Introduction
Early repolarization patterns are characterized by J
point elevation, distinct J waves combined with or without
ST-segment elevation or slurring in the terminal portion of the QRS
wave in inferolateral electrocardiogram (ECG) leads. An early
repolarization pattern on ECGs has traditionally been considered to
be benign (1,2); however, according to previous
experimental studies, a more pathological prognosis has been
suggested (3,4), and subsequently confirmed in clinical
studies reported by Haïssaguerre et al (5) and Nam et al (6,7).
The early repolarization hypothesis could be
explained in terms of ionic and cellular mechanisms. The ionic and
cellular mechanisms associated with generation of an early
repolarization pattern are similar to those responsible for J wave
manifestation and ST-segment elevation in Brugada syndrome (BrS)
(4). A net outward shift in the
balance of the current active in the early phases of the epicardial
action potential (AP), which is secondary to reduction of
ICa or INa or augmentation of
IK-ATP, has been demonstrated to underlie the early
repolarization ECG pattern and substrate responsible for the
development of life-threatening arrhythmias associated with early
repolarization syndrome (ERS) (8-12).
The delayed depolarization hypothesis could be
expressed as follows. An SCN5A loss-of-function mutation
leads to reduced sodium current, which may in turn decrease the
Vmax of the membrane AP and thus reduce membrane excitability. This
may result in conduction delays. The conduction delay between the
right ventricular apex (RVa) and right ventricular outflow tract
(RVot) generates the BrS coved-type ECG.
However, debates on the mechanism underlying J wave
syndrome including BrS and ERS have been ongoing for decades
(13). Theoretically, both the two
mechanisms-delayed depolarization theory and early repolarization
theory are feasible. Recently, Haïssaguerre et al (14) defined ERS with/without a conduction
delay. In other words, they described both ERS with delayed
depolarization and ERS with early repolarization.
The delayed depolarization theory may be explained
by regional conduction velocity heterogeneity in the ventricular
myocardium (15). Thus, if
polymorphic ventricular tachycardia (pVT) develops without any
regional conduction velocity heterogeneity, it would be less
compatible with the delayed depolarization. The aim of the present
study was to identify whether pVT could develop without regional
conduction velocity heterogeneity. In the present study, the
transmural conduction time was evaluated at several transmural
locations using a canine ERS wedge preparation model.
Materials and methods
Wedge preparations and electrogram
recordings
All experiments were conducted in accordance with
the guidelines for the management and use of laboratory animals by
the Institutional Animal Care and Use Committee. The study was
approved by the Animal Care and Use Committee at Chonnam National
University, Gwangju, Republic of Korea (approval number, CNU
IACUC-H-2017-33). Detailed methods for the wedge isolation and
electrogram recording from coronary-perfused canine left ventricle
(LV) wedge preparations have previously been reported (16,17). The
animals were supplied by Orient Bio, Inc. Briefly, adult mongrel
dogs (age, ~1 year-old, weight, 20-35 kg; 9 males, 9 females)
underwent anticoagulation with heparin (300 units/kg IV) and were
anesthetized with pentobarbital (30-35 mg/kg IV). The chest was
opened via a left thoracotomy, and the heart was excised and placed
in a cardioplegic solution [cold (4˚C) Tyrode's solution containing
12 mmol/l KCl]. Death of the animal was confirmed by personnel
trained to recognize cessation of vital signs in euthanasia. The
wedge preparations (2.2-2.4x2.0-2.2x1.8-1.9 cm3) were
transmurally dissected from the inferolateral free wall of the LV.
The second or third diagonal artery ostium was cannulated using a
handmade small plastic cannula and fixed using a thread, while the
cardioplegic solution [Tyrode's solution containing NaCl (129 mM),
KCl (12 mM), NaH2PO4 (0.9 mM), NaHCO3 (20
mM), CaCl2 (1.8 mM), MgSO4 (0.5 mM) and glucose (5.5 mM)] was
delivered via the cannula. Non-perfused tissue was carefully cut
using a razor blade. After being placed in a tissue bath, Tyrode's
solution containing KCl (4 mM) was delivered using a roller pump
(Cole Parmer Instrument Co., Ltd.) at a constant flow rate of 8-10
ml/min and warmed to 37±0.5˚C. The temperature was maintained at
37±0.5˚C throughout the experiment. The pH was 7.4.
The preparation was equilibrated in the tissue bath
until electrically stabilized for ~1 h, while being stimulated at a
cycle length of 1,000 msec using bipolar silver electrodes,
insulated up to the tips. The preparations were stimulated
endocardially. A transmural pseudo-ECG was obtained using two
electrodes, consisting of AgCl half cells placed in the tissue
bath. The tip of the two electrodes were placed along the same axis
as the transmembrane AP recordings. The distance between
endocardial or epicardial surface and the pseudo-ECG electrode was
1.0-1.5 cm; the epicardial electrode was connected to the positive
input of the ECG amplifier.
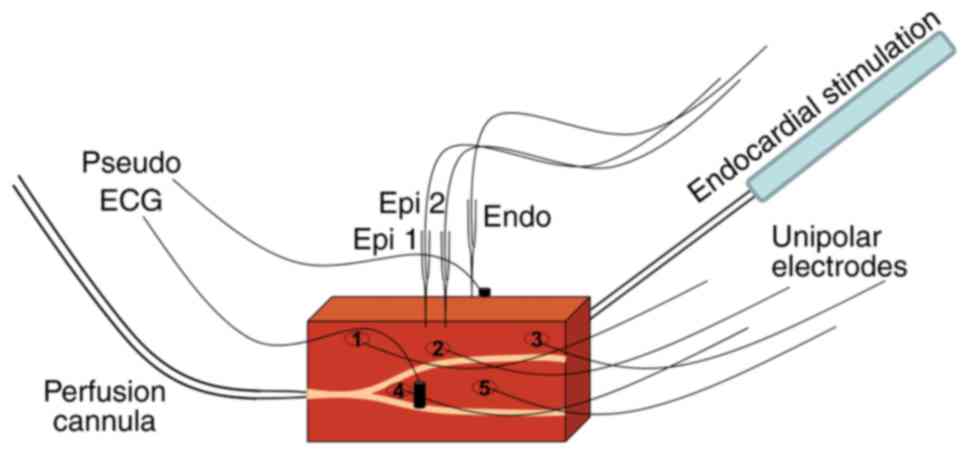
The transmembrane APs were acquired simultaneously
from two epicardial sites (distance from epicardial 1 to 2 was 5-10
mm) and one endocardial site using floating microelectrodes (DC
resistance=10-20 MΩ) filled with 2.7 mol/l KCl; each microelectrode
was connected to a high-input impedance amplifier. Five unipolar
electrodes (1, 2, 3, 4 and 5) were evenly distributed on the
epicardial surface (Fig. 1). Each
individual microelectrode had its own reference electrode at the
shortest possible distance. The virtual bipolar electrograms were
derived as the difference of the adjacent two unipolar electrograms
(1-2, 2-3, 1-4, 2-4, 2-5 and 3-5 pairs).
Measurement of the transmural
conduction time
Spike2 for Windows version 7 (Cambridge Electronic
Design Ltd.) was used to record and analyze ECGs, electrograms and
APs. All electrograms and analyses were manually checked by three
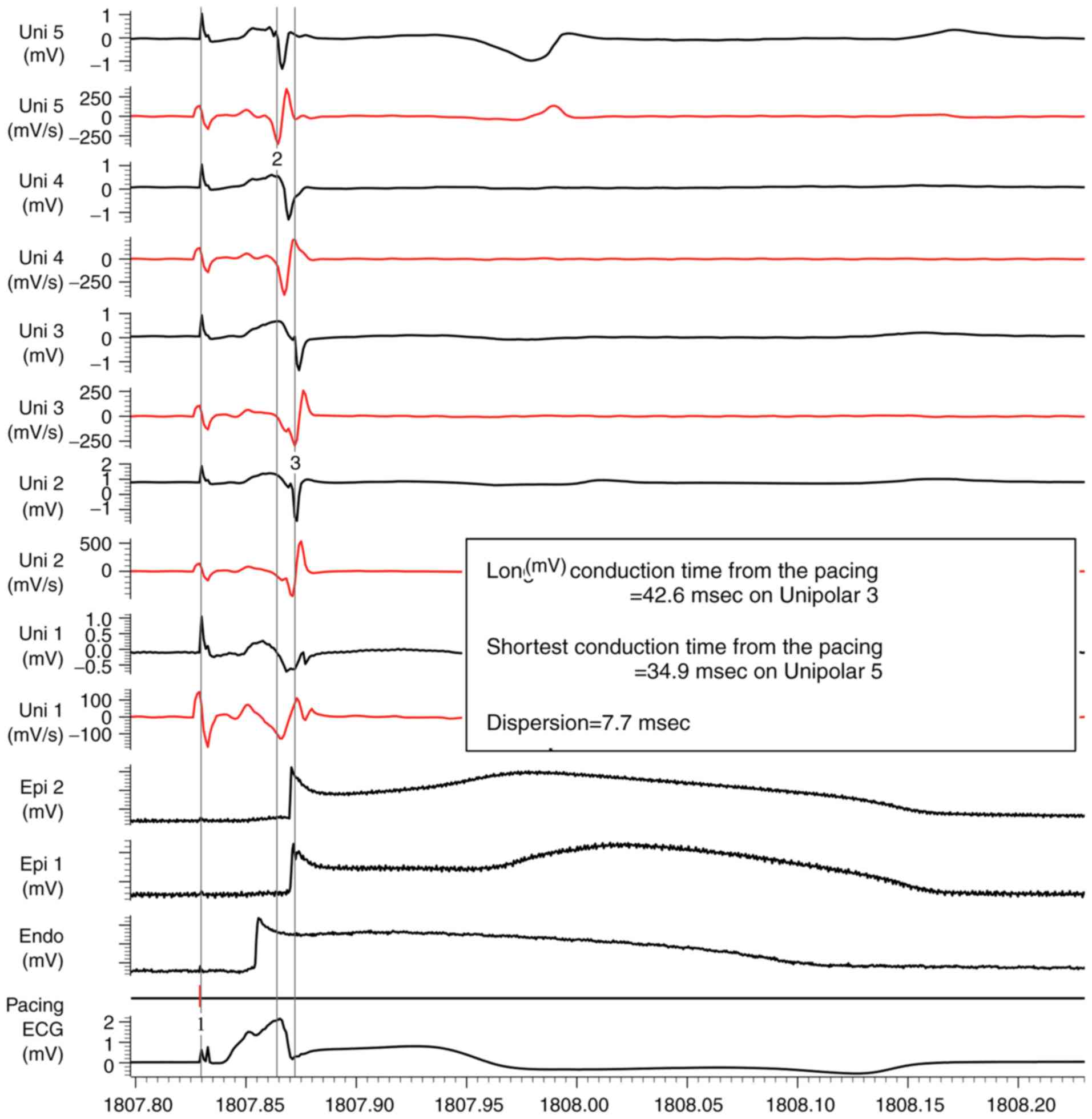
independent observers. The transmural conduction time was defined
as the time from the endocardial pacing to the maximal negative
deflection (dV/dt) of the signal at the unipolar
electrode. The transmural conduction times were measured prior to
the perfusion of provocative agents and immediately before pVT
development at the five fixed epicardial unipolar electrodes and
two fixed epicardial floating microelectrodes. The transmural
conduction times at these seven fixed transmural locations were
evaluated. Conduction time dispersion was defined as the difference
between the longest and the shortest conduction time.
Arrhythmia induction
The ERS model setup and arrhythmia induction
procedure were conducted according to the previously reported
methods (3,9). To produce the pharmacologically similar
ERS genotypes, the Ito agonist NS5806 (9-10 µM), calcium
channel blocker verapamil (2 µM) and acetylcholine (ACh; 2 µM) were
added to the perfusate. All preparations were endocardially
stimulated at a cycle length of 1,000 msec. When ventricular
arrhythmias occurred spontaneously after the perfusion of
provocative agents, this was referred to as arrhythmia
inducibility.
Statistical analysis
For continuous variables, a paired Student's t-test
was used to analyze differences between the before and after the
provocative agents. For statistical analyses, the Statistical
Package for the Social Sciences 25.0 software (IBM corp.) was used.
Data are described as mean ± standard error of the mean (SEM). A
two-tailed analysis was used, and a P-value of <0.05 indicated
statistical significance.
Results
The transmural pseudo-ECG and endocardial/epicardial
APs were recorded in the coronary-perfused canine left ventricular
wedge preparations (n=18). All preparations were endocardially
stimulated at a cycle length of 1,000 msec. The transmural
conduction time and the dispersion were measured. As indicated in
Fig. 2, the longest conduction time
on Unipolar 3 was 42.6 msec and the shortest conduction time on
Unipolar 5 was 34.9 msec. Thus, the transmural conduction time
dispersion was 7.7 msec in the preparation.
Coronary-perfusates of Ito agonist,
calcium channel blocker and ACh were used to induce a state similar
to the genetic defects and conditions known to be associated with
ERS. In the present study, the ERS model was induced in 14/18
preparations. Under baseline conditions, the ECG did not show a
marked J wave and augmentation of the AP notch was not seen in the
epicardial sites (Fig. 3A). In the
ECG, marked J waves with ST-segment elevation were induced by the
Ito agonist NS5806 (9-10 µM), Ca2+ channel
blocker verapamil (2 µM), and ACh (2 µM), secondary to augmentation
of the AP notch in the epicardium but not in the endocardium. For
example, the maintained dome at the epicardial 1 electrode and loss
of the dome at the epicardial 2 electrode were identified (Fig. 3B). It resulted in phase 2 re-entry
(P2R) (Fig. 3B). Successful
propagation of the P2R beat generated VT/VF on the electrograms in
Fig. 3C. The pVT sustained for 1-2
sec in the beginning and sustained for more than 30 sec (Fig. 3D). The pVTs developed in 14/18
preparations. Slight ‘delayed’ phase 0 upstrokes of the
transmembrane AP occurred in the preparations. Increases in the
conduction delay were 3.2±2.9 and 1.8±2.8 msec for the epicardial
glass microelectrodes 1 and 2, respectively.
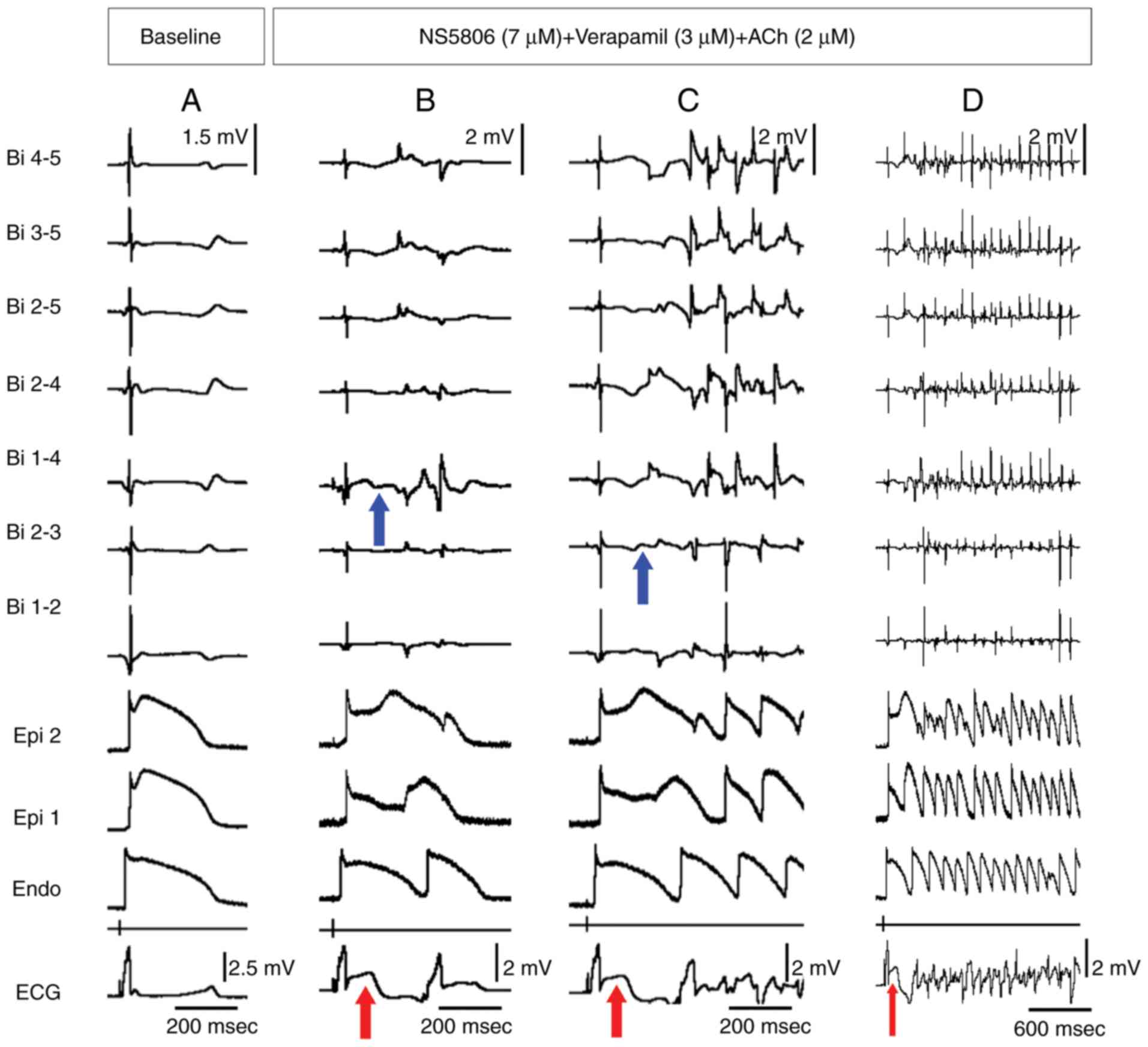 | Figure 3Experimental model of ERS created
using a combination of the Ito agonist (NS5806), calcium channel
blocker (verapamil) and ACh to mimic the genetic defects and
conditions known to be associated with ERS. (A) Baseline. (B)
Recorded during stimulation of the endocardium at a BCL of 1,000
msec at 20 min after the addition of the provocative agents to the
coronary perfusate. Note the appearance of a pronounced ST-segment
elevation (red arrows) in the ECG, low amplitude fractionated
bipolar electrogram activity (Bi 1-4, Bi 2-3; blue arrows)
secondary to epicardial AP maintained dome and loss-of-dome and
phase 2 reentry. The epicardial reentry induced a single echo to
the endocardium. (C) Then, the P2R propagated to the endocardium
and precipitated pVT. The pVT sustained for 1-2 sec in the
beginning. (D) The pVT continued for more than 30 sec. APs, action
potentials; Bi, bipolar electrode; ECG, electrocardiogram; Endo,
endocardial; Epi, epicardial; pVT, polymorphic ventricular
tachycardia; ACh, acetylcholine. |
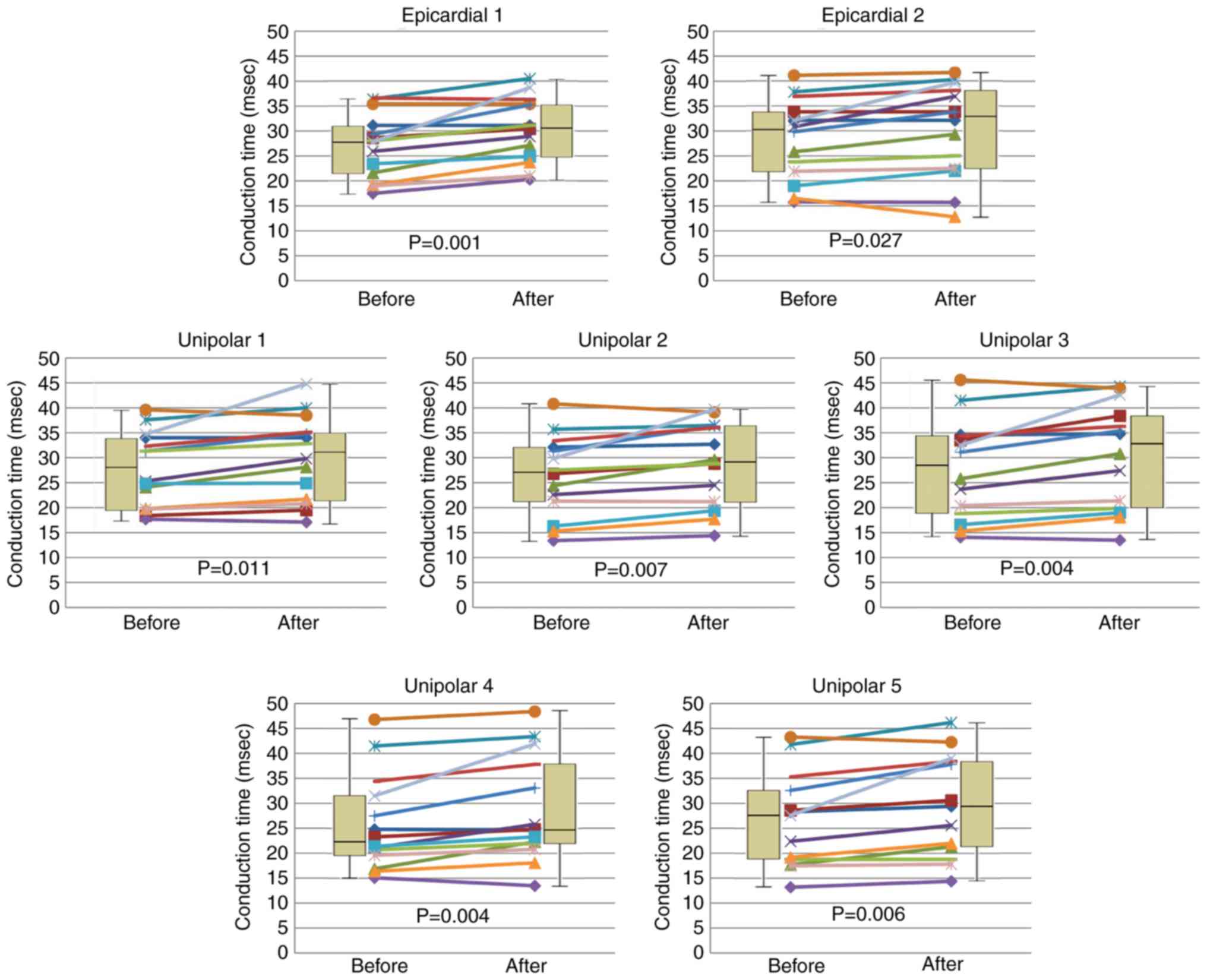
The transmural conduction time, during which the
impulse propagated from the endocardial pacing site to each
epicardial site (two epicardial glass microelectrodes and five
epicardial unipolar electrodes), increased significantly after the
Ito agonist NS5806 (9-10 µM), Ca2+ channel
blocker verapamil (2 µM) and Ach (2 µM) were perfused (Fig. 4; Table
I). The mean increase in the conduction time before and after
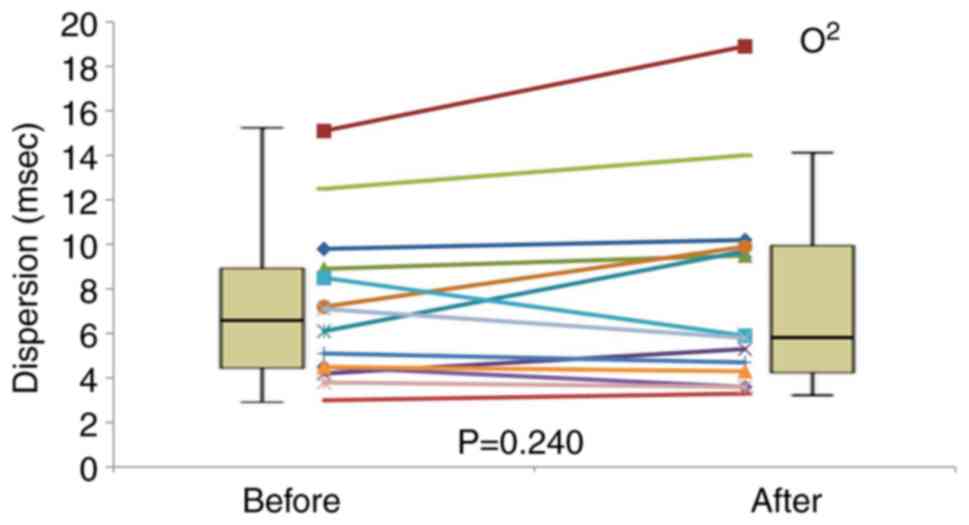
the perfusion of provocative agents was 2.6±0.4 msec. However,
dispersion of the transmural conduction time did not exhibit any
significant difference (7.16±0.93 msec vs. 7.76±1.21 msec; P=0.240;
Fig. 5).
 | Table ITransmural conduction time during
which the impulse propagates from the endocardial pacing site to
each epicardial site (2 epicardial glass microelectrodes and 5
epicardial unipolar electrodes) before (n=14) and after (n=14) the
provocative agents were perfused. |
Table I
Transmural conduction time during
which the impulse propagates from the endocardial pacing site to
each epicardial site (2 epicardial glass microelectrodes and 5
epicardial unipolar electrodes) before (n=14) and after (n=14) the
provocative agents were perfused.
| Electrode | Transmural
conduction time before treatment, msec | Transmural
conduction time after treatment, msec | P-value |
|---|
| Glass electrode
1 | 27.1±1.7 | 30.3±1.7 | 0.001 |
| Glass electrode
2 | 28.3±2.1 | 30.2±2.5 | 0.027 |
| Unipolar 1 | 27.9±1.9 | 30.1±2.3 | 0.011 |
| Unipolar 2 | 26.4±2.1 | 28.9±2.2 | 0.007 |
| Unipolar 3 | 27.7±2.6 | 30.4±2.8 | 0.004 |
| Unipolar 4 | 25.7±2.5 | 28.5±2.8 | 0.004 |
| Unipolar 5 | 26.6±2.6 | 29.5±2.9 | 0.006 |
| Dispersion | 7.16±0.93 | 7.76±1.21 | 0.240 |
Discussion
ERS is associated with the gain-of-function
mutations in the pore-forming subunit of the ATP-sensitive
potassium channel (KCNJ8) (10,12),
loss-of-function mutations in the α1, β2, and α2δ subunits of the
cardiac L-type calcium channel (CACNA1C, CACNB2 and
CACNA2D1) (11), and
loss-of-function mutations in the sodium channel activity
(SCN5A) (18). Moreover, the
greater vulnerability of the inferior wall of LV to early
repolarization has been ascribed to the presence of a higher
density of the transient outward current (Ito) (9). Both the electrocardiographic and
arrhythmic features of ERS are enhanced by vagal influences
(19-24).
Thus, a pharmacological approach was used in the present study to
produce ERS-related conditions and genetic defects. Several agents
were used, such as NS5806 for increased Ito current,
verapamil for the loss-of-function mutation in the calcium channel
activity and ACh for increased vagal tone (4,8,17).
According to the depolarization abnormality theory
of BrS, the syndrome develops due to a difference in the conduction
time between the RVot (25) and RVa,
and a 200 msec difference in the conduction time is necessary
(26). This may be regarded as a
longitudinal conduction time difference; however, the longitudinal
conduction time is different from the transmural conduction time
reported in the present study (endocardial to epicardial conduction
time). Therefore, it may be illogical to explain the
arrhythmogenicity of BrS using the results of the present
transmural conduction time study. However, in certain examples of
ERS reported in a study by Haïssaguerre et al (14), the epicardial depolarization
wavefront did not cross the J wave onset. This means that the local
conduction delay is shorter and, thus, local conduction time
dispersion is small. Therefore, the result of the present study
demonstrated JWS without a conduction delay, which was previously
classified by Haïssaguerre et al (14). It was identified that
arrhythmia reported in the present study was induced spontaneously,
without conduction time heterogeneity. Di Diego et al
(27)reported that there was no
significant conduction delay between the RVot and RVa in their
canine whole heart Langendorff model of BrS.
In the present experiment, the Ito
agonist NS5806 (9-10 µM), Ca2+ channel blocker verapamil
(2 µM) and Ach (2 µM) induced prominent J waves due to the
transmural voltage gradients. In brief, K+ efflux by the
Ito agonist and Ca2+ influx by the Ca channel
blocker were involved in epicardial repolarization due to the dense
distribution of Ito in the epicardium. It was
hypothesized that the P2R was induced by regional AP loss of dome
and maintained dome in the epicardium (Fig. 3B). This phenomenon is associated with
heterogeneous shortening of the epicardial action potential
duration (APD). Eventually, transepicardial heterogeneity induced a
transmural voltage gradient and precipitated VT/VF. Koncz et
al (9) reported the
heterogeneous shortening of APD90 in the same model.
According to our previous study, the QT interval was only prolonged
by 13 msec, and the value did not contribute to the occurrence of
ventricular arrhythmia (28).
Moreover, the results of the present study indicated that there was
no significant difference in the QT interval when compared to the
baseline state.
Assuming that the ERS is generated by delayed
depolarization or early repolarization, one of the key factors is a
voltage gradient (8,13,14). In
all theories, a great enough voltage gradient is required to induce
reentrant arrhythmia. In the present study, the mean increase in
the transmural conduction time after perfusing the provocative
agents was only 2.6±0.4 msec, which was notably smaller than the
200 msec suggested by Wilde et al (26). This would be insufficient to create a
steep transmural voltage gradient to generate arrhythmia. However,
in the present experiment, the transmural dispersion of
repolarization (TDR) was very long. For example, the TDR in
Fig. 3B was 200 msec. The epicardial
1 electrode had a short APD and the endocardial electrode had a
long APD, which induced a large TDR (200 msec). In the example
presented in Fig. 3, the phase 2
voltage gradient between the endocardium and epicardium is very
steep. This was sufficient to create a huge J wave including ST
elevation (red arrows in Fig.
3).
If the J wave in ERS is generated due to temporal
difference in the AP, a sufficient temporal delay of the AP should
exist between the endocardium and epicardium. Therefore, the degree
of temporal difference (conduction velocity difference in other
words) should be, at least the same as, or larger than, the length
of the J wave. When this concept was applied to the present
experiment, it may have been possible to induce a very small J wave
about 2.6 msec long. However, it was near impossible to induce
large J waves, as revealed in Fig.
3B, which was recognized just before the development of VT/VF
because there was not a sufficiently delayed phase 0 upstroke in
the transmembrane AP recording, in any of the preparations. The
delay was not enough to cause a steep transmural voltage gradient
required to generate a reentrant arrhythmia.
As aforementioned, epicardial heterogeneity serves
an important role in the occurrence of ventricular arrhythmias
(29,30). If a sufficient temporal difference in
the AP exists at the local epicardium sites, it may serve a role in
the formation of arrhythmia substrates. Typically, an epicardial
temporal difference in the AP increases the dispersion of the
conduction time (31). The
transmural conduction time, despite being very short, during which
the impulse propagated from the endocardial pacing site to each
epicardial site (two epicardial glass microelectrodes and five
epicardial unipolar electrodes), increased significantly in the
present experiments. However, dispersion of the transmural
conduction time did not exhibit a significant difference (Fig. 5). Thus, this finding indicated that
there was a homogeneous conduction delay.
Srinivasan et al (32) addresses that interventricular
dispersion of the repolarization generates a voltage gradient for
arrhythmias (33). However, we
hypothesize that this theory also has an insufficient probability
of being able to explain the creation of a steep transmural voltage
gradient (34,35).
The present study supports the concept that ECG
patterns of ERS and pVT can be reproduced by difference in the
local repolarization, without heterogeneous conduction delay.
However, the current results do not suggest that local
depolarization heterogeneity is not associated with the underlying
mechanism of ERS, because multiple factors (including autonomic
nerve tones) seemed to be involved in the development of ERS. A
whole-heart global conduction, such as between RVot and RVa, was
not demonstrated in the present study. Therefore, the role of
global depolarization heterogeneity cannot be excluded when
explaining the mechanism underlying ERS. The results of the present
study may be used as a basis to establish the appropriate
pharmacologic treatments for ERS. For example, several agents such
as phosphodiesterase III inhibitors and flavonoids are being
studied (36,37).
The wedge preparation model with a pharmacologically
induced ERS phenotype is representative of a denervated heart.
Thus, the model is in an autonomically denervated state. The canine
wedge preparation model cannot reflect the global physiology of the
whole heart. Notably, the use of whole heart Langendorff models
would overcome this limitation.
Polymorphic ventricular tachycardia was induced in
the canine wedge preparation ERS model without regional conduction
velocity heterogeneity. This suggests that local depolarization
heterogeneity would not greatly contribute to the generation of ERS
with no conduction delay. However, the role of global conduction
delay in ERS cannot be denied. Hence, demonstration of global
conduction delay of action potentials using a whole heart
Langendorff model or human heart is needed in further studies.
Acknowledgements
We are grateful to the late Professor Jae Ha Kim
(Medical School, Chonnam National University, Korea) for the
experimental support. We gratefully acknowledge Mr. John Martin
(Japan Lifeline Co., Ltd., Japan) for linguistic assistance with
the manuscript.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
NY was a major contributor in writing the manuscript
and contributed to the design, literature search, experimental
studies, data acquisition, data analysis, manuscript preparation,
manuscripts editing, manuscript review, approval of the final
version of the manuscript and agreed to all aspects of the work.
HKJ contributed to the literature search, experimental studies,
data analysis, statistical analysis, manuscripts editing,
manuscript review, approval of the final version of the manuscript
and agreed to all aspects of the work. KHL contributed to the
literature search, statistical analysis, manuscript review,
approval of the final version of the manuscript and agreed to all
aspects of the work. HWP contributed in the conception of the work,
manuscript review, approval of the final version of the manuscript
and agreed to all aspects of the work. JGC contributed in the
conception of the work, definition of intellectual content,
manuscripts editing, manuscript review, approval of the final
version of the manuscript and agreed to all aspects of the work.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
All experiments were performed in accordance with
the Guide for Care and Use of Laboratory Animals published by the
National Institutes of Health (38)
and all experiments were approved by the Animal Care and Use
Committee at Chonnam National University, Gwangju, Republic of
Korea (approval number, CNU IACUC-H-2017-33).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Wasserburger RH and Alt WJ: The normal
RS-T segment elevation variant. Am J Cardiol. 8:184–192.
1961.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mehta MC and Jain AC: Early repolarization
on scalar electrocardiogram. Am J MedSci. 309:305–311.
1995.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Gussak I and Antzelevitch C: Early
repolarization syndrome: Clinical characteristics and possible
cellular and ionic mechanisms. J Electrocardiol. 33:299–309.
2000.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Antzelevitch C and Yan GX: J wave
syndromes. Heart Rhythm. 7:549–558. 2010.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Haissaguerre M, Derval N, Sacher F, Jesel
L, Deisenhofer I, de Roy L, Pasquié JL, Nogami A, Babuty D,
Yli-Mayry S, et al: Sudden cardiac arrest associated with early
repolarization. N Engl J Med. 358:2016–2023. 2008.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nam GB, Kim YH and Antzelevitch C:
Augmentation of J waves and electrical storms in patients with
early repolarization. N Engl J Med. 358:2078–2079. 2008.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Nam GB, Ko KH, Kim J, Park KM, Rhee KS,
Choi KJ, Kim YH and Antzelevitch C: Mode of onset of ventricular
fibrillation in patients with early repolarization pattern vs.
brugada syndrome. Eur Heart J. 31:330–339. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Antzelevitch C: J wave syndromes:
Molecular and cellular mechanisms. J Electrocardiol. 46:510–518.
2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Koncz I, Gurabi Z, Patocskai B, Panama BK,
Szél T, Hu D, Barajas-Martínez H and Antzelevitch C: Mechanisms
underlying the development of the electrocardiographic and
arrhythmic manifestations of early repolarization syndrome. J Mol
Cell Cardiol. 68:20–28. 2014.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Hu D, Barajas-Martinez H, Terzic A, Park
S, Pfeiffer R, Burashnikov E, Wu Y, Borggrefe M, Veltmann C,
Schimpf R, et al: ABCC9 is a novel Brugada and early repolarization
syndrome susceptibility gene. Int J Cardiol. 171:431–442.
2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Burashnikov E, Pfeiffer R,
Barajas-Martinez H, Delpón E, Hu D, Desai M, Borggrefe M,
Häissaguerre M, Kanter R, Pollevick GD, et al: Mutations in the
cardiac L-type calcium channel associated with inherited J-wave
syndromes and sudden cardiac death. Heart Rhythm. 7:1872–1882.
2010.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Barajas-Martinez H, Hu D, Ferrer T, Onetti
CG, Wu Y, Burashnikov E, Boyle M, Surman T, Urrutia J, Veltmann C,
et al: Molecular genetic and functional association of brugada and
early repolarization syndromes with S422L missense mutation in
KCNJ8. Heart Rhythm. 9:548–555. 2012.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Di Diego JM and Antzelevitch C:
Inferolateral J-wave syndromes: A reflection of abnormal
repolarization, depolarization, or both? Heart Rhythm. 16:791–792.
2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Haissaguerre M, Nademanee K, Hocini M,
Cheniti G, Duchateau J, Frontera A, Sacher F, Derval N, Denis A,
Pambrun T, et al: Depolarization versus repolarization abnormality
underlying inferolateral J-wave syndromes: New concepts in sudden
cardiac death with apparently normal hearts. Heart Rhythm.
16:781–790. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Veerakul G and Nademanee K: Brugada
syndrome: Two decades of progress. Circ J. 76:2713–2722.
2012.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Fish JM, Welchons DR, Kim YS, Lee SH, Ho
WK and Antzelevitch C: Dimethyl lithospermate B, an extract of
danshen, suppresses arrhythmogenesis associated with the brugada
syndrome. Circulation. 113:1393–1400. 2006.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Di Diego JM, Sicouri S, Myles RC, Burton
FL, Smith GL and Antzelevitch C: Optical and electrical recordings
from isolated coronary-perfused ventricular wedge preparations. J
Mol Cell Cardiol. 54:53–64. 2013.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Watanabe H, Nogami A, Ohkubo K, Kawata H,
Hayashi Y, Ishikawa T, Makiyama T, Nagao S, Yagihara N, Takehara N,
et al: Electrocardiographic characteristics and SCN5A mutations in
idiopathic ventricular fibrillation associated with early
repolarization. Circ Arrhythm Electrophysiol. 4:874–881.
2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Mizumaki K, Nishida K, Iwamoto J, Nakatani
Y, Yamaguchi Y, Sakamoto T, Tsuneda T, Kataoka N and Inoue H: Vagal
activity modulates spontaneous augmentation of J-wave elevation in
patients with idiopathic ventricular fibrillation. Heart Rhythm.
9:249–255. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wilhelm M, Brem MH, Rost C, Klinghammer L,
Hennig FF, Daniel WG and Flachskampf F: Early repolarization, left
ventricular diastolic function, and left atrial size in
professional soccer players. Am J Cardiol. 106:569–574.
2010.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Marcus RR, Kalisetti D, Raxwal V, Kiratli
BJ, Myers J, Perkash I and Froelicher VF: Early repolarization in
patients with spinal cord injury: Prevalence and clinical
significance. J Spinal CordMed. 25:33–38. 2002.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Koutbi L, Roussel M, Haissaguerre M and
Deharo JC: Hyperpnea test triggering malignant ventricular
arrhythmia in a child with early repolarization. Heart Rhythm.
9:1153–1156. 2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Kawata H, Noda T, Yamada Y, Okamura H,
Satomi K, Aiba T, Takaki H, Aihara N, Isobe M, Kamakura S and
Shimizu W: Effect of sodium-channel blockade on early
repolarization in inferior/lateral leads in patients with
idiopathic ventricular fibrillation and brugada syndrome. Heart
Rhythm. 9:77–83. 2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kasanuki H, Ohnishi S, Ohtuka M, Matsuda
N, Nirei T, Isogai R, Shoda M, Toyoshima Y and Hosoda S: Idiopathic
ventricular fibrillation induced with vagal activity in patients
without obvious heart disease. Circulation. 95:2277–2285.
1997.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Meregalli PG, Wilde AA and Tan HL:
Pathophysiological mechanisms of brugada syndrome: Depolarization
disorder, repolarization disorder, or more? Cardiovasc Res.
67:367–378. 2005.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Wilde AA, Postema PG, Di Diego JM, Viskin
S, Morita H, Fish JM and Antzelevitch C: The pathophysiological
mechanism underlying brugada syndrome: Depolarization versus
repolarization. J Mol Cell Cardiol. 49:543–553. 2010.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Di Diego JM, Argenziano M, Chen K, Tabler
M and Antzelevitch C: In a whole-heart model of the brugada
syndrome, delayed conduction in the RVOT ‘does not’ contribute to
inscription of the electrocardiographic J wave/ST segment
elevation. Heart Rhythm. 15(242)2018.
|
|
28
|
Yoon N, Hong SN, Cho JG, Jeong HK, Lee KH
and Park HW: Experimental verification of the value of the
Tpeak-Tend interval in ventricular arrhythmia
inducibility in an early repolarization syndrome model. J
Cardiovasc Electrophysiol. 30:2098–2105. 2019.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Antzelevitch C, Yan GX and Shimizu W:
Transmural dispersion of repolarization and arrhythmogenicity: The
brugada syndrome versus the long QT syndrome. J Electrocardiol.
32:158–165. 1999.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Maoz A, Christini DJ and Krogh-Madsen T:
Dependence of phase-2 reentry and repolarization dispersion on
epicardial and transmural ionic heterogeneity: A simulation study.
Europace. 16:458–465. 2014.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sims JJ, Miller AW and Ujhelyi MR:
Electrical heterogeneity and arrhythmogenesis: Importance of
conduction velocity dispersion. J Cardiovasc Pharmacol. 41:795–803.
2003.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Srinivasan NT, Orini M, Providencia R,
Simon R, Lowe M, Segal OR, Chow AW, Schilling RJ, Hunter RJ,
Taggart P and Lambiase PD: Differences in the upslope of the
precordial body surface ECG T wave reflect right to left dispersion
of repolarization in the intact human heart. Heart Rhythm.
16:943–951. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Malik M, Huikuri HV, Lombardi F, Schmidt
G, Verrier RL and Zabel M: e-Rhythm Group of EHRA. Is the
Tpeak-Tend interval as a measure of
repolarization heterogeneity dead or just seriously wounded? Heart
Rhythm. 16:952–953. 2019.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Antzelevitch C and Di Diego JM: Reply to
the editor-Tpeak-Tend is alive and well.
Heart Rhythm. 16:e49–e50. 2019.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Antzelevitch C and Di Diego JM:
Tpeak-Tend interval as a marker of arrhythmic
risk. Heart Rhythm. 16:954–955. 2019.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Patocskai B, Barajas-Martinez H, Hu D,
Gurabi Z, Koncz I and Antzelevitch C: Cellular and ionic mechanisms
underlying the effects of cilostazol, milrinone, and isoproterenol
to suppress arrhythmogenesis in an experimental model of early
repolarization syndrome. Heart Rhythm. 13:1326–1334.
2016.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Yoon N, Hong SN, Lee KH, Park HW and Cho
JG: Antiarrhythmic effect of artemisinin in brugada syndrome model.
Europace. 20(i138)2018.
|
|
38
|
Clark JD, Gebhart GF, Gonder JC, Keeling
ME and Kohn DF: Special report: The 1996 guide for the care and use
of laboratory animals. ILAR J. 38:41–48. 1997.PubMed/NCBI View Article : Google Scholar
|