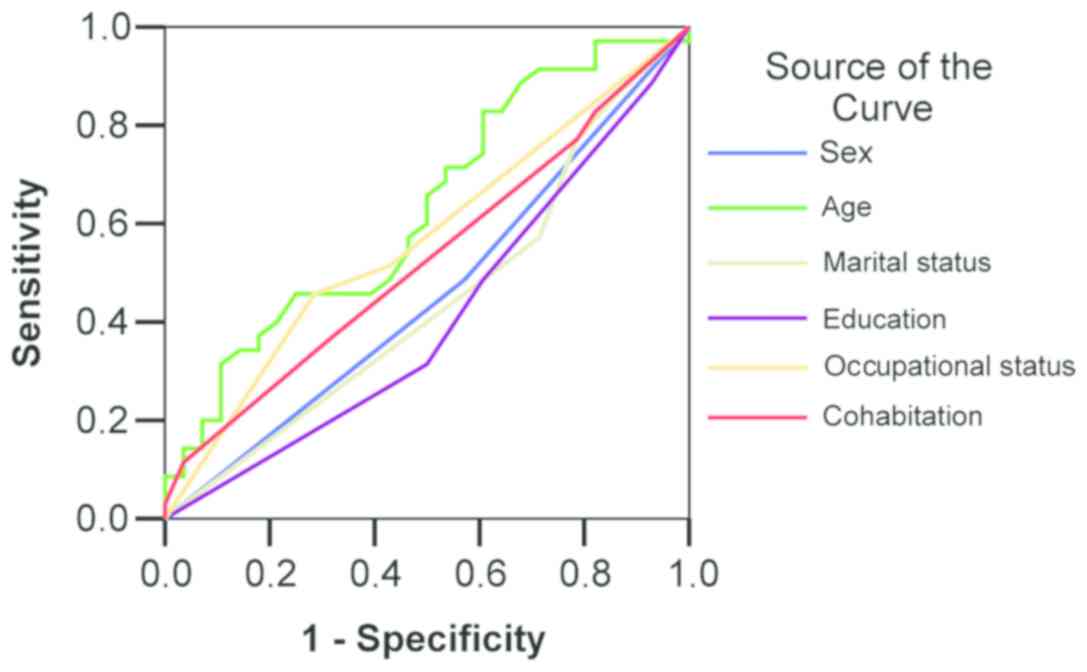
The age of the patients varied from 18 to 86 years,
the mean was 53.95±16.30 years. In both study groups there was a
high educational status (31.4% in the PSO group vs. 50% in the CV
group) without significant difference (P=0.488). The dominant
occupational status in both study groups was that of an employee
(48.6% in the PSO group vs. 57.1% in the CV group, P=0.266). ROC
curve confirmed that the socio-demografic characteristics are not a
predictive method of evaluating the quality diagnostic in patients
with psoriasis in comparison with control group (Fig. 1).
The SF-36 values, which represent physical functions
on a scale from 0 to 100, had no significant difference in the mean
scores of the study groups (42.43 in the PSO group vs. 38.04 in the
CV group, P=0.557). This indicates that physical functions were
reduced in both groups. In a comparative study of mean scores of
SF-36, limited physical health did not reveal significant
differences (56.98 in the PSO group vs. 55.16 in the CV group,
P=0.332). Approximately 43% of the patients with psoriasis and 45%
of those with cardiovascular disease had limitations in daily
physical function caused by their physical health status.
In comparing the mean scores of SF-36, a limitation
due to emotional problems did not reveal significant differences
(74.29 in the PSO group vs. 83.93 in the CV group; P=0.079). In
approximately 25% of the patients with psoriasis and 16% of those
with cardiovascular disease, emotional problems had led to
limitations in physical activity.
The energy/fatigue range recorded a slightly higher
average score in patients with psoriasis (63.43 in the PSO group
vs. 59.64 in the CV group, P=0.281), yet 37%-40% of the patients in
the two study groups reported a decrease in vitality due to health
problems.
In comparison, the mean scores of SF-36 show that
social functions revealed significant differences (75.71 in the PSO
group vs. 86.16 in the CV group, P=0.05). In approximately 24% of
the patients with psoriasis and 14% of those with cardiovascular
disease, the way they perceived their health during the previous
month greatly impacted social interactions. In approximately 40% of
the patients in both study groups, the pain recorded in the last 4
weeks reduced the quality of life (60.86 in the PSO group vs. 60 in
the CV group, P=0.872).
Regarding personality traits in psoriasis, for
patients with an introvert personality the average scores of
physical functions and limitations brought on by emotional problems
were significantly higher according to the Eysenck questionnaire
scores (Table I).
 | Table I.Association between of the quality of
life and neuroticism. |
Table I.
Association between of the quality of
life and neuroticism.
|
| PSO group | CV group |
|---|
|
|
|
|
|---|
| Domain SF-36 | Emotionally
stable | Neuroticism | P-value | Emotionally
stable | Neuroticism | P-value |
|---|
| S1. Physical
functions | 33.95±28.80 | 52.50±31.73 | 0.079 | 39.09±33.82 | 37.35±22.30 | 0.871 |
| S2. Limitations due
to physical health | 55.07±7.66 | 59.26±7.50 | 0.113 | 55.05±8.12 | 55.23±5.45 | 0.945 |
| S3. Limitations due
to emotional problems | 65.79±21.85 | 84.38±20.61 |
0.015a | 72.73±17.12 | 91.18±16.79 |
0.009a |
| S4. Vitality | 66.84±15.29 | 59.38±12.89 | 0.132 | 66.36±8.09 | 55.29±13.28 |
0.020a |
| S5. Emotional
stability | 54.21±10,04 | 54.69±11.03 | 0.894 | 55.91±10.20 | 54.41±8.08 | 0.669 |
| S6. Social
functions | 66.45±22.07 | 86.72±21.15 |
0.009a | 76.14±19.73 | 92.65±17.15 |
0.027a |
| S7. Pain | 72.63±19.10 | 46.88±17.78 |
0.001a | 25.01±7.54 | 13.48±3.27 | 0.417 |
| S8. Perception of
general health status | 65.26±12.64 | 65.00±10.95 | 0.948 | 61.82±7.51 | 57.65±9.70 | 0.238 |
| Total score | 71.81±3.72 | 74.33±5.13 | 0.101 | 72.39±4.71 | 72.28±3.14 | 0.939 |
| Right regression
model | y=0.723–0.005
S1+0.021 | 0.701 | y=−2.991+0.004
S1+0.021 |
0.011a |
|
| S2-0.012
S3+0.005 |
| S2-0.005
S3+0.008 |
|
|
| S4-0.010
S5+0.008 |
| S4+0.008
S5-0.006 |
|
|
| S6-0.001 S7+0.006
S8 |
| S6+0.008 S7+0.049
S8 |
|
In cardiovascular patients with introvert
personality, the mean scores of limitation domains due to emotional
problems and social functions were significantly higher (Table I).
In patients with extrovert personality, the mean
scores in the vitality domain and the perception of their general
condition were significantly higher (Table I).
In patients with psoriasis, who were also
emotionally stable, the mean pain level was significantly higher.
In patients with cardiovascular disease who were also emotionally
stable, the mean vitality scores were significantly higher
(Table I).
P-values for Student's t-test for PSO vs. CV groups:
i) P<0.001; ii) P<0.01 iii) P<0.05 no significant data
were collected.
In patients with psoriasis and high or very high
grade of dysfunctional negative emotions, the mean scores in the
physical function domain were greater (18 and 39.62 vs. 57.86 and
65; P=0.023) and limitations due to emotional problems (53.33 and
67.95 vs. 90.48 and 83.33; P=0.002) were significantly higher. The
mean pain level was significantly higher in patients with low or
average dysfunctional negative emotions (72 vs. 65.38; 50 and 40;
P=0.042) (Table II).
| Table II.Association between the quality of
life and dysfunctional negative emotions in two study groups. |
Table II.
Association between the quality of
life and dysfunctional negative emotions in two study groups.
|
| PSO group | CV group |
|
|---|
|
|
|
|
|
|---|
| Domain SF-36 | Low | Medium | Higher | Very high | P-value | Low | Medium | High | Very high | P-value | F ANOVA test PSO
vs. CV |
|---|
| S1 | 18.00 | 39.62 | 57.86 | 65.00 | 0.023a | 10.00 | 44.00 | 42.89 | 0.00 | 0.016a | F=0.349
P=0.557 |
| S2 | 50.37 | 57.69 | 58.33 | 66.67 | 0.207 | 50.00 | 55.19 | 55.26 | 68.52 | 0.096 | F=3.515
P=0.066 |
| S3 | 53.33 | 67.95 | 90.48 | 83.33 | 0.002a | 66.67 | 80.00 | 89.47 | 50.00 | 0.046a | F=0.026
P=0.872 |
| S4 | 68.00 | 66.92 | 55.71 | 60.00 | 0.035a | 63.33 | 66.00 | 56.32 | 80.00 | 0.137 | F=3.745
P=0.133 |
| S5 | 56.00 | 54.62 | 54.29 | 60.00 | 0.875 | 53.33 | 56.00 | 54.47 | 65.00 | 0.700 | F=1.184
P=0.281 |
| S6 | 57.50 | 73.08 | 86.61 | 100.0 | 0.038 | 66.67 | 82.50 | 53.68 | 80.00 | 0.030a | F=3.188
P=0.079 |
| S7 | 72.00 | 65.38 | 50.00 | 40.00 | 0.042 | 83.33 | 80.00 | 66.00 | 53.68 | 0.026a | F=0.993
P=0.323 |
| S8 | 78.00 | 64.62 | 62.14 | 60.00 | 0.101 | 63.33 | 64.00 | 57.89 | 50.00 | 0.334 | F=0.054
P=0.817 |
| Global score | 69.26 | 72.97 | 74.57 | 77.78 | 0.076 | 68.52 | 73.52 | 72.61 | 72.22 | 0.307 | F=0.362
P=0.550 |
In patients with psoriasis and low or medium grade
dysfunctional negative emotions, the mean scores of vitality (68
and 66.92 vs. 55.71 and 60; P=0.035) and pain (72 and 65.38 vs. 50
and 40; P=0.042) were significantly higher (Table II).
In patients with cardiovascular problems, the
following statistically significant differences in mean values of
SF-36 scores were noted, in terms of dysfunctional negative
emotions: physical functions associated with an average emotional
level (10 and 44 vs. 42.9 and 42.89; P=0.016), limitations due to
emotional problems associated with a level of medium-high
dysfunctional negative emotions (66.67 and 80 vs. 89.47 and 50;
P=0.046), social functions associated with an average or high
emotional level (66.67 and 82.50 vs. 53.68 and 80; P=0.039) and
pain associated with a level of low dysfunctional negative emotions
toward the environment (83.33 and 80 vs. 66 and 63.68; P=0.026)
(Table II).
In patients with psoriasis, introversion and
neuroticism have been associated with a high (71.4%) and very high
level (100%) of dysfunctional negative emotions (P=0.023) (Table III).
| Table III.Association between dysfunctional
negative emotions and PED scores (introversion, extroversion,
neuroticism). |
Table III.
Association between dysfunctional
negative emotions and PED scores (introversion, extroversion,
neuroticism).
|
| Dysfunctional
negative emotions |
|
|---|
|
|
|
|
|---|
|
| PSO group | CV group |
|
|---|
| PDA | Low (%) | Medium (%) | High (%) | Very high (%) | Low (%) | Medium (%) | High (%) | Very high (%) | P-values for
Kruskal-Wallis test PSO vs. CV |
|---|
| Introversion | 80.0 | 15.4 | 71.4 | 100.0 | 0.0 | 0.0 | 52.6 | 0.0 | 0.001b |
| Ambivert | 20.0 | 76.9 | 21.4 | 0.0 | 100.0 | 60.0 | 47.4 | 100.0 | 0.001b |
| Extroversion | 0.0 | 7.7 | 7.1 | 0.0 | 0.0 | 40.0 | 0.0 | 0.0 | 0.423 |
|
P-valuea |
| 0.023b |
|
| 0.014b |
|
|
| Emotionally
stable | 100.0 | 53.8 | 35.7 | 0.0 | 66.7 | 80.0 | 26.3 | 0.0 | 0.713 |
| Neuroticism | 0.0 | 46.2 | 64.3 | 100.0 | 33.3 | 20.0 | 73.7 | 100.0 | 0.075 |
|
P-valuea |
| 0.005b |
|
| 0.031b |
|
|
Of the patients with psoriasis 59.1% had high levels
of distress presenting neurotic features.
Eysenck test
The ability to manipulate responses was noted in
31.7% of the subjects, slightly more frequent in the group of
patients with psoriasis (40% PSO group vs. 21.4% CV group, P=0.272)
and there was no significant sex difference in the study groups who
were inclined to lie or conceal the truth.
Approximately 60% of single patients with psoriasis
have the ability to manipulate the responses while 75% of patients
with cardiovascular disease have reserved responses (P=0.05).
Comparing the two study groups, the responses marked in the lie
domain are not significantly associated with educational
status.
Furthermore, 40% of single patients with psoriasis
and 50% of patients with cardiovascular diseases were introvert,
85.4% of widowed patients with psoriasis and 50% of cardiovascular
patients were introvert and no extravert personality types were
noted among widowed patients (P=0.312).
Neuroticism was noted in 52.4% of the subjects,
slightly more frequent in the group of patients with cardiovascular
disease (60.7% in the CV group vs. 45.7% in the PED group,
P=0.235). Moreover, all patients with elementary education, no
matter which study group they were a part of, presented elements of
neuroticism.
Affective distress profile
Sadness/depression
Functional PDA scores ranged from 6 to 28,
registering a slightly higher average in patients with
cardiovascular disease (16.07 in the CV group vs. 13.60 in the PSO
group, P=0.057), while the functional PDA score varied from 8 to
31, registering a significantly higher mean in patients with
cardiovascular disease (17.86 in the CV group vs. 14.40 in the PSO
group, P=0.024).
Concern/Anxiety
Functional PDA score ranged from 8 to 28, recording
a significantly higher mean in patients with cardiovascular disease
(19.04 in the CV group vs. 15.80 in the PSO group, P=0.016) and the
functional PDA score ranged from 6 to 36, also registering a
significantly higher mean in patients with cardiovascular disease
(14.0 in the CV group vs. 11.60 in the PSO group, P=0.039).
Patients with psoriasis are experiencing less
dysfunctional emotions than patients with cardiovascular disease.
This is associated with a higher level of distress experienced by
patients with cardiovascular disease compared to patients with
psoriasis, as shown by the results below:
i) Functional negative emotions: In the psoriasis
group, 37.1% of the patients had an average level of functional
negative emotions and 37.2% were high and very high, while in the
group with cardiovascular disease, 60.7% of patients had high and
very high levels of functional negative emotions (P=0.011) and ii)
dysfunctional negative emotions: In the psoriasis group, 40% of the
patients had a high level of dysfunctional negative emotions and
37.1% had a medium level of dysfunctional negative emotions, while
in the group with cardiovascular disease, 67.9% of the patients had
a high level of dysfunctional negative emotions (P=0.045).
Positive emotions
The PDA score for positive emotions ranged from 19
to 58, showing a slightly higher average in patients with psoriasis
(37.66 in the PSO group vs. 36.43 in the CV group, P=0.615).
Total PDA
The total PDA score ranged from 61 to 139, with a
significantly higher mean in cardiovascular patients (103.39 in the
CV group vs. 93.06 in the PSO group, P=0.008).
The overall PDA score in 73% of patients was very
high with a significantly higher percentage in patients with
cardiovascular disease (85.7% in the CV group vs. 62.9% in the PSO
group, P=0.039).
Discussion
The main findings of the present study are: i)
Regarding personality traits, neuroticism was present in all
patients with elementary education, regardless of the study group
they were in and anxiety was associated with a low level of
education as well and ii) regarding HRQL, in the PSO group, we
noted a greater impact of diagnosis on social interactions. In
approximately 40% of the patients in both study groups, pain
recorded in the last 4 weeks reduced the quality of life and daily
physical functions were reduced by physical health in approximately
40% in both groups.
The role of stress in modulation of skin
inflammation, the quality of life in patients with psoriasis and
the psychological changes associated with this condition have been
extensively studied and the results have shown differences in
ethnicity, sex or other stress factors (smoking) (21–23). The
severity of the disease or its duration is not of the utmost
importance, but rather the social impact of the lesions. If the
lesions are located in visible areas, they have a greater effect on
the quality of life of the patient, even if their size is small
(24,25). Most studies used an HRQL assessment
method in psoriasis patients with the Dermatology Quality of Life
Index (DLQI) questionnaire in association with the Psoriasis Area
Severity Index (26–28). However, it has been observed that
there is no direct link to the severity of lesional extension,
which is mainly assessed by PASI and the degree of psychological
impairment of the patient (25). The
correlation of PASI with HRQL differs greatly depending on the
patient's temperament (29).
Emotion regulation is a process by which emotions
are modulated both consciously and unconsciously (30) and depression is frequently considered
a disorder that occurs because of a dysfunction of emotion
regulation strategies (31). Our
results show that patients with psoriasis experience a lower degree
of dysfunctional emotions than patients with cardiovascular
disease. It could be interpreted as an association with a higher
level of distress experienced by patients with cardiovascular
disease in a strict relation with their disease.
These ideas highlight the fact that the psychic
component plays a much more important role than previously thought
and its importance should be reevaluated; our results support this
idea. In our case, the patient's health in the month prior to
assessment prevented social engagement. Furthermore, in
approximately 40% of the patients in both study groups, pain
reduced quality of life over the last 4 weeks.
Patients with psoriasis and introverted personality
tend to limit physical activity and are more emotionally
vulnerable, which may exacerbate the effects of the disease and
therapeutic compliance or even aggravation of the symptoms. It is
precisely because of the patient's personality structure, quality
of life and emotional stability that there is a need for additional
psychological support in these patients.
Our result revealed elements of neuroticism in all
patients with psoriasis who had elementary studies, while in those
with higher education only 45.5% presented high scores on
neuroticism. We found that anxiety was associated with a low level
of education and similar conclusions have also been drawn in
studies from other countries (32).
We can consider that emotional instability may
constitute a personality trait and is common for both patients with
psoriasis and patients with cardiovascular disease; a personality
trait that is found in personality type A, but also personality
type D.
We believe that it is necessary to include items
evaluating the patients' affective profile in the assessment
protocols of these diseases, since that could help the clinician in
identifying possible factors that signal worsening of the disease
or of non-response to treatment.
This study used three different tests, which made
comparing the results more difficult. Since testing has only been
done once, the perception of quality of life, affective perception
of the patient may change over the course of the disease and the
treatment. Last, but not least, self-administered testing can
influence the test results due to the desire to impress the tester
or other patients. Considering that psoriasis is a chronic
condition accompanied by exacerbations and remissions, it is also
necessary to evaluate patients at the time of maximum symptoms.
In conclusion, the present study shows interesting
relations between personality traits, such as emotion instability
or neuroticism, and physical problems; also in addition, it shows
an association between these diseases and the quality of life.
Acknowledgements
The authors are grateful to Radu Iliescu, the senior
scientist who made valuable suggestions for improvements to the
manuscript. Professional editing, linguistic and technical
assistance performed by Individual Service Provider Irina Radu,
certified translator in Medicine and Pharmacy.
Funding
Article in the project ‘Cardiovascular risk
assessment protocol in patients with psoriasis’ (PSOCARDIO), funded
by Romanian Society of Dermatology and Venereology.
Availability of data and materials
All data and materials supporting the results of the
present study are available in the published article.
Authors' contributions
All authors contributed to the acquisition of the
data and critical revision of manuscript for important intellectual
content. EPA, LGS were responsible for the research design,
manuscript drafting, analysis and interpretation of data. DV was
responsible for language editing and RP for interpretation of the
questionnaires. LS, CS, AIG, AIP, IAP have shared questionnaires
and statically processed the results. DV contributed to the data
analysis and the critical interpretation. LGS has critically
reviewed the manuscript. All authors read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Clinical
Research Ethics Committee of The Clinical Emergency County Hospital
‘Sf. Spiridon’ (Iași, Romania) and the Ethics Committee of
University of Medicine and Pharmacy ‘Gr. T. Popa’ (Iași, Romania).
Written informed consent was obtained from each patient prior to
publication.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lowe JG: The stigma of acne. Br J Hosp
Med. 49:809–812. 1993.PubMed/NCBI
|
|
2
|
Kouris A, Platsidaki E, Christodoulou C,
Armyra K, Korkoliakou P, Stefanaki C, Tsatovidou R, Rigopoulos D
and Kontochristopoulos G: Quality of life, depression, anxiety and
loneliness in patients with bullous pemphigoid. A case control
study. An Bras Dermatol. 91:601–603. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Solomon I, Ilie MA, Draghici C, Voiculescu
VM, Căruntu C, Boda D and Zurac S: The impact of lifestyle factors
on evolution of atopic dermatitis: An alternative approach. Exp
Ther Med. 17:1078–1084. 2019.PubMed/NCBI
|
|
4
|
Caruntu C, Boda D, Constantin C, Caruntu A
and Neagu M: Catecholamines increase in vitro proliferation of
murine B16F10 melanoma cells. Acta Endo. 10:545–558. 2014.
View Article : Google Scholar
|
|
5
|
Căruntu C, Boda D, Musat S, Căruntu A and
Mandache E: Stress-induced mast cell activation in glabrous and
hairy skin. Mediators Inflamm. 2014:1059502014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Caruntu C, Boda D, Musat S, Caruntu A,
Poenaru E, Calenic B, Savulescu-Fiedler I and Draghia A: Rotaru M
and Badarau AI: Stress effects on cutaneous nociceptive nerve
fibers and their neurons of origin in rats. Rom Biotechnol Lett.
19:9517–9530. 2014.
|
|
7
|
Boda D, Negrei C, Nicolescu F and Balalau
C: Assessment of some oxidative stress parameters in methotrexate
treated psoriasis patients. Farmacia. 62:704–710. 2014.
|
|
8
|
Jafferany M and Franca K:
Psychodermatology: Basics concepts. Acta Derm Venereol. 96:35–37.
2016.PubMed/NCBI
|
|
9
|
Jylhä P and Isometsä E: The relationship
of neuroticism and extraversion to symptoms of anxiety and
depression in the general population. Depress Anxiety. 23:281–289.
2006. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shipley BA, Weiss A, Der G, Taylor MD and
Deary IJ: Neuroticism, extraversion, and mortality in the UK Health
and Lifestyle Survey: A 21-year prospective cohort study. Psychosom
Med. 69:923–931. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kaye JA, Li L and Jick SS: Incidence of
risk factors for myocardial infarction and other vascular diseases
in patients with psoriasis. Br J Dermatol. 159:895–902. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Goyal A, Dey AK, Chaturvedi A, Elnabawi
YA, Aberra TM, Chung JH, Belur AD, Groenendyk JW, Lerman JB, Rivers
JP, et al: Chronic stress-related neural activity associates with
subclinical cardiovascular disease in psoriasis: A prospective
cohort study. JACC Cardiovasc Imaging. Noe 15–2018.(Epub ahead of
print). View Article : Google Scholar
|
|
13
|
Unalan H, Gençosmanoğlu B, Akgün K,
Karamehmetoğlu S, Tuna H, Ones K, Rahimpenah A, Uzun E and Tüzün F:
Quality of life of primary caregivers of spinal cord injury
survivors living in the community: Controlled study with short
form-36 questionnaire. Spinal Cord. 39:318–322. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Doll HA, Petersen SEK and Stewart-Brown
SL: Obesity and physical and emotional well-being: Associations
between body mass index, chronic illness, and the physical and
mental components of the SF-36 questionnaire. Obes Res. 8:160–170.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Leynaert B, Neukirch C, Liard R, Bousquet
J and Neukirch F: Quality of life in allergic rhinitis and asthma.
A population-based study of young adults. Am J Respir Crit Care
Med. 162:1391–1396. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sampogna F, Tabolli S, Söderfeldt B,
Axtelius B, Aparo U and Abeni D; IDI Multipurpose Psoriasis
Research on Vital Experiences (IMPROVE) investigators, : Measuring
quality of life of patients with different clinical types of
psoriasis using the SF-36. Br J Dermatol. 154:844–849. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gül Aİ and Çölgeçen E: Personality traits
and common psychiatric conditions in adult patients with acne
vulgaris. Ann Dermatol. 27:48–52. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bayar N, Güven R, Erkal Z, Akyol KC,
Edebali MI, Küçükseymen S and Arslan Ş: Assessment of the
association between the personality traits of young patients with
acute coronary syndrome and the severity of coronary artery
disease. Turk Kardiyol Dern Ars. 45:514–519. 2017.PubMed/NCBI
|
|
19
|
Liao J, Zhu S, Zhang Q, Wang D and Li X:
Personal characteristics of paradoxical insomnia: A case-control
study. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 42:958–965. 2017.(In
Chinese). PubMed/NCBI
|
|
20
|
Opris D and Macavei B: The profile of
emotional distress; norms for the Romanian population. J Cogn Behav
Psychother. 7:139–157. 2007.
|
|
21
|
Căruntu C, Boda D, Căruntu A, Rotaru M,
Baderca F and Zurac S: In vivo imaging techniques for
psoriatic lesions. Rom J Morphol Embryol. 55 (Suppl):1191–1196.
2014.PubMed/NCBI
|
|
22
|
Grigore O, Mihailescu AI, Solomon I, Boda
D and Caruntu C: Role of stress in modulation of skin neurogenic
inflammation. Exp Ther Med. 17:997–1003. 2019.PubMed/NCBI
|
|
23
|
Ilie MA, Caruntu C, Lixandru D, Tampa M,
Georgescu SR, Constantin MM, Constantin C, Neagu M, Zurac SA and
Boda D: In vivo confocal laser scanning microscopy imaging
of skin inflammation: Clinical applications and research
directions. Exp Ther Med. 17:1004–1011. 2019.PubMed/NCBI
|
|
24
|
Çakmur H and Derviş E: The relationship
between quality of life and the severity of psoriasis in Turkey.
Eur J Dermatol. 25:169–176. 2015.PubMed/NCBI
|
|
25
|
Yang HJ and Yang KC: Impact of psoriasis
on quality of life in Taiwan. Zhonghua Pifuke Yixue Zazhi.
33:146–150. 2015.(In Chinese).
|
|
26
|
Basra MK, Fenech R, Gatt RM, Salek MS and
Finlay AY: The Dermatology Life Quality Index 1994–2007: A
comprehensive review of validation data and clinical results. Br J
Dermatol. 159:997–1035. 2008.PubMed/NCBI
|
|
27
|
Revicki DA, Willian MK, Menter A, Saurat
JH, Harnam N and Kaul M: Relationship between clinical response to
therapy and health-related quality of life outcomes in patients
with moderate to severe plaque psoriasis. Dermatology. 216:260–270.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Olteanu R, Constantin MM, Zota A,
Dorobanțu DM, Constantin T, Șerban ED, Bălănescu P, Mihele D and
Gheucă Solovăstru L: Original clinical experience and approach to
treatment study with interleukine 12/23 inhibitor in
moderate-to-severe psoriasis patients. Farmacia. 64:2–5. 2016.
|
|
29
|
Janowski K and Steuden S: Severity of
psoriasis and health-related quality of life: The moderating
effects of temperament. Br J Dermatol. 158:633–635. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bargh JA and Williams LE: On the non
conscious of emotion regulationGross JJ: Handbook of Emotion
Regulation. Guilford Press; New York: pp. 429–444. 2007
|
|
31
|
Mennin DS, Holaway RM, Fresco DM, Moore MT
and Heimberg RG: Delineating components of emotion and its
dysregulation in anxiety and mood psychopathology. Behav Ther.
38:284–302. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sidlauskaitė-Stripeikienė I, Zemaitienė N
and Klumbienė J: Associations between depressiveness and
psychosocial factors in Lithuanian rural population. Medicina
(Kaunas). 46:693–699. 2010. View Article : Google Scholar : PubMed/NCBI
|