Introduction
Lesions of the long head of the biceps (LHB) tendon
have been widely considered to be a notable trigger for anterior
shoulder pain (1). Patients with
mild symptoms of tendinopathy or partial LHB tears (<50% of
tendon width), non-surgical treatments, such as rest, physical
therapy, non-steroidal anti-inflammatory drug treatment and
intra-articular injection of corticosteroids, can be effective;
however, for most cases, including partial-thickness LHB tears, LHB
instability/subluxation, associated rotator cuff tears, biceps
pulley lesions and superior labrum anterior-posterior (SLAP)
lesions, surgical intervention is still the preferred method of
treatment (2–4). Biceps tenotomy and tenodesis have
become two of the most commonly performed surgical procedures for
lesions of the LHB tendons (5).
Although tenotomy is a relatively simple and reproducible procedure
which can significantly relieve shoulder pain without postoperative
rehabilitation, it is only indicated for patients aged over 60
years, who are not involved in heavy labor and high-demand
activities (6). Moreover, tenotomy
has a higher incidence of cosmetic deformity (Popeye sign) than
that of tenodesis (43 vs. 8%) (7).
Therefore, tenodesis is currently the preferred technique for
treating LHB lesions as it provides a better recovery of physical
activity, fewer cosmetic deformities and more closely aligns with
normal anatomy, despite a longer postoperative rehabilitation time
and higher technical demand (8).
Numerous techniques have been applied with LHB
tenodesis, including arthroscopic techniques and minimally open or
open surgeries (9). Moreover,
tenodesis sites can be positioned in the suprapectoral location
just proximal to the pectoralis major tendon, the subpectoral
location, or other positions such as the conjoint tendon or soft
tissue sites (10). Although
comparably preferable clinical outcomes have been reported in
various studies investigating both open subpectoral biceps
tenodesis (OSPBT) and arthroscopic suprapectoral biceps tenodesis
(ASPBT), the results are still controversial and there is limited
information regarding postoperative complications, such as
re-tears, implant failure, nerve and vascular injuries, bicipital
groove tenderness, deformities, and postoperative infection and
stiffness (11,12).
The present study retrospectively investigated 117
cases who underwent LHB tenodesis. OSPBT and ASPBT were compared,
including pre-/post-surgery shoulder range of motion (ROM), visual
analog scale (VAS) scores, American Shoulder and Elbow Surgeons
(ASES) scores, Constant-Murley shoulder outcome scores and
postoperative complications. The purpose of the present study was
to identify the differences in clinical outcomes and related
complications between OSPBT and ASPBT.
Materials and methods
Study design and patients
This retrospective, single-center study was
performed based on a protocol approved by the institutional review
board at The First Affiliated Hospital of Anhui Medical University
(Hefei, China), and was in accordance with the Good Clinical
Practice guidelines (13) and the
principles of the Declaration of Helsinki. Medical records of adult
patients who had received LHB tenodesis surgeries at the Department
of Orthopedics, The First Affiliated Hospital of Anhui Medical
University between January 2015 and June 2016 were reviewed
(n=259). The inclusion criteria were as follows: The diagnosis of
SLAP tears; complete or partial tearing of the LHB; biceps lesions
(tenosynovitis); and LHB instability/subluxation or associated
rotator cuff tears (small- or medium-sized). Additionally, the
inclusion criteria also included the presence of LHB lesion
symptoms and signs, such as anterior shoulder pain, bicipital
groove tenderness and positive results from the Speeds, Yergason's
and O'Brien's tests; conservative treatments for at least 3 months;
complete clinical evaluations and MRI scans; and followed up for
more than 12 months. The exclusion criteria were as follows:
Patients <18 years old; glenoid labrum lesions; glenohumeral
instability; preoperative ROM deficit due to frozen shoulder or
glenohumeral arthritis; contralateral shoulder injury or surgery;
shoulder arthroplasty; massive rotator cuff tear; and neuromuscular
disorder-related shoulder pain.
Grouping and treatments
A total of 117 patients (60 women and 57 men) who
met the inclusion and exclusion criteria were enrolled in this
study and randomly divided into two groups, the OSPBT group (n=62)
and the ASPBT group (n=55). All tenodesis procedures (OSPBT and
ASPBT) were performed by the same group of experienced orthopedic
surgeons at The First Affiliated Hospital of Anhui Medical
University. The choice of surgical technique was determined by
surgeon preference.
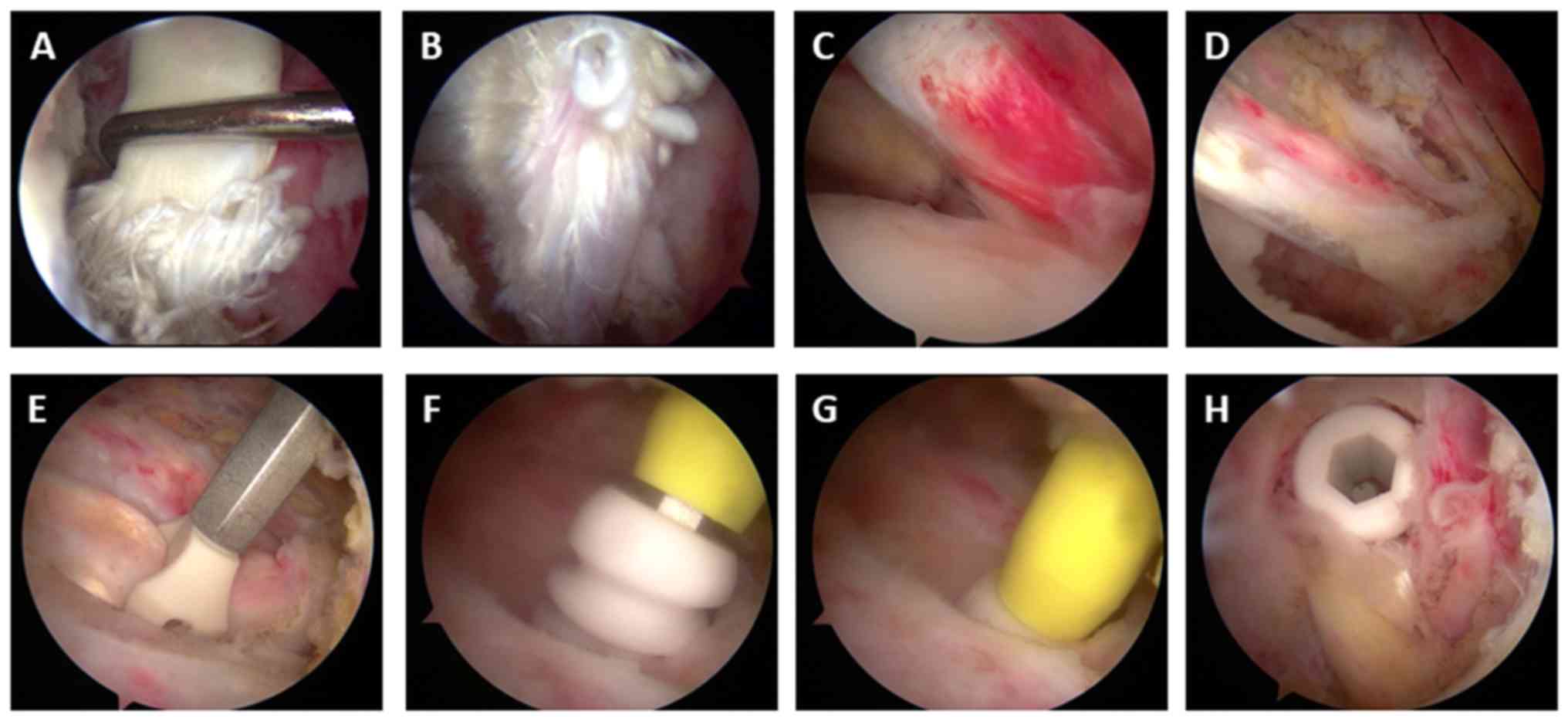
Surgical technique and
rehabilitation
OSPBT was performed using the surgical technique
described by Mazzocca et al (14). After positioning the upper arm in the
external rotation position, the inferior margin of the pectoralis
major was palpated and a 2–3 cm incision was made near the inferior
margin of the pectoralis major in the axillary region. A Hohmann
retractor was placed under the pectoralis major and a Chandler
retractor was placed over the medial side of the humerus to enlarge
the operative visual field. Subsequently, the LHB was isolated and
extracted from the glenohumeral joint and LHB sheath by using a
right-angle clamp (Fig. 1). The end
of the LHB (3–4 cm) was removed and the terminal 3 cm of the tendon
was stitched using a no. 2 high-strength suture. An appropriately
sized interference screw implant (7 mm interference bio-screw;
Arthrex GmbH) was used to affix the tendon into the reamed
tenodesis site.
ASPBT was performed according to previously reported
surgical techniques (15,16). After positioning the upper arm in the
external rotation position, a probe was used to locate the major
tubercle and medial side of the intertubercular groove. The
arthroscope was repositioned into the lateral portal and the biceps
tendon was identified in the sheath within the intertubercular
groove. As shown in Fig. 2,
coblation was then used to release the biceps tendon from the
sheath and an appropriate position for tenodesis was localized
proximal to the pectoralis major tendon. Subsequently, a portal was
established at this location and a guide wire was placed. A 7.5 mm
reamer was drilled in the center of intertubercular groove to the
appropriate depth. A polydioxanone suture was used to stabilize the
proximal tendon and the Swivelock screw (Arthrex GmbH) was then
used to affix the tendon into the reamed tenodesis site. A
postoperative X-ray examination was performed to identify the
position (Fig. 3).
Both treatment groups received the same
postoperative rehabilitation program. In general, only passive
exercises were performed in the first 6 weeks. Thereafter,
active-assisted ROM and active exercises were permitted for the
subsequent 6 weeks. From the 13th week, patients could begin biceps
strengthening exercises. Specifically, for patients with rotator
cuff tears and LHB lesions, the wounded shoulder was fixed with an
abduction brace for 4 weeks and only passive exercises of elbow
joints could be performed for the first 2 of these 4 weeks.
Thereafter, passive exercises of the shoulder joints were allowed.
For patients without rotator cuff tears, the wounded shoulder was
fixed with an abduction brace for 2 weeks and only passive
exercises of the shoulder and elbow joints were performed during
the first 6 weeks.
Demographic characteristics and
clinical examinations
The demographics of each patient were recorded in
detail, including the age, sex, body mass index (BMI), smoking
history, dominant shoulder, duration of pain, injury types,
operation time and hospital stay. Moreover, clinical examinations
of LHB lesions such as shoulder ROM, VAS scores (0, no pain, to 10,
most severe pain), ASES scores and Constant-Murley shoulder outcome
scores (Constant scores) were investigated preoperatively, as well
as at 3, 6 and 12 months post-surgery. All patients received at
least 12 months follow-up care after hospital discharge and the
patients were advised to attend the associated outpatient clinic to
complete these clinical assessments during this period. A total of
12 months following the surgery, the patients were contacted for
follow-up using a telephone enquiry investigating abnormal signs of
pain, instability or deformity, as had been mutually agreed. All
patients were invited to the associated outpatient clinic if any
abnormal signs appeared. Comprehensive evaluations and imaging
examinations were performed to clarify the injury types and
degrees. Furthermore, postoperative complications, including
re-tears, implant failure, nerve and vascular injuries, bicipital
groove tenderness, deformities (Popeye sign), postoperative
infection and stiffness were comprehensively investigated.
Statistical analysis
Statistical analysis was performed using SPSS
software (version 19.0; IBM Corp.). The results are presented as
the mean ± SD. Student's t-test and one/two-way ANOVAs were applied
for continuous data, with Bonferroni post-hoc tests. χ2
tests were applied for the categorical data. P<0.05 was
considered to indicate a statistically significant difference.
Results
Demographic characteristics
A total of 117 adult patients (60 women and 57 men)
with LHB lesions who met the inclusion and exclusion criteria were
enrolled in the present study and divided into two groups, the
OSPBT group (n=62) and the ASPBT group (n=55). The mean age of all
117 patients was 56.51±8.79 years (range, 32–78 years) and there
were no significant differences in the mean ages between the OSPBT
group (57.36±8.81 years old) and the ASPBT group (55.05±8.74 years
old) (P>0.05). As shown in Table
I, there were no significant differences in gender, BMI,
dominant shoulder, duration of pain, injury type and operation time
between the two groups. The mean number of days of hospital stay in
the ASPBT group was significantly lower than that in the OSPBT
group (5.4±1.8 vs. 9.3±2.9 days; P<0.05). All patients had
completed at least 12 months of follow-up and the mean lengths of
follow-up treatment in the OSPBT group and the ASPBT group were
20.11±7.10 and 20.51±7.47 months, respectively. A total of 34
patients abandoned the follow-up study after 12 months, including
18 patients from the OSPBT group and 16 patients from the ASPBT
group.
 | Table I.Demographic characteristics of
patients in the OSPBT group and the ASPBT group. |
Table I.
Demographic characteristics of
patients in the OSPBT group and the ASPBT group.
| Variable | OSPBT (n=62) | ASPBT (n=55) | P-value |
|---|
| Age, years | 57.36±8.81 | 55.05±8.74 | 0.64 |
| Female, n (%) | 33 (53.2%) | 29 (52.7%) | 0.85 |
| BMI,
kg/m2 | 28.38±2.69 | 28.77±2.41 | 0.39 |
| Smoking, n (%) | 9
(14.5%) | 7
(12.7%) | 0.72 |
| Dominant
shoulder |
|
|
|
| Right, n
(%) | 38 (61.3%) | 34 (61.8%) | 0.81 |
| Duration of pain,
months | 16.16±7.77 | 15.74±7.79 | 0.65 |
| Injury types, n
(%) |
|
|
|
| SLAP
tear | 30 (48.4%) | 20 (36.4%) | 0.14 |
| Biceps
tear | 37 (59.7%) | 32 (58.2%) | 0.74 |
|
Tenosynovitis | 9
(14.5%) | 5 (9.1%) | 0.21 |
| LHB
subluxation | 18 (29.0%) | 15 (27.3%) | 0.53 |
| Rotator
cuff tear | 55 (88.7%) | 46 (83.6%) | 0.48 |
|
Small-sized | 26 (41.9%) | 21 (38.2%) | 0.51 |
|
Medium-sized | 29 (46.8%) | 25 (45.5%) | 0.24 |
| Operation time,
h |
2.63±0.63 |
3.12±0.75 | 0.09 |
| Hospital stay,
days |
9.3±2.9 |
5.4±1.8 | 0.03 |
| Follow-up,
months | 20.11±7.10 | 20.51±7.47 | 0.78 |
Clinical examinations
The clinical examinations, including VAS scores,
Constant scores and ASES scores were taken preoperatively, as well
as 3, 6 and 12 months post-surgery. VAS scores (0, no pain, to 10,
most severe pain) were applied for evaluating shoulder pain. As
shown in Table II, the VAS scores
in both groups at 3, 6 and 12 months post-surgery were
significantly lower than the VAS scores of both groups
preoperatively (P<0.05). At 3 months post-surgery, the VAS score
in OSPBT group (2.41±0.76) was significantly lower than that in the
ASPBT group (3.59±1.02; P<0.05). Moreover, there were no
significant differences in the VAS scores between the OSPBT group
and the ASPBT group preoperatively, at 6 or 12 months post-surgery
(P>0.05). The average Constant scores and ASES scores between
the two groups are also presented in Table II. The Constant scores and ASES
scores of both groups at 3, 6 and 12 months post-surgery were
significantly higher than the respective scores preoperatively in
both groups (P<0.05). However, there were no significant
differences observed in the Constant scores and ASES scores between
the OSPBT group and the ASPBT group at any stage of the study
(P>0.05).
| Table II.Clinical examinations of patients in
the OSPBT group and the ASPBT group. |
Table II.
Clinical examinations of patients in
the OSPBT group and the ASPBT group.
| Variable | OSPBT | ASPBT |
|---|
| VAS score |
|
|
|
Preoperative | 5.02±1.05 | 4.92±1.51 |
| 3
months postoperatively |
2.41±0.76a,b |
3.59±1.02a |
| 6
months postoperatively |
1.64±0.81a |
1.77±0.81a |
| 12
months postoperatively |
0.95±0.65a |
1.18±1.36a |
| Constant score |
|
|
|
Preoperative | 53.75±7.19 | 52.08±10.54 |
| 3
months postoperatively |
63.25±7.01a |
60.61±6.39a |
| 6
months postoperatively |
81.16±6.32a |
78.64±5.14a |
| 12
months postoperatively |
90.71±4.29a |
90.38±3.14a |
| ASES score |
|
|
|
Preoperative | 52.89±8.16 | 49.51±11.05 |
| 3
months postoperatively |
68.39±3.98a |
64.84±4.07a |
| 6
months postoperatively |
80.52±5.93a |
78.36±5.53a |
| 12
months postoperatively |
89.05±4.02a |
88.51±3.42a |
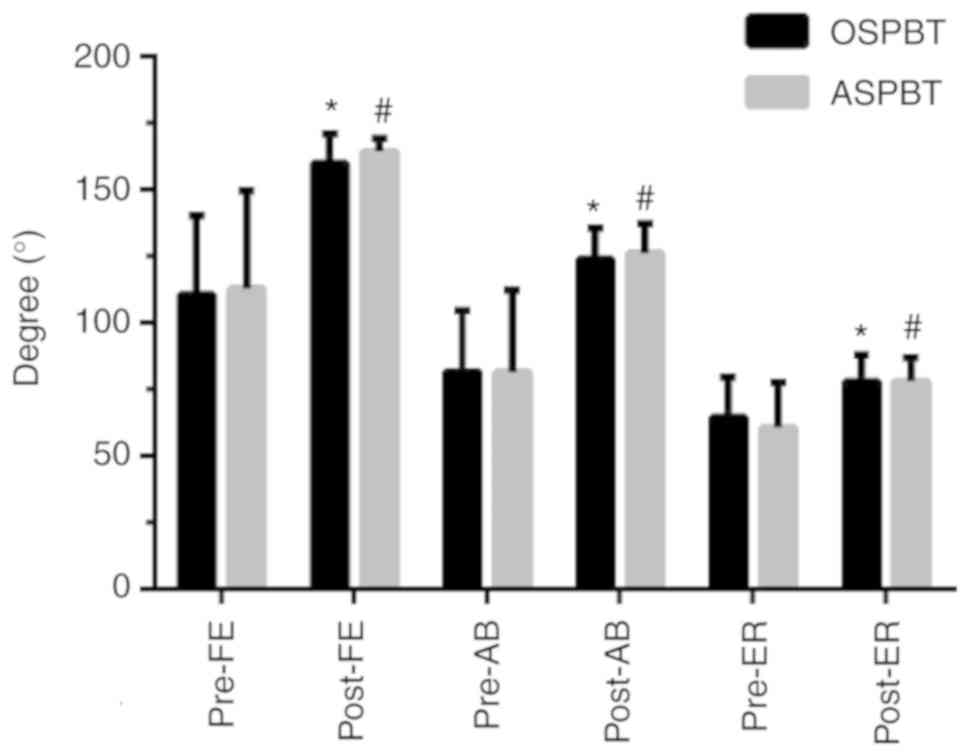
ROM
The active ROMs, including forward elevation,
abduction and external rotation, were evaluated preoperatively and
at 12 months post-surgery. As shown in Fig. 4, the postoperative active ROMs were
significantly higher than the preoperative active ROMs in both
groups (P<0.05). However, there were no significant differences
in the preoperative or postoperative active ROMs between the two
groups (P>0.05).
Postoperative complications
The postoperative complications, including re-tears,
deformities (Popeye sign), implant failure, neurovascular injury,
postoperative infection, stiffness and bicipital groove tenderness,
were comprehensively investigated. As shown in Table III, there were no incidences of
re-tears, deformities (Popeye sign), implant failure, neurovascular
injury or postoperative infection. Moreover, the incidence of
postoperative stiffness in the OSPBT group (3, 5.5%) was
significantly lower than that in the ASPBT group (11, 17.7%;
P<0.05). Furthermore, the incidences of bicipital groove
tenderness in both two groups at 3, 6 and 12 months post-surgery
were significantly lower than the incidences of bicipital groove
tenderness in both groups on discharge day (P<0.05). At 3 months
post-surgery, the incidence of bicipital groove tenderness in OSPBT
group (10, 16.1%) was significantly lower than that in ASPBT group
(23, 41.8%; P<0.05). Similarly, at 6 months post-surgery, the
incidence of bicipital groove tenderness in the OSPBT group (4,
6.4%) was significantly lower than that in the ASPBT group (12,
21.8%; P<0.05). However, there was no significant difference in
the incidences of bicipital groove tenderness between the OSPBT
group and the ASPBT group at 12 months post-surgery
(P>0.05).
| Table III.Postoperative complications of
patients in the OSPBT group and the ASPBT group. |
Table III.
Postoperative complications of
patients in the OSPBT group and the ASPBT group.
| Variable | OSPBT (%) | ASPBT(%) |
|---|
| Re-tears, n
(%) | 0 (0) | 0 (0) |
| Popeye sign, n
(%) | 0 (0) | 0 (0) |
| Implant failure, n
(%) | 0 (0) | 0 (0) |
| Neurovascular
injury, n (%) | 0 (0) | 0 (0) |
| Postoperative
infection, n (%) | 0 (0) | 0 (0) |
| Stiffness, n
(%) | 3
(5.5)b | 11 (17.7) |
| Bicipital groove
tenderness, n (%) |
|
Discharge day | 39 (62.9) | 37 (67.3) |
| 3
months postoperatively | 10
(16.1)a,b | 23
(41.8)a |
| 6
months postoperatively | 4
(6.4)a,b | 12
(21.8)a |
| 12
months postoperatively | 0 (0)a | 3
(5.4)a |
Discussion
In recent years, various techniques regarding LHB
tenodesis have been reported, and among them, bony interference
fixation tenodesis (BIFT) is the most widely used technique,
exhibiting good clinical outcomes and a low rate of surgical
complications (9,17). Furthermore, soft tissue fixation
(STT) is associated with excellent performance, without producing
subscapular lesions or Popeye's deformity (18). Hwang et al (19) suggested that arthroscopic BIFT at the
distal bicipital groove produced a greater improvement in the elbow
flexion strength index and a lower failure rate than STT. Chiang
et al (20) investigated the
biomechanical characteristics of suture anchor and interference
screw fixation in subpectoral tenodesis, and reported that both of
the techniques led to an equivalent ultimate failure load and
stiffness. However, the interference screw fixation technique was
associated with significantly less displacement in response to
cyclic and failure loading.
In regards to the safety of tenodesis, brachial
plexopathy (21), musculocutaneous
nerve injury and lateral antebrachial cutaneous nerve injury
(22,23) have been reported after OSPBT. Ma
et al (24) reported a case
of direct musculocutaneous nerve injury in subpectoral tenodesis,
whereby the nerve was wrapped around the LHB in the revision
surgery. Sethi et al (25)
assessed the risk for neurological injury of open suprapectoral and
subpectoral biceps tenodesis in cadavers, and suggested that
penetration of the posterior humeral cortex at the suprapectoral
location results in a high risk of damaging the axillary nerve due
to its proximity, and should be avoided. Subpectoral bicortical
button fixation drilled uniformly perpendicular to the axis of the
humerus is performed in a safe location with respect to the
axillary nerve. In this present study, it was found that the
incidences of postoperative complications, such as re-tears,
deformities (Popeye sign), implant failure, neurovascular injury
and postoperative infection, were nil. Therefore, both
suprapectoral and subpectoral tenodesis were deemed safe.
The results showed that the clinical outcomes,
including shoulder ROMs, VAS scores, ASES scores and Constant
scores, were significantly improved after OSPBT or ASPBT. Moreover,
there were no significant differences in the improvement of
clinical outcomes between the two groups. However, Gilmer et
al (26) suggested that only 17%
length of LHB tendon can be observed in ASPBT, and only 32% length
of LHB can be observed in ASPBT even when the tendon is pulled into
the joint with an arthroscopic grasper. This indicated that OSPBT
may be the optimal method of tenodesis for the complete removal of
all hidden biceps lesions and for the revision of failed
postoperative LHB lesions (27).
Kolz et al (28) compared the
mechanical properties between OSPBT and ASPBT, and indicated that
LHB in the suprapectoral region tended to have higher tensile
strength than in the subpectoral region, and LHB tenodesis in the
suprapectoral region could withstand higher failure loads and
become more arthroscopically accessible. Furthermore, this present
study found that the incidences of postoperative stiffness and
bicipital groove tenderness in the ASPBT group were significantly
higher than those in the OSPBT group. It was also reported that the
VAS score in the OSPBT group was significantly lower than that in
the ASPBT group at 3 months post-surgery. Similarly, Yi et
al (29) suggested that VAS
scores and tenderness at the bicipital groove were significantly
decreased in the OSPBT group at the early stage post-surgery.
However, there were no significant differences in ASES and Constant
scores in this present study. This indicated that the early results
of VAS score (within 3 months post-surgery) and bicipital groove
tenderness (within 6 months post-surgery) for subpectoral tenodesis
was related to the removal of the biceps tendinitis.
There were several limitations with this study,
including: An insufficient number of enrolled patients; the absence
of extended follow-up research; a lack of MRI data from enrolled
patients preoperatively and postoperatively, especially MRI changes
during the follow-up; and the study was not a prospective,
randomized controlled trial.
In conclusion, the clinical outcomes, including
shoulder ROMs, VAS scores, ASES scores and Constant scores, were
significantly improved after OSPBT or ASPBT. Specifically, the VAS
score, and the incidences of postoperative stiffness and bicipital
groove tenderness in the OSPBT group were significantly lower than
those in the ASPBT group at 3 months post-surgery. Moreover, there
were no significant differences in the improvement of other
clinical outcomes and postoperative complications between the two
groups.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets generated and/or analyzed during the
current study are not publicly available due to statutory
provisions regarding data and privacy protection but are available
from the corresponding author on reasonable request.
Authors' contributions
JT, BX and RG were involved in the conception and
design of the study; the collection, assembly, analysis and
interpretation of the data; and in drafting of the article. They
also provided statistical expertise and contributed to the final
approval of the article, provision of study materials, technical
and logistical support as well as critical revision of the article
for important intellectual content. All authors contributed equally
to this article.
Ethics approval and consent to
participate
This study was approved by the ethics committee of
The First Affiliated Hospital of Anhui Medical University (protocol
no. PJ2014-10-04). Participants provided their written informed
consent to participate in this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nair R, Kahlenberg CA, Patel RM, Knesek M
and Terry MA: All-arthroscopic suprapectoral biceps tenodesis.
Arthrosc Tech. 4:e855–e861. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Werner BC, Brockmeier SF and Gwathmey FW:
Trends in long head biceps tenodesis. Am J Sports Med. 43:570–578.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Levy DM, Meyer ZI, Campbell KA and Bach BR
Jr: Subpectoral biceps tenodesis. Am J Orthop (Belle Mead NJ).
45:68–74. 2016.PubMed/NCBI
|
|
4
|
AlQahtani SM and Bicknell RT: Outcomes
following long head of biceps tendon tenodesis. Curr Rev
Musculoskelet Med. 9:378–387. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Patel KV, Bravman J, Vidal A, Chrisman A
and McCarty E: Biceps tenotomy versus tenodesis. Clin Sports Med.
35:93–111. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Koh KH, Ahn JH, Kim SM and Yoo JC:
Treatment of biceps tendon lesions in the setting of rotator cuff
tears: Prospective cohort study of tenotomy versus tenodesis. Am J
Sports Med. 38:1584–1590. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Slenker NR, Lawson K, Ciccotti MG, Dodson
CC and Cohen SB: Biceps tenotomy versus tenodesis: Clinical
outcomes. Arthroscopy. 28:576–582. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Werner BC, Evans CL, Holzgrefe RE, Tuman
JM, Hart JM, Carson EW, Diduch DR, Miller MD and Brockmeier SF:
Arthroscopic suprapectoral and open subpectoral biceps tenodesis: A
comparison of minimum 2-year clinical outcomes. Am J Sports Med.
42:2583–2590. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abraham VT, Tan BH and Kumar VP:
Systematic review of biceps tenodesis: Arthroscopic versus open.
Arthroscopy. 32:365–371. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Werner BC, Lyons ML, Evans CL, Griffin JW,
Hart JM, Miller MD and Brockmeier SF: Arthroscopic suprapectoral
and open subpectoral biceps tenodesis: A comparison of restoration
of length-tension and mechanical strength between techniques.
Arthroscopy. 31:620–627. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chung SW, Huong CB, Kim SH and Oh JH:
Shoulder stiffness after rotator cuff repair: Risk factors and
influence on outcome. Arthroscopy. 29:290–300. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Johannsen AM, Macalena JA, Carson EW and
Tompkins M: Anatomic and radiographic comparison of arthroscopic
suprapectoral and open subpectoral biceps tenodesis sites. Am J
Sports Med. 41:2919–2924. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Grimes DA, Hubacher D, Nanda K, Schulz KF,
Moher D and Altman DG: The good clinical practice guideline: A
bronze standard for clinical research. Lancet. 366:172–174. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mazzocca AD, Rios CG, Romeo AA and Arciero
RA: Subpectoral biceps tenodesis with interference screw fixation.
Arthroscopy. 21:8962005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
David TS and Schildhorn JC: Arthroscopic
suprapectoral tenodesis of the long head biceps: Reproducing an
anatomic length-tension relationship. Arthrosc Tech. 1:e127–e132.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lutton DM, Gruson KI, Harrison AK,
Gladstone JN and Flatow EL: Where to tenodese the biceps: Proximal
or distal? Clin Orthop Relat Res. 469:1050–1055. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tahal DS, Katthagen JC, Vap AR, Horan MP
and Millett PJ: Subpectoral biceps tenodesis for tenosynovitis of
the long head of the biceps in active patients younger than 45
years old. Arthroscopy. 33:1124–1130. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Baggio M, Martinelli F, Netto MB, Martins
RO, da Cunha RC and Stipp WN: Evaluation of the results from
arthroscopic tenodesis of the long head of the biceps brachii on
the tendon of the subscapularis muscle. Rev Bras Ortop. 51:157–162.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hwang JT, Yang CJ, Noh KC, Yoo YS, Hyun
YS, Lee YB and Liu X: Which is better for arthroscopic tenodesis of
the long head of the biceps: Soft tissue or bony interference
fixation? Arthroscopy. 32:560–567. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chiang FL, Hong CK, Chang CH, Lin CL, Jou
IM and Su WR: Biomechanical comparison of all-suture anchor
fixation and interference screw technique for subpectoral biceps
tenodesis. Arthroscopy. 32:1247–1252. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gombera MM, Kahlenberg CA, Nair R,
Saltzman MD and Terry MA: All-arthroscopic suprapectoral versus
open subpectoral tenodesis of the long head of the biceps brachii.
Am J Sports Med. 43:1077–1083. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rhee PC, Spinner RJ, Bishop AT and Shin
AY: Iatrogenic brachial plexus injuries associated with open
subpectoral biceps tenodesis: A report of 4 cases. Am J Sports Med.
41:2048–2053. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
McCormick F, Nwachukwu BU, Solomon D,
Dewing C, Golijanin P, Gross DJ and Provencher MT: The efficacy of
biceps tenodesis in the treatment of failed superior labral
anterior posterior repairs. Am J Sports Med. 42:820–825. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ma H, Van Heest A, Glisson C and Patel S:
Musculocutaneous nerve entrapment: An unusual complication after
biceps tenodesis. Am J Sports Med. 37:2467–2469. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sethi PM, Vadasdi K, Greene RT, Vitale MA,
Duong M and Miller SR: Safety of open suprapectoral and subpectoral
biceps tenodesis: An anatomic assessment of risk for neurologic
injury. J Shoulder Elbow Surg. 24:138–142. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gilmer BB, DeMers AM, Guerrero D, Reid JB
III, Lubowitz JH and Guttmann D: Arthroscopic versus open
comparison of long head of biceps tendon visualization and
pathology in patients requiring tenodesis. Arthroscopy. 31:29–34.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Euler SA, Horan MP, Ellman MB, Greenspoon
JA and Millett PJ: Chronic rupture of the long head of the biceps
tendon: Comparison of 2-year results following primary versus
revision open subpectoral biceps tenodesis. Arch Orthop Trauma
Surg. 136:657–663. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kolz CW, Suter T and Henninger HB:
Regional mechanical properties of the long head of the biceps
tendon. Clin Biomech (Bristol, Avon). 30:940–945. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yi Y, Lee JM, Kwon SH and Kim JW:
Arthroscopic proximal versus open subpectoral biceps tenodesis with
arthroscopy repair of small- or medium-sized rotator cuff tears.
Knee Surg Sports Traumatol Arthrosc. 24:3772–3778. 2016. View Article : Google Scholar : PubMed/NCBI
|