Introduction
Hematuria is the most common symptom of upper
urinary tract urothelial carcinomas (UUTUC) (1). Early diagnosis of UUTUC is important,
as early treatment of UUTUC increases overall patient survival
(2). There are several established
methods of evaluating hematuria from the UUT. Patients with
hematuria can be diagnosed by radiology, urine cytology, cystoscopy
or fluorescence in situ hybridization (3). Multi-detector computed tomographic
urography (MDCTU) has replaced intravenous pyelography and has
become the gold standard for detection of UUT tumors (4). The sensitivity of these methods is
directly related to the tumor size (5,6): i) For
tumors of 5-10 mm in diameter, the MDCTU sensitivity is 97%; ii)
for tumors with a diameter of <5 mm, the sensitivity is reduced
to 89%; and iii) when the tumor diameter is <3 mm, the
sensitivity is ~40%. For patients who have hematuria of the UUT but
negative MDCTU and cytology results, the probability of having
urothelial carcinoma is 5-10% (7).
As the muscularis of the renal pelvis and ureter is relatively
weaker than the muscular layer of the bladder, tumors may easily
invade the muscle layer, subsequently leading to metastasis
(8). Therefore, early detection of
UUT tumors is necessary to improve survival rates.
With the progression of endoscopic technology,
ureteroscopy now provides a new way to detect UUTUC. Since
retrograde flexible ureteroscopy (RFU) can observe the entire UUT
directly, it is considered to be an important diagnostic method for
judging the location of hematuria and finding early UUT carcinomas
(9). According to the European
Association of Urology guidelines, all patients with UUTUC should
accept an ureteroscopy examination before treatment (9).
For the past few years, RFU has been widely
performed in nearly all Grade IIIA hospitals in China; there were
1308 Grade IIIA hospitals nationwide by the end of 2016(10). However, in most situations the
flexible ureteroscope is used to search for stones in renal calices
and renal pelvis (11). The present
study investigated 65 cases with UUT bleeding who accepted RFU and
34 cases who were diagnosed as UUTUC at Ningbo First Hospital from
June 2006.
Patients and materials
Patients
The ethics approval of the present study was
obtained from the Ethics Committees of Ningbo First Hospital. All
patient consent was obtained before undergoing RFU. Between June
2006 and August 2018, 65 patients (male, 38; female, 27; mean age,
63 years) underwent UUT examination by RFU to determine the
etiology of hematuria originating from UUT in Ningbo First
Hospital. The inclusion criteria were as follows: i) Patients had
painless hematuria; and ii) patients underwent cystoscopy and MDCTU
before the RFU. The exclusion criteria were as follows: i) Position
of bleeding was located in bladder; and ii) patients could be
diagnosed correctly for other diseases such as lower urinary tract
infections or bladder carcinoma.
MDCTU revealed masses in 33 cases. There were 13
cases that exhibited ureteral dilatation, hydronephrosis or
ureteral stenosis, but without evidence of UUT tumors. In total,
five cases had renal cysts and 14 cases did not have obvious
abnormalities. After a complete RFU examination of the entire UUT,
patients with suspicious of neoplasms were biopsied. If the
neoplasm was confirmed to be malignant, a nephroureterectomy would
be performed directly or within 2 weeks after RFU. Patients who
presented with negative findings were followed up regularly.
Hematoxylin-eosin staining
Tumor tissue was fixed with 4% PFA for 1 h at room
temperature, embedded in paraffin and cut into samples of 5 µm
thickness. H&E staining was conducted using a Hematoxylin and
Eosin Staining kit (Shanghai Sixin Biotechnology Co., Ltd.)
according to the manufacturer's protocol, Briefly, thin paraffin
sections were deparaffinized in xylene and rehydrated in a graded
series of aqueous ethanol solution. Following staining with
hematoxylin and eosin, the tissue was sealed by neutral gum.
Samples were observed under an Olympus CKX31 microscope (Olympus
Corporation) at 10X objective.
Statistical analysis
The statistical software program SPSS 22.0 (IBM
Corp.) was used to determine the statistical significance of the
results by comparing the age/sex to the success ratio of flexible
ureteroscopy examination (Table I).
The relationship between age/sex and the ratio was analyzed by
using an independent sample t-test and the Fisher test,
respectively. P<0.05 was considered to indicate a statistically
significant difference.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Characteristic | Patients with UUTUC
or RCC | Patients without
carcinoma | P-value |
|---|
| Number | 35 | 30 | |
| Age (years) | 59.85±16.865 | 66.61±9.236 | 0.037 |
| Success rate of
RFU | 0.857 (30/35) | 0.867 (26/30) | 0.004 |
| Complications | 2 (fever) | 0 | |
Results
All 65 patients received cystoscopy and imaging
examination such as ultrasound and MDCTU before the RFU. All
patients were found to be bleeding from the UUT by cystoscopy. In
total, 33 patients who had positive MDCTU results were considered
to have UUTUC or renal carcinoma. The remaining 32 patients were
not detected to have obvious tumors by MDCTU; only stones,
hydronephrosis, nephropyelitis or ureterostenosis were found.
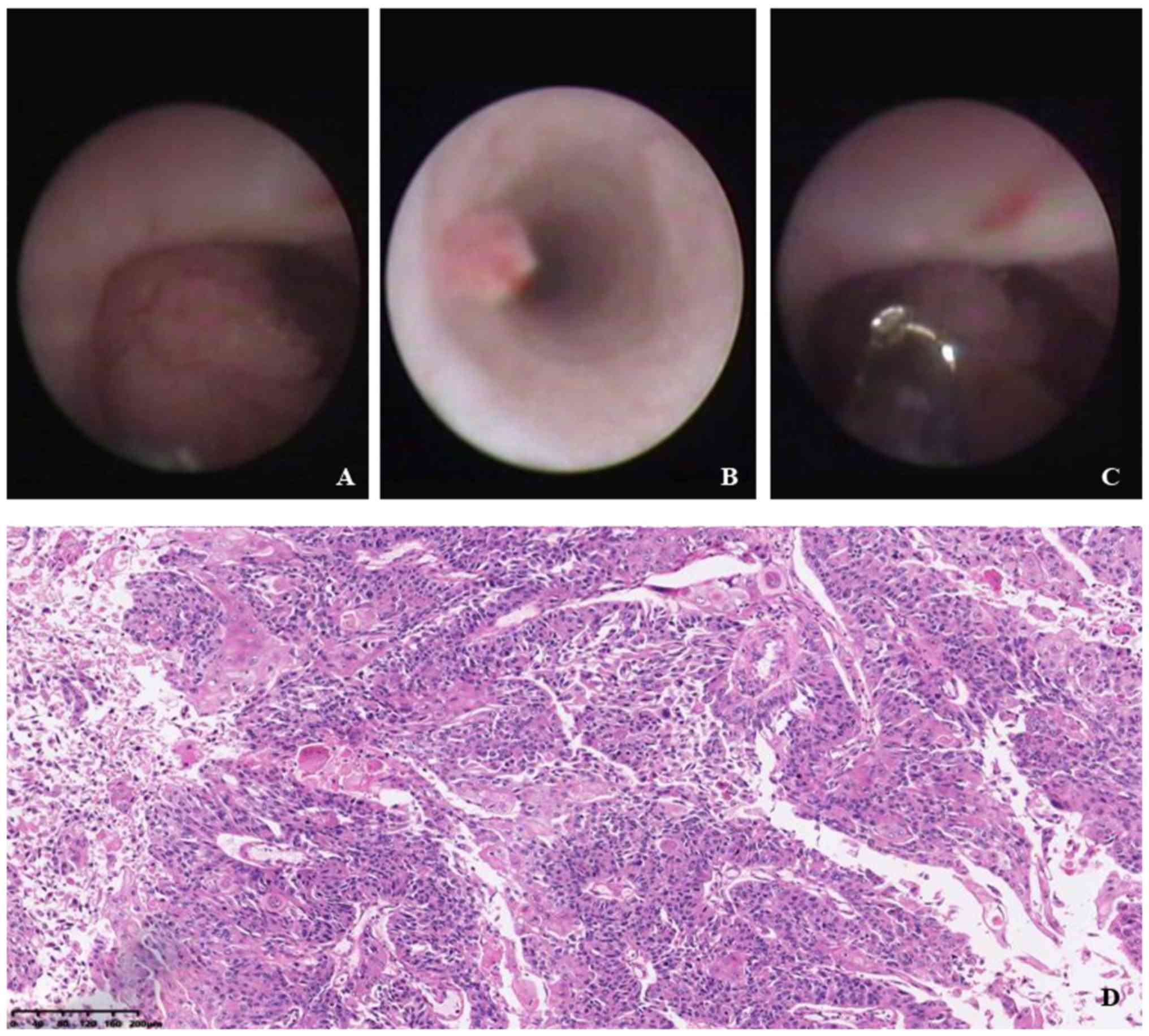
Among the 65 patients only 85.2% (56/65) patients
were examined by RFU successfully. Urothelial masses were found in
37 cases (Fig. 1A and B). Renal calculi were found in two cases
and no obvious abnormalities were found in 17 cases. The 37
patients with urothelial masses who received surgical treatment.
Among them, 17 cases underwent immediate nephroureterectomy after
the RFU and ureteroscopic biopsy. The other 19 patients accepted
nephroureterectomy within 2 weeks after RFU (Fig. 1C). There was one patient who had
renal cell carcinoma treated by radical nephrectomy. Among the 65
patients, 19 patients were considered to have UUTUC and 17 patients
were found to be negative for UUTUC by both RFU and MDCTU (Table II). However, RFU found UUTUC in 11
patients who had negative results from MDCTU, and RFU found
non-neoplastic diseases in nine patients who had positive results
from MDCTU (Table II).
| Table IIPositive and negative results detected
by MDCTU or RFU. |
Table II
Positive and negative results detected
by MDCTU or RFU.
| | MDCTU results | |
|---|
| RFU | + | - | Total |
|---|
| + | 19 | 11 | 30 |
| - | 9 | 17 | 26 |
| Total | 28 | 28 | 56 |
Pathology
Pathology (Fig. 1D)
confirmed UUT epithelial carcinoma in 29 cases (Table III). There was one case was
confirmed as renal clear cell carcinoma. In total, two cases were
confirmed as atypical hyperplasia and two cases were confirmed as
polyps. The present results identified three cases as undetermined
for reasons such as lack of samples or that the pathological
results were inconsistent with the clinical manifestation (data not
shown).
| Table IIIMDCTU and RFU results in all
patients. |
Table III
MDCTU and RFU results in all
patients.
| Confirmed | UUTUCa | Other diseases | Normal | Failed | Total |
|---|
| MDCTU | 33(18) | 21 | 11 | 0 | 65 |
| RFU | 37(29) | 2 | 17 | 9 | 65 |
Patients with RFU
RFU could not be performed in nine patients due to
ureteral stenosis. There were five patients who had positive MDCTU
results, received nephroureterectomy directly and were confirmed to
have transitional cell carcinoma by pathology. In total, four
patients who had negative MDCTU results did not receive surgical
treatment and did not present with abnormalities during the 6 month
follow-up. There were complications in three cases who presented
with a slight fever after the RFU. No cases presented with severe
complications after RFU.
Follow-up
With regards to postoperative follow-up, the present
study did not follow up two patients who were diagnosed with
ureteral stones. The remaining patients were followed up for 6-58
months (average for 34 months). Among them, five patients with
UUTUC were lost to follow up. In total, four patients with UUTUC
died; two succumbed to UUT carcinoma in the third and the fourth
year after the operation and two died due to other diseases (one
died due to prostate cancer after surgery, and the other died
because of renal failure after 14 months). In total, two patients
were found to have bladder tumors. There was one patient who
received transurethral cystectomy 18 months after RFU and was
followed up again for 2 years without recurrence. In total, one
case occurred 14 months after the RFU and received both radical
cystectomy and cutaneous ureterostomy; the patient was then
followed up for 1 year and no obvious abnormalities were found. No
tumor recurrence was detected in the remaining patients. The
present results identified two patients with ureteral polyps who
had no obvious abnormalities after the follow-up. There were two
patients with negative RFU results who were followed up after 58
months and 10 months, and no obvious abnormality was found in
either patient. Due to ureteral stricture, one patient who was not
examined successfully by RFU was not found to have obvious
abnormalities during the 6 months follow up.
Discussion
The most common symptom of UUT tumors is hematuria,
which consists of either macroscopic or microscopic hematuria, and
occurs in 56-98% of patients with urothelial tumors (12,13).
Other sources of hematuria include benign fibroepithelial polyps,
angioma and stone disease (14,15).
Upper urinary tract carcinoma has been prevalent in China in recent
years (16). People with
asymptomatic hematuria have a 3.3% risk of urinary tract malignancy
(17) and multiple factors such as
age, sex, environment or drug abuse have been reported to increase
the risk of urinary tract malignancy (18). As hematuria from the UUT may be
caused by benign or malignant disease, it is important to
differentiate between these to avoid unnecessary surgical
interventions.
In the present study, the sensitivity of RFU for the
diagnosis of UUT tumors was ~78.4% (29/37; Table III) and the sensitivity of MDCTU
was ~54.5% (18/33). In the present study, ureteral stenosis was the
main reason for the failure of ureteroscopy. In nine patients with
ureteral strictures, MDCTU revealed masses in four patients and
these masses were confirmed to be ureteral urothelial carcinomas
after the operation. In total, one patient presented with ureteral
dilatation, hydronephrosis and ureteral stenosis in the
preoperative imaging examination, which was later confirmed to be
ureteral carcinoma after surgery. The present results identified
four cases that were considered to be benign by preoperative
imaging methods and received conservative treatment; no tumors were
found during the follow-up.
Although the complication rate of RFU is low,
complications reported included ureteral perforation, postoperative
fever, impaired renal function and postoperative ureteral stenosis
(19). Ureteral perforation is
usually due to large tumor size or deep resection caused by the
laser, and can generally be treated with an indwelling ureteral
stent (20). Ureteral stricture is a
long-term postoperative complication. The incidence of ureteral
strictures is 0-13%, which has greatly increased in recent years
due to holmium laser-induced thermal injuries to the ureter
(21). In the present study, RFU was
performed as a short-time medical procedure without the holmium
laser treatment. Only three patients had a transient fever and all
recovered within 24 h after antibiotic treatment. Complications
such as renal impairment, ureteral perforation or ureteral stenosis
were not observed in the present study.
Whether RFU increases the risk of tumor cell
metastasis and decreases the survival rate is still inconclusive.
Boorjian et al (22) reported
the long-term follow-up results of 121 patients diagnosed with
UUTUC with a mean follow-up time of 40 months. Boorjian et
al (22) found that the number
of disease-free patients who underwent nephroureterectomy with
imaging and/or urinary cytology results was 81.3% (61/75), and
those who underwent nephroureterectomy after ureteroscopy and laser
ablation was 85.3% (29/34), and therefore concluded that there was
no significant difference between the two methods. Ishikawa et
al (23) conducted a
retrospective study of UUTUC in 208 patients who underwent
nephroureterectomy; 55 received ureteroscopy before surgery and the
other patients only received surgery. Postoperative follow-up found
no significant difference in tumor recurrence between the two
groups (23). The estimated 5 year
tumor-specific survival rate was 88.3% in patients receiving
ureteroscopy and 78.1% in the control group; the difference between
groups was not statistically significant (23). In the present study, 18 patients
received nephroureterectomy immediately after the ureteroscopy and
the remaining 19 patients received the operation within 2 weeks;
surgical procedures were performed after the pathology results were
returned. In the patients that were successfully followed up for
6-58 months (34 months on average), two patients died due to
distant metastasis (5.4%) and two patients were diagnosed with
bladder cancer during the follow-up. There was no evidence that the
ureteroscopic procedure increased the risk of tumor metastasis in
the present study. However, the present study had limitations such
as a small sample size of patients, retrospective design and the
lack of a control group.
The present results indicated RFU was highly
sensitive and specific to the diagnosis of UUT tumors, and had few
complications. The present results suggested RFY could be used as a
routine examination for patients with hematuria originating from
the UUT to improve the detection rate of UUT tumors and to avoid
unnecessary surgeries.
Acknowledgements
The authors would like to thank Dr Hui-Zhi Zhang at
Ningbo Diagnostic Pathology Center for her assistance in the review
of the pathological slides.
Funding
The present study was supported in part by The
Ningbo Natural Science Fund (grant no. 2018A610297).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
KYW and JSH searched the literature, extracted the
data and wrote the manuscript. JSH, LF, DXZ, QL and GHX performed
the RFU. DMN and MH conducted literature search, analyzed the data
and edited the manuscript. GHX and QM designed the study and
revised the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The ethics approval of this study was obtained from
The Ethics Committees of Ningbo First Hospital. Patient consent was
obtained before undergoing RFU.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chlapoutakis K, Theocharopoulos N,
Yarmenitis S and Damilakis J: Performance of computed tomographic
urography in diagnosis of upper urinary tract urothelial carcinoma,
in patients presenting with hematuria: Systematic review and
meta-analysis. Eur J Radiol. 73:334–338. 2010.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rouprêt M, Babjuk M, Compérat E, Zigeuner
R, Sylvester RJ, Burger M, Cowan NC, Böhle A, Van Rhijn BW,
Kaasinen E, et al: European association of urology guidelines on
upper urinary tract urothelial cell carcinoma: 2015 update. Eur
Urol. 68:868–879. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Wang J, Wu J, Peng L, Tu P, Li W, Liu L,
Cheng W, Wang X, Zhou S, Shi S, et al: Distinguishing urothelial
carcinoma in the upper urinary tract from benign diseases with
hematuria using FISH. Acta Cytol. 5:533–538. 2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Cowan NC, Turney BW, Taylor NJ, McCarthy
CL and Crew JP: Multidetector computed tomography urography for
diagnosing upper urinary tract urothelial tumour. BJU Int.
99:1363–1370. 2007.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Rouprêt M, Yates DR, Comperat E and
Cussenot O: Upper urinary tract urothelial cell carcinomas and
other urological malignancies involved in the hereditary
nonpolyposis colorectal cancer (lynch syndrome) tumor spectrum. Eur
Urol. 54:1226–1236. 2008.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Colin P, Koenig P, Ouzzane A, Berthon N,
Villers A, Biserte J and Rouprêt M: Environmental factors involved
in carcinogenesis of urothelial cell carcinomas of the upper
urinary tract. BJU Int. 104:1436–1440. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Wang LJ, Wong YC, Huang CC, Wu CH, Hung SC
and Chen HW: Multidetector computerized tomography urography is
more accurate than excretory urography for diagnosing transitional
cell carcinoma of the upper urinary tract in adults with hematuria.
J Urolo. 183:48–55. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Osmanov YI, Gaibov ZA, Kogan EA,
Radenska-Lopovok SG and Tursunov KZ: Comparative morphological
characteristics and immunophenotype of urothelial carcinomas of the
renal pelvis and bladder. Arkhiv Patol. 80:23–32. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Taneja SS: Re: European guidelines for the
diagnosis and management of upper urinary tract urothelial cell
carcinomas: 2011 update. J Urol. 186(455)2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
National Health Commission of the People's
Republic of China. Statistics on the Development of Health and
Family Planning in China in 2016 (EB/OL). http://www.nhc.gov.cn/guihuaxxs/s10748/201708/d82fa7141696407abb4ef764f3edf095.shtml.
2017-08-18.
|
|
11
|
Ding J, Xu D, Cao Q, Huang T, Zhu Y, Huang
K, Chen Y, Liang C, Qi J and Huang Y: Comparing the efficacy of a
multimodular flexible ureteroscope with its conventional
counterpart in the management of renal stones. Urology. 86:224–229.
2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Guinan P, Vogelzang NJ, Randazzo R, Sener
S, Chmiel J, Fremgen A and Sylvester J: Renal pelvic cancer: A
review of 611 patients treated in illinois 1975-1985. Cancer
incidence and end results committee. Urology. 40:393–399.
1992.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Raabe NK, Fossã SD and Bjerkehagen B:
Carcinoma of the renal pelvis. Experience of 80 cases. Scand J Uro
Nephrol. 26:357–361. 1992.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Brito AH, Mazzucchi E, Vicentini FC,
Danilovic A, Chedid Neto EA and Srougi M: Management of chronic
unilateral hematuria by ureterorenoscopy. J Endourol. 23:1273–1276.
2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Dolan R, Morton S and Granitsiotis P:
Presentation of a benign fibroepithelial polyp with frank
haematuria: An unusual diagnosis. Scott Med J. 60:24–26.
2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Lin SH, Luo HL, Chen YT and Cheng YT:
Using hematuria as detection of post-kidney transplantation upper
urinary tract urothelial carcinoma is associated with delayed
diagnosis of cancer occurrence. Transplant Proc. 49:1061–1063.
2017.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Davis R, Jones JS, Barocas DA, Castle EP,
Lang EK, Leveillee RJ, Messing EM, Miller SD, Peterson AC, Turk TM,
et al: Diagnosis, evaluation and follow-up of asymptomatic
microhematuria (AMH) in adults: AUA guideline. J Urol.
188:2473–2481. 2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Lisanti CJ, Toffoli TJ, Stringer MT,
DeWitt RM and Schwope RB: CT evaluation of the upper urinary tract
in adults younger than 50 years with asymptomatic microscopic
hematuria: Is IV contrast enhancement needed? AJR Am J Roentgenol.
203:615–619. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
De S, Autorino R, Kim FJ, Zargar H,
Laydner H, Balsamo R, Torricelli FC, Di Palma C, Molina WR, Monga M
and De Sio M: Percutaneous nephrolithotomy versus retrograde
intrarenal surgery: A systematic review and meta-analysis. Eur
Urol. 67:125–137. 2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
May PC, His RS, Tran H, Stoller ML, Chew
BH, Chi T, Usawachintachit M, Duty BD, Gore JL and Harper JD: The
morbidity of ureteral strictures in patients with prior
ureteroscopic stone surgery: Multi-Institutional outcomes. J
Endourol. 32:309–314. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Troy AJ, Anagnostou T and Tolley DA:
Flexible upper tract endoscopy. BJU Int. 93:671–679.
2004.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Boorjian S, Ng C, Munver R, Palese MA,
Vaughan ED Jr, Sosa RE, Del Pizzo JJ and Scherr DS: Impact of delay
to nephroureterectomy for patients undergoing ureteroscopic biopsy
and laser tumor ablation of upper tract transitional cell
carcinoma. Urology. 66:283–287. 2005.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ishikawa S, Abe T, Shinohara N,
Harabayashi T, Sazawa A, Maruyama S, Kubota K, Matsuno Y Osawa T,
Shinno Y, et al: Impact of diagnostic ureteroscopy on intravesical
recurrence and survival in patients with urothelial carcinoma of
the upper urinary tract. J Urol. 184:883–887. 2010.PubMed/NCBI View Article : Google Scholar
|