Introduction
Clavicle fractures account for 5% of all fractures
in adults and are usually as a result of sports-associated
accidents or motor vehicle collisions (1). Approximately 80% of clavicular
fractures involve the midshaft and >70% of such fractures are
usually displaced (2,3). Traditionally, midshaft clavicular
fractures (MSCF) have been treated non-surgically, as early
evidence suggested that clavicular non-unions were rare and
clavicular malunion, observed radiographically, was clinically
irrelevant (4). However, since
higher non-union rates and increased functional deficits following
non-operative management of displaced MSCF were reported more
recently, there has been a gradual shift towards internal fixation
as a treatment alternative for MSCF (5).
A number of plate and intramedullary fixation
devices have been used to hasten recovery and early return to daily
activities following MSCF. However, the optimal fixation method
remains a matter of debate (6).
Plate fixation provides immediate rigid fixation with rotational
stability and may be less technique-sensitive. However,
hypertrophic scarring, skin irritation due to implant prominence,
infections and implant failure are potential drawbacks (7). On the other hand, intramedullary
fixation is less invasive with comparatively reduced implant
prominence and better cosmetic results. However, it has certain
disadvantages, including the requirement of intra-operative
radiation exposure, injury to neurovascular structures and the need
for implant removal to prevent migration (8).
A number of meta-analyses, published in the years
2015-16, have compared clinical outcomes following plate vs.
intramedullary fixation of MSCF (6,9-12).
The results of these meta-analyses, however, have been conflicting.
Certain reviews suggested that intramedullary fixation is superior
to plate fixation in the management of MSCF (10-12),
while others reported no significant differences (9,13). The
conflicting results among previous studies have resulted in
dilemmas for clinicians looking for level-1 evidence to choose
between the different fixation methods for MSCF. In view of the
discordant results of previous meta-analyses and new trials
published thereafter (14,15), there was a requirement for a more
robust and updated systematic review and meta-analysis comparing
clinical outcomes following plate vs. intramedullary fixation of
MSCF, which was provided by the present study.
Data and methods
Literature search strategy and
inclusion criteria
The present systematic review and meta-analysis was
performed in accordance with the recommendations of the Preferred
Reporting Items for Systematic Reviews and Meta-analyses statement
(16) and the Cochrane Handbook for
Systematic Reviews of Intervention (17). The Population, Intervention,
Comparison, Outcome and Study design outline was used for including
studies (16). The following studies
were included: Randomised controlled trials (RCTs) conducted on
adult patients (age, >18 years) with MSCF (Population);
evaluating any type of plate fixation (Intervention); comparing it
with any type of intramedullary fixation (Comparison) and assessing
post-operative shoulder function and complications (Outcomes).
Quasi-RCTs (trials where the randomisation method was
inappropriate, including an alternate/odd-even numbering technique
for randomisation) were excluded. In studies where the
randomisation method was not described, the corresponding authors
were contacted for clarification. In the case of no response, the
studies were included in the meta-analysis and marked with ‘unclear
risk of bias’ for randomisation. Non-randomised trials,
retrospective studies, case-series and studies not published in the
English language were also excluded.
The PubMed, Scopus, BioMed Central, Cochrane Central
Register of Controlled Trials and Google Scholar databases were
searched for entries from inception up to 1st July 2019. The
following key words were used for the literature search:
‘Clavicle’, ‘clavicle fracture’, ‘surgery’, ‘intramedullary
fixation’, ‘plate fixation’, ‘titanium elastic nail’, ‘fixation’,
‘randomised controlled trials’, ‘shoulder function’ and
‘complications’. In addition, references of selected studies and
review papers on the subject were hand-searched to identify any
further missed studies.
Data extraction and outcomes
The literature search was performed by two reviewers
(SM and WJ) independently. Articles were screened by their titles
and abstracts. The articles selected then underwent full-text
evaluation for inclusion in the review. Any discrepancies were
settled by consensus. Data were extracted from the included trials
by two independent reviewers (SM and WJ) using an abstraction form.
The following details were extracted: Authors, year of publication,
number of participants, inclusion/exclusion criteria, type of
fixation used, rehabilitation protocol, shoulder function and
complications.
The primary outcome was long-term shoulder function
assessed after a follow-up of at least 6 months. The two commonly
scored shoulder function questionnaires, the Constant-Murley
Shoulder Outcome questionnaire (16)
and the Disabilities of the Arm, Shoulder and Hand questionnaire
(DASH) (17), were used. Secondary
outcomes were the incidence of complications requiring non-routine
surgery (termed as treatment failure) and complications not
requiring non-routine surgery. This classification was sourced from
a previous meta-analysis by Hussain et al (18). Any complication such as non-union,
malunion, implant failure/fracture and refracture requiring
non-routine re-intervention, was judged as treatment failure. Other
complications, including infection, hypertrophic scar,
paraesthesia, dysesthesia, skin irritation, implant prominence, any
asymptomatic malunion/non-union or any other minor complication not
requiring re-intervention were grouped under ‘complications not
requiring non-routine surgery’. Pin removal and routine hardware
removal were not included as complications.
Risk of bias
The quality of included studies was assessed using
the Cochrane Collaboration risk assessment tool for RCTs (19). Risk of bias (low, unclear or high)
was rated for random sequence generation, allocation concealment,
blinding of participants and personnel, blinding of outcome
assessment, incomplete outcome data, selective reporting and other
biases. A score of 2 was given for low risk of bias, a score of 1
for unclear risk of bias and a score of 0 for high risk of bias.
Studies were then categorized depending on the overall score. A
score of 0-5 was considered to indicate low quality, a score of
6-10 medium quality and a score of 11-14 high quality.
Statistical analysis
Shoulder function scores were presented as the mean
and standard deviation (SD). Complications were presented as the
number of events in each group. A random-effects model was used for
the meta-analysis. Continuous data were pooled and differences
between groups were presented as the mean difference (MD) and 95%
CI. Categorical data were summarised using the Mantel-Haenszel risk
ratio (RR) and 95% CI. The I2 statistic was used to
assess heterogeneity, wherein values of 25-50% denoted low, 50-75%
denoted medium and >75% denoted considerable heterogeneity.
Review Manager (version 5.3; Cochrane Collaboration) was used for
the meta-analysis. A sensitivity analysis was performed to assess
the influence of each study on the pooled effect size. By using the
one-study-out method, it was evaluated whether deletion of one
individual study would significantly change the results of the
meta-analysis. A sub-group analysis was performed for studies
excluding comminuted fractures.
Results
Search results and baseline
characteristics
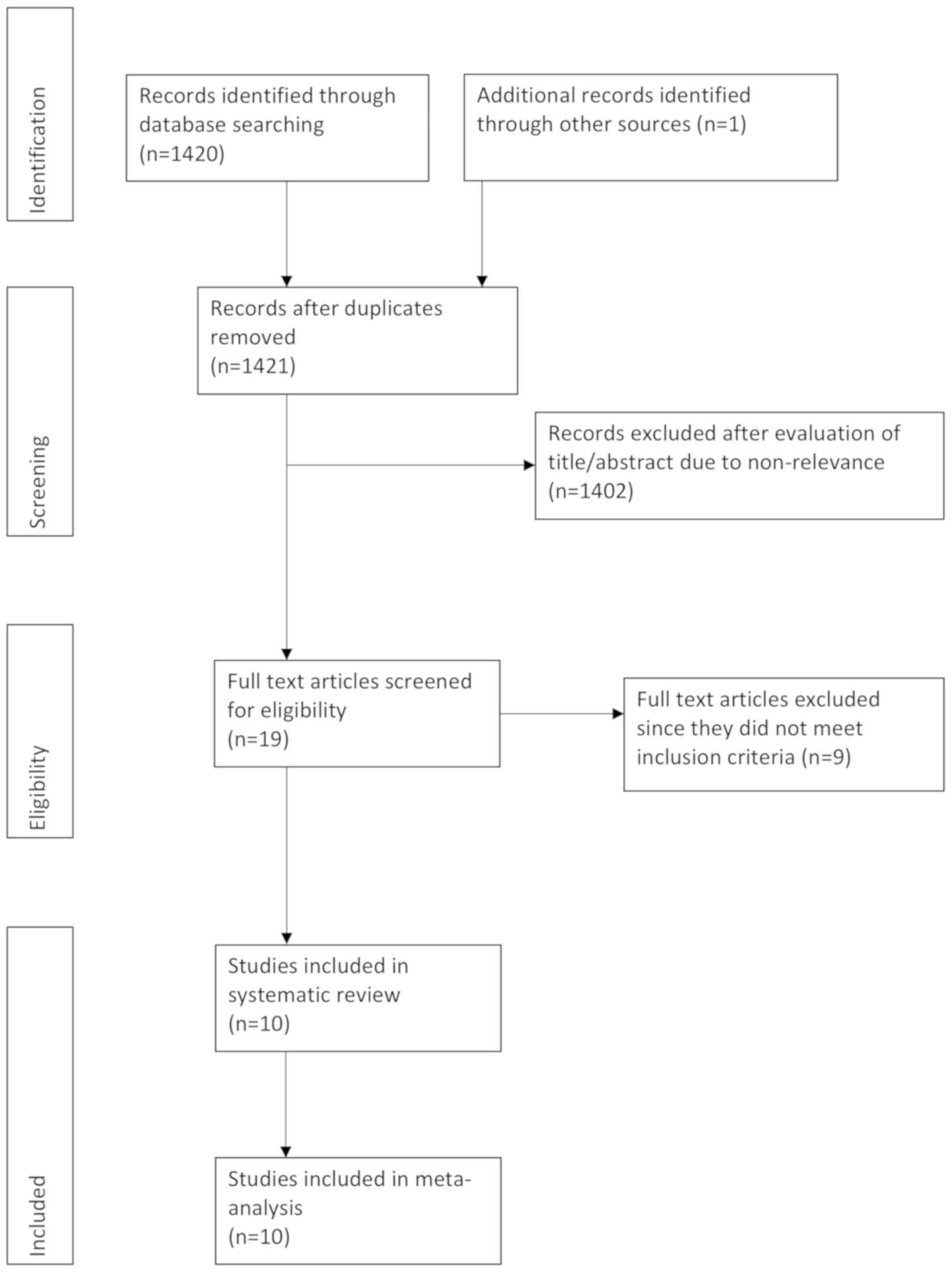
In the database search, 1,420 records were retrieved
and 1 study was identified through reference searching (Fig. 1). A total of 19 articles were
selected for full-text analysis. From these, 9 studies were
excluded, including 4 that were quasi-randomized studies utilizing
an alternate/odds-even method for randomization (20-23),
3 that were non-randomized studies (21,24,25), 1
that was a combined prospective and retrospective study (26) and 1 study (27) that was a long-term follow-up of a
previously published trial (duplicate data). A total of 10 RCTs
were finally included in the present systematic review and
meta-analysis (14,15,28-35).
The baseline characteristics of the included studies
are presented in Table I. The type
of clavicle fracture included was mentioned in six trials (14,29-32,35).
All trials were performed on displaced MSCF. Comminuted fractures
were included in all studies except for 3 trials (28,29,34). The
sample size varied from 15-63 patients per group. The type of plate
fixation used was different across studies: Titanium elastic nail
was the choice of intramedullary fixation in 7 studies (15,28-30,32,33,35),
while 2 utilized a Sonoma CRx Collarbone pin (Sonoma) (14,31) and
1 trial reported on the use of the Rookwood pin (34). Post-operative data were obtained
after a follow-up of 12 months in the majority of studies, while 1
study reported follow-up data at 6 months (32).
 | Table ICharacteristics of included
studies. |
Table I
Characteristics of included
studies.
| | Patients (n) | Age (years)
Mean±SD | Male sex (n) | |
|---|
| Author (year) | Plate | IMF | Plate | IMF | Plate | IMF | Fracture type | Displaced fractures
included | Comminuted
fractures included | Plate type | IMF type | Rehabilitation | Patients Follow-up
duration | lost to follow-up
(n) | (Refs.) |
|---|
| Ferran (2010) | 15 | 17 | 35.4±NS | 23.8±NS | 13 | 14 | NS | Yes | No | Recon plate,
LCDCP | Rookwood pin | Sling for 2 wks
followed by 6 wks of PROM | 12 months | NS | (34) |
| Assobhi (2011) | 19 | 19 | 32.6±5.9 | 30.3±4.8 | 17 | 16 | NS | Yes | No | 3.5-mm Recon
plate | TEN | Sling for 2 wks,
ADL at 4 wks, strenuous exercise at 6 wks | 12 months | NS | (28) |
| Narsaria
(2014) | 32 | 33 | 40.2±11.2 | 38.9 ±9.1 | 26 | 24 | Robinson | Yes | No | DCP | TEN | Sling for 2 wks,
early AROM | 24 months | NS | (29) |
| Andrade-Silva
(2015) | 29 | 25 | 31.2±12.2 | 28.3±9.4 | 28 | 19 | OTA B | Yes | Yes | Recon plate | TEN | Sling for 4 wks,
AROM for 2 wks | 12 months | Plate: 4 IMF:
1 | (35) |
| Meijden (2015) | 55 | 62 | 38.4±14.6 | 39.6±13.2 | 53 | 60 | OTA A,B,C | Yes | Yes | Surgeon's
preference | TEN | Sling for comfort
and early AROM | 12 months | Plate: 3 | (30) |
| Zehir (2015) | 21 | 24 | 32.38±8.41 | 33.17±8.6 | 12 | 14 | Robinson
2B1,B2 | Yes | Yes | LCP | CRx | Sling for 2 wks,
early AROM | Up to 38
months | Plate: 6 IMF:
5 | (31) |
| Calbiyik
(2016) | 40 | 35 | 39.07±7.04 | 42.02±13.87 | 25 | 21 | Robinson
2B1,B2 | Yes | Yes | LCP | CRx | Sling for 1 wk,
early AROM, weight bearing at 1 month | 12 months | None | (14) |
| Fuglesang
(2017) | 63 | 60 | 34.6±NS | 36.4±NS | 54 | 51 | NS | Yes | Yes | 3.5-mm superior
clavicular plate | TEN | Sling for 1-2 wks,
early pendulum movements but not to transmit load or abduct the arm
by >90° until 6 wks | 12 months | Plate: 1 IMF:
2 | (15) |
| Kumar (2018) | 23 | 19 | 30.17±NS | 24±NS | 19 | 13 | Robinson
2B1,B2 | Yes | Yes | Pre-contoured
LCP | TEN | Sling for 2 wks,
early pendulum movements and PROM from 2 wks | 6 months | NS | (32) |
| Sahu (2018) | 25 | 25 | 34.76±11.8 | 33.28±10.7 | 18 | 18 | NS | Yes | Yes | 3.5-mm Recon | TEN | Sling for 2 wks,
early plate, LCP pendulum movements and PROM at 4-6 wks with
limited abduction | 12 months | NS | (33) |
Primary outcome
A total of 5 studies evaluated shoulder function
outcomes using Constant-Murley scores as well as DASH scores
(14,15,30,33,35).
Shoulder function was assessed exclusively by Constant-Murley
scoring in 4 studies (28,29,32,34) and
only by DASH scoring in 1 study (31). Data were not presented as the mean
and SD by 2 studies (15,32) and attempts to contact the authors
were unsuccessful; hence, they were not included in the
meta-analysis (Table SI).
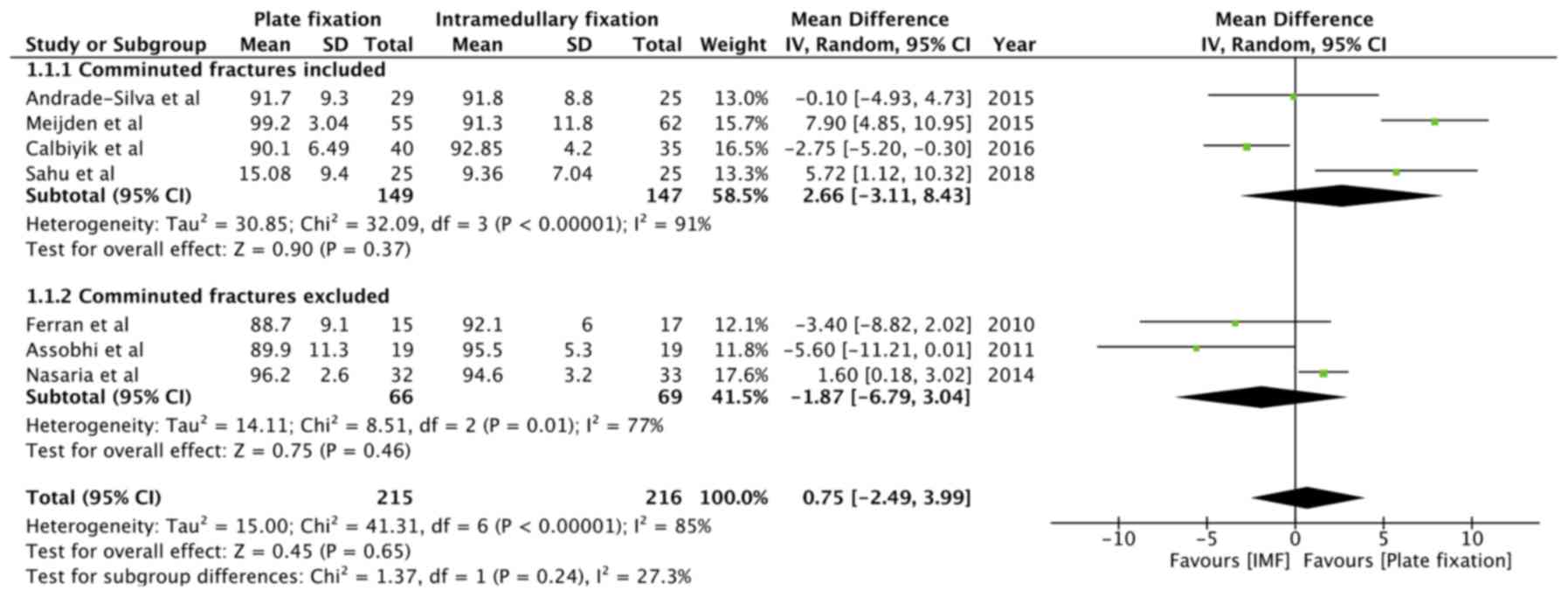
Sufficient data on Constant-Murley scores for
meta-analysis were available from 7 studies (14,28-30,33-35).
Analysis of the pooled data of 215 patients undergoing plate
fixation and 216 patients undergoing intramedullary fixation
revealed no statistically significant difference in Constant-Murley
scores between the two groups (MD=0.75, 95% CI: -2.49 to 3.99,
P=0.65; I2=85%; Fig. 2).
A sub-group analysis was performed for studies including comminuted
clavicle fracture (MD=2.66, 95% CI: -3.11 to 8.43, P=0.37;
I2=91%) and those excluding comminuted fractures
(MD=-1.87, 95% CI: -6.79 to 3.04, P=0.46; I2=77%). The
overall effect was not significant for both sub-groups (Fig. 2).
Data on the DASH scores were extracted from five
studies (14,30,31,33,35).
Comminuted fractures were included in all five trials. Pooled
scores from 170 patients in the plate fixation group and 171
patients in the intramedullary fixation group demonstrated no
statistically significant difference in DASH scores (MD=1.55, 95%
CI: -1.12 to 4.23, P=0.26; I2=89%; Fig. 3).
Secondary outcomes
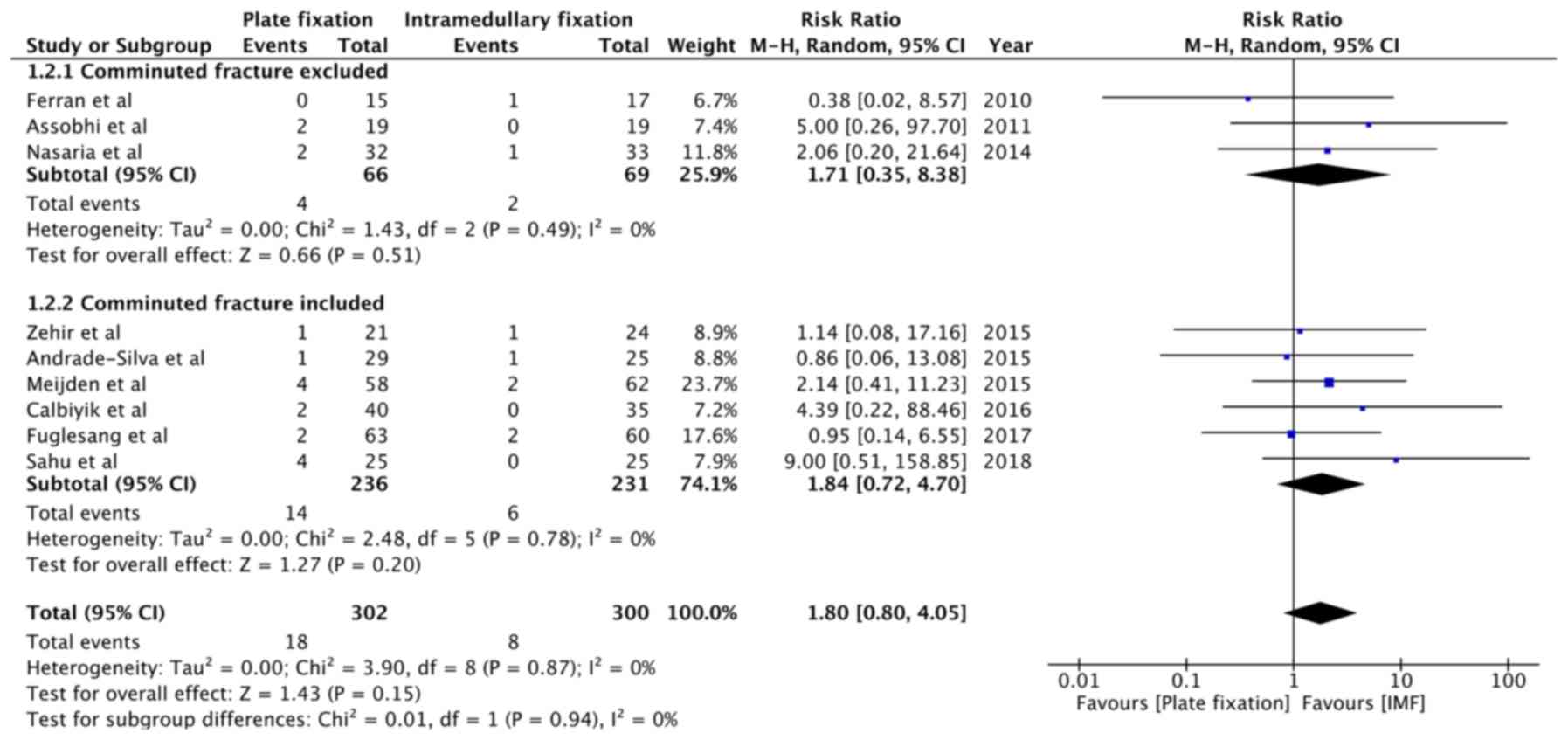
The first secondary outcome was the incidence of
treatment failure (i.e., complications requiring non-routine
surgery). Causes of treatment failure in the included studies are
presented in Table II. While the
present analysis indicated that clavicle fractures treated with
plate fixation had a 1.8-times greater risk of developing treatment
failure, the overall effect was not statistically significant
(RR=1.80, 95% CI: 0.80 to 4.05, P=0.15; I2=0%; Fig. 4). The overall risk in studies
excluding comminuted fractures (RR=1.71, 95% CI: 0.35 to 8.38,
P=0.51; I2=0%) and those including comminuted fractures
(RR=1.84, 95% CI: 0.72 to 4.70, P=0.20; I2=0%) was also
not statistically significant (Fig.
4).
| Table IITreatment failures in included
studies. |
Table II
Treatment failures in included
studies.
| | Plate fixation | Intramedullary
fixation | |
|---|
| Author (year) | Complication | Number | Complication | Number | (Refs.) |
|---|
| Ferran (2010) | Nil | | Loose hardware | 1 | (34) |
| Assobhi (2011) | Non-union | 1 | Nil | | (28) |
| | Refracture after
implant removal | 1 | | | |
| Narsaria
(2014) | Major revision
surgery | 2 | Implant
failure | 1 | (29) |
| Andrade-Silva
(2015) | Implant
failure | 1 | Non-union | 1 | (35) |
| Meijden (2015) | Refracture after
implant removal | 2 | Implant
failure | 2 | (30) |
| | Non-union | 1 | | | |
| | Implant
breakage | 1 | | | |
| Zehir (2015) | Implant
failure | 1 | Implant
failure | 1 | (31) |
| Calbiyik
(2016) | Implant
failure | 2 | Nil | | (14) |
| Fuglesang
(2017) | Deep infection | 2 | Implant
failure | 1 | (15) |
| | Refracture | 1 | Non-union | 1 | |
| Kumar (2018) | Nil | | Nil | | (32) |
| Sahu (2018) | Non-union | 1 | Nil | | (33) |
| | Re-fracture after
implant removal | 1 | | | |
| | Loose hardware | 2 | | | |
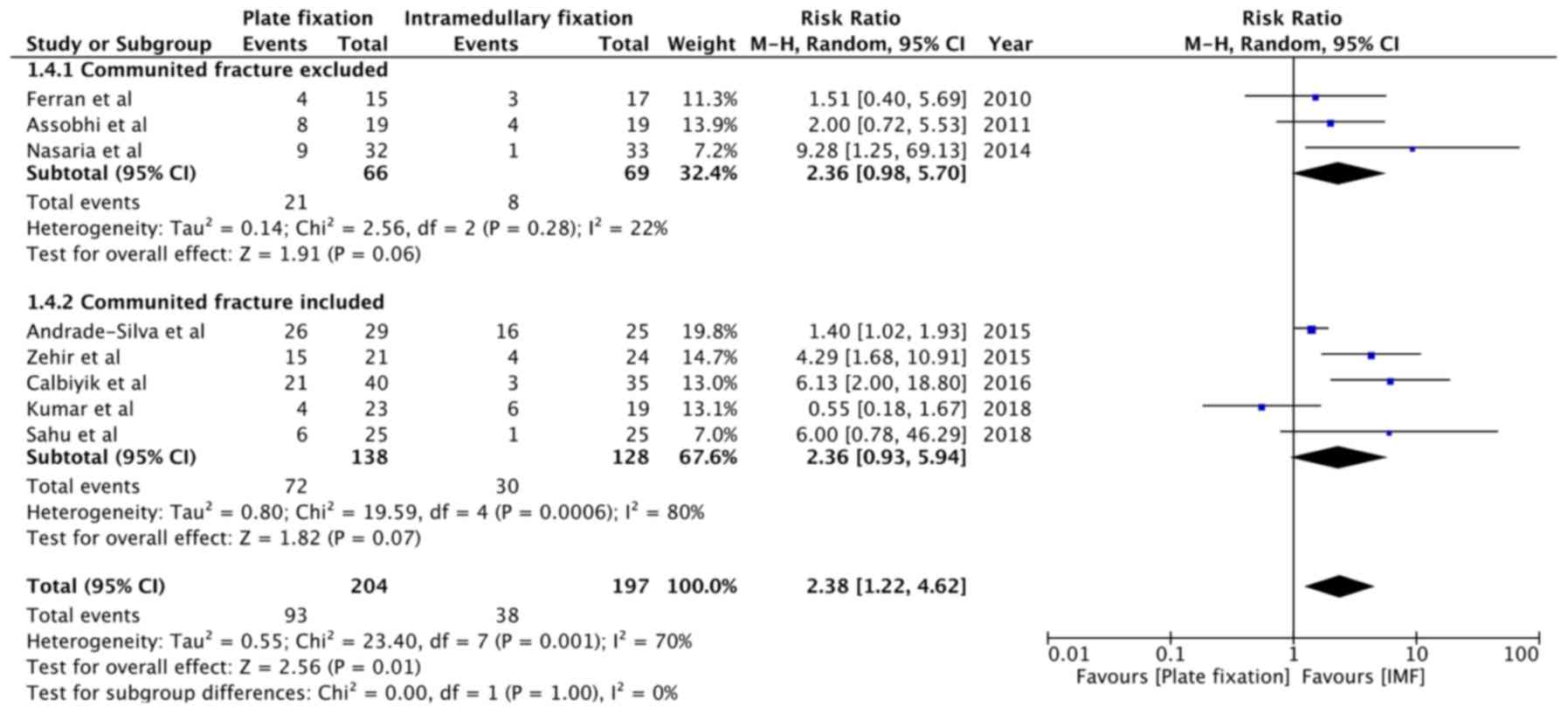
A summary of complications not requiring non-routine
surgery reported in the included studies is presented in Table III. Patient-level data were not
available from two studies (15,30);
hence, they were excluded from the quantitative analysis. The
results indicated that plate fixation was associated with a
2.38-fold increased risk of complications not requiring non-routine
surgery, as compared to intramedullary fixation (RR=2.38, 95% CI:
1.22 to 4.62, P=0.001; I2=70%; Fig. 5). Sub-group analysis indicated a
2.36-fold increased risk of complications with plate fixation in
both cohorts, i.e., studies excluding comminuted fractures
(RR=2.36, 95% CI: 0.98 to 5.70, P=0.06; I2=22%) and
studies including comminuted fractures (RR=2.36, 95% CI: 0.93 to
5.94, P=0.07; I2=80%). The results were close but did
not achieve statistical significance in the two sub-groups
(Fig. 5).
| Table IIIAdverse events not requiring
non-routine surgery. |
Table III
Adverse events not requiring
non-routine surgery.
| | Plate fixation | Intramedullary
fixation | |
|---|
| Author (year) | Complication | Number | Complication | Number | (Refs.) |
|---|
| Ferran (2010) | Infection | 3 | Scar numbness | 2 | (34) |
| | Scar numbness | 1 | Soft tissue
irritation | 1 | |
| Assobhi (2011) | Hypertrophic
scar | 4 | Prominent implant
under skin | 3 | (28) |
| | Prominent implant
under skin | 3 | | | |
| | Infection | 1 | Hypertrophic
callus | 1 | |
| Narsaria
(2014) | Hypertrophic
scar | 4 | Infection | 1 | (29) |
| | Wound
dehiscence | 3 | | | |
| | Infection | 2 | | | |
| Andrade-Silva
(2015) | Implant
bending | 11 | Implant
bending | 1 | (35) |
| | Paraesthesia | 8 | Implant related
pain | 10 | |
| | Implant-related
pain | 4 | Partial implant
migration | 5 | |
| | Partial implant
migration | 2 | | | |
| | Infection | 1 | | | |
| Meijden
(2015)a | Infection | 3 | Hematoma | 6 | (30) |
| | Hematoma | 5 | Transient
neuropraxia | 1 | |
| | Irritation due to
implant protrusion | 25 | Irritation due to
implant protrusion | 44 | |
| | Implant
breakage | 1 | Implant
failure | 2 | |
| | Nonunion | 1 | | | |
| | Refracture after
implant removal | 2 | | | |
| Zehir (2015) | Cosmetic
dissatisfaction | 9 | Cosmetic
dissatisfaction | 4 | (31) |
| | Skin
irritation | 3 | | | |
| | Dysesthesia | 2 | | | |
| | Infection | 1 | | | |
| Calbiyik
(2016) | Cosmetic
dissatisfaction | 14 | Cosmetic
dissatisfaction | 1 | (14) |
| | Skin
irritation | 2 | Implant
failure | 2 | |
| | Dysesthesia | 3 | | | |
| | Painful
shoulder | 2 | | | |
| Fuglesang
(2017)a | Superficial
infection | 5 | Wound
dehiscence | 4 | (15) |
| | Incisional
numbness | 31 | Incisional
numbness | 10 | |
| | Pain over
hardware | 26 | Pain over
hardware | 19 | |
| | Implant
failure | 5 | Implant
failure | 1 | |
| Kumar (2018) | Infection | 1 | Nail
impingement | 6 | (32) |
| | Plate
prominence | 3 | | | |
| Sahu (2018) | Infection | 2 | Infection | 1 | (33) |
| | Malunion | 1 | | | |
| | Hypertrophic
scar | 3 | | | |
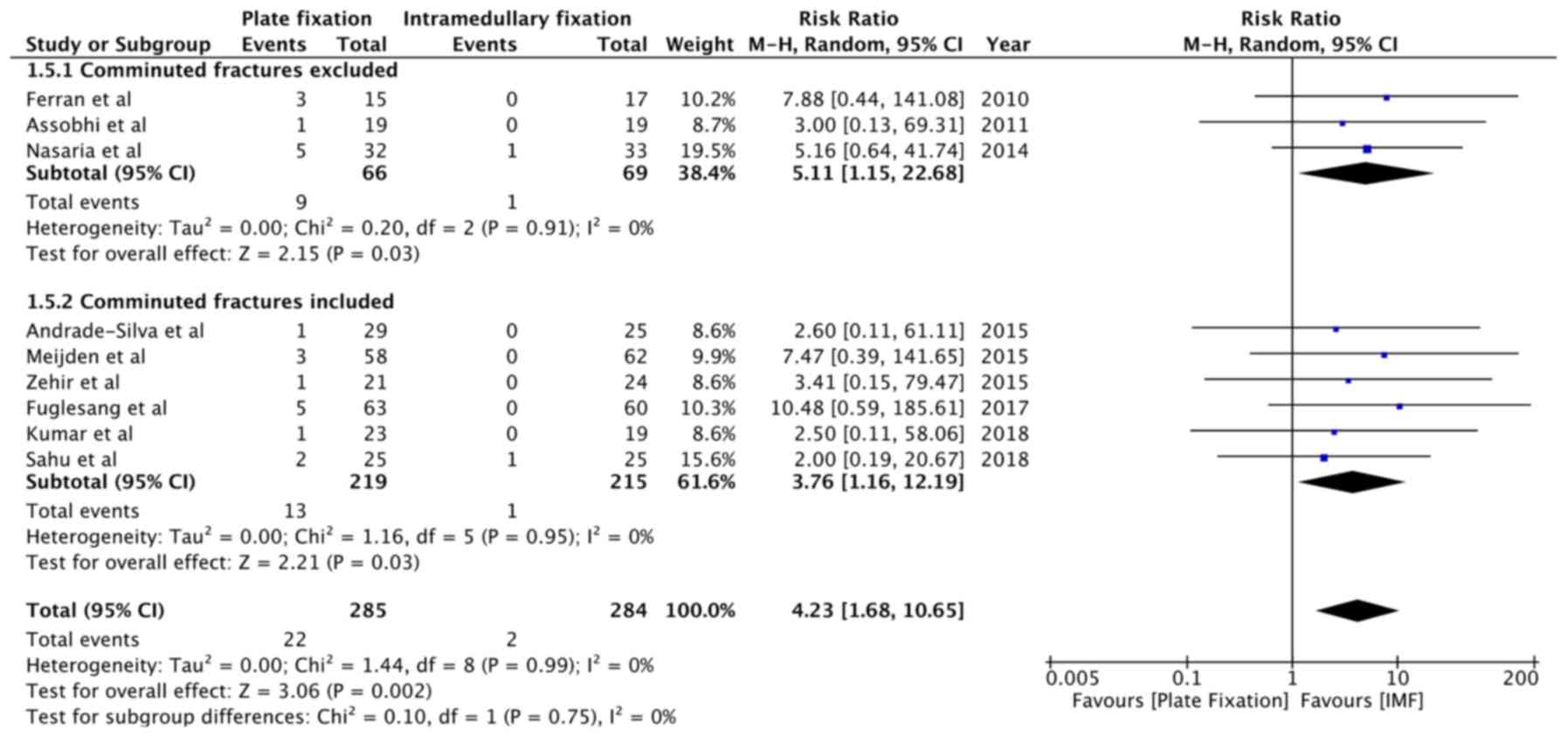
Meta-analysis was also performed for specific minor
complications. Infection rates were reported by 9 studies (15,28-35).
With a rate of 7.7% with plate fixation and 0.7% with
intramedullary fixation, pooled analysis indicated a statistically
significant 4.23-fold increased risk of infection with plate
fixation (RR=4.23, 95% CI: 1.68 to 10.65, P=0.002;
I2=0%; Fig. 6). The risk
was increased for studies excluding comminuted fractures (OR=5.11,
95% CI: 1.15 to 22.68, P=0.03; I2=0%) and those studies
including comminuted fractures (RR=3.76, 95% CI: 1.16 to 12.19,
P=0.03; I2=0%; Fig. 6).
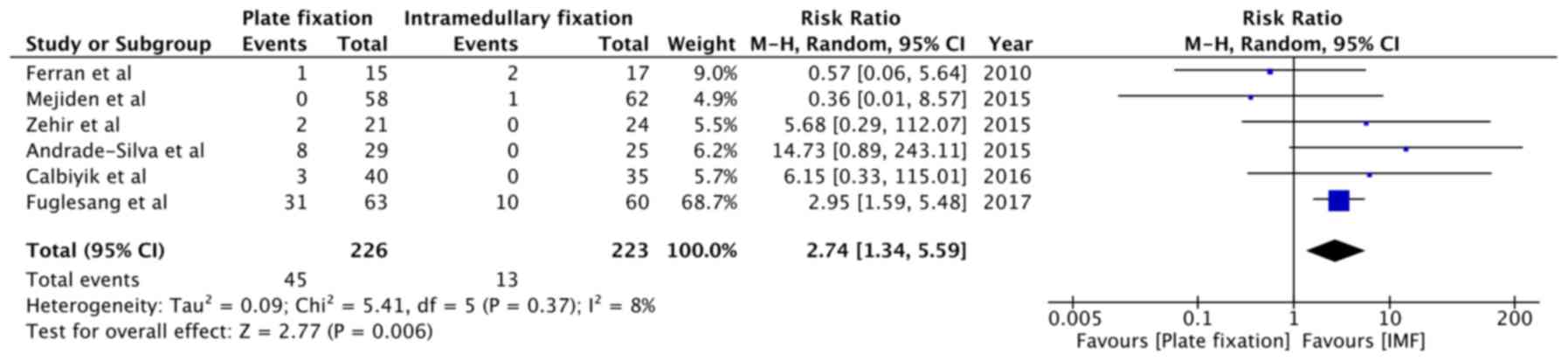
All complications related to nerve injury (including scar numbness,
dysesthesia and paraesthesia) were pooled for quantitative
analysis. Meta-analysis indicated a statistically significant
2.74-fold increased risk of nerve injury-related complications with
plate fixation (RR=2.74, 95% CI: 1.34 to 5.59, P=0.006;
I2=8%; Fig. 7).
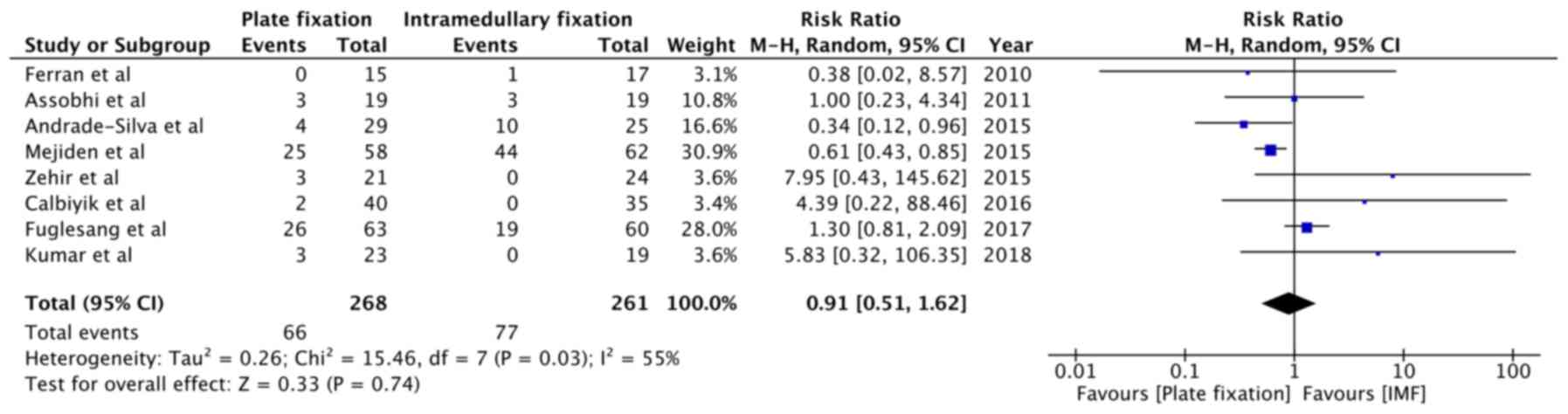
Implant-associated complications, including implant protrusion,
skin irritation and pain over hardware were reported by eight
studies (14,15,28,30-32,34,35).
Pooled analysis indicated no statistically significant difference
between plate fixation and intramedullary fixation (RR=0.91, 95%
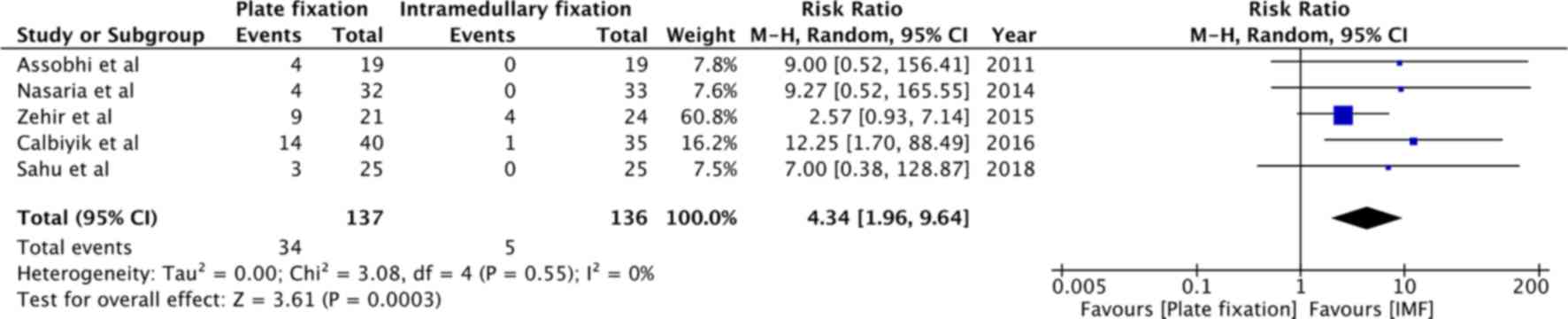
CI: 0.51 to 1.62, P=0.74; I2=55%; Fig. 8). Data on complications of cosmetic
dissatisfaction were reported by five studies (14,28,29,31,33).
Patients undergoing plate fixation were at a 4.34-fold increased
risk of complications of cosmetic dissatisfaction as compared to
patients undergoing intra-medullary fixation (RR=4.34, 95% CI: 1.96
to 9.64, P=0.0003; I2=0%; Fig. 9).
Sensitivity analysis
Sensitivity analysis was performed to evaluate
changes in the pooled effect size after removal of one study at a
time compared with the entire dataset. It was indicated that when
the results of Calbiyik et al (14) and Fuglesang et al (15) were removed sequentially, the overall
pooled estimate for nerve injury, while still demonstrating an
increased risk with intramedullary fixation, became statistically
insignificant [Calbiyik et al (14) excluded: RR=2.46, 95% CI: 0.95 to
6.39, P=0.06; I2=22% (Fig.
S1); and Fuglesang et al (15) excluded: RR=2.40, 95% CI: 0.55 to
10.43, P=0.06; I2=27%] (Fig.
S2). No changes were observed for any other variables.
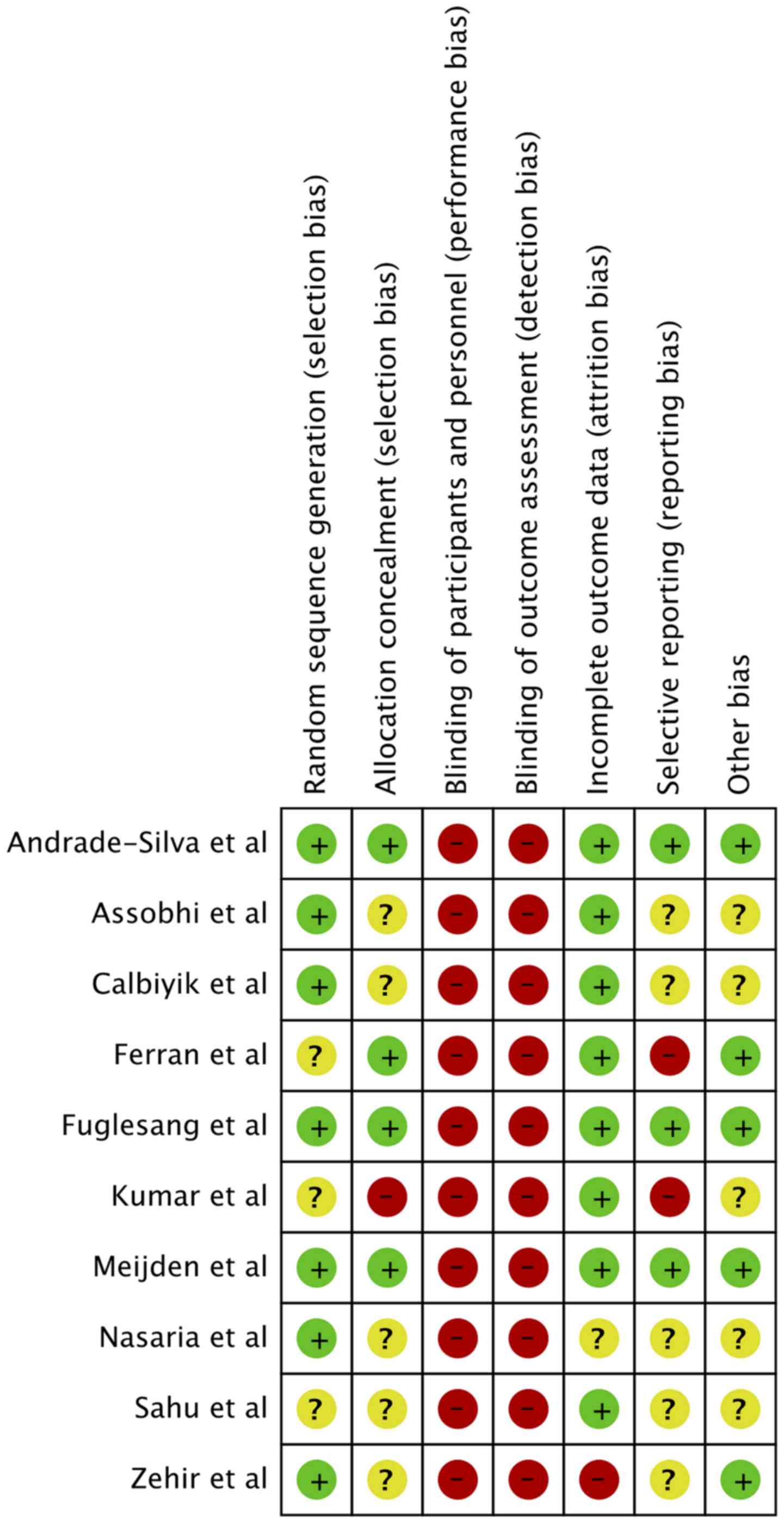
Risk of bias
The authors' judgement of risk of bias of included
studies is presented in Fig. 10. A
total of 3 studies did not clearly specify the method of
randomization (32-34).
Appropriate methods of allocation concealment were used in 4
studies (15,30,34,35). A
high risk of attrition bias was noted in one trial (31). Only three studies were pre-registered
with clinical trial registries (15,30,35).
Based on the scoring criteria, all studies were rated as being of
‘medium quality’, except one (32),
which was rated as being of ‘low quality’. Removal of the
‘low-quality’ study in the sensitivity analysis did not affect the
results for any variable.
Discussion
In line with the growing trend of operative
treatment for MSCF, studies have demonstrated superior results with
both plate and intramedullary fixation as compared to non-operative
management of MSCF (5,7). However, the choice between the two
fixation modalities has remained a matter of debate. To the best of
our knowledge, to date, a total of 9 meta-analyses have attempted
to compare clinical outcomes after plate vs. intramedullary
fixation of MSCF (9-13,18,36-38).
The majority of these reports were published in the years 2015
(10,12,13,37) and
2016 (9,11,18,36) with
the last literature search performed in January 2016(18). While 4 studies (9,13,37,38)
concluded that there is no difference in outcomes after plate or
intramedullary fixation of MSCF, the remaining 5 reviews (10-12,18,36)
inferred that intramedullary fixation is superior to plate fixation
for the management of MSCF. The disparity amongst these studies has
been attributed to the different clinical questions, study
inclusion/exclusion criteria, data extraction, quality evaluation
and statistical methods used for meta-analysis (6). Considering the conflicting results of
previous studies and the availability of new trials for inclusion,
the present study was performed to provide updated results to
clarify this disputed topic.
The results of the present study indicated no
difference in long-term functional outcomes after plate or
intramedullary fixation of MSCF. These present results are in
agreement with those of Hussain et al (18), which did not obtain any such
difference from a pooled analysis of 7 RCTs and 3 quasi-RCTs. The
study by Houwert et al (9),
in which 20 studies (RCTs and cross-sectional studies) were
analyzed, also indicated no significant difference in
Constant-Murley scores at short-term and long-term follow-ups after
MSCF. An earlier analysis demonstrating better shoulder functions
with intramedullary fixation may have been incorrect due to the
limited number of included studies (10).
It has been indicated that plate fixation is more
appropriate for the management of comminuted fractures. Telescoping
of the fracture site and limited exercise capacity due to
suboptimal stability are observed when markedly comminuted
fractures are fixed using intramedullary fixation (39). Since 3 RCTs (28,29,34) did
not include comminuted fractures, a sub-group analysis was
performed in the present study to provide more clarity on the
results. There was no statistically significant difference in
Constant-Murley scores in the two groups of studies including or
excluding comminuted fractures. The RCT by Fuglesang et al
(15) indicated that the DASH scores
were higher when comminuted fractures were treated with
intramedullary fixation. However, this difference was only observed
at up to six months of follow-up, with no significant difference in
DASH scores between plate and intramedullary fixation at 12 months.
It was postulated that, while plate fixation bridges the fracture
site to negate the effect of comminution, intramedullary fixation
achieves stability more gradually as the callus consolidates
(40). Since only long-term shoulder
function scores were pooled in the present study, it was not
possible to determine any such differences in early shoulder
function. Furthermore, as data on the actual number of comminuted
fractures treated were not presented in the included studies, it is
not possible to draw any definite conclusions regarding the effect
of fracture comminution on clinical outcomes following plate vs.
intramedullary fixation of MSCF.
Complications following operative treatment of MSCF
are influenced by a number of factors, including patient
characteristics (e.g., old age, history of diabetes, drug use,
alcohol intake), patient's occupational status (e.g., performance
of load-bearing activities), degree of fracture comminution,
surgical technique, type of fixation, surgeon's experience and
compliance with post-operative instructions (15,41,42).
While the influence of baseline patient characteristics is expected
to be nullified by appropriate randomization, the results may still
be biased considering the methodological heterogeneity and the
different types of fixation devices used amongst the included
trials. Another limitation is the inconsistent definition and
classification of complications across studies. To provide a more
comprehensible picture, complications were grouped into those
requiring non-routine surgery (treatment failure) and those not
requiring non-routine surgery (18).
The results of the present study indicated that plate and
intramedullary fixation had similar rates of treatment failure.
These results concur with a previous meta-analysis of RCTs on this
subject, which also reported a non-significant result (RR=2.19, 95%
CI: 0.93-5.15, P=0.07; I2=0%) (18). However, it is important to note that
the CI of the RR for treatment failure in the present analysis was
wide with an upper limit of 4 (denoting a 4-fold risk of
complications with plate fixation). The small number of events and
limited sample size of individual studies may have influenced the
overall results.
In terms of complications not requiring non-routine
surgery, the present results indicated that plate fixation is
associated with a 2.38-fold increased risk as compared to
intramedullary fixation. The difference may be attributed to the
requirement for greater exposure, increased surgical time and
soft-tissue stripping with plate fixation, which translates into a
higher risk of infection, nerve injury and hypertrophic scars
(7,43). The present meta-analysis on specific
complications supported this notion, as a 4.23-fold increased risk
of infection, 2.74-fold increased risk of nerve injury-associated
complications and 4.34 times increased risk of complications of
cosmetic dissatisfaction were determined for plate fixation.
Although the results of nerve injury-associated complications were
skewed in the sensitivity analysis, the CI was relatively wide and
the difference became only just insignificant after removal of two
particular studies (14,15).
While a large number of reviews were already
published on this subject, the present study has the strength of an
updated literature search, allowing for inclusion of 4 more RCTs
(14,15,32,33)
compared with a previous meta-analysis (18). Furthermore, to circumvent the
intrinsic bias associated with cross-sectional studies and avoid
the higher risk of methodological bias of quasi-randomized trials
from influencing the present results, these study types were
excluded from the present review. A sub-group analysis based on
inclusion of comminuted fractures was also performed for primary
and secondary outcomes. However, the present study has certain
limitations. Despite the inclusion criteria, the quality of the
included studies was not high. Bias with regard to randomization
and allocation concealment may have influenced the results.
Furthermore, the high degree of methodological heterogeneity, with
different types of plates and intramedullary fixation devices used,
may have skewed the outcomes. In addition, the influence of varied
operator experience and surgical techniques on outcomes cannot be
completely excluded. As another limitation, the sample size of the
majority of studies was small with only two studies (15,32)
including >50 patients per group. Finally, as previously
discussed, the number of patients with comminuted fractures in the
included studies is not known. The impact of this variable on
clinical outcomes should be elucidated by further studies.
Despite these limitations, the present study, a
meta-analysis of only RCTs, provides the most up-to-date evidence
on this controversial topic. Data of 322 patients randomized to
receive plate fixation and 319 patients randomized to receive
intramedullary fixation for MSCF were pooled in the present study.
The consistency of the direction and magnitude of the overall
effect and the stability of the results after sensitivity analysis
support the study's conclusions.
In conclusion, the results of the present study
provide strong evidence that there is no difference in long-term
functional outcomes between plate and intramedullary fixation of
MSCF. However, the effect of the fixation technique on short-term
functional outcomes remains to be clarified. In addition, while the
present review indicates that the two fixation techniques may have
similar treatment failure rates, the results do not permit any
strong assumptions due to the small number of events and wide CI in
the present analysis. However, there is evidence that plate
fixation is associated with an increased risk of complications not
requiring non-routine surgery. Specifically, infections and
complications of cosmetic dissatisfaction tend to be higher with
plate fixation.
The present study hereby presents the most current
level-1 evidence on clinical outcomes following plate vs.
intramedullary fixation of MSCF. In line with the conclusions,
clinicians may prefer intramedullary fixation for managing MSCF due
to its reduced rate of complications. However, individual patient
factors and the surgeon's experience shall continue to influence
the final choice of fixation for MSCF. Further homogenous
high-quality RCTs will further strengthen the evidence on this
subject.
Supplementary Material
Forest plot for nerve
injury-associated complications after the exclusion of Calbiyik
et al (14). IMF,
intramedullary fixation; M-H, Mantel-Haentzel; df, degrees of
freedom.
Forest plot for nerve
injury-associated complications after the exclusion of Fuglesang
et al (15). IMF,
intramedullary fixation; M-H, Mantel-Haentzel; df, degrees of
freedom.
Outcomes of shoulder function reported
by included studies.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
BQ conceived and designed the study. SM and WJ
collected the data and performed the literature search. WJ was
involved in the writing of the manuscript. All authors have read
and approved the final manuscript.
Ethical approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Robinson CM: Fractures of the clavicle in
the adult Epidemiology and classification. J Bone Joint Surg Br.
80:476–84. 1998.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Nordqvist A and Petersson C: The incidence
of fractures of the clavicle. Clin Orthop Relat Res. 300:127–132.
1994.PubMed/NCBI
|
|
3
|
Postacchini F, Gumina S, De Santis P and
Albo F: Epidemiology of clavicle fractures. J Shoulder Elb Surg.
11:452–456. 2002.PubMed/NCBI View Article : Google Scholar
|
|
4
|
CS NEER II: Nonunion of the clavicle. J Am
Med Assoc. 172:1006–1011. 1960.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Smekal V, Irenberger A, Struve P,
Wambacher M, Krappinger D and Kralinger FS: Elastic stable
intramedullary nailing versus nonoperative treatment of displaced
midshaft clavicular fractures-a randomized, controlled, clinical
trial. J Orthop Trauma. 23:106–112. 2009.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Xu B, Lin Y, Wang Z, Cao J, Yang Y, Xia H
and Zhang Y: Is intramedullary fixation of displaced midshaft
clavicle fracture superior to plate fixation? Evidence from a
systematic review of discordant meta-analyses. Int J Surg.
43:155–162. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Wijdicks F-JG, Van der Meijden OAJ,
Millett PJ, Verleisdonk EJMM and Houwert RM: Systematic review of
the complications of plate fixation of clavicle fractures. Arch
Orthop Trauma Surg. 132:617–625. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wijdicks FJ, Houwert RM, Millett PJ,
Verleisdonk EJ and Van der Meijden OA: Systematic review of
complications after intramedullary fixation for displaced midshaft
clavicle fractures. Can J Surg. 56:58–64. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Houwert RM, Smeeing DPJ, Ahmed Ali U,
Hietbrink F, Kruyt MC and van der Meijden OA: Plate fixation or
intramedullary fixation for midshaft clavicle fractures: A
systematic review and meta-analysis of randomized controlled trials
and observational studies. J Shoulder Elb Surg. 25:1195–1203.
2016.
|
|
10
|
Zhu Y, Tian Y, Dong T, Chen W, Zhang F and
Zhang Y: Management of the mid-shaft clavicle fractures using plate
fixation versus intramedullary fixation: An updated meta-analysis.
Int Orthop. 39:319–328. 2015.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Gao Y, Chen W, Liu YJ, Li X, Wang HL and
Chen ZY: Plating versus intramedullary fixation for mid-shaft
clavicle fractures: A systemic review and meta-analysis. PeerJ.
4(e1540)2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Zhang B, Zhu Y, Zhang F, Chen W, Tian Y
and Zhang Y: Meta-analysis of plate fixation versus intramedullary
fixation for the treatment of mid-shaft clavicle fractures. Scand J
Trauma Resusc Emerg Med. 23(27)2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Wang XH, Cheng L, Guo WJ, Li AB, Cheng GJ,
Lei T and Zhao YM: Plate versus intramedullary fixation care of
displaced midshaft clavicular fractures: A meta-analysis of
prospective randomized controlled trials. Medicine (Baltimore).
94(e1792)2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Calbiyik M, Ipek D and Taskoparan M:
Prospective randomized study comparing results of fixation for
clavicular shaft fractures with intramedullary nail or locking
compression plate. Int Orthop. 41:173–179. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Fuglesang HFS, Flugsrud GB, Randsborg PH,
Oord P, Benth J and Utvåg SE: Plate fixation versus intramedullary
nailing of completely displaced midshaft fractures of the clavicle.
Bone Joint J. 99:1095–1101. 2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Constant CR and Murley AH: A clinical
method of functional assessment of the shoulder. Clin Orthop Relat
Res. 160–164. 1987.PubMed/NCBI
|
|
17
|
Hudak PL, Amadio PC and Bombardier C:
Development of an upper extremity outcome measure: The DASH
(disabilities of the arm, shoulder and hand) [corrected]. The upper
extremity collaborative group (UECG). Am J Ind Med. 29:602–608.
1996.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hussain N, Sermer C, Prusick PJ, Banfield
L, Atrey A and Bhandari M: Intramedullary nailing versus plate
fixation for the treatment displaced midshaft clavicular fractures:
A systematic review and meta-analysis. Sci Rep.
6(34912)2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Higgins J, Altman D and Sterne J: Cochrane
statistical methods group and the cochrane bias methods group.
Chapter 8: Assessing risk of bias in included studies. In: Cochrane
handbook for systemic reviews of interventions, version 5. The
Cochrane Collaboration, 2011.
|
|
20
|
Lee YS, Lin CC, Huang CR, Chen CN and Liao
WY: Operative treatment of midclavicular fractures in 62 elderly
patients: Knowles pin versus plate. Orthopedics. 30:959–964.
2007.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Tabatabaei S and Shalamzari S: Treatment
of displaced midshaft clavicular fractures: A comparison between
smooth pin and LCDCP and reconstruction plate fixation. Pakistan J
Med Sci. 27:1129–1134. 2011.
|
|
22
|
Saha P, Datta P, Ayan S, Garg A,
Bandyopadhyay U and Kundu S: Plate versus titanium elastic nail in
treatment of displaced midshaft clavicle fractures A comparative
study. Indian J Orthop. 48:587–593. 2014.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Krishnan A, Barot MP, Dave BR, Bang P,
Devanand D, Patel D and Jain A: Percutaneous transforaminal
endoscopic decompression and cageless percutaneous bone graft
transforaminal lumbar interbody fusion: A feasibility study. J
Orthop Allied Sci. 6:21–27. 2018.
|
|
24
|
Kumar R, Kumar S, Singh D and Goel SC:
Role of bone marrow derived autologous mesenchymal stem cells in
fracture healing in rabbits. JBJD. 32:7–13. 2017.
|
|
25
|
Balachandar S, Mohankumar K and Kathir AS:
Outcome of plate and intramedullary fixation of midshaft clavicle
fractures: A search for optimal surgical management. Int J Orthop
Sci. 3:1050–1061. 2017.
|
|
26
|
Kingsly P, Sathish M and Ismail NDM:
Comparative analysis of functional outcome of anatomical
precontoured locking plate versus reconstruction plate in the
management of displaced midshaft clavicular fractures. J Orthop
Surg (Hong Kong). 27(2309499018820351)2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Hulsmans MHJ, van Heijl M, Houwert RM,
Hammacher ER, Meylaerts SA, Verhofstad MH, Dijkgraaf MG and
Verleisdonk EJ: High irritation and removal rates after plate or
nail fixation in patients with displaced midshaft clavicle
fractures. Clin Orthop Relat Res. 475:532–539. 2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Assobhi JEH: Reconstruction plate versus
minimal invasive retrograde titanium elastic nail fixation for
displaced midclavicular fractures. J Orthop Traumatol. 12:185–192.
2011.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Narsaria N, Singh AK, Arun GR and Seth
RRS: Surgical fixation of displaced midshaft clavicle fractures:
Elastic intramedullary nailing versus precontoured plating. J
Orthop Traumatol. 15:165–171. 2014.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Van Der Meijden OA, Marijn Houwert R,
Hulsmans M, Wijdicks FJ, Dijkgraaf MG, Meylaerts SA, Hammacher ER,
Verhofstad MH and Verleisdonk EJ: Operative treatment of dislocated
midshaft clavicular fractures: Plate or intramedullary nail
fixation?: A randomized controlled trial. J Bone Joint Surg Am.
97:613–619. 2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Zehir S, Zehir R, Şahin E and Çalbıyık M:
Comparison of novel intramedullary nailing with mini-invasive
plating in surgical fixation of displaced midshaft clavicle
fractures. Arch Orthop Trauma Surg. 135:339–344. 2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Kumar DM, Mishra DA, Kumar DD, Singh DA,
Pandey DD and Sinha DAK: A comparative study of displaced midshaft
clavicle fracture managed by precontoured locking compression
plates and titanium elastic nails. Int J Orthop Sci. 4:116–121.
2018.
|
|
33
|
Sahu AK, Lenka BS, Mishra AK, Panda CK and
Kar M: A comparative study between plating versus titanium elastic
nail system in mid-shaft clavicle fracture management. Int J Res
Orthop. 4(741)2018.
|
|
34
|
Ferran NA, Hodgson P, Vannet N, Williams R
and Evans RO: Locked intramedullary fixation vs plating for
displaced and shortened mid-shaft clavicle fractures: A randomized
clinical trial. J Shoulder Elb Surg. 19:783–789. 2010.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Andrade-Silva F, Kojima KD, Joeris A,
Silva JS and Rames Mattar Jr: Single, superiorly placed
reconstruction plate compared with flexible intramedullary nailing
for midshaft clavicular fractures: A prospective, randomized
controlled trial. J Bone Joint Surg Am. 97:620–626. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Xiao H, Gao H, Zheng T, Zhao J and Tian Y:
Plate fixation versus intramedullary fixation for midshaft clavicle
fractures: Meta-analysis of complications and functional outcomes.
J Int Med Res. 44:201–215. 2016.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Lenza M and Faloppa F: Surgical
interventions for treating acute fractures or non-union of the
middle third of the clavicle. Cochrane Database Syst Rev.
7(CD007428)2015.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Duan X, Zhong G, Cen S, Huang F and Xiang
Z: Plating versus intramedullary pin or conservative treatment for
midshaft fracture of clavicle: A meta-analysis of randomized
controlled trials. J Shoulder Elbow Surg. 20:1008–1015.
2011.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Smekal V, Irenberger A, Attal R El,
Oberladstaetter J, Krappinger D and Kralinger F: Elastic stable
intramedullary nailing is best for mid-shaft clavicular fractures
without comminution: Results in 60 patients. Injury. 42:324–329.
2011.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Zeng L, Wei H, Liu Y, Zhang W, Pan Y,
Zhang W, Zhang C, Zeng B and Chen Y: Titanium elastic nail (TEN)
versus reconstruction plate repair of midshaft clavicular
fractures: A finite element study. PLoS One. 10(e0126131)2015.
|
|
41
|
Schemitsch LA, Schemitsch EH, Kuzyk P and
McKee MD: Prognostic factors for reoperation after plate fixation
of the midshaft clavicle. J Orthop Trauma. 29:533–537. 2015.
|
|
42
|
Leroux T, Wasserstein D, Henry P, Khoshbin
A, Dwyer T, Ogilvie-Harris D, Mahomed N and Veillette C: Rate of
and risk factors for reoperations after open reduction and internal
fixation of midshaft clavicle fractures. J Bone Joint Surg Am.
96:1119–1125. 2014.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Canadian Orthopaedic Trauma Society.
Nonoperative treatment compared with plate fixation of displaced
midshaft clavicular fractures. J Bone Joint Surg. 89:1–10.
2007.PubMed/NCBI View Article : Google Scholar
|