Introduction
Acute respiratory distress syndrome (ARDS) refers to
acute inflammatory injury to the lung. The condition is
characterized by increased vascular permeability, extravasation of
plasma, pulmonary edema and acute hypoxemic respiratory failure
(1). ARDS is associated with a high
mortality rate. Several treatment strategies have been applied for
patients affected; however, only few of these, with the exception
of lung-protective mechanical ventilation, have had an impact on
ARDS outcomes (2,3). Since inflammation is a key pathogenetic
mechanism of ARDS (1), it is
reasonable to explore therapies that modulate acute lung
inflammation.
Glucocorticoids are the most commonly used
anti-inflammatory and immunomodulatory drugs. Studies that
investigated the role of glucocorticoids in ARDS have yielded
inconsistent results. Several studies indicated that
glucocorticoids did not reduce the risk of ARDS-associated
mortality (4–6). However, in one study, glucocorticoids
were reported to reduce the intensive care unit (ICU) mortality in
patients with ARDS (7). The present
meta-analysis was performed to assess the effect of glucocorticoid
therapy on mortality in patients with ARDS.
Materials and methods
Selection of studies
The PubMed (reference period: January 1, 1966 to
December 31, 2016), Chinese Knowledge Infrastructure and Wanfang
databases (reference period: January 1,1982 to December 31, 2016),
and the Cochrane trials database (reference period: January 1, 1966
to December 31, 2016) were searched for all relevant publications
pertaining to acute lung injury and ARDS.
The following search terms were used: ‘acute lung
injury’, ‘acute respiratory distress syndrome’ AND
‘glucocorticoids’, ‘corticosteroid’, ‘steroid’,
‘methylprednisolone’, ‘dexamethasone’, ‘hydrocortisone’,
‘prednisolone’ AND ‘randomized’, ‘random’, ‘randomly’ AND
‘patient’. If a study was included in a review and was indexed in
the PubMed database, associated studies were further explored using
the ‘Related Articles’ option. The reference lists of relevant
papers were manually screened to identify additional studies.
Randomized controlled trials (RCTs) that fulfilled
the following criteria were included: i) Patients with ARDS; ii)
patients aged ≥18 years; and iii) use of glucocorticoids. The
trials were excluded if they i) were non-RCTs; ii) were published
as an abstract only; or iii) did not report the mortality data.
Quality assessment
Three reviewers independently assessed the
methodological quality using a 10-point scoring system based on a
previous meta-analysis (8). This
10-piont scoring system includes ‘Randomization’, ‘Allocation
concealment’, ‘Blinding’, ‘Inclusion and exclusion criteria
defined’, ‘Similar baseline at study entry’, ‘Treatment protocol
clearly described’, ‘Cointervention that may affect outcome’,
‘Outcome definition’, ‘Extent of follow-up clearly described’ and
‘Intention-to-treat analysis’. In contrast, Cochrane system
includes ‘Sequence generation’, ‘Allocation concealment’, ‘Blinding
of participants, personnel and outcome assessors’, ‘Incomplete
outcome data’, ‘Selective outcome reporting’ and ‘Other sources of
bias’ (Cochrane Handbook for Systematic Reviews of Interventions).
Since the 10-point scoring system includes more parameters compared
with Cochrane, the former scoring system was chosen.
Data extraction and clinical
outcomes
The identification of trials and data extraction
were independently performed by two reviewers (QL and CYZ), and any
disagreements were resolved via consultation with a third reviewer
(RH). The outcome measure was mortality.
Statistical analysis
Meta-analysis was performed using the
Mantel-Haentzel method to calculate the odds ratios (OR) for
mortality along with 95% confidence interval (CI) (8). Heterogeneity among the studies was
assessed using the Cochran's Q statistic. In case of lack of
significant heterogeneity (P>0.05), the fixed-effects model was
used for the meta-analysis, while a random-effects model was used
in case of significant heterogeneity (P≤0.05). The degree of
heterogeneity was tested with I2 statistics using the
Review Manager software; values <25% were considered indicative
of low heterogeneity, while values of 25–50% and >50% were
considered indicative of moderate and high heterogeneity,
respectively (9). The meta-analysis
was performed using Review Manager 5.0.24 (Cochrane Library
Software).
Results
Selection and characteristics of
trials
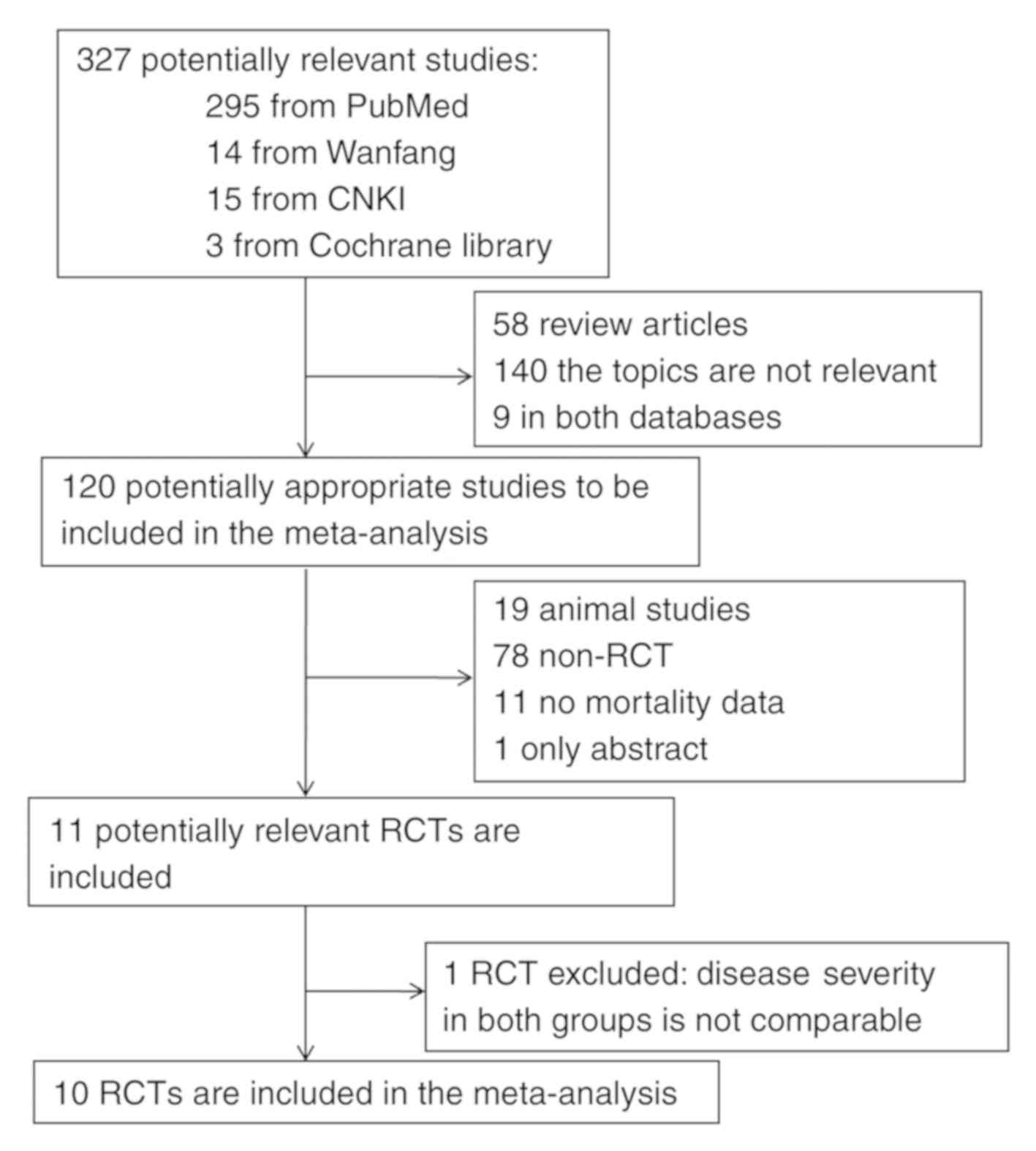
A flow chart depicting the study selection is
provided in Fig. 1. A total of 327
articles (298 in English language and 29 in Chinese), were
retrieved in the database search. Any studies published in
languages other than English and Chinese were excluded. Of these,
316 studies that were not relevant were excluded. One study was
excluded due to the serum creatinine levels in the
methylprednisolone group were significantly higher compared with
those in the control group (10),
implying that disease severity in the two groups was not
comparable. Except for serum creatinine levels, other baseline
parameters, including age, sex, etiology and blood pressure in both
groups were comparable (10). A
total of 10 RCTs fulfilled the inclusion criteria and were selected
for the final analysis (4–7,11–16). The
characteristics of the studies included are summarized in Table I. The major categories of ARDS risk
factors included pneumonia, sepsis, trauma, shock and aspiration.
The definition of ARDS in the studies included was largely
consistent with the Berlin definition (17).
 | Table I.Characteristics of the randomized
controlled trials included in the meta-analysis. |
Table I.
Characteristics of the randomized
controlled trials included in the meta-analysis.
| First author
(year) | Group | Age
(years)a |
PaO2/FiO2 | ARDS definition | Etiologic
factors | (Refs.) |
|---|
| Weigelt (1985) | GC (n=25) | 19–75 | 165–350 | PaO2
<100 mmHg | Sepsis, shock,
massive | (4) |
|
| Control (n=14) | 19–72 | 95–345 | on 40% oxygen or | transfusion,
contusion, |
|
|
|
|
|
| PaO2
<350 mmHg | alveolar
hypoventilation, |
|
|
|
|
|
| on 100% oxygen. | aspiration. |
|
| Bernard (1987) | GC (n=50) | 55±2 | NA | (1) PaO2 ≤70 mmHg | Sepsis, aspiration,
infectious | (11) |
|
| Control (n=49) | 56±2 | NA | on 40% oxygen; | pneumonia,
pancreatitis, |
|
|
|
|
|
| (2) Bilateral diffuse | shock, fat emboli,
and other |
|
|
|
|
|
| infiltrates on
chest | causes or multiple
causes. |
|
|
|
|
|
| radiography
and |
|
|
|
|
|
|
| (3) PAWP ≤18 mmHg. |
|
|
| Luce (1988) | GC (n=38) | 50±2.5 | NA | (1) The new onset of | Pneumonia,
peritonitis | (5) |
|
| Control (n=37) | 53±2.5 | NA | diffuse infiltrates
involving | and others. |
|
|
|
|
|
| all 4 quadrants of
the chest |
|
|
|
|
|
|
| roentgenogram; |
|
|
|
|
|
|
| (2) PaO2/PAO2 <0.30
and |
|
|
|
|
|
|
| (3) PAWP ≤18 mmHg. |
|
|
| Meduri (1998) | GC (n=16) | 47±3.9 | 110±11 | AECC criteria | NA | (12) |
|
| Control (n=8) | 51±6.6 | 123±11 |
|
|
|
| Confalonieri
(2005) | GC (n=23) | 60.4±17.3 | 141±49 | AECC criteria | CAP | (13) |
|
| Control (n=23) | 66.6±14.7 | 178±58 |
|
|
|
| Steinberg
(2006) | GC (n=89) | 49.0±19.0 | 126±42 | AECC criteria | Trauma, sepsis,
multiple | (6) |
|
| Control (n=91) | 49.2±16.5 | 126±40 |
| transfusions,
aspiration, |
|
|
|
|
|
|
| pneumonia and
other. |
|
| Annane (2006) | GC (n=85) | 61±16 | NA | AECC criteria | Lung and other
infections | (14) |
|
| Control (n=92) | 59±18 | NA |
| with septic
shock. |
|
| Meduri (2007) | GC (n=63) | 50.1±15.3 | 118.4±51.2 | AECC criteria | Pneumonia,
aspiration of | (7) |
|
| Control (n=28) | 53.2±15.3 | 125.9±38.6 |
| gastric content,
sepsis and |
|
|
|
|
|
|
| other. |
|
| Seam (2012) | GC (n=55) | 49.7±2.1 | 119.5±6.9 | AECC criteria | CAP, HAP,
intra-abdominal | (15) |
|
| Control (n=24) | 53.9±3.4 | 126.2±8.2 |
| and urinary tract
infection, |
|
|
|
|
|
|
| endocarditis,
necrotizing |
|
|
|
|
|
|
| fasciitis,
bacteremia of |
|
|
|
|
|
|
| unknown source,
ehrlichiosis, |
|
|
|
|
|
|
| aspiration,
postoperation, |
|
|
|
|
|
|
| pancreatitis and
other. |
|
| Tongyoo (2016) | GC (n=98) | 64.5±17.3 | 175.4±6.9 | AECC criteria | Severe sepsis or
septicshock. | (16) |
|
| Control (n=99) | 64.3±16.0 | 172.4±6.7 |
|
|
|
The treatment regimens and mortality data are
provided in Table II. The treatment
regimens varied considerably between studies (Table II). In 8 studies, glucocorticoid
treatment was initiated in the early phase of ARDS (within 1 week
of diagnosis) (4,5,7,11,13,14–16); in
2 studies, glucocorticoid therapy was initiated in the later phase
of ARDS (>1 week after diagnosis) (6,12). The
dosage of glucocorticoids ranged from 40 to 60 or 1 to 2 mg/kg/day
of methylprednisolone or equivalent. Glucocorticoid doses were
tapered in 4 studies (6,7,12,15). The
treatment duration was also different among studies (range, 1–32
d). Due to limitations in the understanding of the mechanisms and
characteristics of ARDS, in that ARDS was at first thought to be a
short-term acute inflammation in the lung in the past,
glucocorticoids were used only for 1 or 2 days in 3 early studies
(4,5,11).
Glucocorticoids were used to treat but not prevent ARDS in most
studies except for one study (5).
| Table II.Treatment regimens and mortality data
of the trials included in the meta-analysis. |
Table II.
Treatment regimens and mortality data
of the trials included in the meta-analysis.
| First author
(year) | Treatment
timing | Drug | Dosing and course
of treatment | Intention
(prevention or treatment) | Mortality
end-point | Mortality status
(dead/alive) | (Refs.) |
|---|
| Weigelt (1985) | Early | MTPS | 120 mg/kg/d for 2
d | Treatment | Hospital | GC: 11/14 | (4) |
|
|
|
|
|
|
| Control: 6/8 |
|
| Bernard (1987) | Early | MTPS | 120 mg/kg/d for 1
d | Treatment | 45 d | GC: 30/20 | (11) |
|
|
|
|
|
|
| Control: 31/18 |
|
| Luce (1988) | Early | MTPS | 8 mg/kg/d for 1
d | Prevention | Hospital | GC: 9/4 | (5) |
|
|
|
|
|
|
| Control: 12/2 |
|
| Meduri (1998) | Later | MTPS | 2 mg/kg/d for 4
d | Treatment | Hospital | GC: 2/14 | (12) |
|
|
|
| and tapering; 32
d |
|
| Control: 5/3 |
|
| Confalonieri
(2005) | Early | Hyd | Single 200 mg | Treatment | Hospital | GC: 0/23 | (13) |
|
|
|
| followed by |
| and 60 d | Control: 7/16 |
|
|
|
|
| 240 mg/d; 7 d |
|
|
|
|
| Steinberg
(2006) | Later | MTPS | Single 2 mg/kg | Treatment | 60 d | GC: 28/61 | (6) |
|
|
|
| followed by |
|
| Control: 29/62 |
|
|
|
|
| 2 mg/kg/d for 14
d |
|
|
|
|
|
|
|
| and tapering; 25
d |
|
|
|
|
| Annane (2006) | Early | Hyd | 200 mg/d; 7 d | Treatment | 28 d | GC: 54/31 | (14) |
|
|
|
|
|
|
| Control: 67/25 |
|
| Meduri (2007) | Early | MTPS | Single 1 mg/kg | Treatment | Hospital | GC: 15/48 | (7) |
|
|
|
| followed by |
|
| Control: 12/16 |
|
|
|
|
| 1 mg/kg/d for 14
d |
|
|
|
|
|
|
|
| and tapering; 28
d |
|
|
|
|
| Seam (2012) | Early | MTPS | 1 mg/kg/d for 14
d | Treatment | ICU stay | GC: 11/44 | (15) |
|
|
|
| and tapering; 28
d |
|
| Control: 10/14 |
|
| Tongyoo (2016) | Early | Hyd | 50 mg 4/d; 7 d | Treatment | 60 d | GC: 34/64 | (16) |
|
|
|
|
|
|
| Control: 40/59 |
|
A summary of the methodological quality and the
score for each of the trials included is provided in Table III. The studies included in the
meta-analysis scored 7 points on average in the 10-point scoring
system, which was indicative of high quality.
| Table III.Methodological quality assessment for
each of the studies included. |
Table III.
Methodological quality assessment for
each of the studies included.
| First author
(year) | Randomization | Allocation
concealment | Blinding | Inclusion and
exclusion criteria defined | Similar baseline at
study entry | Treatment protocol
clearly described | Cointervention that
may affect outcome | Outcome
definition | Extent of
follow-upclearly described | Intention-to-treat
analysis | Final score | (Refs.) |
|---|
| Weigelt (1985) | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 | (4) |
| Bernard (1987) | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 7 | (11) |
| Luce (1988) | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 6 | (5) |
| Meduri (1998) | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 9 | (12) |
| Confalonieri
(2005) | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 7 | (13) |
| Steinberg
(2006) | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 8 | (6) |
| Annane (2006) | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 6 | (14) |
| Meduri (2007) | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 6 | (7) |
| Seam (2012) | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 7 | (15) |
| Tongyoo (2016) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | (16) |
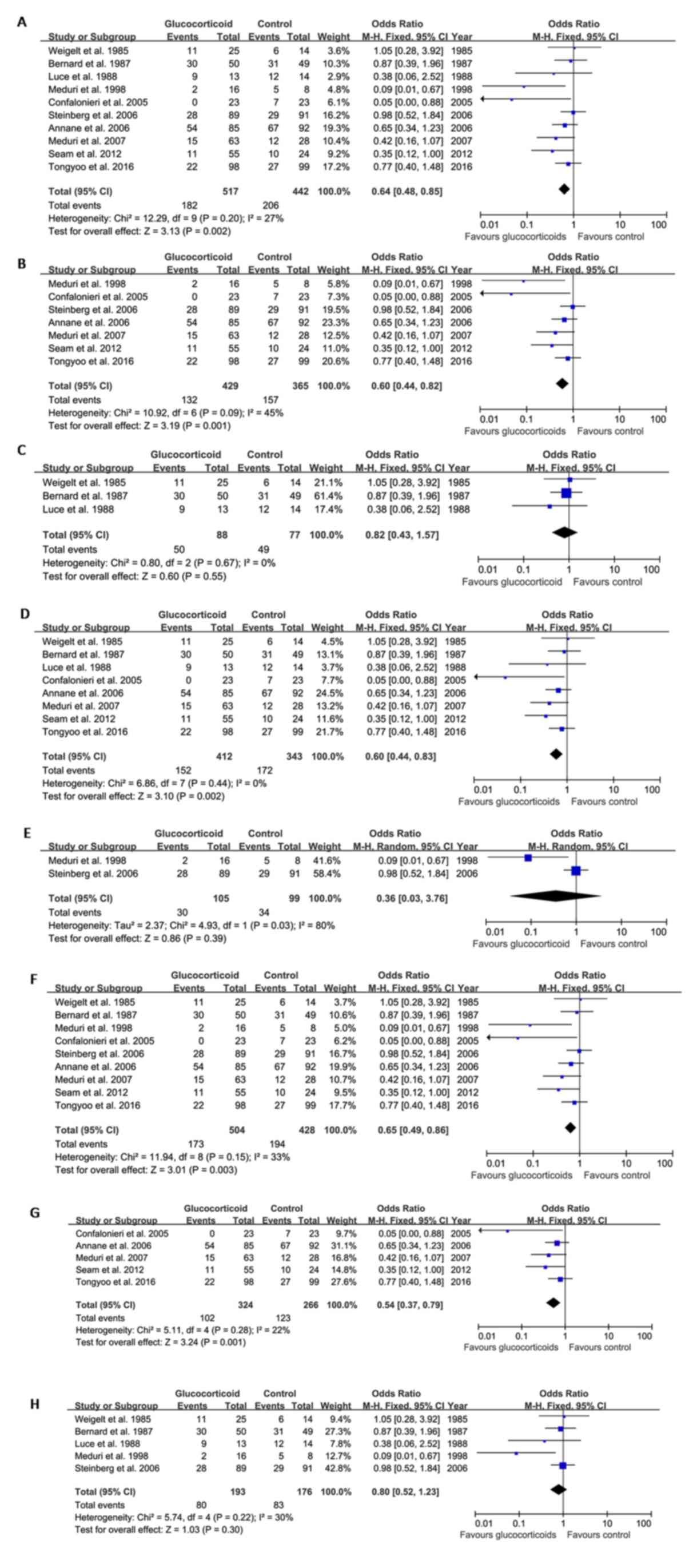
Mortality outcomes
The pooled analysis revealed that glucocorticoid
therapy for ARDS was associated with reduced mortality compared
with the controls. The OR for mortality after glucocorticoid
therapy was 0.64 (95% CI: 0.48–0.85, P=0.002; fixed-effects model)
compared with the control group (Fig.
2A).
Next, subgroup analysis according to the dose,
duration of glucocorticoid therapy and the timing of intervention
were performed. The results indicated that long-term (≥7 d)
low-dose glucocorticoid therapy (40–60 or 1–2 mg/kg/d
methylprednisolone or equivalent) (6,7,12,13,14–16)
reduced ARDS-associated mortality compared with that in the control
group (OR=0.60, 95% CI: 0.44–0.82, P=0.001; fixed-effects model;
Fig. 2B). A total of 3 studies
evaluated short-term (<7 days) high-dose glucocorticoid therapy
(4,5,11) and
the result showed that short-term (<7 days) high-dose
glucocorticoid therapy did not affect ARDS-associated mortality
(OR=0.82, 95% CI: 0.43–1.57, P=0.55; fixed-effects model; Fig. 2C).
Initiation of glucocorticoid therapy in the early
phase of ARDS (within 1 week of diagnosis) significantly reduced
ARDS-associated mortality compared with that in the control group
(OR=0.60, 95% CI: 0.44–0.83, P=0.002; fixed-effects model; Fig. 2D); however, initiation of
glucocorticoid therapy in the later phase of ARDS (>1 week after
diagnosis) had no effect on mortality (OR=0.36, 95% CI: 0.03–3.76,
P=0.39; random-effects model; Fig.
2E).
Preventive use of glucocorticoids in critically ill
patients did not reduce ARDS-associated mortality compared with
that in the control group (5);
however, therapeutic use of glucocorticoids significantly reduced
ARDS-associated mortality (OR=0.65, 95% CI: 0.49–0.86, P=0.003;
fixed-effects model; Fig. 2F).
The effect of combined early initiation, long-term
low dose glucocorticoids on ARDS-associated mortality were next
compared to all other combinations. The pooled analysis results
showed that the combination of early initiation, long-term low dose
glucocorticoids (7,13,14–16)
significantly reduced ARDS-associated mortality (OR=0.54, 95% CI:
0.37–0.79, P=0.001; fixed-effects model; Fig. 2G), whilst all other combinations
(4–6,11,12)
exerts no effects on ARDS-associated mortality (OR=0.80, 95% CI:
0.52–1.23, P=0.30; fixed-effects model; Fig. 2H).
Discussion
ARDS is a common type of organ failure in critically
ill patients and is associated with high morbidity and mortality
(18). Development of effective
therapies for ARDS is an active area of research. Although
lung-protective mechanical ventilation improves outcomes for
patients with ARDS (2), there are
currently pharmacological therapies for ARDS with proven
effectiveness. Considering the pivotal role of acute inflammation
in the pathogenesis of ARDS, several studies have investigated the
use of glucocorticoids in these patients (4,7,13); however, the results were largely
inconsistent. The present meta-analysis suggested that
glucocorticoids reduce ARDS-associated mortality. In particular,
long-term low-dose glucocorticoid therapy, when initiated at an
early stage, was associated with reduced mortality. These results
indicate that glucocorticoids have a promising role in ARDS.
There was much variability between the studies
included with regard to the dosage and duration of glucocorticoid
therapy. In early times, short-term (<7 days) high-dose
glucocorticoids (up to 120 mg/kg/d of methylprednisolone or
equivalent) were typically used to treat or prevent ARDS (4,5,11). For the early studies did not show the
benefit from short-term high-dose glucocorticoids treatment, and
then most studies used low-dose glucocorticoids (40–60 or 1–2
mg/kg/day omethylprednisolone or equivalent) with tapering over a
relatively long period for therapeutic rather than prophylactic
purposes (6,7,12,13,14–16).
Based on the results of the present pooled analysis, long-term
treatment with low-dose glucocorticoid provided a survival benefit,
while short-term treatment at a high dose did not, which is similar
to the results obtained by Meduri et al (19). The reason may be that in ARDS,
inflammation tends to persist for a long time (20); therefore, the long-term use of
glucocorticoids may have a persistent effect on ARDS. On the
contrary, short-term use of high-dose glucocorticoids had no
significant beneficial effect to reduce mortality and was
associated with a high incidence of side effects (4,5,11). Relevant Guidelines of the Society of
Critical Care Medicine and European Society of Intensive Care
Medicine 2017 conditionally recommend the use of methylprednisolone
in early ARDS (up to day 7 of onset) at a dose of 1 mg/kg/d; for
late persistent ARDS (after day 6 of onset), the guidelines
recommend a dose of 2 mg/kg/d followed by gradual tapering
(21).
The timing of initiation of glucocorticoid therapy
for ARDS is another issue of interest. The present results suggest
that glucocorticoid treatment initiation within 1 week of ARDS
onset provided a significant survival benefit, while treatment
initiation at >1 week after ARDS diagnosis did not. This
indicates that the use of glucocorticoids after the stage of
irreversible lung injury may not offer much of a benefit.
Certain studies have explored the preventive
application of glucocorticoids in critically ill patients; the
results suggested that preventive use of glucocorticoids did not
improve ARDS-associated mortality (5,10,13),
while therapeutic use of glucocorticoids, based on the pooled
analysis results, reduced ARDS-associated mortality. It is obvious
that an adequate inflammatory response in critically ill patients,
particularly in infection patients, helps to eliminate invading
pathogens; therefore, use of glucocorticoids in this phase may lead
to adverse effects (22). However,
when acute lung inflammation has progressed to ARDS, the use of
glucocorticoids appears to provide a benefit by reducing excessive
inflammation and the associated tissue injury.
The present meta-analysis has various limitations
that should be considered. First, the studies included in the
meta-analysis spanned >20 years. With advances in intensive care
medicine, various novel techniques and therapeutic strategies have
been developed, including lung-protective ventilation strategy and
extracorporeal membrane oxygenation; these are likely to have had
an impact on the mortality rate of patients with ARDS. Furthermore,
although the studies included reported on in-hospital mortality
data, the mortality end-points were not identical among the
different studies since they either ICU or hospital mortality were
also assessed; this may have introduced an element of bias. In
addition, there are several etiological factors of ARDS, including
infection, trauma, major operations and sepsis, and ARDS induced by
different etiologic factors may be classified into different
subphenotypes (23), which may
influence the therapeutic response. However, based on the present
results, it is impossible to identify any sub-groups of patients
that are likely to benefit from glucocorticoid therapy. Finally,
the effect of glucocorticoids on the long-term prognosis of
patients with ARDS (>6 months) is uncertain due to the
relatively short duration of follow-up in most studies.
Overall, the present study suggested that early
initiation of low-dose glucocorticoids with long-term
administration reduces ARDS-associated mortality. Further
well-designed prospective trials are required to provide
recommendations for glucocorticoid use in ARDS subpopulations.
Acknowledgements
The authors would like to thank Professor Yi Shi
from the Department of Pulmonary and Critical Care Medicine,
Clinical School of Nanjing University (Nanjing, China) for the
valuable discussion regarding the statistical analysis.
Funding
The present study was supported by the Six Talent
Peaks Project of Jiangsu Province (grant no. 2019-SWYY-324),
Jiangsu Province Key Medical Talents Program (grant no.
QNRC2016504), Jiangsu Provincial Health and Family Planning
Commission Science Foundation (grant no. H201558) and the
Lianyungang Science and Technology Bureau Foundation (grant no.
SH1401).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
QZ, JXS and JSL conceived and designed the present
study. RH, QL and CYZ performed data extraction. JXS and JSL
ensured the quality of the data. QZ and QL analyzed the data. QZ,
JXS and RH drafted the manuscript. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Leaver SK and Evans TW: Acute respiratory
distress syndrome. BMJ. 335:389–394. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Acute Respiratory Distress Syndrome
Network, ; Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson
BT and Wheeler A: Ventilation with lower tidal volumes as compared
with traditional tidal volumes for acute lung injury and the acute
respiratory distress syndrome. N Engl J Med. 342:1301–1308. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Boyle AJ, Mac Sweeney R and McAuley DF:
Pharmacological treatments in ARDS; a state-of-the-art update. BMC
Med. 11:1662013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Weigelt JA, Norcross JF, Borman KR and
Snyder WH III: Early steroid therapy for respiratory failure. Arch
Surg. 120:536–540. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Luce JM, Montgomery AB, Marks JD, Turner
J, Metz CA and Murray JF: Ineffectiveness of high-dose
methylprednisolone in preventing parenchymal lung injury and
improving mortality in patients with septic shock. Am Rev Respir
Dis. 138:62–68. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Steinberg KP, Hudson LD, Goodman RB, Hough
CL, Lanken PN, Hyzy R, Thompson BT and Ancukiewicz M; National
Heart, Lung, and Blood Institute Acute Respiratory Distress
Syndrome (ARDS) Clinical Trials Network, : Efficacy and safety of
corticosteroids for persistent acute respiratory distress syndrome.
The New England journal of medicine. 354:1671–1684. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Meduri GU, Golden E, Freire AX, Taylor E,
Zaman M, Carson SJ, Gibson M and Umberger R: Methylprednisolone
infusion in early severe ARDS: Results of a randomized controlled
trial. Chest. 131:954–963. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Peter JV, John P, Graham PL, Moran JL,
George IA and Bersten A: Corticosteroids in the prevention and
treatment of acute respiratory distress syndrome (ARDS) in adults:
meta-analysis. BMJ. 336:1006–1009. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bone RC, Fisher CJ Jr, Clemmer TP, Slotman
GJ and Metz CA: Early methylprednisolone treatment for septic
syndrome and the adult respiratory distress syndrome. Chest.
92:1032–1036. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bernard GR, Luce JM, Sprung CL, Rinaldo
JE, Tate RM, Sibbald WJ, Kariman K, Higgins S, Bradley R, Metz CA,
et al: High-dose corticosteroids in patients with the adult
respiratory distress syndrome. N Engl J Med. 317:1565–1570. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Meduri GU, Headley AS, Golden E, Carson
SJ, Umberger RA, Kelso T and Tolley EA: Effect of prolonged
methylprednisolone therapy in unresolving acute respiratory
distress syndrome: A randomized controlled trial. JAMA.
280:159–165. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Confalonieri M, Urbino R, Potena A,
Piattella M, Parigi P, Puccio G, Della Porta R, Giorgio C, Blasi F,
Umberger R and Meduri GU: Hydrocortisone infusion for severe
community- acquired pneumonia: A preliminary randomized study. Am J
Respir Crit Care Med. 171:242–248. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Annane D, Sébille V and Bellissant E;
Ger-Inf-05 Study Group, : Effect of low doses of corticosteroids in
septic shock patients with or without early acute respiratory
distress syndrome. Crit Care Med. 34:22–30. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Seam N, Meduri GU, Wang H, Nylen ES, Sun
J, Schultz MJ, Tropea M and Suffredini AF: Effects of
methylprednisolone infusion on markers of inflammation,
coagulation, and angiogenesis in early acute respiratory distress
syndrome. Crit Care Med. 40:495–501. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tongyoo S, Permpikul C, Mongkolpun W,
Vattanavanit V, Udompanturak S, Kocak M and Meduri GU:
Hydrocortisone treatment in early sepsis-associated acute
respiratory distress syndrome: Results of a randomized controlled
trial. Crit Care. 20:3292016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
ARDS Definition Task Force, ; Ranieri VM,
Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E,
Camporota L and Slutsky AS: Acute respiratory distress syndrome:
The Berlin definition. JAMA. 307:2526–2533. 2012.PubMed/NCBI
|
|
18
|
Vincent JL, Akça S, De Mendonça A,
Haji-Michael P, Sprung C, Moreno R, Antonelli M and Suter PM; SOFA
Working Group. Sequntial organ failure assessment, : The
epidemiology of acute respiratory failure in critically ill
patients(*). Chest. 121:1602–1609. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Meduri GU, Bridges L, Shih MC, Marik PE,
Siemieniuk RAC and Kocak M: Prolonged glucocorticoid treatment is
associated with improved ARDS outcomes: Analysis of individual
patients' data from four randomized trials and trial-level
meta-analysis of the updated literature. Intensive Care Med.
42:829–840. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Meduri GU, Muthiah MP, Carratu P, Eltorky
M and Chrousos GP: Nuclear factor-kappaB- and glucocorticoid
receptor alpha- mediated mechanisms in the regulation of systemic
and pulmonary inflammation during sepsis and acute respiratory
distress syndrome. Evidence for inflammation-induced target tissue
resistance to glucocorticoids. Neuroimmunomodulation. 12:321–338.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Annane D, Pastores SM, Rochwerg B, Arlt W,
Balk RA, Beishuizen A, Briegel J, Carcillo J, Christ-Crain M,
Cooper MS, et al: Guidelines for the diagnosis and management of
critical illness-related corticosteroid insufficiency (CIRCI) in
critically Ill patients (Part I): Society of Critical Care Medicine
(SCCM) and European Society of Intensive Care Medicine (ESICM)
2017. Crit Care Med. 45:2078–2088. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Snijders D, Daniels JM, de Graaff CS, van
der Werf TS and Boersma WG: Efficacy of corticosteroids
incommunity-acquired pneumonia: A randomized double-blinded
clinical trial. Am J Respir Crit Care Med. 181:975–982. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Calfee CS, Delucchi K, Parsons PE,
Thompson BT, Ware LB and Matthay MA; NHLBI ARDS Network, :
Subphenotypes in acute respiratory distress syndrome: Latent class
analysis of data from two randomised controlled trials. Lancet
Respir Med. 2:611–620. 2014. View Article : Google Scholar : PubMed/NCBI
|