Introduction
Increasing evidence has indicated that ozone therapy
is effective for treating numerous types of diseases featuring
chronic pain, including osteoarthritis (1-4),
neck and shoulder pain (5), lower
back pain (6-9),
myofascial pain syndrome (10),
fibromyalgia (11), complex regional
pain syndrome (12),
zoster-associated pain (13,14) and other diseases, such as intractable
headache and cardiovascular diseases (15,16).
Medical ozone is administered in a flexible manner and may be
applied externally or orally. It may also be administered locally
or intravenously. Ozonated autohemotherapy (OAH) is widely used in
the treatment of chronic pain (14,16,17). It
has been reported that OAH alleviated pain of patients with
post-herpetic neuralgia (14),
intractable headache (16), as well
as hyperuricemia and gout (17).
Moderate concentrations of ozone (10 or 50 µg/ml) have been
reported to increase deformability of red blood cells (18) and OAH is able to ameliorate renal
ischemia-reperfusion injury in patients with kidney injury
(19).
The specific mechanisms of action of ozone treatment
in various diseases remain to be further studied. It is thought
that the effects of ozone treatment are based on its strong
oxidative and anti-pathogenic effects and immune regulation
ability, as well as the increase of oxygen supply and reduction of
oxidative stress (12,20-27).
For instance, ozone was proven to relieve pain by causing the
following effects: i) Release of endorphins (26); ii) inhibition of the activation of
microglia via adenosine monophosphate (AMP)-dependent protein
kinase signaling (28); iii)
inhibition of the expression of purinergic receptors P2X3 and P2X7
in the spinal dorsal horn (29); iv)
promoting phosphodiesterase 2A-cyclic guanosine
monophosphate/cyclic AMP/NFκB-p65 signaling (30); v) inhibition of autophagy (31,32); vi)
reduction of the expression of pro-inflammatory/pro-apoptotic
caspases (33); and vii) increase of
oxygen supply in tissues and cells (22).
OAH comprises the drawing of blood and blood
transfusion through a steel needle, which causes vascular damage.
To prevent infection, the blood transfusion operation requires
strict aseptic conditions in the operating room. Furthermore, OAH
is time-consuming and cumbersome. Therefore, clinicians are
exploring novel techniques for systemic ozone delivery. It has been
proposed that ozonated saline infusion may be able to replace OAH.
Compared to OAH, ozonized saline infusion is easy to perform and
does not require the drawing of blood or blood transfusions.
Furthermore, the requirements for the operating room are easy to
fulfill and the cost is relatively low, making ozonated saline
infusion a possible alternative to OAH therapy. Compared to the
OAH, the ozonated saline is more convenient and more operable,
however there is controversial about clinical application of
ozonated saline. A comparison of the two types of infusion is
presented in Table I.
 | Table IComparisons of OAH and ozonated
saline infusion. |
Table I
Comparisons of OAH and ozonated
saline infusion.
| Treatment | Blood drawing and
transfusion | OD of puncture
needle | Infusion
environment | Operational
difficulty | Patient
acceptance | Treatment
duration | Cost | Dispute in the
medical fielda |
|---|
| OAH | Yesb | 20 G | Clean area for
operation | High | Difficult | Relatively
long | Relatively
high | No |
| Ozonated saline
infusion | No | 24 G | Low
requirement | Low | Easy | Relatively
short | Relatively low | Yes |
Intravenous infusion of ozonated saline has been
used in the clinic to treat a variety of diseases. A clinical study
suggested that intravenous infusion of ozonated saline contributes
to the elimination of macrophages from wounds, mainly through
regulating genetically programed cell death (apoptosis), which has
a significant role in the inflammatory process (34). Intravenous infusion of ozonated
saline may improve symptoms of ischemia and hypoxia in the lower
limbs of patients with occlusive atherosclerosis by stabilizing
lysosomal hydrolase activity (35).
Intravenous infusion of ozonized saline may also reduce the
viscosity of blood and the aggregation of red blood cells, as well
as enhance the deformability of red blood cells (36).
Animal studies have indicated that intravenous
injection of 5 ml/kg ozonized saline bubbled with 4 µg/ml ozone in
dogs increased the number of polymorphonuclear neutrophilic
leukocytes, as well as their ability to capture bacteria for 2
days. In addition, this treatment led to an increase in the
adaptability and compensatory capacity of the body (37). Intravenous infusion of ozonated
saline may relieve liver injury induced by CCl4 via its
effects on reactive oxygen species (ROS) and the Kelch-like
ECH-associated protein 1/nuclear factor, erythroid 2-like 2/ARE
signaling pathway in rats (38).
With the development of ozonated saline infusion, it
has been suggested that ozonated saline may contain toxic
substances, including hypochlorite, chlorite, chlorate or even
perchlorate (39). However, it was
reported that ozone interacts neither with Na+ nor with
Cl- and no sodium hypochlorite or other
chlorine-containing oxygen ions were detected (40). The possible reaction mechanisms
include the following: i) Chloride ions in normal saline are first
oxidized by ozone to form chlorine atoms, initiating a chain
reaction. The chlorine atoms are then oxidized by ozone to form
harmful substances including chlorite, chlorate and perchlorate;
ii) chloride ions are directly oxidized by ozone to form
hypochlorite and oxygen, and hypochlorite is then oxidized by ozone
to form chlorite, chlorate and perchlorate (39). These suggestions bring the clinical
safety of ozonated saline infusion therapy into question (41).
In the present study, the safety of ozonated saline
that may be used for intravenous infusion therapy was investigated.
Ion chromatography-mass spectrometry (IC-MS) was used to determine
the presence and content of chlorite, chlorate and perchlorate in
ozonated saline at various time-points following preparation.
Materials and methods
Materials
The following products were used in the present
study: Medical ozone generator (Medozon compact, Herrmann
Apparatebau GmbH); Dionex ICS5000+ ion chromatograph
with EGC eluent autogenerator (Thermo Fisher Scientific, Inc.); AB
4000 QTRAP triple-quadrupole mass spectrometry system with
electrospray ion source and Analyst 1.6.2 workstation (AB Sciex API
4000 Qtrap; AB Sciex LLC); Dionex Ion Pac AS16 anion analysis
column (Thermo Fisher Scientific, Inc.); C18 solid-phase extraction
(SPE) column (Agela Technologies); ozone-resistant blood bag
(S-200; Sichuan Nigale Biomedical Co., Ltd.); bottled saline
(Sichuan Kelun Pharmaceutical Co., Ltd.); and ozone-resistant
syringe (Shenli).
Preparation of ozonated saline
Ozone was produced with a medical ozone generator
and various groups were set up. Ozone concentrations were set as 0
(100% oxygen), 20, 40 and 60 µg/ml in oxygen. Ozone and saline were
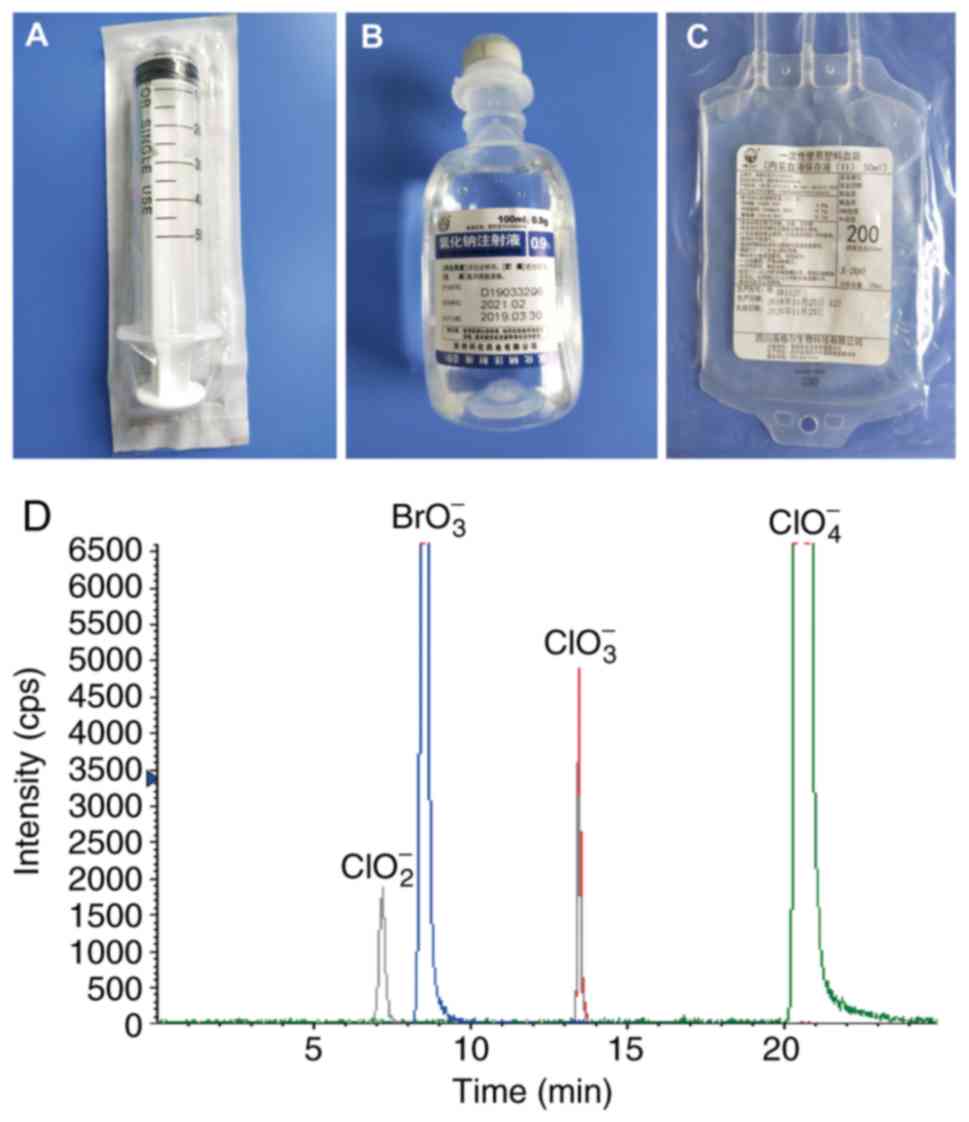
mixed at a volume ratio of 1:1. Using a 50-ml anti-oxidation
syringe (Fig. 1A), 100 ml ozone of
varying concentrations in oxygen, and 100 ml saline were drawn and
mixed in saline bottles (Fig. 1B) or
ozone-resistant blood transfusion bags (Fig. 1C). Ozonated saline was prepared and
stored in room temperature without protection from light. On the
3rd, 6 and 15th day after the preparation, chlorite, chlorate and
perchlorate in the ozonated saline were detected. The saline
bottles and the blood bags had all been produced with the same
batch numbers (E218092707 and 180808, respectively).
Confirmation of chromatographic
conditions
A Dionex ICS5000+ ion chromatograph
system (Thermo Fisher Scientific, Inc.) was used. The mobile phase
was KOH, the flow rate was set to 0.25 ml/min and the separation
was performed on a Dionex Ion Pac AS16 analysis column (250x2 mm;
Thermo Fisher Scientific, Inc.), and attached a Dionex Ion Pac AS16
anion guard column (50x2 mm; Thermo Fisher Scientific, Inc.). The
column temperature was maintained at 25˚C during the operation. The
injection volume was 25 µl. A 2-mm ASRS 500 anion suppressor
(Thermo Fisher Scientific, Inc.) was used with an external water
mode.
Confirmation of mass spectrometry
conditions
An AB 4000 Qtrap triple-quadrupole mass spectrometer
was used for mass spectrometry. The ion source was set as
electrospray negative ion mode. The source temperature was 500˚C.
Further parameters were as follows: Ion spray voltage, -4,500 V;
sprayer 1 (GS1), 206.84 kPa; GS2, 344.74 kPa. The transitions were
used in multiple-reaction monitoring (MRM) mode. The collision gas
was set to the medium mode. The surface heating system was set to
open and the scan time was 200 msec.
Selection of column and elution
gradient
The Dionex Ion Pac AS16 anion analysis column (250x2
mm) and the corresponding guard column may rapidly and accurately
detect trace amounts of perchlorate and other highly excited anions
in multiple aqueous samples (42),
and were therefore selected for the present study. In this
experiment, 3, 25 and 45 mmol/l mobile phase (KOH) were used to
analyze the separation effect of chlorite, chlorate and
perchlorate.
Optimization of mass spectrometry
A total of 5 ml of 1 mg/l chlorite, chlorate and
perchlorate standard solution were prepared and a needle pump was
used to continuously inject at a flow rate of 10 µg/min. First, a
primary precursor ion scan (Q1MS mode) was performed. Under the
selected mass spectrometry conditions, chlorite, chlorate and
perchlorate demonstrated a good response. After the precursor ion
was determined, the solution was subjected to a two-stage scan
(Q1MI mode). The product ions with the highest response value were
selected separately. The declustering potential (DP) value was
optimized, and a three-stage mass spectrometry fragment scan (MS2
mode) was then performed, and the collision energy (CE) value was
optimized. Finally, the solution was analyzed in MRM mode. Detected
ion pairs and optimized DP and CE voltage values for chlorite,
chlorate and perchlorate are presented in Table II.
| Table IIMass spectrometry conditions. |
Table II
Mass spectrometry conditions.
| Analyte | Detected ion pairs
(m/z) | DP (V) | CE (V) |
|---|
| Chlorite | 66.9/50.8 | -80 | -20 |
| Chlorate | 82.9/66.9 | -50 | -30 |
| Perchlorate | 98.9/82.9 | -60 | -30 |
Confirmation of linear association,
detection limit and quantitation limit
A total of five standard solutions (developed by the
Ministry of Agriculture Environmental Protection Research
Institute, Tianjin, China) with various concentrations (1, 2, 5, 10
and 20 µg/l) were accurately prepared and measured under optimized
IC-MS conditions, as described above. Linear regression
calculations were performed using the peak area (y-axis) of the
analytes and the corresponding mass concentration (x-axis, µg/l) to
obtain a linear regression equation and a linear correlation
coefficient (R). This was used to determine the detection limit of
an ion chromatographic peak at a signal-to-noise ratio (S/N)=3 and
quantitation limit of peak at S/N=10. The results indicated that
chlorite, chlorate and perchlorate had a good linear correlation in
the corresponding mass concentration range and the linear
correlation coefficient was >0.999. The detection limits of
chlorite, chlorate and perchlorate were 0.2, 0.5, and 0.01 µg/l,
respectively. The quantitation limits of chlorite, chlorate and
perchlorate were 0.7, 1.5 and 0.05 µg/l, respectively.
Evaluation of precision and recovery
rate
Samples were accurately weighed using 1, 2, 5, 10
and 20 µg/l of single standard solution and spiked recovery and
precision tests were performed. The average recovery of each
analyte was between 83.5 and 106.2%, and the relative standard
deviation (n=6) was between 3.7 and 5.8%.
Sample detection
The chloride ions in the sample solution were
removed using a C18 SPE column at a flow rate of 3 ml/min and the
concentrations of chlorite, chlorate and perchlorate in the sample
were then measured using the method described above.
Statistical analysis
Statistical analysis was performed using Prism
(v.7.0; GraphPad Software, Inc.) or SPSS 19.0 (IBM Corp.). Values
are expressed as the mean ± standard deviation. Statistical
analysis between the groups of varying concentrations or containers
was performed using repeated-measures two-way analysis of variance
(ANOVA) tests followed by Sidak's multiple-comparisons tests.
Statistical analysis of differences within the same concentration
group at different time-points were performed using
repeated-measures two-way ANOVA followed by Tukey's
multiple-comparisons tests. P<0.05 was considered to indicate a
statistically significant difference.
Results
Chlorite, chlorate and perchlorate
presented a good separation effect
Dionex Ion Pac AS16 anion analysis columns (250x2
mm) demonstrated a good separation effect on the chlorite, chlorate
and perchlorate. An improved separation of chlorite, chlorate and
perchlorate was achieved at the low mobile-phase concentration of 3
mmol/l KOH under the experimental conditions. The retention time of
7.2 min corresponded to chlorite, 13.5 min corresponded to chlorate
and 20.8 min corresponded to perchlorate (Fig. 1D).
Chlorite was not detected in the
ozone-saline or oxygen-saline solution
A total of five standard solutions (developed by the
Ministry of Agriculture Environmental Protection Research
Institute, Tianjin, China) with different concentrations (1, 2, 5,
10 and 20 µg/l) were added from low to high concentration for the
spiked recovery test. Recovery rates on the 3rd day were
96.0-105.4%, those on the 6th day were 88.5-103.5% and those on the
15th day were 84.0-102.6%. The mass spectrometry results indicated
that chlorite was not detected on the 3rd, 6 and 15th day in either
the ozone-saline or oxygen-saline solutions.
Chlorate was detected in the
ozone-saline subgroups at the three time-points
The five standard solutions with different
concentrations (1, 2, 5, 10 and 20 µg/l) were added from low to
high concentration for the spiked recovery test. The recovery rates
on the 3rd day were 88.5-106.0% and those on the 6th day were 83.5
and 106.2%. The recovery rates on the 15th day were
88.0-102.2%.
From the 3rd day to the 15th day after the ozonated
saline was prepared, chlorate was detected in the blood bag
subgroup (Fig. 2A and B) and the saline bottle subgroup (Fig. 2C and D). As time increased, the chlorate content
in the two subgroups increased. There was no significant difference
in the chlorate content between the 3rd and the 6th day in the
blood bag and the saline bottle subgroups. However, on the 15th
day, the chlorate content in the ozone-saline blood bag subgroup
was significantly increased at all ozone concentrations compared
with the corresponding levels on the 3rd and 6th days (Fig. 2B). In the saline bottle subgroup, the
chlorate content on the 15th day was only significantly increased
compared with that on the 3rd and 6th day in the same group (20
µg/ml ozone). No significance was observed for the 0, 40 and 60
µg/ml ozone groups across the time-points examined (Fig. 2D).
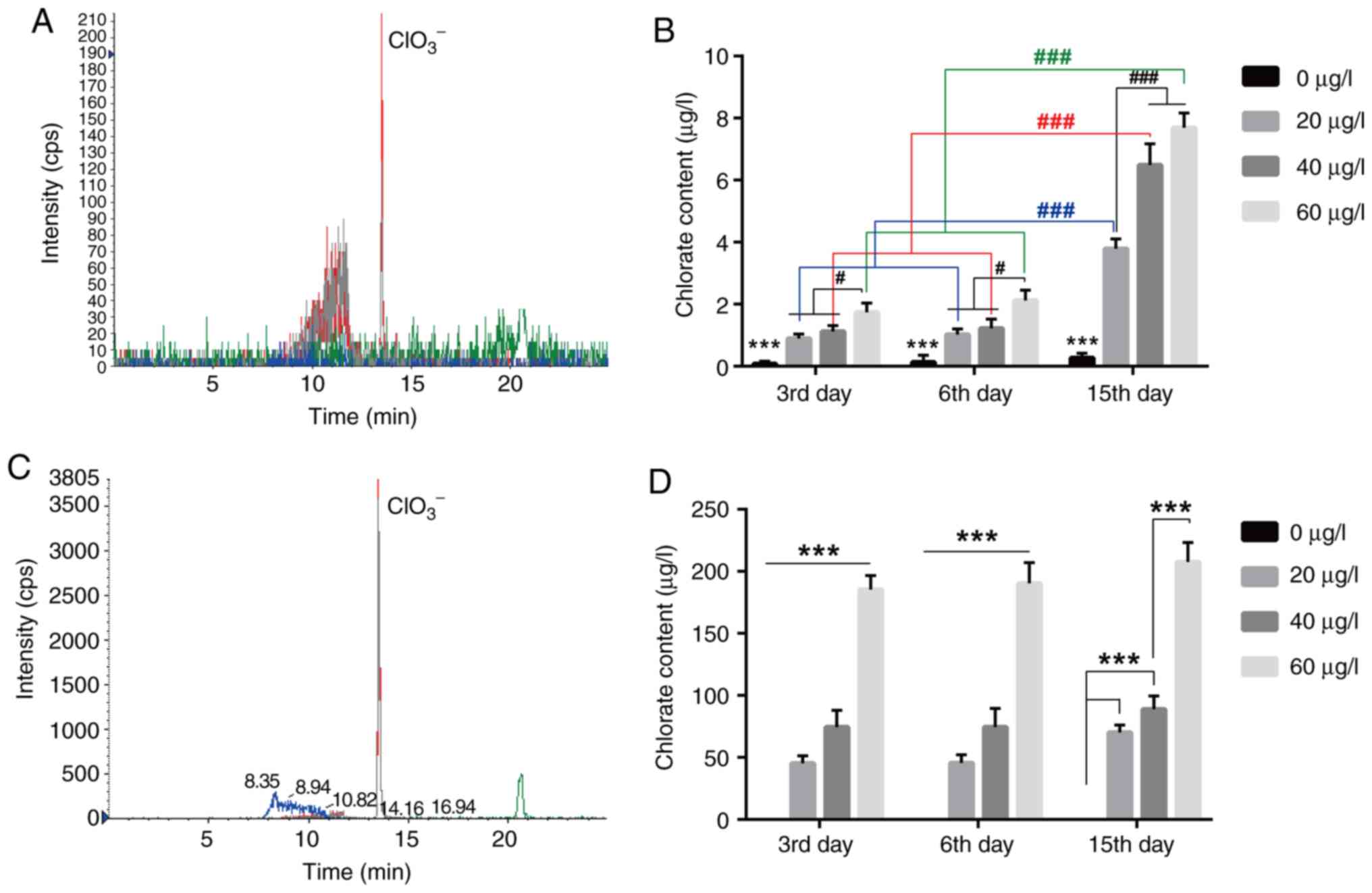 | Figure 2Changes in the chlorate content in
ozonated saline on the 3rd, 6 and 15th day. By using IC-MS, the
chlorate content was detected on the 3rd, 6 and 15th day in (A and
B) the blood bag and (C and D) saline bottle subgroups. The
chlorate concentration appeared to increase with time. (A) IC-MS
detected chlorate in 40 µg/ml ozonated saline in the blood bag
subgroup (peak time, 13.5 min; intensity, 210 cps) on the 3rd day.
(B) Chlorate content in the blood bag subgroup with varying
concentrations of ozonated saline on the 3rd, 6 and 15th day after
mixing. There was no statistically significant difference in the
chlorate content between the 3rd day and the 6th day after treating
with any concentration of ozone. On the 15th day, the chlorate
content increased significantly compared with that on the 3rd and
6th days in all treatment groups. (C) Chlorate was detected by
IC-MS on the 3rd day in 40 µg/ml ozonated saline in the saline
bottle subgroup (peak time, 13.5 min; intensity, 3,805 cps). (D)
Chlorate content in the saline bottle subgroup with varying
concentrations of ozonated saline on the 3rd, 6 and 15th day after
mixing. On the 15th day, the chlorate content increased
significantly compared with that on the 3rd day and the 6th day in
the 20 µg/ml ozone-saline solution. There was no significant
difference between the 3rd day, the 6th day and the 15th day in the
40 and 60 µg/ml ozone-saline solution. However, the chlorate
content in ozonated saline was elevated with the increase of the
ozone concentration. Values are expressed as the mean ± standard
deviation (n=3 for each group). Statistical analyses were performed
by repeated-measures two-way analysis of variance, followed by
Tukey's multiple-comparisons tests. ***P<0.001
compared with the 3rd day and the 6th day; #P<0.05,
###P<0.001. IC-MS, ion chromatography-mass
spectrometry; cps, counts per second. |
On the 3rd, 6 and 15th day, for the blood bag
subgroup (Fig. 2B) and the saline
bottle subgroup (Fig. 2D) at the
same time-points, the chlorate concentration increased with
increasing concentrations of ozone.
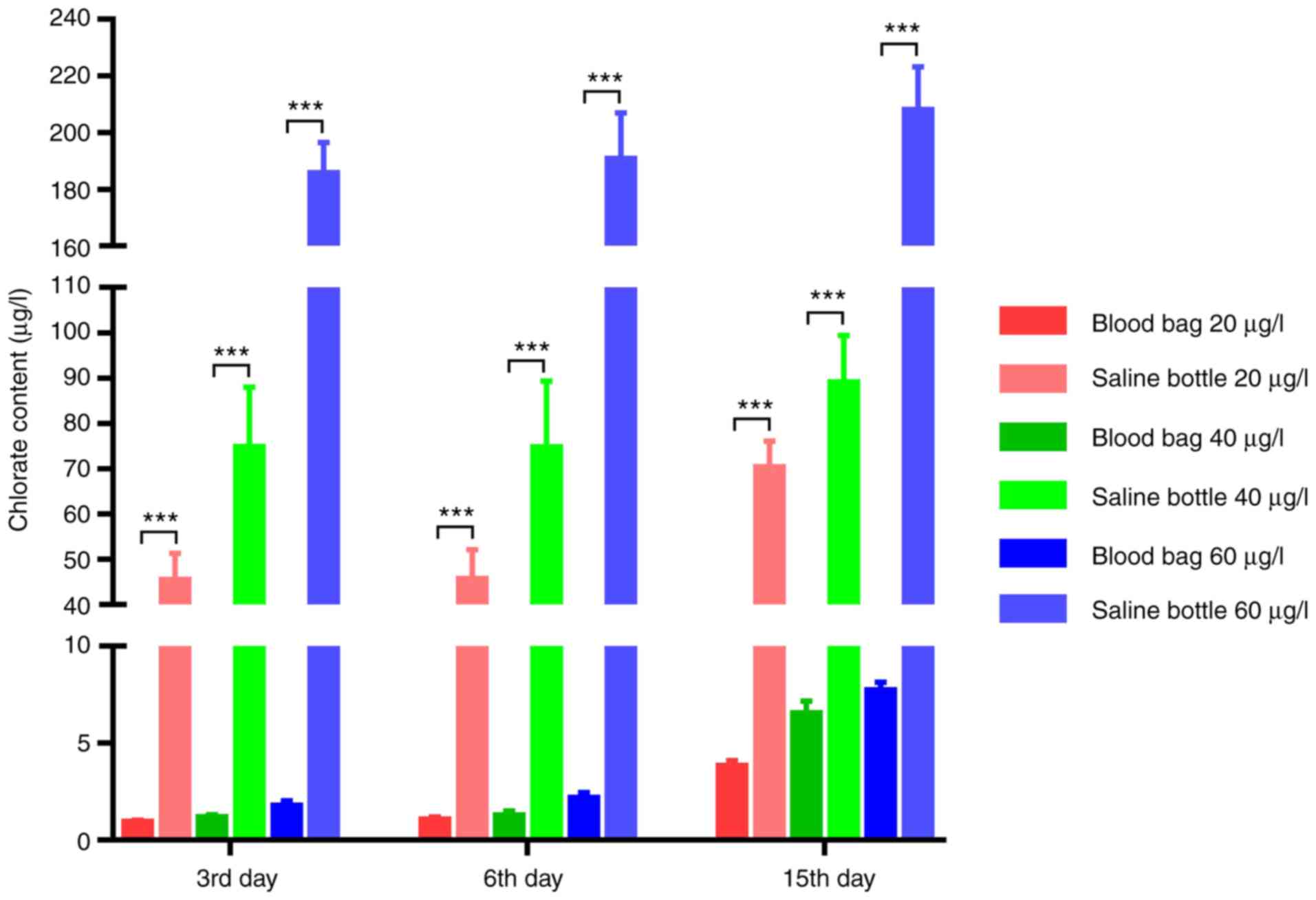
Under the same conditions (at the same time-points
and the same ozone concentration), in the ozone-resistant blood bag
subgroup, the chlorate content in the ozonated saline was
significantly lower than that in the saline bottle subgroup
(Fig. 3).
Perchlorate was not detected in the
ozone-saline or oxygen-saline solution
The Five standard solutions with different
concentrations (1, 2, 5, 10 and 20 µg/l) were added from low to
high concentration for the spiked recovery test. The recovery rates
were 86.6-101.0% on the 3rd day, 89.4-105.0% on the 6th day and
83.6-102.0% on the 15th day. The mass spectrometry results
indicated that perchlorate was not detected on the 3rd, 6 and 15th
day in either the ozone-saline or oxygen-saline solutions.
Discussion
The results of the present study indicated that
ozone is able to oxidize chloride ions in saline to form chlorate
and the chlorate content gradually increased with time. In
addition, higher ozone concentrations result in increased chlorate
levels. Importantly, ozone may react with its container and thereby
increase the levels of toxic substances in the ozone solution.
In the present study, when 100 ml of 20-60 µg/ml
ozone was mixed with an equal volume of saline, the content of
chlorate in the ozonated saline was between 0.90±0.14 and
207.6±15.63 µg/l. A low level (<0.4 µg/l) of chlorate was
detected in the absence of ozone in the blood bag, this could be a
result of detection errors of the machine, or from the material of
the blood bag. To the best of our knowledge, no study has reported
the toxic dose of intravenously infused chlorate, although the
World Health Organization Guidelines for drinking-water quality
stipulated that the maximum permitted concentration of chlorate in
drinking water is 0.7 mg/l (43).
One study observed the effect of intravenous or oral sodium
chlorate administration on the fecal shedding of Escherichia
coli in sheep. Sodium chlorate (150 mg/kg) was infused over 3 h
or less (a volume of 0.9% physiological saline containing 150 mg/kg
sodium chlorate in a total volume of 250 ml), whilst the control
group was administered the same dose of sodium chlorate orally. The
content of NaClO3 in the serum of sheep was measured at
4, 8, 16, 24 and 36 h after administration. The highest
concentration of NaClO3 in the serum was observed at 4 h
of infusion (194.1±28.4 µg/l). The same dose (150 mg/kg
NaClO3) was given orally, which also indicated a peak
serum level after 4 h, reaching 138.9±13.2 µg/l (44). According to the results of the
present study, the chlorate content in 100 ml ozonized saline was
between 0.90±0.14 µg/l and 207.6±15.63 µg/l; this was much lower
than the aforementioned toxic dose of chlorate and the maximum
limit of the drinking-water standard setting after metabolism in
the serum. However, since the chlorate in the ozone-saline solution
is administered intravenously, its toxicity requires careful
re-evaluation.
On the 3rd, 6 and 15th day, no chlorite was detected
in any of the groups. It is speculated that the ozonated saline did
not form any chlorite or the chlorite that had been formed within 3
days continued to be oxidized by ozone, turning into chlorate. On
the 3rd, 6 and 15th day, no perchlorate was detected in the two
groups. It appears that ozone mixed with normal saline does not
produce perchlorate within the observed timeframe (15 days) in the
present study. Since hypochlorite is formed instantaneously and
decomposes rapidly, no hypochlorite was detected in the present
study.
In order to simulate the ozone and saline reaction
scenarios in the clinic, the present study used two ozone-saline
containers that are commonly used in clinical settings: Saline
bottles (polypropylene) and ozone-resistant blood transfusion bags
[medical polyvinyl chloride, di(2-ethyl) hexyl phthalate
plasticized]. The results suggested that under the same conditions,
the chlorate content in ozonated saline in the blood bag made of
ozone-resistant material was much lower than that in the saline
bottle. As the reaction time went on, the chlorate content
increased significantly. It may therefore be indicated that the
material of the infusion container is able to affect the content of
the toxic substances in the solution. The saline bottle material
(polypropylene) may be oxidized by ozone, resulting in an increase
of the chlorate content. These results suggested that the syringe
and reaction container used for ozone therapy should consist of
ozone-resistant materials, which would be effective in reducing the
production of chlorate or any other toxic substances.
Previous studies indicated that oral administration
of chlorate has multiple toxic effects. Ali et al (45) reported that a single oral dose of
100-750 mg/kg sodium chlorate in rats caused intestinal DNA damage
through the production of ROS. Another study from the same group
suggested that the same dose of sodium chlorate caused acute kidney
injury in rats by producing an imbalance of redox reactions
(46). Furthermore, different doses
of sodium chlorate (0.106-1.06 mg/ml) not only induced oxidative
stress in human red blood cells in vitro, leading to
extensive damage to the cell membrane and reducing the anti-oxidant
response, but also changed the morphology of red blood cells,
increasing osmotic fragility. At the same time, exposure to
different concentrations of sodium chlorate (0-10 nM) may lead to
dose-dependent hemolysis (47).
Chlorate and perchlorate affect the function of the thyroid gland.
Following short-term (7 days) exposure to perchlorate (10 mg/l) and
chlorate (100 mg/l) in rats, serum T4 was significantly lower than
that in the control group (48). The
incidence of thyroid follicular cell hypertrophy in male and female
rats administered sodium chlorate was higher and the incidence of
thyroid cancer was higher in the 2,000 mg/l chlorate group compared
with that in the control group; furthermore, a small amount of
islet cell tumors were produced in female rats exposed to sodium
chlorate (49). As intravenous
infusion therapy with ozonated saline usually requires repeated
administrations in the short-term, further basic and clinical
research is required to determine whether the accumulation of
chlorate is able to affect blood, kidney and thyroid function.
According to Bocci et al (41), intravenous infusion of ozonated
saline is potentially toxic and therefore, they do not support the
systemic administration of ozone in this way. The specific reasons
are as follows: i) Ozonated saline may contain toxic substances
including H2O2, hypochlorous and hypochlorous
acid; ii) ozonation of saline is an unstable process and if it is
not injected on time, O3 will completely decompose
within 60 min; iii) during the infusion, the blood flow rate in the
vein affects the concentration of
H2O2-O3, suggesting that there may
be a variable biological oxidation process. Therefore, the therapy
does not meet the therapeutic principles of clinical drugs, namely
stability and clearly defined active components (41).
The present study suggests that there may be toxic
substances, e.g. chlorate, in ozonated saline, and the toxic dose
of these substances in the human body remains to be determined. As
such, the outcome of long-term intravenous infusion of ozonized
saline remains uncertain.
Of note, the present study has several limitations.
The content of chlorite, chlorate and perchlorate in ozonated
saline was only measured after 3 days in the present study, and it
remains elusive whether any chlorite was present in the ozonated
saline at earlier stages. In the clinic, ozonated saline is
prepared upon its use. In addition, chlorate and perchlorate are
relatively stable; therefore, their concentrations in the first 3
days should be less than that detected on the third day. As such,
the current data are instructive for clinical work. Usually, 100 ml
of ozonated saline is infused within half an hour during clinical
treatment. Bocci et al (41)
reported that ozone totally decomposed within 60 min and that
intravenous infusion of ozone solutions should be completed within
one hour; therefore, detection of chlorite, chlorate and
perchlorate in ozonated saline as soon as possible would provide
results that are more representative of the clinical scenario.
However, in the present study, differences between 3, 6 and 15 days
observed indicate that there may have still been some ozone
present, that may have led to the generation of chlorate beyond
several days.
In conclusion, ozonated saline solution contains
chlorate and the ozone may react with the polypropylene of the
saline bottle to increase the chlorate content in the solution.
Although studies have reported that intravenous infusion of
ozonated saline is safe and effective, due to the lack of blood
chlorate toxicology studies, it remains elusive whether the levels
of chlorate detected in the ozonated saline in this present study
(0.90±0.14-207.6±15.63 µg/l) are safe for the solution to be given
intravenously. Therefore, clinical intravenous infusion of ozonated
saline should be used with caution. Importantly, ozone reacts with
various containers and an ozone-resistant container for ozonated
solution infusion is recommended.
Acknowledgements
Not applicable.
Funding
This work was supported by the Science and
Technology Department of Guizhou Province [grant no. LH(2015)7554],
the Excellent Young Talents Project (grant no. 18zy-004) and the
Innovative Training Program of Zunyi Medical University [grant no.
(2015) 3109].
Availability of data and materials
The datasets generated and analyzed during the
present study are available from the corresponding author on
reasonable request.
Authors' contributions
LM, SW, JY, DZ, YYL, YZ and SC performed the
experiments, wrote the manuscript and prepared figures. YL and SC
conceived and designed the experiments and provided the reagents,
materials and analysis tools. All authors reviewed the data and
drafts of the paper.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Manoto SL, Maepa MJ and Motaung SK:
Medical ozone therapy as a potential treatment modality for
regeneration of damaged articular cartilage in osteoarthritis.
Saudi J Biol Sci. 25:672–679. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Baranova IV: The use of the functional
state of the joints for the estimation of the effectiveness of the
application of oxygen/ozone therapy for the rehabilitative
treatment of the patients suffering from knee arthritis. Vopr
Kurortol Fizioter Lech Fiz Kult. 95:42–48. 2018.PubMed/NCBI View Article : Google Scholar : (In Russian).
|
|
3
|
Lopes de Jesus CC, Dos Santos FC, de Jesus
LMOB, Monteiro I, Sant'Ana M and Trevisani VFM: Comparison between
intra-articular ozone and placebo in the treatment of knee
osteoarthritis: A randomized, double-blinded, placebo-controlled
study. PLoS One. 12(e0179185)2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Raeissadat SA, Tabibian E, Rayegani SM,
Rahimi-Dehgolan S and Babaei-Ghazani A: An investigation into the
efficacy of intra-articular ozone (O2-O3) injection in patients
with knee osteoarthritis: A systematic review and meta-analy. J
Pain Res. 11:2537–2550. 2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Beyaz SG and Sayhan H: Six-month results
of cervical intradiscal oxygen-ozone mixture therapy on patients
with neck pain: Preliminary findings. Pain physician. 21:E449–E456.
2018.PubMed/NCBI
|
|
6
|
Elawamy A, Kamel EZ, Hassanien M, Wahba OM
and Amin SE: Implication of two different doses of intradiscal
ozone-oxygen injection upon the pain alleviation in patients with
low back pain: A randomized, single-blind study. Pain Physician.
21:E25–E31. 2018.PubMed/NCBI
|
|
7
|
Biazzo A, Corriero AS and Confalonieri N:
Intramuscular oxygen-ozone therapy in the treatment of low back
pain. Acta Biomed. 89:41–46. 2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Costa T, Linhares D, Ribeiro da Silva M
and Neves N: Ozone therapy for low back pain. A systematic review.
Acta Reumatol Port. 43:172–181. 2018.PubMed/NCBI
|
|
9
|
Braidy N, Izadi M, Sureda A,
Jonaidi-Jafari N, Banki A, Nabavi SF and Nabavi SM: Therapeutic
relevance of ozone therapy in degenerative diseases: Focus on
diabetes and spinal pain. J Cell Physiol. 233:2705–2714.
2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Raeissadat SA, Rayegani SM, Sadeghi F and
Rahimi-Dehgolan S: Comparison of ozone and lidocaine injection
efficacy vs dry needling in myofascial pain syndrome patients. J
Pain Res. 11:1273–1279. 2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tirelli U, Cirrito C, Pavanello M,
Piasentin C, Lleshi A and Taibi R: Ozone therapy in 65 patients
with fibromyalgia: An effective therapy. Eur Rev Med Pharmacol Sci.
23:1786–1788. 2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Rowen RJ and Robins H: Ozone therapy for
complex regional pain syndrome: Review and case report. Curr Pain
Headache Rep. 23(41)2019.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Lin SY, Zhang SZ, An JX, Qian XY, Gao XY,
Wang Y, Zhao WX, Eastwood D, Cope DK and Williams JP: The effect of
ultrasound-guided percutaneous ozone injection around cervical
dorsal root ganglion in zoster-associated pain: A retrospective
study. J Pain Res. 11:2179–2188. 2018.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Hu B, Zheng J, Liu Q, Yang Y and Zhang Y:
The effect and safety of ozone autohemotherapy combined with
pharmacological therapy in postherpetic neuralgia. J Pain Res.
11:1637–1643. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Di Mauro R, Cantarella G, Bernardini R, Di
Rosa M, Barbagallo I, Distefano A, Longhitano L, Vicario N,
Nicolosi D, Lazzarino G, et al: The Biochemical and pharmacological
properties of ozone: The smell of protection in acute and chronic
diseases. Int J Mol Sci. 20(pii: E634)2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Clavo B, Santana-Rodriguez N, Gutierrez D,
Lopez JC, Suarez G, Lopez L, Robaina F and Bocci V: Long-term
improvement in refractory headache following ozone therapy. J
Altern Complement Med. 19:453–458. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Li LY and Ni JX: Efficacy and safety of
ozonated autohemotherapy in patients with hyperuricemia and gout: A
phase I pilot study. Exp Ther Med. 8:1423–1427. 2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Akbudak IH, Kucukatay V, Kilic-Erkek O,
Ozdemir Y and Bor-Kucukatay M: Investigation of the effects of
major ozone autohemotherapy application on erythrocyte
deformability and aggregation. Clin Hemorheol Microcirc.
71:365–372. 2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sancak EB, Turkön H, Çukur S, Erimsah S,
Akbas A, Gulpinar MT, Toman H, Sahin H and Uzun M: Major ozonated
autohemotherapy preconditioning ameliorates kidney
ischemia-reperfusion injury. Inflammation. 39:209–217.
2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Bocci V: Ozonization of blood for the
therapy of viral diseases and immunodeficiencies A hypothesis. Med
Hypotheses. 39:30–34. 1992.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Bocci V, Borrelli E, Travagli V and
Zanardi I: The ozone paradox: Ozone is a strong oxidant as well as
a medical drug. Med Res Rev. 29:646–682. 2009.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Bocci V: Autohaemotherapy after treatment
of blood with ozone A reappraisal. J Int Med Res. 22:131–144.
1994.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Tusat M, Mentese A, Demir S, Alver A and
Imamoglu M: Medical ozone therapy reduces oxidative stress and
testicular damage in an experimental model of testicular torsion in
rats. Int Braz J Urol. 43:1160–1166. 2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Al-Saadi H, Potapova I, Rochford ET,
Moriarty TF and Messmer P: Ozonated saline shows activity against
planktonic and biofilm growing Staphylococcus aureus in vitro: A
potential irrigant for infected wounds. Int Wound J. 13:936–942.
2016.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Sagai M and Bocci V: Mechanisms of action
involved in ozone therapy: Is healing induced via a mild oxidative
stress? Med Gas Res. 1(29)2011.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Borrelli E: Mechanism of action of oxygen
ozone therapy in the treatment of disc herniation and low back
pain. Acta Neurochir Suppl. 108:123–125. 2011.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Azuma K, Mori T, Kawamoto K, Kuroda K,
Tsuka T, Imagawa T, Osaki T, Itoh F, Minami S and Okamoto Y:
Anti-inflammatory effects of ozonated water in an experimental
mouse model. Biomed Rep. 2:671–674. 2014.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Lu L, Pan C, Chen L, Hu L, Wang C, Han Y,
Yang Y, Cheng Z and Liu WT: AMPK activation by peri-sciatic nerve
administration of ozone attenuates CCI-induced neuropathic pain in
rats. J Mol Cell Biol. 9:132–143. 2017.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Yu M, Zhao Y and Zhang X: Gardenoside
combined with ozone inhibits the expression of P2X3 and P2X7 purine
receptors in rats with sciatic nerve injury. Mol Med Rep.
17:7980–7986. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Wang J, Wu M, Lin X, Li Y and Fu Z:
Low-concentration oxygen/ozone treatment attenuated radiculitis and
mechanical allodynia via PDE2A-cAMP/cGMP- NF-κB/p65 signaling in
chronic radiculitis rats. Pain Res Manag.
2018(5192814)2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Wu MY, Xing CY, Wang JN, Li Y, Lin XW and
Fu ZJ: Therapeutic dosage of ozone inhibits autophagy and apoptosis
of nerve roots in a chemically induced radiculoneuritis rat model.
Eur Rev Med Pharmacol Sci. 22:1787–1797. 2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Zhao X, Li Y, Lin X, Wang J, Zhao X, Xie
J, Sun T and Fu Z: Ozone induces autophagy in rat chondrocytes
stimulated with IL-1β through the AMPK/mTOR signaling pathway. J
Pain Res. 11:3003–3017. 2018.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Fuccio C, Luongo C, Capodanno P, Giordano
C, Scafuro MA, Siniscalco D, Lettieri B, Rossi F, Maione S and
Berrino L: A single subcutaneous injection of ozone prevents
allodynia and decreases the over-expression of pro-inflammatory
caspases in the orbito-frontal cortex of neuropathic mice. Eur J
Pharmacol. 603:42–49. 2009.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Karatieieva S, Muzyka N, Semenenko S,
Bakun O and Kozlovskaya I: Ultrastructural changes of wound
macrophages under the influence of intravenous ozone therapy in
patients with diabetes and inflammatory processes of soft tissues.
Georgian Med. News:98–101. 2018.PubMed/NCBI
|
|
35
|
Tafil-Klawe M, Woźniak A, Drewa T,
Ponikowska I, Drewa J, Drewa G, Włodarczyk K, Olszewska D, Klawe J
and Kozłowska R: Ozone therapy and the activity of selected
lysosomal enzymes in blood serum of patients with lower limb
ischaemia associated with obliterative atheromatosis. Med Sci
Monit. 8:CR520–CR525. 2002.PubMed/NCBI
|
|
36
|
Katiukhin LN: Influence of the course of
treatment by injections of ozonized saline on rheological
properties of erythrocytes in patients with complex pathology. Hum
Physiol. 42:672–677. 2016.PubMed/NCBI
|
|
37
|
Volkhovskaya NB, Tkachenko SB and
Belopolsky AA: Modulation of phagocytic activity of blood
polynuclear leukocytes with ozonized physiological saline. Bull Exp
Biol Med. 146:559–561. 2008.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Qu DD, Peng FJ, Liu L, Yang SL and Guo YB:
Effect of ozonized saline on signaling passway of Keap1-Nrf2-ARE in
rat hepatocytes. Zhonghua Gan Zang Bing Za Zhi. 19:367–371.
2011.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
39
|
Razumovskii SD, Konstantinova ML,
Grinevich TV, Korovina GV and Zaitsev VY: Mechanism and kinetics of
the reaction of ozone with sodium chloride in aqueous solutions.
Kinet Catal. 51:492–496. 2010.
|
|
40
|
Boyarinov GA, Gordetsov AS, Peretyagin SP,
Boyarinova LV and Martusevich AK: Chemical transformations in
treatment of saline solution with ozone-oxygen gas mixture. J
Health Inequal. 2:194–199. 2016.
|
|
41
|
Bocci V, Zanardi I, Borrelli E and
Travagli V: Reliable and effective oxygen-ozone therapy at a
crossroads with ozonated saline infusion and ozone rectal
insufflation. J Pharm Pharmacol. 64:482–489. 2012.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Zhang T, Cui H, Hu D, Cai F, Ma J and Zhu
Q: Simultaneous determination of chlorite, chlorate, perchlorate
and bromate of seafood processed products by IC-MS. Food Sci
Technol. 42:326–330. 2017.(In Chinese).
|
|
43
|
WHO. Guidelines Approved by the Guidelines
Review Committee. In: Guidelines for drinking-water quality: Fourth
edition incorporating the first addendum World Health Organization,
Geneva, 2017.
|
|
44
|
Smith DJ, Taylor JB, West M and Herges G:
Effect of intravenous or oral sodium chlorate administration on the
fecal shedding of Escherichia coli in sheep. J Anim Sci.
91:5962–5969. 2013.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Ali SN, Ansari FA, Arif H and Mahmood R:
Sodium chlorate induces DNA damage and DNA-protein cross-linking in
rat intestine: A dose dependent study. Chemosphere. 177:311–316.
2017.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Ali SN, Arif H, Khan AA and Mahmood R:
Acute renal toxicity of sodium chlorate: Redox imbalance, enhanced
DNA damage, metabolic alterations and inhibition of brush border
membrane enzymes in rats. Environ Toxicol. 33:1182–1194.
2018.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Ali SN, Ahmad MK and Mahmood R: Sodium
chlorate, a herbicide and major water disinfectant byproduct,
generates reactive oxygen species and induces oxidative damage in
human erythrocytes. Environ Sci Pollut Res Int. 24:1898–1909.
2017.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Khan MA, Fenton SE, Swank AE, Hester SD,
Williams A and Wolf DC: A mixture of ammonium perchlorate and
sodium chlorate enhances alterations of the pituitary-thyroid axis
caused by the individual chemicals in adult male F344 rats. Toxicol
Pathol. 33:776–783. 2005.PubMed/NCBI View Article : Google Scholar
|
|
49
|
National Toxicology Program: Toxicology
and carcinogenesis studies of sodium chlorate (Cas No. 7775-09-9)
in F344/N rats and B6C3F1 mice (drinking water studies). Natl
Toxicol Program Tech Rep Ser: 1-255, 2005.
|