Introduction
Teenage pregnancy is defined by the United Nations
Children's Fund (UNICEF) as being pregnant between the age of 13
and 19 years (1). Each year, all
over the world 16 million teenage women give birth each year; this
represents ~11% of all births (1).
The real problem is that 95% of all these births occur in low, and
middle income countries (1). Romania
occupies the second place in Europe in teenage pregnancy (1).
Adolescent pregnancies are associated with a high
number of risks for the newborn and mother (2,3). The
pathologies associated with teenage pregnancy are: Preterm
delivery, low birthweight, gestational hypertension,
preeclampsia-eclampsia and neonatal death (4-7).
Due to these conditions, an increased number of emergency caesarean
extractions is performed in adolescent pregnant patients (2,4,5).
It is estimated that the mortality due to
obstetrical complications in a pregnant adolescent is twice that in
a woman between 20 and 30 years (8).
Obstetrical related pathologies are the main cause of mortality in
teenagers (8-11).
It is estimated that 27.5% of the maternal deaths in this group of
patients occur after vaginal delivery, 18.7% due to complications
of pregnancy, 9.4% due to other maternal care related to the fetus
and 5.4% of deaths due to abortion (8).
Gestational diabetes and fetal anomalies are also
relatively frequent in teenage pregnancy (2). In a retrospective cohort study 2 groups
of pregnant patients were analyzed and compared: A group of
adolescents aged 11-19 years and a second group of patients aged
20-24 years were included (2). In
this study the incidence of gestational diabetes, fetal anomalies
and preeclampsia were compared. Torvie et al (2) demonstrated that preeclampsia,
gestational diabetes and fetal anomalies are more frequent in young
teenagers aged 11-14 years). However, caesarean extraction was more
rare in adolescents under 17 years at 28.1%, increasing with age,
reaching 36.2% between 18-24 years (2).
Pregnancy during adolescence represents an important
challenge also for the physical status of the patient (4,12). As
adolescence is a transitional period of physical and psychological
development between childhood and adulthood, pregnancy at this age
can determine imbalances that can be transitory or can become
chronic if they are not properly managed (12).
The aim of this study was to analyze the
pregnancy-related conditions, the way of delivery and the neonatal
outcome of all the patients who delivered in the Department of
Obstetrics and Gynecology of University Emergency Hospital in
Bucharest, a tertiary unit in Romania in a period of 5 years.
Patients and methods
An observational, retrospective study was performed
on a group of 686 patients, aged 12-19 years, who delivered in the
Department of Obstetrics and Gynecology of University Emergency
Hospital in Bucharest, between January 1, 2014 and December 31,
2018. The pregnant women were divided into two age groups. In the
first group pregnant patients aged under 18 years were analyzed,
the group represented patients who had not reached legal adulthood
while in a second group pregnant adolescents aged 18-19 years. The
information regarding pregnancy, delivery outcomes and neonatal
data were retrieved from the hospitalization sheets and the Base
Data System of University Emergency Hospital in Bucharest.
Maternal age was defined as that recorded at the
time of delivery. Expulsions of the gestational product after
completed 24 weeks were defined as deliveries, while before 24
weeks were considered abortions and were not included in this
study.
It was first analyzed if the patients in the two
groups underwent routine medical visits during pregnancy (defined
as prenatal screening) which include: physical examination, fetal
ultrasound scan and laboratory tests.
The age of the patients were compared and the rate
of caesarean extraction and vaginal birth, the obstetrical
complications and the management of patients were analyzed in the
two groups. The outcome of the newborns was assessed based on Apgar
score at 1 min and birth weight.
Results
A total of 686 adolescents were included in study.
Three hundred and forty-three patients aged 12-17 years were
analyzed in group A, while the others aged 18-19 years formed group
B.
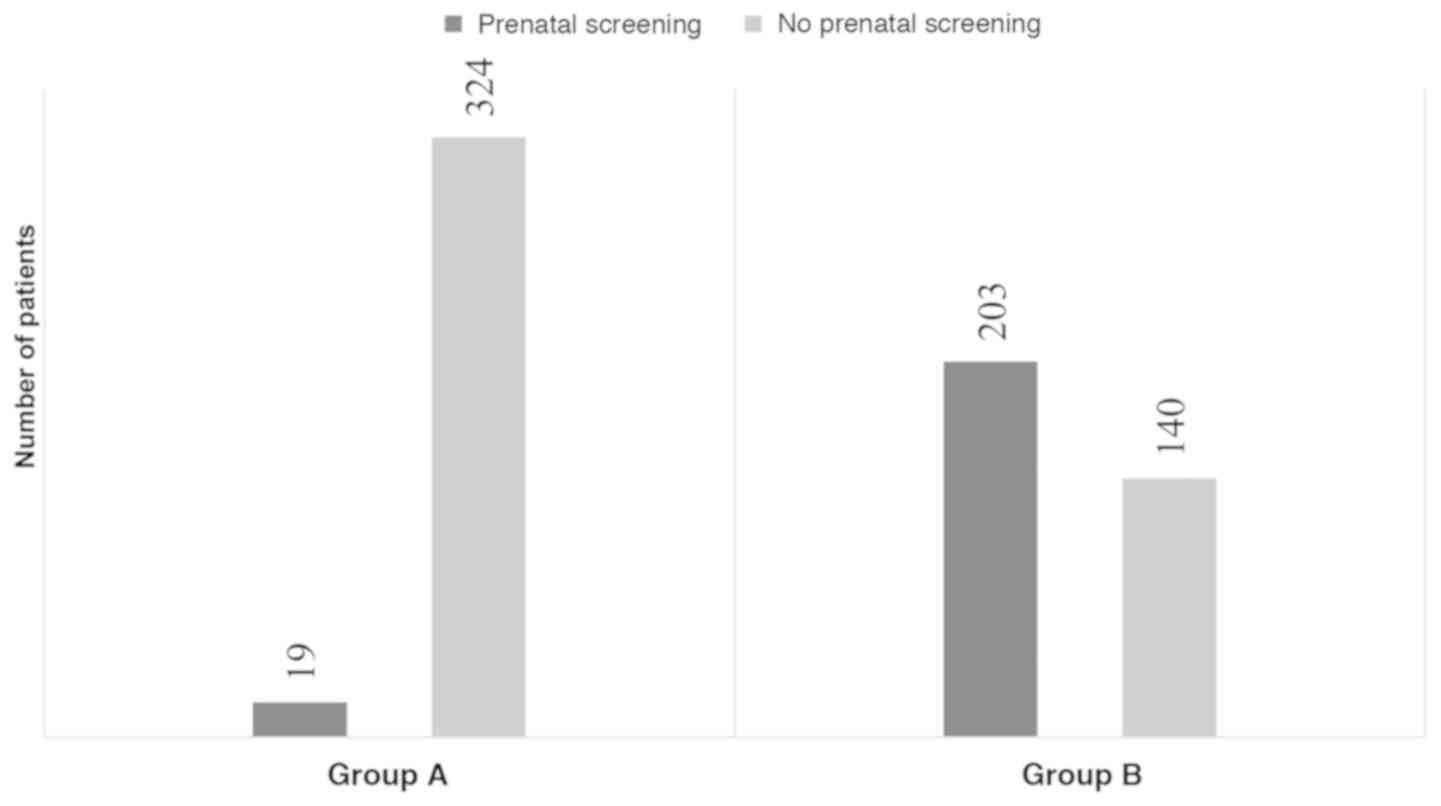
First it was evaluated if the patients included into
the two age groups underwent routine medical visits (Fig. 1). An enormous percent of patients
included in this study did not undergo any routine medical visits,
94.46% (n=324) of the patients in group A and 40.81% (n=140) in
group B did not undergo any prenatal screening (Fig. 1).
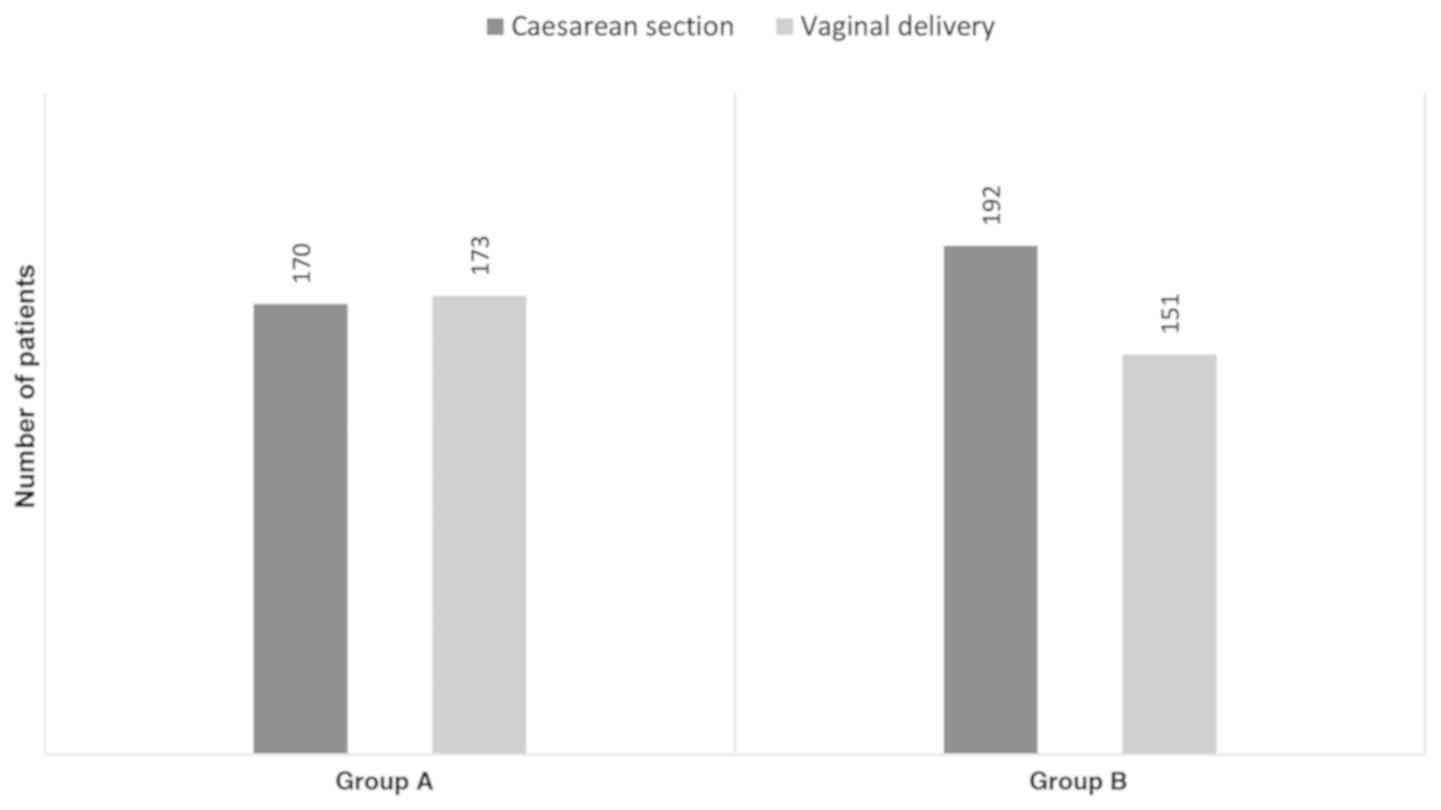
Analyzing the delivery method (Fig. 2), an approximately equal number of
vaginal spontaneous deliveries were recorded (n=173) and caesarean
extraction (n=170) in patients from group A. In group B caesarean
section was performed in 55.97% (n=192) of the cases. The rest of
the patients delivered vaginally; instrumental delivery was
performed in 5 cases, forceps delivery in 4 cases and one vacuum
assisted delivery.
The indications of caesarean extraction of patients
evaluated in the two groups were analyzed and compared (Table I). The most frequent indication for
caesarean extraction was cephalo-pelvic disproportion, while fetal
distress was the second most common indication, in both analyzed
groups (Table I).
 | Table IDistribution of the patients in the
two analyzed groups according to the indication for caesarean
section. |
Table I
Distribution of the patients in the
two analyzed groups according to the indication for caesarean
section.
| Indication of
caesarean section | Group A (n=170), %
(n) | Group B (n=192), %
(n) |
|---|
| Cephalo-pelvic
disproportion | 25.88(44) | 21.3(41) |
| Fetal distress | 20.59(35) | 18.7(36) |
| Uterine Scar after
caesarean section | 15.88(27) | 14.06(27) |
| Dystocic
presentation | 7.65(13) | 11.46(22) |
| Preeclampsia | 6.47(11) | 7.81(15) |
| Placenta Praevia | 3.53(6) | 5.21(10) |
| Negative induction of
labor | 8.24(14) | 10.94(21) |
| Intrauterine growth
restriction | 2.35(4) | 3.65(7) |
| Other | 9.41(16) | 6.77(13) |
Surprising, the third most frequent indication for
this type of delivery in entire lot of adolescents analyzed was the
high risk of rupture of uterine scar after caesarean section, 27
patients from each group. The youngest patient with a uterine scar
after caesarean section was a 16-year old patient.
It is important to mention that in the category of
‘Other’ (indication for caesarean section) of both groups included
patients with various obstetrical and non-pregnancy-related
pathologies. Group A patients diagnosed with umbilical cord
prolapse, HIV positive, uterine malformations, lymphomas, or other
operated malignancies were included. Group B included patients
diagnosed with fetal malformations, retinal dystrophy, or severe
depression.
The outcome of the neonates was evaluated using the
Apgar score at 1 min. The neonatal status of all the fetuses that
were delivered by patients pertaining to both groups were analyzed
and compared (Table II).
| Table IIDistribution of the patients in the
two analyzed groups according to the Apgar score of the fetus at 1
min and according to the method of delivery in each group. |
Table II
Distribution of the patients in the
two analyzed groups according to the Apgar score of the fetus at 1
min and according to the method of delivery in each group.
| | Group A (n=343
cases) | Group B (n=343
cases) |
|---|
| Apgar score | % of 343 cases
(n) | Caesarean section %
of 170 cases (n) | Vaginal delivery % of
173 cases (n) | % of 343 cases
(n) | Caesarean section %
of 192 cases (n) | Vaginal delivery % of
151 cases (n) |
|---|
| 1 | 0.87(3) | 1.17(2) | 0.57(1) | 1.16(4) | 1.56(3) | 0.66(1) |
| 2 | 0 | 0 | 0 | 0.29(1) | 0 | 0.66(1) |
| 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| 4 | 0 | 0 | 0 | 0.58(2) | 0 | 1.32(2) |
| 5 | 0.58(2) | 1.17(2) | 0 | 0.87(3) | 0.52(1) | 1.32(2) |
| 6 | 1.74(6) | 2.35(4) | 1.15(2) | 2.33(8) | 4.17(8) | 0 |
| 7 | 3.79(13) | 4.11(7) | 3.46(6) | 6.7(23) | 6.77(13) | 6.62(10) |
| 8 | 20.11(69) | 22.35(38) | 17.91(31) | 17.2(59) | 17.19(33) | 17.22(26) |
| 9 | 51.89(178) | 57.64(98) | 46.24(80) | 54.81(188) | 63.54(122) | 43.71(66) |
| 10 | 20.99(72) | 11.17(19) | 30.63(53) | 16.03(55) | 6.25(12) | 28.48(43) |
Table II shows that
most patients analyzed delivered a fetus who received a calculated
Apgar score of 9; a good immediate evolution. The mean Apgar score
was 8.69 and the mean Apgar score for group A was 8.78 and for
group B was 8.60. It was noted that twice as many of the patients
in group B delivered a baby with an Apgar score between 1 and 5,
compared with group A.
Giving the fact that fetal distress was the second
most common indication for caesarean section in both analyzed
groups we were interested to evaluate if there are significant
differences of fetal outcome (interpreted in relation with Apgar
score) and the method of delivery (Table II). As shown in Table II no significant differences of
Apgar score were noted in relation with the method of delivery.
The weight of the fetuses of the patients were also
analyzed and compared in the two groups (Table III). The newborns of patients
pertaining to both groups were distributed into 8 categories of
fetal weight.
| Table IIIDistribution of the patients in the
two analyzed groups according to the weight of the fetus and
according to the method of delivery in each group. |
Table III
Distribution of the patients in the
two analyzed groups according to the weight of the fetus and
according to the method of delivery in each group.
| | Group A (n=343
cases) | Group B (n=343
cases) |
|---|
| Newborn weight
(g) | % of 343 cases
(n) | Caesarean section %
of 170 cases (n) | Vaginal delivery % of
173 cases (n) | % of 343 cases
(n) | Caesarean section %
of 192 cases (n) | Vaginal delivery % of
151 cases (n) |
|---|
| <1,000 | 0.29(1) | 0 | 0.57(1) | 0.58(2) | 0.52(1) | 0.66(1) |
| 1,000-1,499 | 0.87(3) | 1.18(2) | 0.57(1) | 1.45(5) | 0 | 3.31(5) |
| 1,500-1,999 | 1.74(6) | 2.35(4) | 1.15(2) | 1.74(6) | 2.08(4) | 1.32(2) |
| 2,000-2,499 | 11.95(41) | 11.18(19) | 12.71(22) | 5.83(20) | 8.85(17) | 1.99(3) |
| 2,500-2,999 | 34.69(119) | 32.94(56) | 36.41(63) | 29.44(101) | 34.9(67) | 22.52(34) |
| 3,000-3,499 | 36.15(124) | 38.82(66) | 33.52(58) | 44.89(154) | 40.63(78) | 50.33(76) |
| 3,500-4,000 | 13.7(47) | 12.35(21) | 15.02(26) | 14.57(50) | 10.94(21) | 19.21(29) |
| >4,000 | 0.58(2) | 1.18(2) | 0 | 1.45(5) | 2.08(4) | 0.66(1) |
Table III shows
that there are no significant differences between the weights of
fetuses of patients evaluated in the two groups, according to the 8
pre-formed categories.
Giving the fact that cephalo-pelvic disproportion
was the most frequent indication for caesarean extraction in both
analyzed groups we were interested to evaluate if there are
significant differences between the fetal weight and the method of
delivery. The mean weight was 3.028 g, but 20% of all patients
delivered a fetus with a weight under 2,500 g (Table III). The distribution of patients
in group B according to fetal weight is interesting; 19.77% of the
patients who delivered vaginally had a fetus that weighted
>3,500 g, while only 13.02% of the patients who delivered by
caesarean section had a fetus with the same weight. A significant
difference was seen in category 2,000-2,500 g, approximately a
double number of patients delivered by caesarean section in group
B. In group A all fetuses weighing over 4,000 g were delivered by
caesarean section.
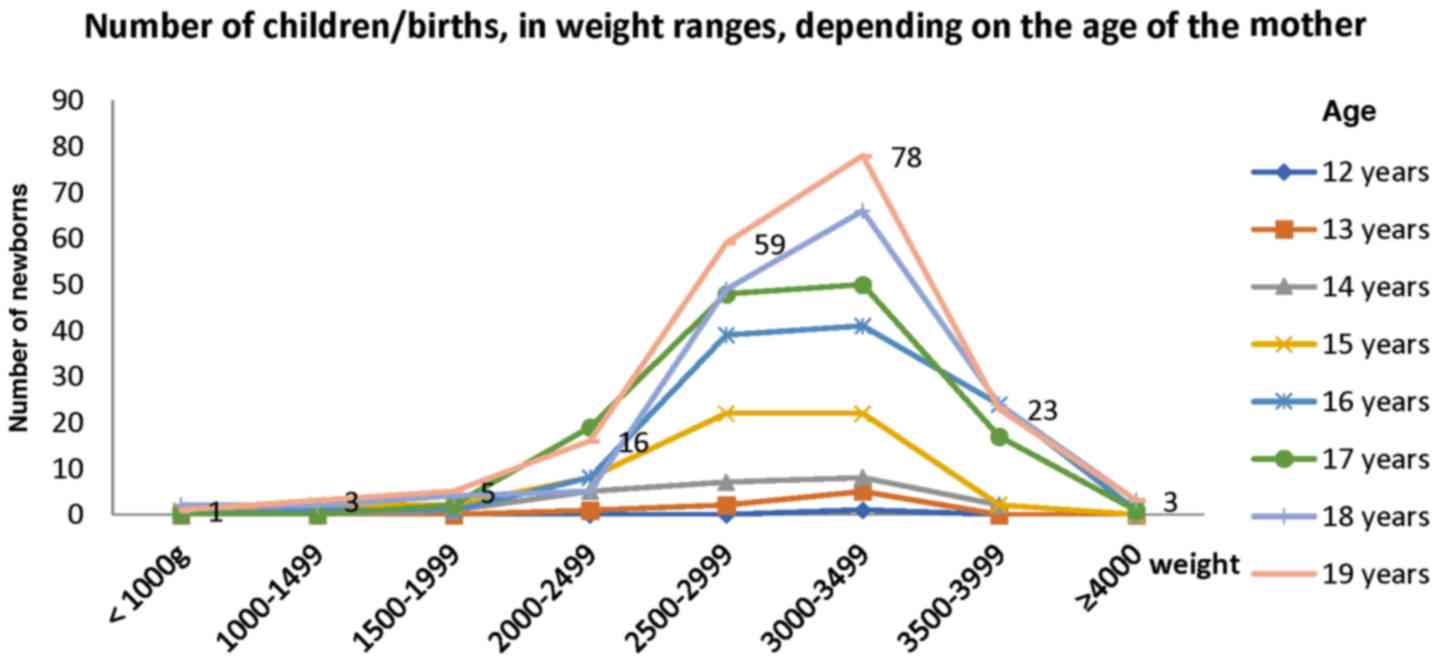
In Fig. 3 it is shown
that most of the analyzed teenagers gave birth to fetuses weighing
between 3,000-3,499 g, even the youngest adolescent, who was 12
years old. Furthermore, even mothers with low age delivered
newborns weighing >3,500 g.
Discussion
Between January 1, 2014 and December 31, 2018, 686
patients, aged between 12 and 19 years, delivered in the Department
of Obstetrics and Gynecology of University Emergency Hospital in
Bucharest, Romania. Unfortunately, 464 of these patients, 94.46% of
the adolescents aged between 12 and 17 years and 40.81% of the
teenagers aged between 18 and 19 years did not undergo any routine
medical visits during pregnancy (Fig.
1). This aspect is particularly important because, as already
highlighted by other specialists, lack of medical visits during
pregnancy in adolescent population involves multiple adverse birth
outcomes increasing both maternal and fetal morbidity and mortality
(13,14). The socioeconomic status of these
patients can also increase the risks highlighted above (13,14).
In our study a high rate of caesarean sections was
observed as a method of delivery in adolescent pregnant patients.
Half of the teenagers aged between 12 and 17 years delivered by
caesarean section. In the group of patients aged between 18 and 19
years we observed an even higher rate of caesarean extraction,
55.97% of the cases (Fig. 2). Torvie
et al (2), in a study in
which 8,028 patients were included, also observed that caesarean
extraction is less frequent in patients aged between 15 and 17
years. However, in another retrospective study, on a period of 37
years, in which patients under 20 years were included, concluded
that women under 20 years had a significantly higher rate of
vaginal delivery compared with women aged between 20 and 30 years
(15).
In our study, in both analyzed groups, the most
frequent indication for caesarean extraction was cephalo-pelvic
disproportion (Table I). However, we
did not detect any significant differences between the fetal weight
and the method of delivery (Table
III). Cephalo-pelvic disproportion is one of the most common
indications for caesarean extraction (16). However, in adolescent population,
rigorous criteria for establishing this diagnosis and therefore
caesarean extraction still need to be evaluated. Jain and Gupta
also observed, in a study on 100 adolescent patients, that
cephalo-pelvic disproportion was the most frequent indication for
caesarean section (17).
In our study, in both analyzed groups, the second
most frequent indication for caesarean extraction was fetal
distress (Table I). Similarly to our
conclusion, Jain and Gupta (17)
also observed that fetal distress was the second most frequent
indication for caesarean section (25% of all caesarean sections).
The fetal outcome was interpreted in relation with the Apgar score.
However, no significant differences of Apgar score were noted in
relation with the method of delivery (Table II). Adequate management and prompt
decision to extract the fetus by caesarean section decreased the
risk of short-, mid- and probably even long-term fetal
complications. Other authors also demonstrated that emergency
caesarean section in adolescents with fetal distress could decrease
fetal morbidity and mortality (18).
An important number of patients in our study, who
delivered by caesarean section were included in the category of
‘Other’ (indication for caesarean section). All these patients had
various obstetrical and non-pregnancy-related pathologies. From
group A we included in this category patients diagnosed with:
umbilical cord prolapse, HIV positive, uterine malformations,
lymphomas, or other operated malignancies. From group B we included
in this category patients diagnosed with fetal malformations,
retinal dystrophy, or severe depression. University Emergency
Hospital in Bucharest is a multidisciplinary medical unit and the
Department of Obstetrics and Gynecology is a tertiary center that
manages a high number of pregnant adolescents with rare conditions
or important comorbidities, which require caesarean delivery in
many cases.
In the present study, in both analyzed groups, the
third most frequent indication for caesarean extraction was uterine
scar after caesarean section (Table
I). As previously discussed an important number of adolescents
deliver by caesarean section in first pregnancy. The risk of
uterine rupture among patients who try to deliver vaginally with a
uterine scar after caesarean section has already been demonstrated
in adult population (19). However,
there are no significant statistical studies regarding this matter
in adolescent population. This is why most obstetricians recommend
delivery by caesarean section if an adolescent has a uterine
scar.
Regarding the results, 464 of the 686 patients
analyzed in our study on adolescent pregnancy did not undergo any
medical visits during pregnancy (Fig.
1). Moreover, most of these patients presented at the Emergency
Room in advanced stages of labor. As shown caesarean extraction was
performed in an important number of cases (Fig. 2). However, the fetal outcome was very
good in the majority of cases (Table
II). The lack of specific protocols regarding the ante-, peri-
and post-natal management of adolescents is probably the cause of
the alarmingly increasing number of patients pertaining to this
group who deliver by caesarean section. This is why future study is
required in this field that is a major health problem
worldwide.
In conclusion, of the 686 patients, aged between 12
and 19 years, who delivered in the Department of Obstetrics and
Gynecology of University Emergency Hospital in Bucharest, 464 did
not undergo any routine medical visits during pregnancy.
Half of the teenagers aged between 12 and 17 years
delivered by caesarean section. In the group of patients aged
between 18 and 19 years an even higher rate of caesarean extraction
at 55.97% of the cases was observed. The most frequent indications
for caesarean extraction were cephalo-pelvic disproportion, fetal
distress and uterine scar after caesarean section.
The lack of specific protocols regarding the ante-,
peri- and post-natal management of adolescents is probably the
cause of the alarmingly increasing number of patients pertaining to
the group who deliver by caesarean section.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AVU and OM collected, analyzed and interpreted the
patient data regarding adolescent pregnancy and the outcome of
delivery. REB, DN and MMC were involved in the conception of the
study and substantially contributed to the writing of the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cook SM and Cameron ST: Social issues of
teenage pregnancy. Obstet Gynecol Reprod Med. 25:243–248. 2015.
|
|
2
|
Torvie AJ, Callegari LS, Schiff MA and
Debiec KE: Labor and delivery outcomes among young adolescents. Am
J Obstet Gynecol. 213:95.e1–95.e8. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Fraser AM, Brockert JE and Ward RH:
Association of young maternal age with adverse reproductive
outcomes. N Engl J Med. 332:1113–1117. 1995.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Gortzak-Uzan L, Hallak M, Press F, Katz M
and Shoham-Vardi I: Teenage pregnancy: Risk factors for adverse
perinatal outcome. J Matern Fetal Med. 10:393–397. 2001.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Chen XK, Wen SW, Fleming N, Demissie K,
Rhoads GG and Walker M: Teenage pregnancy and adverse birth
outcomes: A large population based retrospective cohort study. Int
J Epidemiol. 36:368–373. 2007.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ganchimeg T, Ota E, Morisaki N, Laopaiboon
M, Lumbiganon P, Zhang J, Yamdamsuren B, Temmerman M, Say L,
Tunçalp Ö, et al: WHO Multicountry Survey on Maternal Newborn
Health Research Network: Pregnancy and childbirth outcomes among
adolescent mothers: A World Health Organization multicountry study.
BJOG. 121 (Suppl 1):40–48. 2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hoque M and Hoque S: Comparison of
perinatal and obstetrics outcomes among early adolescents, late
adolescents and adult pregnant women from rural South Africa. East
Afric J Pub Health. 7:171–176. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
González-Andrade F and Saeteros-Cordero X:
Pregnancy in adolescence and adverse neonatal outcomes in
Ecuadorian mestizo newborns. Pediatr Neonatol. 61:216–223.
2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Sánchez-Gómez A, Cevallos W, Grijalva MJ,
Silva-Ayçaguer LC, Tamayo S, Jacobson JO, Costales JA,
Jiménez-Garcia R, Hernández-Barrera V, Serruya S, et al: Social
factors associated with use of prenatal care in Ecuador. Rev Panam
Salud Publica. 40:341–346. 2016.PubMed/NCBI
|
|
10
|
Parra-Pingel PE, Quisiguiña-Avellán LA,
Hidalgo L, Chedraui P and Pérez-López FR: Pregnancy outcomes in
younger and older adolescent mothers with severe preeclampsia.
Adolesc Health Med Ther. 8:81–86. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Svanemyr J, Guijarro S, Riveros BB and
Chandra-Mouli V: The health status of adolescents in Ecuador and
the country's response to the need for differentiated healthcare
for adolescents. Reprod Health. 14(29)2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Paladugu RK, Donipudi PC, Chimata D and
Jasti M: Adolescent pregnancy and its outcomes: A cross-sectional
study. Int J Comm Med Pub Health. 5:4408–4414. 2018.
|
|
13
|
Rogers MM, Peoples-Sheps MD and Suchindran
C: Impact of a social support program on teenage prenatal care use
and pregnancy outcomes. J Adolesc Health. 19:132–140.
1996.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Bohîlțea RE, Zugravu CA, Neacsu A, Navolan
D, Berceanu C, Nemescu D, Bodean O, Turcan N, Baros Al and Cîrstoiu
MM: The prevalence of vitamin D deficiency and its obstetrical
effects. A prospective study on Romanian patients. Rev Chim.
70:1228–1233. 2019.
|
|
15
|
Tyrberg RB, Blomberg M and Kjølhede P:
Deliveries among teenage women - with emphasis on incidence and
mode of delivery: A Swedish national survey from 1973 to 2010. BMC
Pregnancy Childbirth. 13:204–214. 2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Munteanu O, Ispas A, Berceanu C and
Vladareanu S: Development of scoring system for evaluating the risk
of vephalopelvic disproportion. Res Sci Today. 7:120–125. 2014.
|
|
17
|
Jain P and Gupta M: Maternal outcome in
teenage pregnancy. Indian J Obstet Gynecol Res. 6:263–267.
2019.
|
|
18
|
Levy DM: Emergency Caesarean section: Best
practice. Anaesthesia. 61:786–791. 2006.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Smith D, Stringer E, Vladutiu CJ, Zink AH
and Strauss R: Risk of uterine rupture among women attempting
vaginal birth after cesarean with an unknown uterine scar. Am J
Obstet Gynecol. 213:80.e1–80.e5. 2015.PubMed/NCBI View Article : Google Scholar
|