Introduction
Syphilis is a bacterial infection caused by the
Treponema pallidum subspecies pallidum. The World
Health Organization estimated that 5.6 million new cases of
syphilis occurred among those aged 15–49 years worldwide in 2012,
with a global incidence rate of 1.5 cases per 1,000 people, despite
the availability of effective treatments (1,2). The
estimated 18 million prevalent cases of syphilis in 2012 translates
to a global prevalence of 0.5% among females and 0.5% among males
aged 15–49 years, with the highest prevalence in the WHO African
Region (3). In China, according to
an epidemiological study performed on syphilis cases reported from
31 provinces, autonomous regions, and municipalities between 2000
and 2013, the reported syphilis incidence increased yearly from
6.43 per 100,000 person-years in 2000 to 32.86 per 100,000
person-years in 2013, with an average annual growth rate of 13.37%
(4).
If untreated, the disease lasts many years and has
several stages. Early syphilis consists of primary syphilis,
secondary syphilis and early latent syphilis, while late syphilis
consists of late latent syphilis and tertiary syphilis
(neurosyphilis, cardiosyphilis and gumma). Primary syphilis
classically presents as a painless chancre at the site of
inoculation after a mean incubation period of 21 days (range: 9–90
days). The primary lesion begins as a raised papule and ulcerates
before healing within 3 to 10 weeks, with or without treatment
(1). The primary chancre may be
ignored by patients. If untreated, the disease progresses to the
secondary stage, 4 to 8 weeks after the appearance of the primary
lesion, which is characterized by generalized mucocutaneous lesions
affecting both skin and mucous membranes. The symptoms and signs of
secondary syphilis spontaneously resolve, even without treatment,
and if left untreated, the patient enters the latent stage, which
is often categorized in two phases: Early latent syphilis
(infection for less than two years) and late latent syphilis
(infection for two years or more). Patients with unknown duration
of infection should be treated for late latent syphilis. If left
untreated, most patients will remain in the latent stage.
Approximately 25% will develop the late clinical sequelae of
tertiary syphilis (5), which can
affect any organ system up to 30 years or more after infection.
Cerebral syphilitic gumma is a rare disease of the
central nervous system that is an unusual type of tertiary
syphilis. Due to the lack of knowledge regarding the imaging of
cerebral syphilitic gumma, pre-operative misdiagnosis often occurs,
with glioma being the most commonly misdiagnosed (6–9).
Treatment with penicillin G can treat most gummas and only a few
patients with intracranial hypertension crisis or
penicillin-resistance require surgical resection (7,10).
Therefore, a definitive diagnosis of syphilitic gumma may help
clinicians choose an appropriate treatment strategy and reduce the
risk of unnecessary surgery. There have been limited case reports
describing the neuroimaging features of intracranial syphilitic
gumma (6–9). Magnetic resonance imaging (MRI) of a
cerebral gumma was first described by Agrons et al (11) in 1991. The purpose of the present
study was to characterize the neuroimaging features of 6 cases of
syphilitic gumma. In the present study, a retrospective analysis
using medical records and neuroimaging data was performed to
evaluate the neuroimaging features of syphilitic gumma, with an
emphasis on MRI.
Patients and methods
Patients
From August 2012 to July 2016, 6 consecutive patient
records with histologically proven syphilitic gumma were reviewed
after receiving approval from the institutional review board at The
Affiliated Hospital of Southwest Medical University (Luzhou,
China). The 6 patients included 2 females and 4 males, ranging in
age from 32 to 61 years, with a mean age of 44.3 years. All
patients underwent CT, MRI or positron emission tomography (PET)/CT
at The Affiliated Hospital of Southwest Medical University. Five
patients with a single lesion underwent complete surgical
resection. One patient with multiple lesions underwent resection of
the largest lesion on the left parietal lobe and the remaining four
lesions were not surgically removed.
CT and MRI examination
All the patients were scanned with a 3.0-T scanner
(Koninklijke Philips, N.V.) using an eight-channel SENSE head coil
(SENSE acceleration factor of 8). The following MRI sequences were
included for the brain MRI: Axial T1-weighted imaging [T1WI;
repetition time (TR), 2,000 msec; echo time (TE), 20 msec], T2WI
(TR, 3,000 msec; TE, 80 msec), fluid-attenuated inversion recovery
(TR, 11,000 msec; TE, 125 msec), diffusion weighted imaging (DWI;
TR, 4,000 msec; TE, 64 msec; b-value, 1,000). Axial, sagittal and
coronal gadolinium-enhanced (0.1 mmol/kg) T1WI were acquired. All
CT images were obtained using a 4-detector CT scanner (LightSpeed;
GE Healthcare) with a 5 mm section thickness, 120 kV and 250
mA.
Due to multiple brain lesions and the suspicion of
brain metastases before operation, 18F-FDG PET/CT was performed in
only one patient.
Imaging analysis
Two experienced radiologists working in the
Affiliated Hospital of Southwest Medical University (Luzhou, China)
retrospectively reviewed the CT and MRI scans by consensus for the
location, size, density, T1 and T2 signal-intensity
characteristics, extent of vasogenic oedema (VE) and enhancement
patterns. VE was graded using the following scale: 0, No oedema and
an absence of increased T2 signal surrounding the gumma; I, mild
oedema with the width of the oedema <2 cm; II, moderate oedema
with the width of the oedema >2 cm and the range being <50%
of the ipsilateral cerebral hemisphere; III, severe oedema where
the range of the oedema was >50% of the ipsilateral cerebral
hemisphere.
Histopathology
All tissues came from surgically resected specimens.
First, all the specimens were fixed at room temperature for 24 h
with 4% neutral formaldehyde solution, then the tissues were
embedded in paraffin, and tissues were sectioned (4 µm). Finally,
hematoxylin-eosin (HE) staining at room temperature for 55 min and
a light microscopic examination was performed (magnification, ×200
or ×400).
Results
Patient clinical features
The present study included 6 patients with a
confirmed diagnosis of syphilitic gumma. All 6 patients expressed
positive results when tested with the Treponema pallidum
antibody and 5 patients expressed positive results in the
treponema pallidum particle agglutination test. Out of the 6
patients, 4 demonstrated positive results in the serological rapid
plasma reagin test. The Treponema pallidum spirochete was
found in pathological tissues using a Warthin-Starry silver stain
in 2 of the cases. The human immunodeficiency virus (HIV) test was
negative in all 6 patients. All the above tests were completed
between August 2012 and July 2016. A single patient died a week
after the operation and the other 5 patients received
post-operative penicillin treatment, as penicillin 18 million U/day
intravenously for a period of 2 weeks. Patient clinical features
are summarized in Tables I and
II.
 | Table I.Patient clinical characteristics. |
Table I.
Patient clinical characteristics.
| Case | Sex | Age (years) | RPR | TPPA | Anti-TP | HIV | Treponema
pallidum spirochete |
|---|
| 1 | M | 56 | (+) | (+) | (+) | (−) | No |
| 2 | M | 38 | (+) | (+) | (+) | (−) | Yes |
| 3 | M | 61 | (+) | (+) | (+) | (−) | No |
| 4 | M | 50 | (−) | (−) | (+) | (−) | No |
| 5 | F | 40 | (+) | (+) | (+) | (−) | Yes |
| 6 | F | 32 | (−) | (+) | (+) | (−) | No |
| Table II.Patient clinical features. |
Table II.
Patient clinical features.
| Case | Number of
lesion(s) | Symptoms and
durations | Treatment | Follow-up |
|---|
| 1 | Single lesion | Headache for ~6
months, and vomiting for ~1 month | Surgical resection
and Penicillin | No recurrence at 12
months |
| 2 | Single lesion | Intermittent
headache and dizziness for ~1 month | Surgical resection
and Penicillin | No recurrence at 18
months |
| 3 | Single lesion | Headache and
intermittent vomiting for ~3 months | Surgical resection
and Penicillin | No recurrence at 18
months |
| 4 | Multiple lesions
(five) | Headache with
decreased muscle strength for ~6 months | Surgical resection
and penicillin | No recurrence at 6
months |
| 5 | Single lesion | Sudden headache
with limb weakness | Surgical resection
and Penicillin | No recurrence at 12
months |
| 6 | Single lesion | Headache with
vomiting for ~2 months | Surgical
resection | Death one week
after surgery |
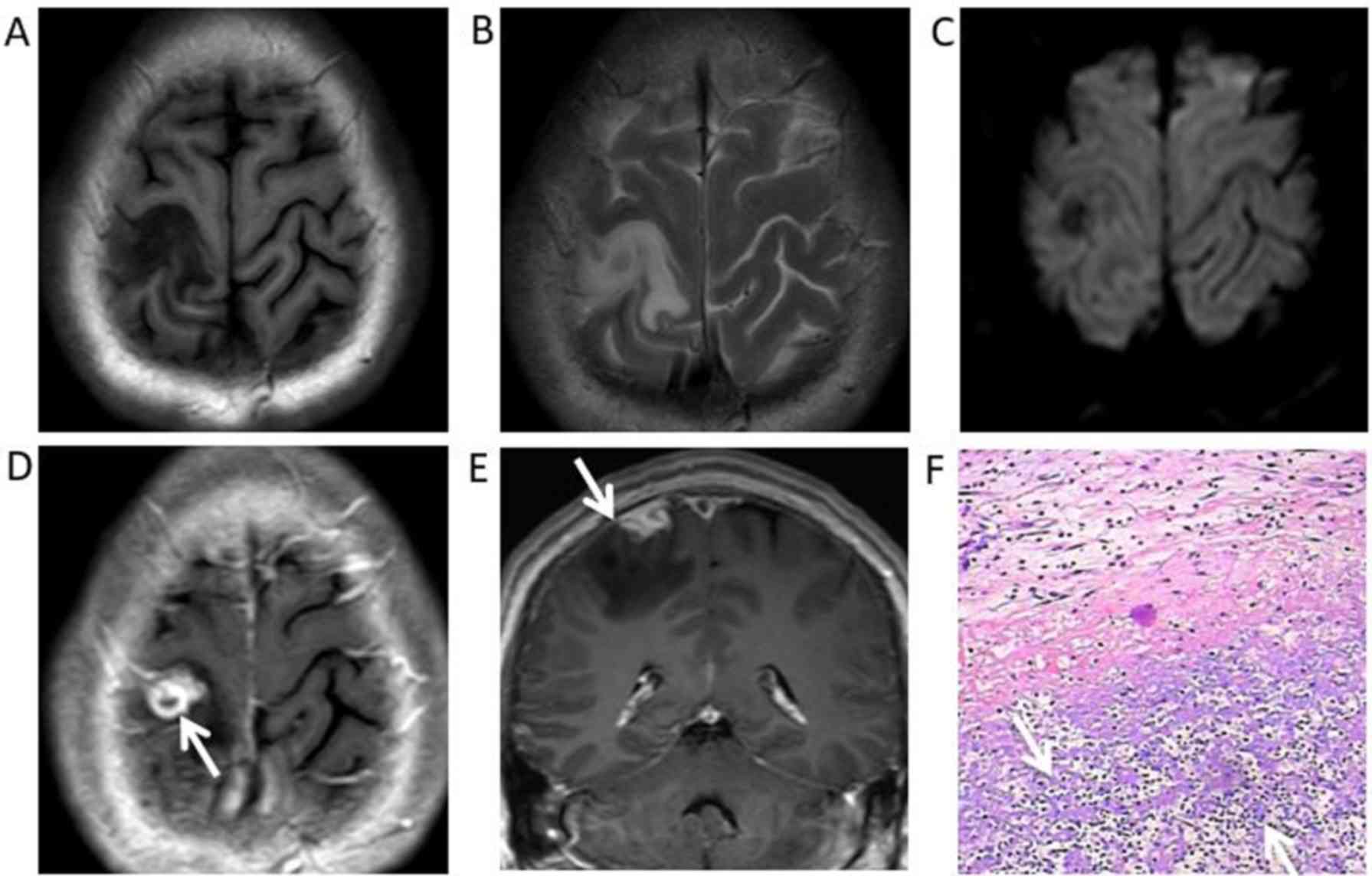
The imaging features
The 6 patients exhibited a total of 10 lesions, nine
of these lesions were located in the superficial region of the
cerebral hemisphere (Figs.
1–4), which involved both grey
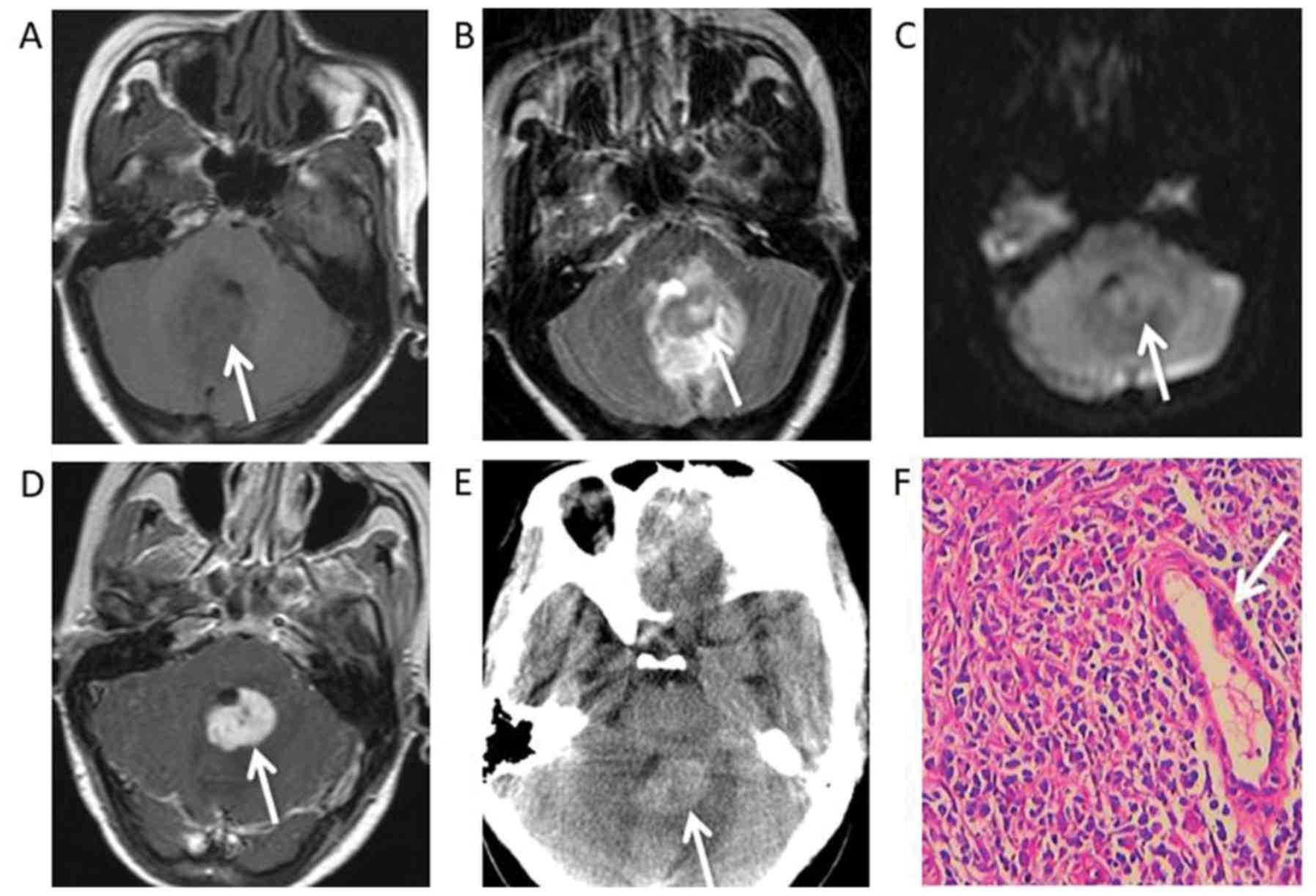
and white matter. In particular, one lesion was located in the
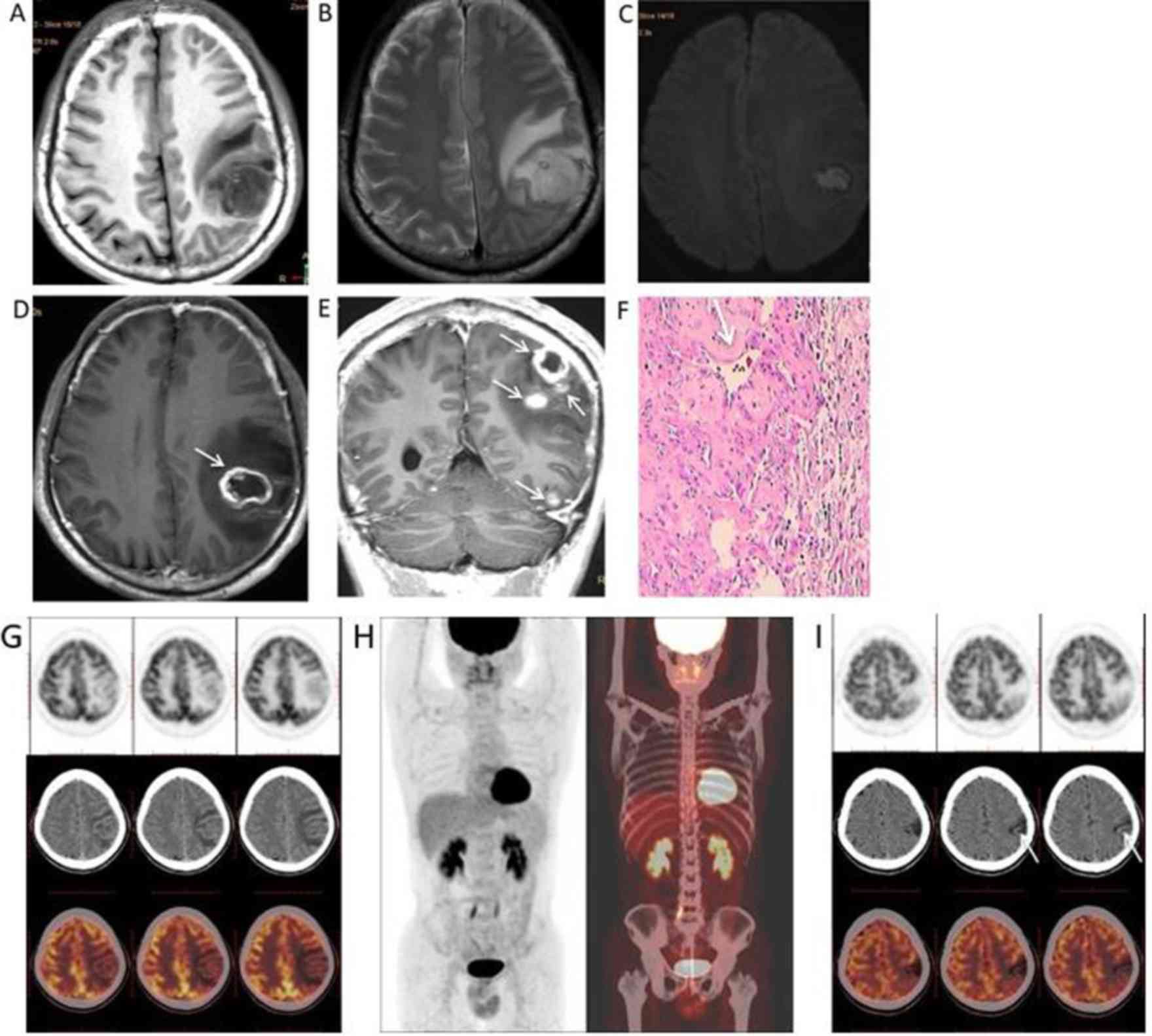
fourth ventricle, leading to mild hydrocephalus (Fig. 5A-E). A single patient had multiple
lesions, including five lesions located in the left
parietal-occipital lobe and temporal lobe (Fig. 3A). The 10 lesions ranged in size from
0.9–6.5 cm in diameter, with a mean diameter of 3.9 cm.
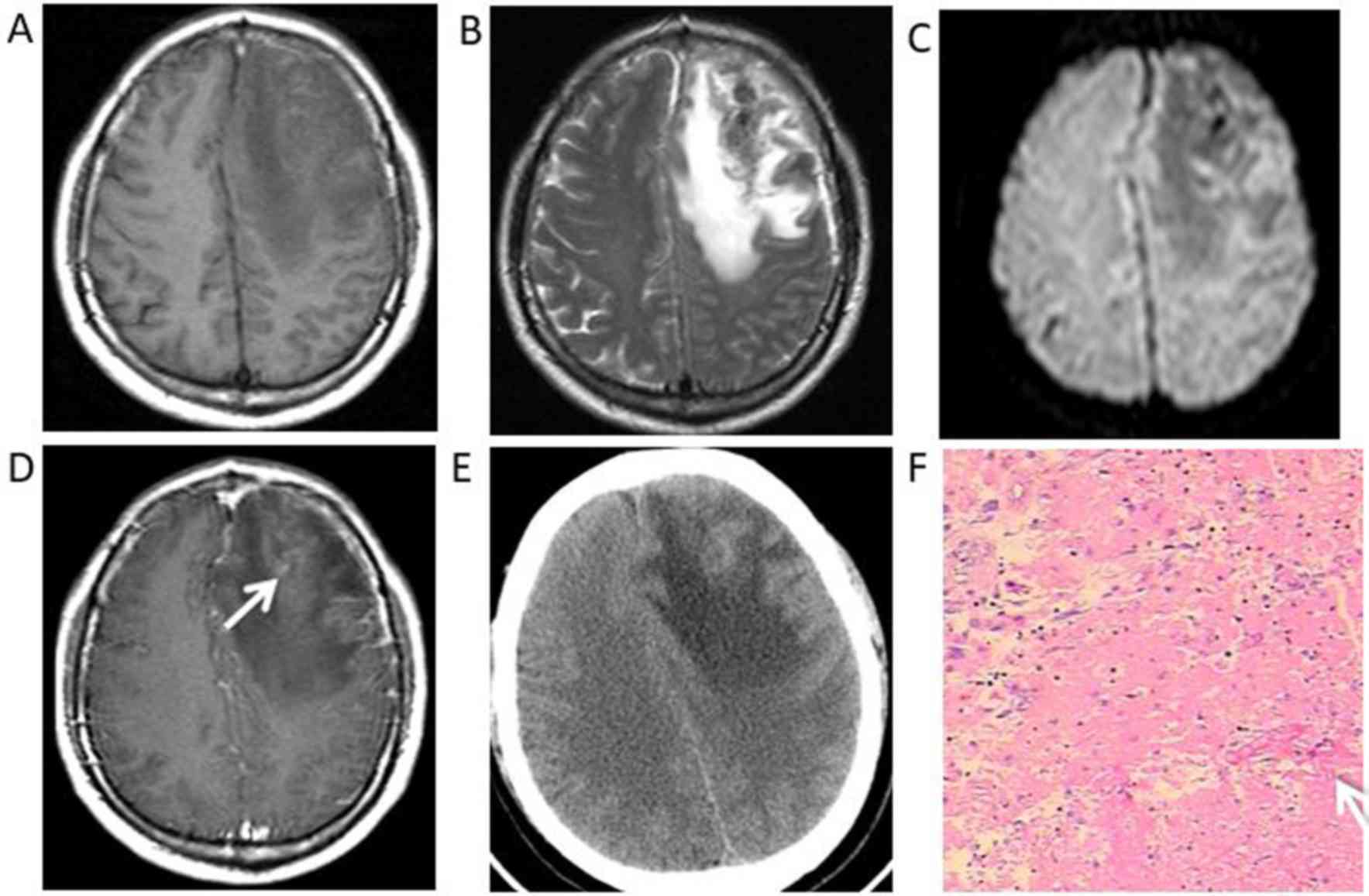
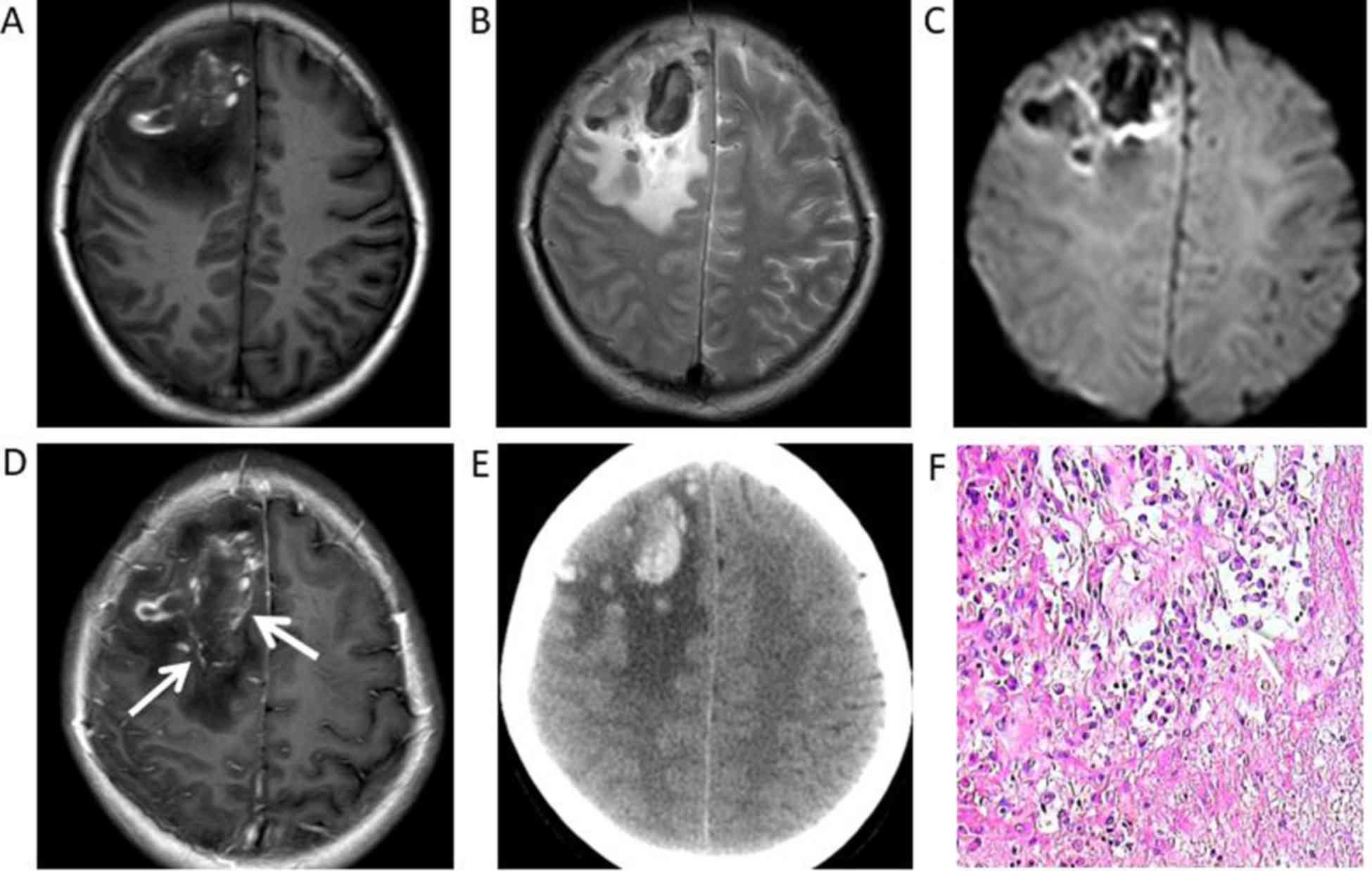
The CT and MRI features are summarized in Table III. Four patients were hypointense
in T1WI and hyperintense in T2WI. Furthermore, a single patient
exhibited hyperintensity under DWI. Furthermore, under T1WI and
T2WI, 2 patients exhibited mixed signal intensity with
hypointensity, hyperintensity and isointensity, while non-enhanced
CT scans revealed haemorrhage and focal haemorrhage in the right
frontal lobe and left frontal lobe, respectively (Figs. 2A, B, 4A,
B). All 6 patients had grade I–III vasogenic oedema surrounding
the masses, and a single case was accompanied by a midline
structure shift (Fig. 4A-E). The
results of contrast-enhanced MRI demonstrated masses with mild
(n=2) or marked (n=3) ring-like or strip-like enhancements in the
cerebral hemisphere (Figs. 1D,
2D, 3D,
E and 4D). The mass in the
fourth ventricle exhibited marked homogeneous enhancement (n=1)
(Fig. 5D), which led to
mild-to-moderate hydrocephalus. An enhanced dura mater adjacent to
the masses was observed in 2 of the 6 patients under enhanced T1WI.
This was described as ‘the dural tail sign’ (Fig. 1E).
| Table III.Neuroimaging findings of cerebral
syphilitic gumma. |
Table III.
Neuroimaging findings of cerebral
syphilitic gumma.
| Case | T1WI | T2WI | DWI | Enhancement
patterns | Dural tail
sign | CT | VE |
|---|
| 1 | Hyper/iso
intensity | Hypo/iso
intensity | Hypo intensity | Mild
strip-like | No | High density | III |
| 2 | Hypo intensity | Hyper
intensity | Hypo intensity | Marked
ring-like | Yes | Low density | I |
| 3 | Hypo intensity | Hyper
intensity | Hypo intensity | Marked
strip-like | No | Low density | II |
| 4 | Hypo intensity | Hyper
intensity | Hyper
intensity | Marked
ring-like | No | Low density | II |
| 5 | Hyper/hypo
intensity | Hypo/iso
intensity | Hypo intensity | Marked
ring-like | Yes | High density | II |
| 6 | Hypo intensity | Hyper
intensity | Iso intensity | Marked
homogeneous | No | High density | II |
Whole-body 18F-FDG PET/CT was performed on a single
patient (patient 4) before surgery and at 6 months after surgery.
The first 18F-FDG PET/CT examination revealed low uptake and low
metabolism in the gumma (Fig. 3G)
and 18F-FDG uptake in the gumma was lower than that of normal grey
matter (Fig. 3G). No other primary
or metastatic tumors were identified in the patient (Fig. 3H). Follow-up 18F-FDG PET/CT scans at
6 months after high-dose penicillin treatment revealed that the
lesions tended to calcify post-operatively (Fig. 3I).
The pathological features
Syphilitic gumma is a classic example of
granulomatous inflammation. Microscopic examination showed that
each of the resected lesions had multifocal haemorrhage (Fig. 4F) and necrosis with small necrotic
vessels (Figs. 1F, 3F). There was also prominent perivascular
chronic inflammatory lymphocyte and plasma cell infiltration
surrounding areas of necrosis (Figs.
2F, 5F).
Discussion
Syphilis is a chronic infectious disease caused by
Treponema pallidum that is distinguishable among other
infectious diseases due to its large variety of clinical
manifestations (2,4). According to guidelines from the Centers
for Disease Control and Prevention, syphilis can be divided into
the following four phases: Primary, secondary, latent and tertiary
(12). Neurosyphilis can occur at
each of these stages with various clinical presentations, including
cranial nerve dysfunction, meningitis and acute or chronic changes
in mental status. The main neuroimaging manifestations include
diffuse cerebral atrophy followed by cerebral infarction (13). However, neurosyphilis may also be
asymptomatic, which frequently leads to a lack of diagnosis
(14). Cerebral syphilitic gumma is
a rare manifestation of advanced meningovascular syphilis that has
presented following the introduction of penicillin and usually
occurs 10–30 years after contracting syphilis (12). However, the progression of syphilis
is reported to be faster in patients with HIV compared with those
not infected with HIV (15). A
definitive diagnosis can be difficult as syphilitic gumma can
present with a variety of central nervous system manifestations
that mimic other diseases, including malignant neoplasms and other
inflammatory diseases. In the present study, the clinical
manifestations of 6 patients were assessed and were determined to
be unspecific. Of the 6 patients, 3 patients experienced headaches
and vomiting, 2 patients exhibited headaches and decreased muscle
strength, and a single patient suffered recurrent dizziness. None
of the patients had typical lesions of stage three syphilis, such
as erythema and papules. According to literature and the author's
clinical experience, the clinical manifestations of syphilitic
gumma are not specific for its diagnosis (9,11). The
course, symptoms and signs of the disease were not significantly
different from those of other brain lesions, including tumors,
tuberculosis and abscesses, except for the history of syphilis.
However, in some cases, the history of syphilis provided by
patients is not objective or is inaccurate as many patients with
syphilis tend not to disclose their disease history. Of the 6 cases
assessed in the present study, 4 cases were misdiagnosed as glioma,
a single case was misdiagnosed as a metastatic tumor and another
case was misdiagnosed as ependymoma. Neuroimaging may provide an
insight into the pathology of the diverse clinical manifestations
of gumma. MRI is the best choice for detecting central nervous
system diseases. Compared with CT, the signal characteristics of
MRI more accurately and objectively reflect the pathological
features of the lesions being investigated (16–18).
However, CT is more sensitive for small calcifications, which is
helpful for the differential diagnosis of central nervous system
diseases (19).
Fargen et al (20) reported that cerebral syphilitic
gummata were more common in men (64%) and in those aged between
18–39 years in 156 cases that presented with 185 lesions.
Additionally, lesions may be located anywhere, but were most common
on the convexities (66%), as cerebral gumma is thought to arise
from a direct extension of syphilitic meningovascular inflammation
into the adjacent brain. This inflammation usually entails
extension from the pia mater or via small intracerebral vessels
that course into the subcortical grey nuclei. In the present study,
all lesions were located in a superficial region of the cerebral
hemisphere, except in a single case where the lesion was located in
the fourth ventricle. The results of the present study are
consistent with the findings of this aforementioned study.
MRI generally demonstrated hypointensity under T1WI
and hyperintensity under T2WI with adjacent oedema, while CT images
revealed low density results. Occasionally, syphilitic gumma was
accompanied by haemorrhage, necrosis or calcification, with a
heterogeneous signal. In the present study, all the masses
performed as ring-like, strip-like or uniform enhancements under
gadolinium-enhanced T1WI. The enhancement pattern of the lesion was
associated with the disrupted blood-brain barrier in the peripheral
blood vessels of inflammatory granulation tissue (7,8,13). In the present study, 2 cases of dural
enhancement were identified adjacent to masses, which were deemed
‘dural tail sign’. Bourekas et al (21) proposed that gummas are mass lesions
of inflammatory granulomatous tissue. It was therefore hypothesized
that the dural tail is caused by reactive changes in adjacent
connective tissue and by hypervascularity. Additionally,
pathological specimens frequently exhibit dural thickening and
inflammation adjacent to cerebral gumma (7). The dural tail sign has also been
reported in previous studies on syphilitic gumma (7–9,20,21). In
a previous study, Tsuboi et al (22) revealed that all the cases studied
exhibited marked enhancement with gadolinium administration, with
~35% of cases presenting with perilesional meningeal enhancement
and thickening or a dural tail via MRI. Massive haemorrhage was
also accompanied by syphilitic gumma in a female patient.
Therefore, the present study speculated that the cause of
haemorrhage may be associated with vascular endothelial cell injury
and the long-term inflammatory stimulation of the vascular wall,
leading to the rupture of small vessels. A single case analyzed in
the present study with left hemisphere lesions of different sizes
and ring-like enhancement on gadolinium-enhanced T1WI was
misdiagnosed as brain metastasis before surgery. The patient was
pre-operatively subjected to a whole-body 18F-FDG PET-CT to
determine whether there were other primary or metastatic tumors,
but none were identified. 18F-FDG PET/CT examination revealed gumma
exhibited a lower metabolism and lower uptake of 18F-FDG, and the
18F-FDG uptake by the gumma was lower than that of the surrounding
normal grey matter. Follow-up 18F-FDG PET-CT scans 6 months after
high-dose penicillin treatment, revealed that the lesions tended to
calcify post-operatively. To the best of our knowledge, there are
no studies assessing the 18F-FDG PET/CT results of syphilis gumma.
Similarly, in one case report of syphilitic gumma, CT perfusion
revealed no increase in the cerebral blood volume of the enhancing
lesion compared with the ipsilateral normal-appearing white matter
(23). The 6th case in the present
study that had a mass in the fourth ventricle with uniform
enhancement on gadolinium-enhanced T1WI was highly suspected to be
ependymocytoma based on pre-operative MRI. In the present study, it
was difficult to distinguish between the gumma and ependymocytoma,
according to the neuroimaging findings. Due to the various forms of
intracranial gumma images and a lack of radiologist experience,
pre-operative misdiagnosis occurs frequently in clinical
practice.
Intracranial syphilitic gumma have extensive
differential diagnoses, including glioma, metastasis, malignant
meningioma and abscess. Malignant gliomas possess profuse
neovascularisation characterized by disorganized, irregular and
tortuous vessels with arteriovenous shunting (24). An irregular tumor vascular structure
consequently causes abnormal vascular function with increased
permeability and perfusion (24,25).
Malignant gliomas are characterized by increased perfusion and
heterogeneous disruption of the blood-brain barrier (26). The tumor exhibits irregular ring-like
or nodular enhancement under gadolinium-enhanced T1WI and its
margin presents vasogenic oedema with infiltrative tumor cells
along with perivascular spaces (24–26).
However, gumma is a chronic perivascular inflammation that is
characterized by the proliferation of small vessels and the
infiltration of lymphocytes and plasmocytes around regions of
necrosis. Patients with metastases usually exhibit a history of
primary malignant tumors and mostly occur in grey and white matter
junctions. Malignant meningioma presents features of an aggressive
disease, with no demarcation between the tumor and brain
parenchyma, and invasion of surrounding structures, including the
skull, scalp and venous sinus. They characteristically invade the
brain in a mushroom shape from their dural attachment (27,28).
However, syphilitic gumma encroaches on and is closely associated
with the meninges. The edge of the lesion often intersects with the
surrounding meninges at an obtuse angle (2). The pus of most abscesses show as
hyperintense under DWI, hyperintense under T2WI and as a peripheral
hypointense rim and iso- to hypointense under T1WI, which are
characteristics of integument-term brain abscesses (29).
Functional MRI techniques, including magnetic
resonance spectroscopy (MRS), perfusion weighted imaging (PWI) and
DWI, are helpful for the diagnosis and differential diagnosis of
tumors and non-neoplastic lesions. The proton-MRS technique
produces an increase in the choline (Cho)/creatine (Cr) ratio and a
reduction in the N-acetylaspartate (NAA)/Cr ratio in brain tumors
(30). In a previous study published
by Ventura et al (31), a
mild increase in the Cho/NAA ratio in syphilitic gumma was
identified. Furthermore, the brain PWI reflected the degree of
tumor vascular proliferation and vascular permeability, but PWI is
not directly associated with damage of the blood-brain barrier
(32,33). The perfusion of high-grade glioma was
significantly increased, while infectious lesions, such as brain
abscess, were significantly reduced (34,35). To
the best of our knowledge, there are no studies on the magnetic
resonance perfusion imaging of intracranial syphilis gumma.
However, it is speculated that functional MRI may be helpful in the
diagnosis and differential diagnosis of intracranial syphilitic
gumma.
In conclusion, two important points are suggested
regarding the neuroimaging findings of intracranial syphilitic
gumma. First, syphilitic gumma predominantly appeared in the
superficial part of the cerebral hemisphere, which mostly involved
the grey matter. Second, meningeal thickening and enhancement
adjacent to syphilitic gumma could be of great significance. These
two points, combined with advanced neuroimaging techniques and
laboratory examinations could aid accurate pre-operative
diagnoses.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CL and GC collected and analysed the clinical data
and prepared the manuscript; LL, SW and GT collected the clinical
data. The final version of the manuscript has been read and
approved by all authors and each author believes that the
manuscript represents honest work.
Ethical approval and consent to
participate
The present study was approved by the Ethics
Committee of Affiliated Hospital of Southwest Medical
University.
Patient consent for publication
Patients provided written informed consent for
publication.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
HIV
|
human immunodeficiency virus
|
|
VE
|
vasogenic oedema
|
|
MRS
|
magnetic resonance spectroscopy
|
|
PWI
|
perfusion weighted imaging
|
References
|
1
|
World Health Organization (WHO), . WHO
guidelines for the treatment of Treponema pallidum
(syphilis)WHO; Geneva: 2016, https://www.who.int/reproductivehealth/publications/rtis/syphilis-treatment-guidelines/en/
|
|
2
|
Grillova L, Jolley K, Šmajs D and
Picardeau M: A public database for the new MLST scheme for
Treponema pallidum subsp. pallidum: Surveillance and
epidemiology of the causative agent of syphilis. Peer J.
6:e61822019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Newman L, Rowley J, Vander Hoorn S,
Wijesooriya NS, Unemo M, Low N, Stevens G, Gottlieb S, Kiarie J and
Temmerman M: Global estimates of the prevalence and incidence of
four curable sexually transmitted infections in 2012 based on
systematic review and global reporting. PLoS One. 10:e01433042015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gong XD, Yue XL, Teng F, Jiang N and Men
PX: Syphilis in China from 2000 to 2013: Epidemiological trends and
characteristics. Chin J Dematol. 47:310–315. 2014.
|
|
5
|
Clark EG and Danbolt N: The Oslo study of
the natural course of untreated syphilis: An epidemiologic
investigation based on re-study of the Boeck-Bruusgaard material.
Med Clin North Am. 48:613–623. 1964. View Article : Google Scholar
|
|
6
|
Roeske LC and Kennedy PR: Images in
clinical medicine. Syphilitic gummas in a patient with human
immunodeficiency virus infection. N Engl J Med. 10:11231996.
View Article : Google Scholar
|
|
7
|
Shao XF, Qiang D, Liu YH, Yuan Q, Tao J
and Ji BH: Diagnosis and treatment of cerebral syphilitic gumma: A
report of three cases. Front Neurosci. 27:1002018. View Article : Google Scholar
|
|
8
|
Xia DY, Zhu MF, Liu CG, Dai Y, Li ZB,
Jiang XC and Xu SS: Cerebral syphilitic gumma misdiagnosed as a
malignant brain tumor. J Craniofac Surg. 28:e170–e172. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Baek HJ and Kim WJ: Cerebral gumma
mimicking a brain tumor in a human immunodeficiency virus-negative
patient: A case report. J Korean Soc Radiol. 69:181–185. 2013.
View Article : Google Scholar
|
|
10
|
Kikuchi Y, Hiwatashi A, Togao O, Yamashita
K, Momosaka D and Honda H: Cerebral syphilitic gumma mimicking
glioma: Utility of CT perfusion. Diagn Interv Imaging. 99:755–757.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Agrons GA, Han SS, Husson MA and Simeone
F: MR imaging of cerebral gumma. Am J Neuroradiol. 12:80–81.
1991.PubMed/NCBI
|
|
12
|
Fan SR and Liang LF: CDC 2015 guideline
for the diagnosis and treatment of syphilis. Chin Gen Pract.
18:3260–3264. 2015.
|
|
13
|
Nagappa M, Sinha S, Taly AB, Rao SL,
Nagarathna S, Bindu PS, Bharath RD and Murthy P: Neurosyphilis: MRI
features and their phenotypic correlation in a cohort of 35
patients from a tertiary care university hospital. Neuroradiology.
55:379–388. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang Z, Liu L, Shen YZ, Zhang RF, Qi TK,
Tang Y, Song W, Chen J and Lu H: The clinical and laboratory
features of neurosyphilis in HIV-infected patients: A retrospective
study in 92 patients. Medicine. 97:e00782018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Johns DR, Tierney M and Felsenstein D:
Alteration in the natural history of neurosyphilis by concurrent
infection with the human immunodeficiency virus. N Engl J Med.
316:1569–1572. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Scatliff JH: MRI of the central nervous
system. Investigative Radiol. 26:622–623. 1991. View Article : Google Scholar
|
|
17
|
Mori K: IntroductionMori K: MRI of the
Central Nervous System. Springer; Tokyo: 1991, View Article : Google Scholar
|
|
18
|
Kimura M and da Cruz LCH Jr:
Multiparametric MR imaging in the assessment of brain tumors. Magn
Reson Imaging Clin N Am. 24:87–122. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Laughlin S and Montanera W: Central
nervous system imaging. When is CT more appropriate than MRI?
Postgrad Med. 104:73–76, 81-84, 87–88. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fargen KM, Alvernia JE, Lin CS and Melgar
M: Cerebral syphilitic gummata: A case presentation and analysis of
156 reported cases. Neurosurgery. 64:568–576. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bourekas EC, Wildenhain P, Lewin JS, Tarr
RW, Dastur KJ, Raji MR and Lanzieri CF: The dural tail sign
revisited. AJNR Am J Neuroradiol. 16:1514–1546. 1995.PubMed/NCBI
|
|
22
|
Tsuboi M, Nishijima T, Teruya K, Kikuchi
Y, Gatanaga H and Oka S: Cerebral syphilitic gumma within 5 months
of syphilis in HIV-infected patient. Emerg Infect Dis.
22:1846–1848. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kikuchi Y, Hiwatashi A, Togao O, Yamashita
K, Momosaka D and Honda H: Cerebral syphilitic gumma mimicking
glioma: Utility of CT perfusion. Diagn Interv Imaging. 99:755–757.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Soda Y, Myskiw C, Rommel A and Verma IM:
Mechanisms of neovascularization and resistance to anti-angiogenic
therapies in glioblastoma multiforme. J Mol Med (Berl). 91:439–448.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jain RK, di Tomaso E, Duda DG, Loeffler
JS, Sorensen AG and Batchelor TT: Angiogenesis in brain tumours.
Nat Rev Neurosci. 8:610–622. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhang J, Liu H, Tong H, Wang S, Yang Y,
Liu G and Zhang W: Clinical applications of contrast-enhanced
perfusion MRI techniques in gliomas: Recent advances and current
challenges. Contrast Media Mol Imaging. 2017:70641202017.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
O'Leary S, Adams WM, Parrish RW and
Mukonoweshuro W: Atypical imaging appearances of intracranial
meningiomas. Clin Radiol. 62:10–17. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lyndon D, Lansley JA, Evanson J and
Krishnan AS: Dural masses: Meningiomas and their mimics. Insights
Imaging. 10:112019. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gupta RK, Hasan KM, Mishra AM, Jha D,
Husain M, Prasad KN and Narayana PA: High fractional anisotropy in
brain abscesses versus other cystic intracranial lesions. Am J
Neuroradiol. 26:1107–1114. 2005.PubMed/NCBI
|
|
30
|
Son HS, Kim EN, Kim SH, Yoo YR, Jung YA,
Jung SG, Hong YG, Lee YS and Choi BY: Evaluation of Glioma with
Thallium-201 Brain SPECT: The correlation with 1H MR spectroscopy
and pathology. Korean J Nucl Med. 34:465–477. 2000.
|
|
31
|
Ventura N, Cannelas R, Bizzo B and
Gasparetto EL: Intracranial syphilitic gumma mimicking a brain stem
glioma. AJNR Am J Neuroradiol. 33:E110–E111. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Maia AC Jr, Malheiros SM, da Rocha AJ, da
Silva CJ, Gabbai AA, Ferraz FA and Stávale JN: MR cerebral blood
volume maps correlated with vascular endothelial growth factor
expression and tumor grade in nonenhancing gliomas. AJNR Am J
Neuroradiol. 26:777–783. 2005.PubMed/NCBI
|
|
33
|
Fu L and Li K: Principles & clinical
application of brain PWI. Chin Comput Med Imag. 19:180–183.
2013.(In Chinese).
|
|
34
|
Britt RH, Enzmann DR and Yeager AS:
Neuropathological and computerized tomographic findings in
experimental brain abscess. J Neurosurg. 55:590–603. 1981.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hakyemez B, Erdogan C, Ercan I, Ergin N,
Uysal S and Atahan S: High-grade and low-grade gliomas:
Differentiation by using perfusion MR imaging. Clin Radiol.
60:493–502. 2005. View Article : Google Scholar : PubMed/NCBI
|