Introduction
Endovascular stent technology is a method commonly
employed for treating peripheral arterial disease (PAD) and recent
developments in this field have advanced conventional treatments,
including percutaneous transluminal angioplasty (PTA), which is
commonly used in patients with chronic lower limb PAD, e.g. elastic
recoil, residual stenosis and flow-limiting dissection (1–6).
However, secondary interventions may be required in several
patients with PAD treated with stenting due to femoropopliteal
in-stent restenosis, which is a regular defect associated with long
and complex lesions (7,8). It has been reported that
femoropopliteal in-stent restenosis occurs during the first year of
treatment in 18–40% of patients who have undergone stenting in the
femoropopliteal segment (9,10).
Aggressive debulking may be applied for
intravascular plaque treatment, hyperproliferative endometrial
tissue and clearance of thrombi. The debulking is performed using
an excimer laser, an ultraviolet (308 nm) cold-tipped laserthat
delivers ultra-short energy bursts (0.05 vs. 0.3–2.0 mm/pulse in
the hot-tip laser). The photochemical, photothermal and
photomechanical energy delivered by the excimer laser interacts
with tissue, breaks down molecular bonds and creates vapor bubbles
that generate kinetic energy. Long total superficial femoral artery
(SFA) occlusions, as in the Peripheral Excimer Laser Angioplasty
trial, as well as below-the-knee lesions in critical limb ischemia
patients have been treated with excimer laser, providing improved
results over those obtained with standard PTA alone, as well as
excellent limb-salvage rates (11–13). The
excimer laser probe is capable of ‘step-by-step’ debulking and
hence, excimer laser atherectomy (ELA) outperforms other mechanical
atherectomy treatments (14).
With the advent of drug-coated balloon (DCB)
technology, a potential novel treatment modality for
femoropopliteal arterial disease has become available (with or
without debulking). DCBs have been associated with inhibition of
restenosis in several randomized studies on native SFA lesions with
good results (15–17). DCBs alter the mitotic process of the
smooth muscle cells and, in turn, confer improvements that may be
sustained for at least 2 years. However, the effectiveness of DCB
angioplasty (DCBA) has been reported to decline after the first
year post-intervention (18,19). The use of DCBA as an additional
treatment following ELA has been proven to be superior to ELA
treatment alone (20–22). In addition, the abovementioned
studies have reported that DCBA treatment is critical for the
success and sustained durability of ELA.
To date, little is known on ELA with adjunctive DCBA
with regard to patency and target lesion revascularization rates
associated with the treatment of stable chronic occlusive disease
of the femoropopliteal artery. The aim of the present study was to
assess the safety, feasibility and the primary results of ELA
combined with adjunctive DCBA therapy in chronic obstructive
femoropopliteal arterial disease.
Materials and methods
Study design and patient samples
The present study analyzed the clinical data of 17
consecutive patients with symptomatic chronic obstructive
femoropopliteal arterial disease who were hospitalized at Tianjin
First Central Hospital (Tianjin, China) between May and December
2017. The analysis included patients aged between 59 and 83 years
who were diagnosed with either intermittent claudication or
critical limb ischemia (Rutherford categories 3–5) (23). The patients' ankle-brachial index was
≤0.8 in the target limb in all cases. All patients were treated
with ELA (Turbo-Elite laser catheter, Spectranetics; Philips
Medical Systems, Inc.), followed by angioplasty using DCBs (Orchid
paclitaxel-coated balloon catheter; Acotec Scientific). In
addition, Nitinol stents (Everflex; Medtronic Vascular, Inc.) were
only implanted in cases with suboptimal results due to recoil or
flow-limiting dissection.
The data of the present study included the baseline
clinical characteristics, procedure, angiographic variables and
outcomes that were extracted retrospectively, according to the
electronic medical records and angiographic images at Tianjin First
Central Hospital (Tianjin, China). Two physicians independently
reviewed all angiographic images for lesion morphology and
characteristics, according to the TransAtlantic Inter-Society
Consensus (TASC) II classification system (6), and for distal run-off (24). Follow-up results were collected from
all patients and their medical records were reviewed by a dedicated
research coordinator.
In all patients, the onset of symptoms occurred
>6 months prior to the primary crossing attempt. In patients
with intermittent claudication, conservative medical treatment and
exercise achieved no significant alleviation of the symptoms. The
ankle-brachial index was determined prior to the intervention and
in the follow-up examinations. All patients underwent a duplex
ultrasound prior to the procedure; a focal increase in the peak
systolic velocity of ≥140% (corresponding to a peak velocity ratio
of >2.4) was considered indicative of a >50% stenosis at that
site (25). Pre-interventional
diagnostics included CT angiography in all patients. The patients
underwent follow-up evaluation at 12 months with duplex ultrasound
and ankle-brachial index. Clinical examination was performed during
the follow-up visits.
Definitions and outcome measures
The primary efficacy endpoint of the present study
was the primary patency rate at 12 months. Secondary endpoints
included the following: Technical success and acute procedural
success rates, clinically driven target lesion revascularization
during the 12-month follow-up, bailout stenting during the index
procedure, ankle-brachial index and change in the Rutherford
category score. Primary patency was defined as ≤50% diameter
stenosis as assessed by duplex ultrasound in the absence of target
lesion revascularization, amputation and/or surgical bypass. The
patency threshold used for peak systolic velocity ratio was ≤2.4.
The technical success rate was defined as successful lesion
crossing and treatment, with a final residual stenosis of <30%.
Procedure success was defined as technical success with no major
adverse events at the end of the procedure (26). Clinically driven target lesion
revascularization was defined as a re-intervention performed for
>50% diameter stenosis or in the target lesion after
documentation of recurrent clinical symptoms following the index
procedure. The primary safety endpoints were evaluated as follows:
Adverse events occurring during and after the intervention, prior
to discharge, at the 30-day follow-up (including urgent target
lesion thrombolysis/thrombectomy due to thrombosis/embolism,
flow-limiting dissection, perforation, major bleeding and lower
extremity bypass) and major adverse events (including all-cause
death, unplanned major amputation and target lesion
revascularization).
Endovascular procedure
All patients were treated using a standard technique
and by the same operators, and were administered dual antiplatelet
therapy [100 mg/day (d) aspirin and 75 mg/d clopidogrel] at the
time of the procedure. Percutaneous access to the common femoral
artery was obtained in all patients. The approach of contralateral
crossover was preferred in the majority of cases. Unfractionated
heparin was recommended during the endovascular procedure at
sufficient doses (Initial dose, 100–150 U/kg; subsequent
administrations, 50 U/kg/h) to maintain an activated clotting time
of ≥250 sec. In all cases, a 7F or 8F Flexor Balkin Sheath or short
sheath (Cook Medical) were employed to establish access.
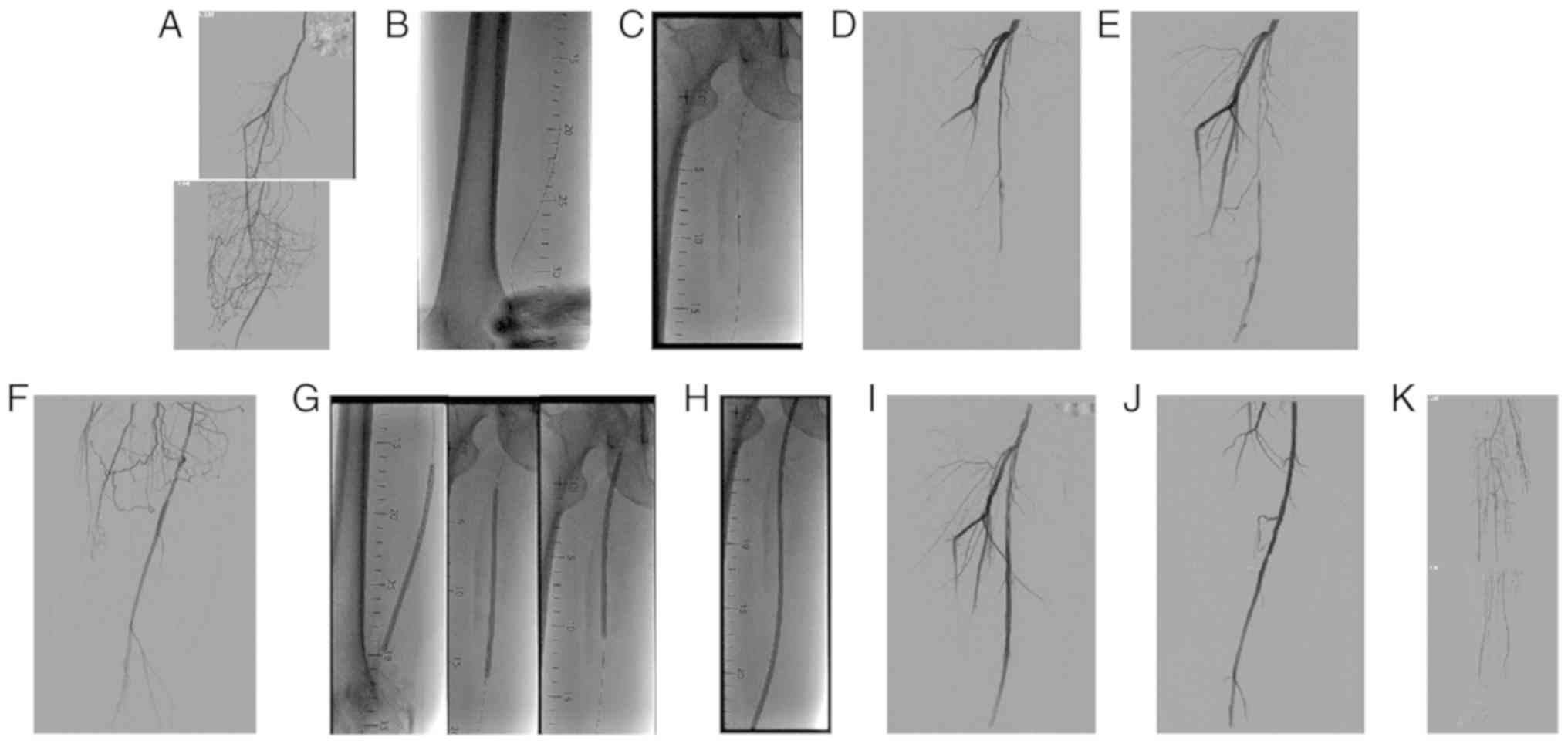
Stenosis/occlusion grade and lesion length were determined
angiographically (Fig. 1A). The
distal run-off status was also evaluated. The preferred technique
used was endoluminal recanalization, which allowed for directly
crossing the obstruction with the guidewire [0.035-inch Radiofocus
angled soft hydrophilic (Terumo Medical); 0.018-inch V18 control
wire (Boston Scientific)] and/or catheters [4F MPA catheter
(Cordis); 2.6F CXI (Cook Medical)] avoiding the intentional
subintimal approach. A total of seven cases suffered retrograde
puncture of the normal artery at the distal end of the occlusion,
or retrograde distal run-off vessels (SFA, posterior tibial artery,
peroneal artery; Fig. 1B). The
excimer laser (CVX-300 Excimer Laser System; Spectranetics; Philips
Medical Systems, Inc.; wavelength, 308 nm) was used and the
Turbo-Elite laser catheter (2.0–2.5 mm, Spectranetics; Philips
Medical Systems, Inc.) that was suitable for the vessel diameter
was inserted via a V18 control wire (Fig. 1C). The laser catheter was advanced
0.5–1 mm/sec. The angiographic results of ELA are depicted in
Fig. 1D-F. Following ELA, PTA was
routinely performed for ≥1 min with pressure-only balloons
(Pacific/Admiral Xtreme/Amphirion Deep; Medtronic Vascular) matched
to the reference vessel diameter (Fig.
1G). Subsequently, adjunctive DCBA was performed with a
paclitaxel-coated (3 µg/mm2) balloon catheter (Orchid;
Acotec Scientific) for 3 min (Fig.
1H). Bailout stenting was used for the treatment of
flow-limiting dissection or suboptimal angiographic results with
residual stenosis (>30%). The use of a distal embolic protection
device and the number of passes and energy delivered by ELA were at
the operator's discretion. Completion angiography was then
performed with distal run-off vessels to evaluate evidence of
distal embolization. A successful procedure was assumed if a
straight-line flow from the iliac arteries through ≥1 tibial artery
to the pedal arteries in the foot was achieved. The final
angiographic results are depicted in Fig. 1I-K. A Perclose ProGlide
Suture-Mediated Closure System (Abbott Vascular) was used for
hemostasis of the common femoral artery access site and a bandage
with mild compression was applied for 24 h.
Patients were instructed to continue taking aspirin
for ≥12 months and clopidogrel for ≥6 months following the
procedure. Vessel calcification was graded angiographically using
the following criteria as previously described (27): None/mild, no radio-opacities;
moderate, radio-opacities appearing unilaterally on the arterial
wall or for a length of <1 cm prior to contrast injection or
digital subtraction angiography; and severe, radio-opacities
appearing bilaterally on the arterial wall and extending for a
length of >1 cm prior to contrast injection or digital
subtraction angiography.
Statistical analysis
Continuous variables are expressed as the mean ±
standard deviation and categorical variables as n (%). The primary
patency rate was analyzed using Kaplan-Meier curves. P<0.05 was
considered to indicate a statistically significant difference. The
pre-procedure ankle-brachial index was compared to the follow-up
values using a paired t-test. Statistical analysis was performed
using SPSS version 23.0 (IBM Corp.).
Results
Patient characteristics
The patients' demographic and clinical
characteristics are summarized in Table
I. The mean age of the patients was 68.9±7.4 years and 94.1% of
the patients were male. The patients had multiple comorbidities,
with a high frequency of hypertension (76.5%), hyperhomocysteinemia
(58.8%), cerebrovascular disease (52.9%), smoking history (76.5%)
and diabetes (52.9%). The baseline ankle-brachial index of the
treated leg was 0.36±0.25. The majority of the patients were
severely symptomatic. In detail, a Rutherford category of 3 was
determined in 52.9%, a category of 4 in 17.7% and a category of 5
in 29.4% of the cases. The mean hospitalization time was 15.5±2.4
days. The angiographic and procedural detailed characteristics are
listed in Table II. The majority of
the cases required a contralateral cross-over approach to cross the
lesion (88.2%) and 7 cases (41.2%) required retrograde puncture of
the normal artery at the distal end of the occlusion. Therefore,
lesion crossing was achievable in all patients, including those
with heavily calcified lesions, without the assistance of the
step-by-step technique. The mean lesion length was 23.3±8.9 cm
(range, 5.6–40.5 cm) and 58.8% of the lesions were TASC II type D.
All patients had chronic total occlusion in the femoropopliteal
artery. Pre-interventional angiography revealed occlusion of the
SFA in 41.2% and of the SFA + popliteal artery in 58.8% (including
the P1-P3 segment), whereas certain patients also displayed iliac
artery lesions (17.7%). The lesions were pre-treated with ELA and
PTA in all cases. Turbo Elite catheters were used, mainly 2-mm
(41.2%), 2.3-mm (41.2%) and 2.5-mm (17.6%) in the femoral and
popliteal segments. Proper lumen sizing was generally assured by
angioplasty using long (8-20-cm) balloons. The number of
pressure-only balloons and DCBs was 2.8±1.2 and 1.0±0.0/patient,
respectively. One TASC II type D patient experienced flow-limiting
dissection. Bailout stenting was required in 5/17 patients who were
recanalized by ELA and adjunctive drug-coated BA due to
flow-limiting dissection (5.9% of the patients) and recoil
(residual stenosis of >30%; 23.5% of the patients). The mean
stent length was 182±50.4 mm. The mean number of run-off vessels
was 2.1±0.8/patient. A total of 6 patients had a 1-vessel run-off,
4 had a 2-vessel and 7 had a 3-vessel run-off.
 | Table I.Demographic and clinical
characteristics of the subjects (n=17). |
Table I.
Demographic and clinical
characteristics of the subjects (n=17).
| Variable | Value |
|---|
| Age (years) | 68.9±7.4
(59–83) |
| Male | 16 (94.1) |
| Medical
history |
| DM | 9 (52.9) |
|
Hypertension | 13 (76.5) |
|
Dyslipidemia | 4 (23.5) |
|
CAD | 6 (35.3) |
| Prior
PCI/bypass surgery | 2 (11.8) |
|
CVD | 9 (52.9) |
|
COPD | 1 (5.9) |
| Carotid
stenosis | 6 (35.3) |
| Renal
artery stenosis | 4 (23.5) |
|
Hyperhomocysteinemia | 10 (58.8) |
|
Homocysteine (µmol/ml) | 24.3±12.2
(11.8–119.7) |
| Current
or former smoker | 13 (76.5) |
| History
of other diseasesa | 4 (23.5) |
| Target lesion side
ABI | 0.36±0.25
(0–0.82) |
| Pre-operative
Rutherford category |
|
| 3 | 9 (52.9) |
| 4 | 3 (17.7) |
| 5 | 5 (29.4) |
| Hospital stay, days
(range) | 15.5±2.4
(9–28) |
| Total cost, dollars
(range) | 18,689±3,347.3 |
|
|
(11,576–25,941) |
| CTO | 17 (100) |
| Target lesion
side |
|
|
Right | 9 (53.0) |
|
Left | 8 (47.0) |
| Table II.Detailed angiographic and procedural
characteristics for the patients (n=17). |
Table II.
Detailed angiographic and procedural
characteristics for the patients (n=17).
| Variable | Value |
|---|
| Access
approach |
|
|
Contralateral cross-over | 15/17 (88.2) |
|
Antegrade | 2/17 (11.8) |
|
Adjunctive
access | 7/17 (41.2) |
|
Retrograde
distal SFA/popliteal artery P1 | 5/7 (71.4) |
|
Retrograde
PTA | 1/7 (14.3) |
|
Retrograde
peroneal artery | 1/7 (14.3) |
| TASC II |
|
| B | 5/17 (29.4) |
| C | 2/17 (11.8) |
| D | 10/17 (58.8) |
| Lesion
location |
|
| IA | 3/17 (17.7) |
| Only
SFA | 7/17 (41.2) |
| Only
popliteal artery | 0/17 (0) |
| SFA and
popliteal artery | 10/17 (58.8) |
| Calcification |
|
|
None/mild | 10/17 (58.8) |
|
Moderate | 3/17 (17.7) |
|
Severe | 4/17 (23.5) |
| FPA occlusion
length (cm) | 23.3±8.9
(5.6–40.5) |
| Below-knee
runoff | 2.1±0.8 |
| 0 | 0/17 (0) |
| 1 | 6/17 (35.3) |
| 2 | 4/17 (23.5) |
| 3 | 7/17 (41.2) |
| Laser
parameters |
|
| Laser
catheter size (mm) | 2.2±0.2 |
|
2.0 | 7/17 (41.2) |
|
2.3 | 7/17 (41.2) |
|
2.5 | 3/17 (17.6) |
| Number of
balloons/patient | 2.8±1.2 |
| Number of
DCBs/patient | 1±0 |
| DCB diameter
(mm) | 4.5±0.7 |
| DCB length
(mm) | 210.9±90.0 |
| EPD | 4/17 (23.5) |
| Bailout
stenting | 5/17 (29.4) |
| Stent length
(mm) | 182±50.4 |
| Reason for bailout
stenting |
|
| Recoil
(residual stenosis >30%) | 4/17 (23.5) |
|
Flow-limiting dissection | 1/17 (5.9) |
Procedural outcomes
A summary of the procedural outcomes is provided in
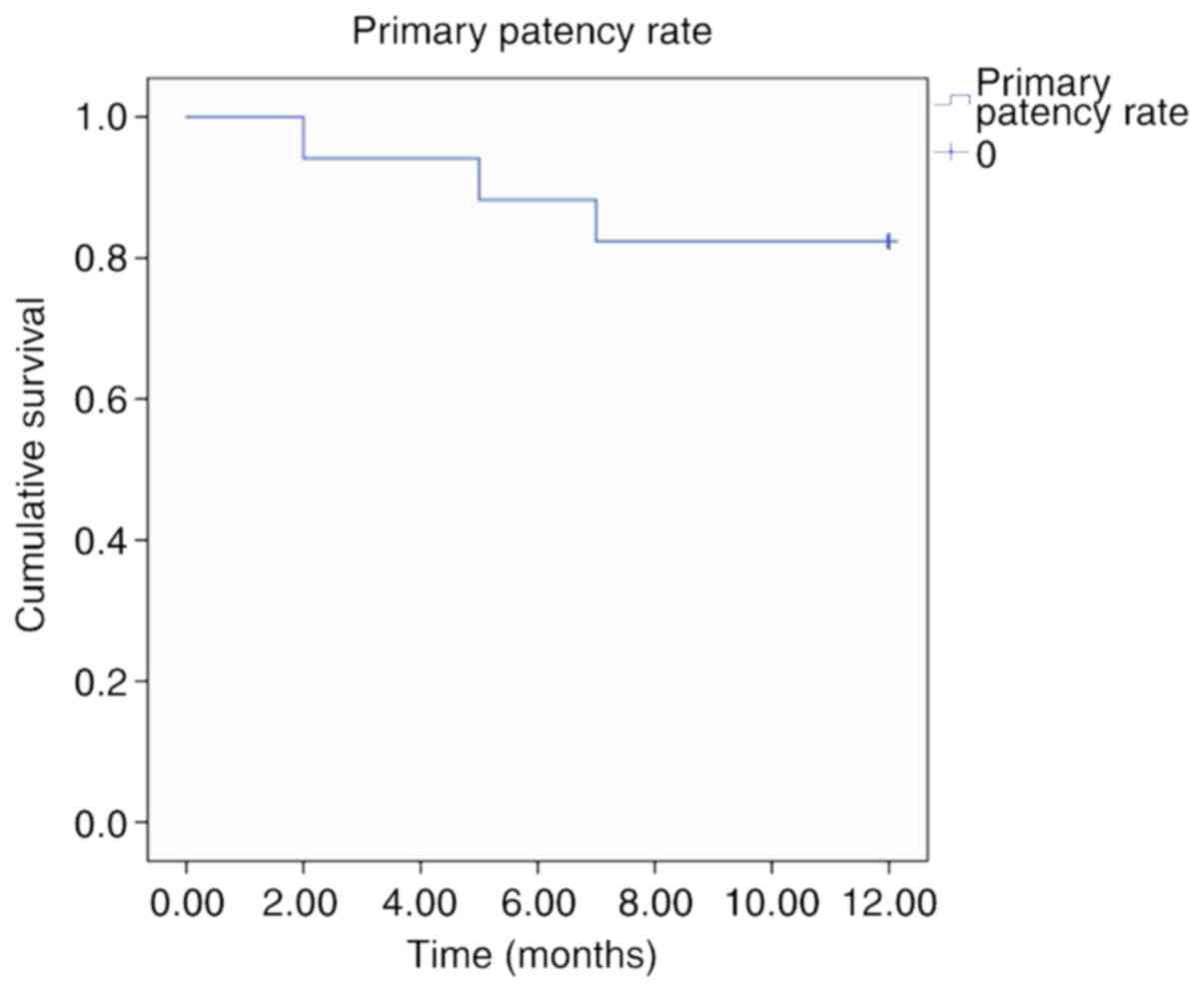
Table III. The primary patency
rate was 82.4% at 12 months (Table
III; Fig. 2), meeting the
primary efficacy endpoint. Two patients with duplex ultrasound
evidence of restenosis had an ankle-brachial index of >0.7 and
were Rutherford category 1–2; therefore, repeat intervention was
not performed. Technical and procedural success rates were 100 and
88.2%, respectively. One TASC II type C patient experienced distal
embolization intra-operatively, when balloon dilation of the target
lesion after ELA resulted in emboli to the distal popliteal artery,
which was successfully treated with rotational thrombectomy
(Rotarex®; Straub Medical). Another TASC II type D
patient experienced flow-limiting dissection intra-operatively,
which was successfully treated with bailout stenting. The rate of
clinically driven target lesion revascularization at 12 months was
5.9% (1/17). One patient who reported rest pain was diagnosed with
clinically significant acute re-occlusion with duplex ultrasound at
2 months post-intervention and underwent rotational thrombectomy
due to acute thrombosis. In patients who underwent repeat
intervention, there was restenosis at the edge of the stent. Ulcer
healing were observed in all patients with immediate procedural
success. None of the patients underwent amputation and no deaths
were reported throughout the follow-up period. Table IV summarizes the changes in the
ankle-brachial index immediately post-intervention and at 12 months
compared with that pre-intervention. There was a significant
improvement in the ankle-brachial index from 0.36±0.25 prior to the
intervention to a mean value of 0.94±0.13 prior to discharge
(P<0.001). In the follow-up period, no significant decrease in
the ankle-brachial index (0.81±0.26) compared with the
post-interventional control value (0.94±0.13) was obtained
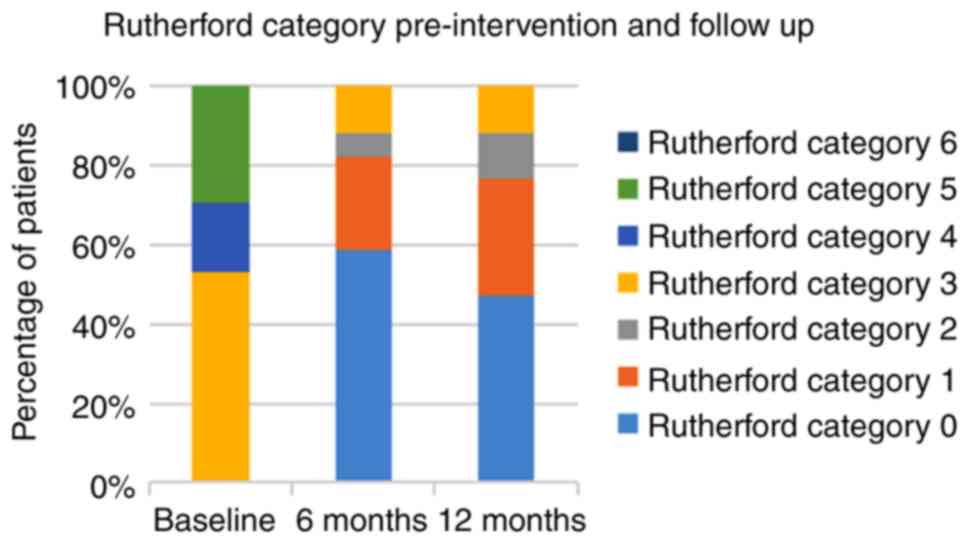
(P>0.05). At 6 and 12 months, there were more patients with
Rutherford categories of 0 and 1 compared with those at baseline
(Fig. 3). Overall, the Rutherford
category had improved at 12 months when compared with that at
baseline. At baseline, 52.9, 17.7 and 29.4% of the patients were
Rutherford category 3, 4 and 5, respectively, and at 12 months,
47.0, 29.4, 11.8 and 11.8% of the patients were Rutherford category
0, 1, 2 and 3, respectively.
| Table III.Procedural outcomes. |
Table III.
Procedural outcomes.
| Variable | Value |
|---|
| Primary patency
rate at 12 months | 14/17 (82.4) |
| Technical success
rate | 17/17 (100) |
| Procedural success
rate | 15/17 (88.2) |
| Clinically-driven
TLR at 12 months | 1/17 (5.9) |
| Adverse events
during hospitalization and at 30-day follow-up |
|
|
Embolism in all patients | 1/17 (5.9) |
|
Embolism in
patients with EPD | 1/4 (25) |
|
Distal
Embolization requiring treatment | 1/17 (5.9) |
|
Thrombosis | 0/17 (0) |
|
Flow-limiting
dissection | 1/17 (5.9) |
|
Perforation | 0/17 (0) |
|
Major
bleeding | 0/17 (0) |
| MAEs |
|
|
All-cause
death | 0/17 (0) |
|
Unplanned
minor/major amputation | 0/17 (0) |
|
TLR | 0/17 (0) |
| Table IV.Change in ABI in the patients (n=17)
across the study period. |
Table IV.
Change in ABI in the patients (n=17)
across the study period.
| Time-point | ABI | F-value | P-value, vs.
Pre-intervention |
|---|
|
Pre-intervention | 0.36±0.25 |
|
|
|
Post-intervention | 0.94±0.13 | 29.18 | <0.001 |
| Follow-up at 12
months | 0.81±0.26 | 17.56 | <0.001 |
Discussion
SFA disease accounts for 40–50% of patients with PAD
(28). The first clinical
manifestation is frequently the appearance of intermittent
claudication. In patients with critical limb ischemia, more severe
consequences may occur, which are associated with an increased risk
of amputation and mortality (29).
It is currently estimated that the incidence of PAD in Chinese
patients aged >60 years is 20% (30). A study by Luo et al (31) demonstrated that the all-cause
mortality rate for PAD was 22%. Regarding treatment, bypass surgery
is considered to be the gold standard for infrainguinal chronic
occlusions (32). However, patients,
particularly diabetics, with critical limb ischemia are not
considered as candidates for bypass surgery due to the multiple
comorbidities and high surgical risk. Subsequently, endovascular
therapy has been increasingly used due to its lower morbidity and
mortality rates compared with those of bypass surgery. BA plus
stenting is the most commonly used technique for revascularization
in femoropopliteal arterial disease. However, revascularization of
the femoropopliteal arteries with stable long-term results remains
a challenge for endovascular specialists. While self-expanding
Nitinol stents have demonstrated excellent immediate results,
restenosis remains a limitation in the femoropopliteal segment,
with restenosis rates of 20–37% at 12 months (2,10,33) and
≤49% at 2 years (4). This makes
in-stent occlusion another significant clinical stumbling block.
Lesion crossing and recanalization of chronic total occlusions in
the femoropopliteal arteries is often challenging.
ELA involves employing photochemical,
photomechanical and photothermal processes to debulk and ablate
tissue (thrombi, atherosclerotic plaques) and has been proven to be
a useful supplement to chronic obstructive arterial treatment
(11,34). The patency rates of successfully
treated lesions (freedom from target lesion revascularization) have
been reported to be 96.6% at 12 and 82.7% at 24 months (14). The same study also reported the
expected limb-salvage rates at 12 and 24 months to be 100 and 94%,
respectively. Therefore, ELA appears to be an effective treatment
for potential long occlusion and complex disease, since it provides
a better angiographic result and lowers the requirement for
stenting. High success rates of recanalization have been
demonstrated in large earlier trials, even in long symptomatic SFA
occlusions (35). In 2009, Dave
et al (36) published a
prospective multi-center study (17 hospitals in the US) evaluating
the safety and efficacy of ELA in the treatment of primary
femoropopliteal artery occlusive disease. Their study included 65
patients with a mean lesion length of 5.6 cm, of which 13 cases
were occluded; the mean lumen loss rate was reduced from 77 to
34.7%, which was reduced to 21±14.5% after adjunctive therapy with
BA (n=42, 64.6%) or BA + stenting (n=15, 23.3%), and the patency
rate was 59 and 54% at 6 and 12 months, respectively. Target lesion
revascularization was not required in 76.9% of CliRpath Excimer
Laser System to Enlarge Lumen Openings participants within the
1-year follow-up period. The safety and efficacy of this technique
were validated in 65 patients without major adverse events or
complications. Simultaneously, DCBs have achieved satisfactory
results in the treatment of lower extremity occlusive primary
lesions and in-stent restenosis (15,16,19,37).
LEVANT-2 is a large prospective, multi-center, single-blinded
randomized controlled trial (RCT) comprising a total of 476
patients. Comparing the effects of DCB (Lutonix™; Bard) and PTA in
the treatment of femoropopliteal artery occlusive disease, the
results demonstrated that the patency rate of the DCB group was
significantly higher compared with that of normal PTA at 1 year
(65.2 vs. 52.6%, respectively; P=0.015) (38). IN.PACT SFA is also a prospective,
multicenter RCT with a total of 331 patients enrolled. The patients
were randomly assigned to the DCB (IN.PACT Admiral; Medtronic) and
the normal PTA groups, and the results demonstrated that the target
lesion revascularization of the DCB group was significantly lower
compared with that in the normal PTA group (2.4 vs. 20.6%,
respectively; P=0.001). The 1-year patency rate was 82.2% in the
DCB and 52.5% in the normal PTA group, respectively (P=0.001)
(39). In addition, ELA has been
employed for the treatment of femoropopliteal in-stent restenosis
(27). Specifically, Dippel et
al (27) observed that ELA
combined with PTA demonstrated superior procedural success compared
with the PTA alone group (93.5 vs. 82.7%; P<0.01) and
significantly fewer procedural complications. At 6 months, freedom
from target lesion revascularization with ELA combined with PTA
compared with PTA alone was observed in 73.5 vs. 51.8% of the
patients, respectively (P<0.005), and the 30-day major adverse
event rates were 5.8 vs. 20.5% (P<0.001), respectively. The
above-mentioned study concluded that ELA combined with PTA
significantly lowered target lesion revascularization by 52%
(hazard ratio=0.48; 95% CI, 0.31–0.74).
The present study was a retrospective analysis
aiming to evaluate the role of ELA combined with adjunctive DCBA in
the treatment of femoropopliteal arterial disease. Previously
published studies (the LACI phase 2 and LACI Belgium studies) have
reported on the success of ELA-assisted angioplasty in the lower
extremities (12,13). The LACI phase 2 study evolved from a
25-patient phase I registry to enrollment of 145 patients with
critical limb ischemia. Restoration of the straight-line flow to
the foot was achieved in 89% of the patients, and adjunctive PTA
and stenting were employed in 96 and 45% of cases, respectively,
with a patency rate at 6 months of 83%. The 6-month limb-salvage
rate was 92.5%, with a major amputation rate of 8%. The LACI
Belgium study included 48 patients with critical limb ischemia
(13). In the majority of the
patients, the straight-line flow to the foot was restored, and
adjunctive PTA and stenting were used in 80 and 52.9% of cases,
respectively. The 6-month patency rate was at 76% and the limb
salvage rate at 6 months was 90.5%, with a major amputation rate of
8%.
Comparison of the results of the present study with
those reported by the above-mentioned studies (12,13)
indicated similar lesion site observations and similar clinical
characteristics of the patients. The LACI 2 and the LACI Belgium
studies only included patients who were poor surgical candidates;
however, in the present study, all patients with chronic total
occlusion undergoing peripheral revascularization procedures were
included, and ELA was employed in combination with DCBA in order to
treat femoropopliteal arterial disease. This change in the patient
criteria may explain the differences in the patency rates (82.4% at
12 months) as well as bailout stenting rates (29.4%) between the
present study and the two LACI trials. Other possible explanations
may be the reduced use of stents, smaller patient samples, the
selection criteria and the single-center design of the present
study. The ELA technique offers a theoretical advantage when
compared with PTA, which is the reduced stretching of the vessel
achieved by the ablation effect that allows for remodeling of the
vascular lumen. Satisfactory long-term patency and limb-salvage
rates are supported by the results of the present study and are in
agreement with other published results on mechanical atherectomy
(Rotarex or TurboHawk) (40). The
in-stent restenosis incidence is more frequently encountered among
diabetic patients and, during long-term endovascular intervention
therapy, the high incidence of in-stent restenosis may lead to
unproficient use of stents. Subsequently, ELA may offer better
results than DCBA, as well as reduce the requirement for
stenting.
An experience with 40 patients undergoing
unsuccessful angioplasty of TASC C and D lesions in femoropopliteal
arteries treated via ELA was reported by Wissgott et al
(41). Their study reported a mean
occlusion length of 17.5 cm (range, 12–25 cm). Recanalization using
the step-by-step method of crossing was performed with an excimer
laser catheter (catheter diameter range, 1.7–2.5 mm). Balloon
dilation was performed in all cases after successful crossing and
stent placement was required in 10% of the procedures. The initial
technical success rate of 90% (36/40) resulted in a primary patency
rate of 58.9% after 12 months. No serious complications
attributable to the intervention were reported. The present study
involved significantly longer occlusion lesions (23.3 vs. 17.5 cm)
and more TASC II D cases compared with those in the above-mentioned
study. In addition, DCBs were used in the present study, which may
explain for the higher primary patency and lower target lesion
revascularization rates in the present study. Furthermore, all
patients exhibited a marked improvement in their Rutherford
category and their ankle-brachial index that persisted at the
12-month follow-up.
Lüdtke et al (42) reported that 15 patients (15/67, 22%)
who underwent ELA-assisted PTA of the femoropopliteal arteries were
treated via a retrograde transpopliteal approach. Technically
successful recanalization was achieved in 14 of the 15 patients.
There were no major adverse events regarding the laser atherectomy
or popliteal access site. Compared with the results reported by
Lüdtke et al (42), 7
patients of the present study required a retrograde recanalization
access (including distal SFA/popliteal artery P1 segment, posterior
tibial artery and peroneal artery). The technical success rate was
100%. Retrograde access achieves a high recanalization rate in
femoropopliteal arterial disease when conventional crossing
attempts have failed. An advantage of the retrograde approach may
be easier entry into the occlusion due to a softer distal cap. The
popliteal approach was used more frequently compared with other
access approaches. Sangiorgi et al (43) reported technical success rates of
~96% in long TASC C and D lesions, and proposed the transpopliteal
access as a safe and effective alternative when antegrade
recanalization attempts have failed.
The present study takes into consideration the cost
of ELA combined with DCB in the treatment of femoropopliteal
arterial disease, and cost is one of the drawbacks of laser
technology. It was estimated that the cost of ELA combined with DCB
was higher compared with that of standard techniques (PTA and
stenting), with a mean cost of 18,689 dollars per procedure.
The limitations of the present study include its
observational retrospective design, the small patient sample and
the lack of a control group with the use of angioplasty combined
with stenting for comparison. To date, no published randomized data
are available to evaluate the efficacy of ELA combined with that of
adjunctive DCBA in the treatment of chronic obstructive
femoropopliteal arterial disease.
The results of the present study suggest that the
ELA technique achieved a good technical success rate with a low
complication rate in the treatment of TASC II B, C and D lesions.
The use of ELA reduced the requirement for stenting in the lower
limb arteries. The present study also demonstrated that the ELA
approach may be valuable and effective even in long, complex
occlusive lesions. Therefore, future large-scale randomized studies
addressing complex cases of obstructive femoropopliteal arterial
disease should be encouraged.
Acknowledgements
Not applicable.
Funding
This study was financially supported by the Science
and Technology Plan Project of Tianjin (grant no. 18ZXDBSY00110)
and the Tianjin Health and Family Planning Commission Science and
Technology Fund Project (grant no. 2015KZ033).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
Conception and design: HL and FZ. Analysis and
interpretation: HL, FZ and JH. Data collection: HL, YG and SY.
Writing of the manuscript: HL, YG, SY, JH and FZ. Critical revision
of the manuscript: HL, JH and FZ. Final approval of the manuscript:
HL, YG, SY, JH and FZ. Statistical analysis: HL. Overall
responsibility: FZ.
Ethics approval and consent to
participate
The study was performed in accordance with the
ethical principles of the Declaration of Helsinki. The study
protocol was reviewed and approved by the Tianjin First Central
Hospital (Tianjin, China) institutional review board and all
procedures were performed after obtaining informed consent from all
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferreira M, Lanziotti L, Monteiro M,
Abuhadba G, Capotorto LF, Nolte L and Fearnot N: Superficial
femoral artery recanalization with self-expanding nitinol stents:
Long-term follow-up results. Eur J Vasc Endovasc Surg. 34:702–708.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Krankenberg H, Schlüter M, Steinkamp HJ,
Bürgelin K, Scheinert D, Schulte KL, Minar E, Peeters P, Bosiers M,
Tepe G, et al: Nitinol stent implantation versus percutaneous
transluminal angioplasty in superficial femoral artery lesions up
to 10 cm in length: The femoral artery stenting trial (FAST).
Circulation. 116:285–292. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zeller T, Tiefenbacher C, Steinkamp HJ,
Langhoff R, Wittenberg G, Schlüter M, Buergelin K, Rastan A,
Krumsdorf U, Sixt S, et al: Nitinol stent implantation in TASC A
and B superficial femoral artery lesions: The femoral artery
conformexx trial (FACT). J Endovasc Ther. 15:390–398. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schillinger M, Sabeti S, Dick P, Amighi J,
Mlekusch W, Schlager O, Loewe C, Cejna M, Lammer J and Minar E:
Sustained benefit at 2 years of primary femoropopliteal stenting
compared with balloon angioplasty with optional stenting.
Circulation. 115:2745–2749. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rocha-Singh KJ, Jaff MR, Crabtree TR,
Bloch DA and Ansel G; VIVA Physicians, Inc, : Performance goals and
endpoint assessments for clinical trials of femoropopliteal bare
nitinol stents in patients with symptomatic peripheral arterial
disease. Catheter Cardiovasc Interv. 69:910–919. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Norgren L, Hiatt WR, Dormandy JA, Nehler
MR, Harris KA, Fowkes FG; TASC II Working Group, ; Bell K,
Caporusso J, Durand-Zaleski I, et al: Inter-society consensus for
the management of peripheral arterial disease (TASCII). Eur J Vasc
Endovasc Surg. 33 (Suppl 1):S1–S75. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gur I, Lee W, Akopian G, Rowe VL, Weaver
FA and Katz SG: Clinical outcomes and implications of failed
infrainguinal endovascular stents. J Vasc Surg. 53:658–666. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Armstrong EJ, Saeed H, Alvandi B, Singh S,
Singh GD, Yeo KK, Anderson D, Westin GG, Dawson DL, Pevec WC and
Laird JR: Nitinol self-expanding stents vs. balloon angioplasty for
very long femoropopliteal lesions. J Endovasc Ther. 21:34–43. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schillinger M, Sabeti S, Loewe C, Dick P,
Amighi J, Mlekusch W, Schlager O, Cejna M, Lammer J and Minar E:
Balloon angioplasty versus implantation of nitinol stents in the
superficial femoral artery. N Engl J Med. 354:1879–1888. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Laird JR, Katzen BT, Scheinert D, Lammer
J, Carpenter J, Buchbinder M, Dave R, Ansel G, Lansky A, Cristea E,
et al: Nitinol stent implantation versus balloon angioplasty for
lesions in the superficial femoral artery and proximal popliteal
artery: Twelve-month results from the RESILIENT randomized trial.
Circ Cardiovasc Interv. 3:267–276. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Scheinert D, Laird JR Jr, Schröder M,
Steinkamp H, Balzer JO and Biamino G: Excimer laser-assisted
recanalization of long, chronic superficial femoral artery
occlusions. J Endovasc Ther. 8:156–166. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Laird JR, Zeller T, Gray BH, Scheinert D,
Vranic M, Reiser C and Biamino G; LACI Investigators, : Limb
salvage following laser-assisted angioplasty for critical limb
ischemia: Results of the LACI multicenter trial. J Endovasc Ther.
13:1–11. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bosiers M, Peeters P, Elst FV, Vermassen
F, Maleux G, Fourneau I and Massin H: Excimer laser assisted
angioplasty for critical limb ischemia: Results of the LACI Belgium
study. Eur J Vasc Endovasc Surg. 29:613–619. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Serino F, Cao Y, Renzi C, Mascellari L,
Toscanella F, Raskovic D, Tempesta P, Bandiera G and Santini A:
Excimer laser ablation in the treatment of total chronic
obstructions in critical limb ischaemia in diabetic patients.
Sustained efficacy of plaque recanalisation in mid-term results.
Eur J Vasc Endovase Surg. 39:234–238. 2010. View Article : Google Scholar
|
|
15
|
Werk M, Langner S, Reinkensmeier B,
Boettcher HF, Tepe G, Dietz U, Hosten N, Hamm B, Speck U and Ricke
J: Inhibition of restenosis in femoropopliteal arteries:
Paclitaxel-coated versus uncoated balloon: Femoral paclitaxel
randomized pilot trial. Circulation. 118:1358–1365. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tepe G, Zeller T, Albrecht T, Heller S,
Schwarzwälder U, Beregi JP, Claussen CD, Oldenburg A, Scheller B
and Speck U: Local delivery of paclitaxel to inhibit restenosis
during angioplasty of the leg. N Engl J Med. 358:689–699. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ansel GM and Lumsden AB: Evolving
modalities for femoropopliteal interventions. J Endovasc Ther. 16
(Suppl 2):II82–II97. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Grotti S, Liistro F, Angioli P, Ducci K,
Falsini G, Porto I, Ricci L, Ventoruzzo G, Turini F, Bellandi G and
Bolognese L: Paclitaxel-eluting balloon vs standard angioplasty to
reduce restenosis in diabetic patients with in-stent restenosis of
the superficial femoral and proximal popliteal arteries: Three-year
results of the DEBATE-ISR study. J Endovasc Ther. 23:52–57. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Virga V, Stabile E, Biamino G, Salemme L,
Cioppa A, Giugliano G, Tesorio T, Cota L, Popusoi G, Pucciarelli A,
et al: Drug-eluting balloons for the treatment of the superficial
femoral artery in-stent restenosis: 2-year follow-up. JACC
Cardiovasc Interv. 7:411–415. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kokkinidis DG, Hossain P, Jawaid O,
Alvandi B, Foley TR, Singh GD, Waldo SW, Laird JR and Armstrong EJ:
Laser atherectomy combined with drug-coated balloon angioplasty is
associated with improved 1-year outcomes for treatment of
femoropopliteal in-stent restenosis. J Endovasc Ther. 25:81–88.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Van den Berg JC, Pedrotti M, Canevascini
R, Chimchila Chevili S, Giovannacci L and Rosso R: In-stent
restenosis: Mid-term results of debulking using excimer laser and
drug-eluting balloons: Sustained benefit? J Invasive Cardiol.
26:333–337. 2014.PubMed/NCBI
|
|
22
|
Sixt S, Carpio Cancino OG, Treszl A,
Beschorner U, Macharzina R, Rastan A, Krankenberg H, Neumann FJ and
Zeller T: Drug-coated balloon angioplasty after directional
atherectomy improves outcome in restenotic femoropopliteal
arteries. J Vasc Surg. 58:682–686. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rutherford RB, Baker JD, Ernst C, Johnston
KW, Porter JM, Ahn S and Jones DN: Recommended standards for
reports dealing with lower extremity ischemia: Revised version. J
Vasc Surg. 26:517–538. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Popma JJ, Tiroch K, Almonacid A, Cohen S,
Kandzari DE and Leon MB: A qualitative and quantitative
angiographic analysis of stent fracture late following
sirolimus-eluting stent implantation. Am J Cardiol. 103:923–929.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ranke C, Creutzig A and Alexander K:
Duplex scanning of the peripheral arteries: Correlation of the peak
velocity ratio with angiographic diameter reduction. Ultrasound Med
Biol. 18:433–440. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Shammas NW, Shammas GA, Helou TJ,
Voelliger CM, Mrad L and Jerin M: Safety and 1-year
revascularization outcome of SilverHawk atherectomy in treating
in-stent restenosis of femoropopliteal arteries: A retrospective
review from a single center. Cardiovasc Revasc Med. 13:224–227.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Dippel EJ, Makam P, Kovach R, George JC,
Patlola R, Metzger DC, Mena-Hurtado C, Beasley R, Soukas P,
Colon-Hernandez PJ, et al: Randomized controlled study of excimer
laser atherectomy for treatment of femoropopliteal in-stent
restenosis: Initial results from the EXCITE ISR trial (EXCImer
Laser Randomized Controlled Study for Treatment of FemoropopliTEal
In-Stent Restenosis). JACC Cardiovasc Interv. 8:92–101. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Gonzalez L, Chen A, Lin PH, Pisimisis G,
Barshes NR, Bechara CF and Kougias P: Latest recanalization
techniques for complex superficial femoral artery occlusions. J
Cardiovasc Surg (Torino). 53:487–494. 2012.PubMed/NCBI
|
|
29
|
Golomb BA, Dang TT and Criqui MH:
Peripheral arterial disease: Morbidity and mortality implications.
Circulation. 114:688–699. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
He Y, Jiang Y, Wang J, Fan L, Li X and Hu
FB: Prevalence of peripheral arterial disease and its association
with smoking in a population-based study in Beijing, China. J Vasc
Surg. 44:333–338. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Luo Y, Li X, Li J, Wang X, Qiao Y, Hu D,
Merriam PA and Ma Y: Combined effects of smoking and peripheral
arterial disease on all-cause and cardiovascular disease mortality
in a Chinese male cohort. J Vasc Surg. 51:673–678. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Dormandy JA and Rutherford RB: Management
of peripheral arterial disease (PAD). TASC working group.
TransAtlantic inter-society consensus (TASC). J Vasc Surg.
31:S1–S296. 2000.PubMed/NCBI
|
|
33
|
Bosiers M, Torsello G, Gissler HM, Ruef J,
Müller-Hülsbeck S, Jahnke T, Peeters P, Daenens K, Lammer J, Schroë
H, et al: Nitinol stent implantation in long superficial femoral
artery lesions: 12-month results of the DURABILITY I study. J
Endovasc Ther. 16:261–269. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhou W, Bush RL, Lin PH, Peden EK and
Lumsden AB: Laser atherectomy for lower extremity
revascularization: An adjunctive endovascular treatment option.
Vasc Endovascular Surg. 40:268–274. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Sultan S, Tawfick W and Hynes N: Cool
excimer laser-assisted angioplasty (CELA) and tibial balloon
angioplasty (TBA) in management of infragenicular arterial
occlusion in critical lower limb ischemia (CLI). Vasc Endovascular
Surg. 47:179–191. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Dave RM, Patlola R, Kollmeyer K, Bunch F,
Weinstock BS, Dippel E, Jaff MR, Popma J and Weissman N; CELLO
Investigators, : Excimer laser recanalization of femoropopliteal
lesions and 1-year patency: Results of the CELLO registry. J
Endovasc Ther. 16:665–675. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Liistro F, Grotti S, Porto I, Angioli P,
Ricci L, Ducci K, Falsini G, Ventoruzzo G, Turini F, Bellandi G and
Bolognese L: Drug-eluting balloon in peripheral intervention for
the superficial femoral artery: The DEBATE-SFA randomized trial
(drug eluting balloon in peripheral intervention for the
superficial femoral artery). JACC Cardiovasc Interv. 6:1295–1302.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Rosenfield K, Jafr MR, White CJ,
Rocha-Singh K, Mena-Hurtado C, Metzger DC, Brodmann M, Pilger E,
Zeller T, Krishnan P, et al: Trial of a paclitaxel-coated balloon
for femoropopliteal artery disease. N Engl J Med. 373:145–153.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Tepe G, Laird J, Schneider P, Brodmann M,
Krishnan P, Micari A, Metzger C, Scheinert D, Zeller T, Cohen DJ,
et al: Drug-coated balloon versus standard percutaneous
transluminal angioplasty for the treatment of superficial femoral
and popliteal peripheral artery disease: 12-month results from the
IN.PACT SFA randomized trial. Circulation. 131:495–502. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
McKinsey JF, Goldstein L, Khan HU, Graham
A, Rezeyat C, Morrissey NJ, Sambol E and Kent KC: Novel treatment
of patients with lower extremity ischemia: Use of percutaneous
atherectomy in 579 lesions. Ann Surg. 248:519–528. 2008.PubMed/NCBI
|
|
41
|
Wissgott C, Kamusella P, Lüdtke C and
Andresen R: Excimer laser atherectomy after unsuccessful
angioplasty of TASC C and D lesions in femoropopliteal arteries. J
Cardiovasc Surg (Torino). 54:359–365. 2013.PubMed/NCBI
|
|
42
|
Lüdtke CW, Scheer F, Kamusella P, Wissgott
C and Andresen R: Transpopliteal balloon-assisted excimer-laser
atherectomy for the treatment of chronic femoropopliteal
occlusions: Feasibility and initial results. Clin Med Insights
Cardiol. 8 (Suppl 2):S23–S28. 2014.
|
|
43
|
Sangiorgi G, Lauria G, Airoldi F, Godino
C, Politi L, Colombo A, Clerici G, Modena MG and Biondi-Zoccai G:
Retrograde popliteal access as bail-out strategy for challenging
occlusions of the superficial femoral artery: A multicenter
registry. Catheter Cardiovasc Interv. 79:1188–1193. 2012.
View Article : Google Scholar : PubMed/NCBI
|