Introduction
Dentigerous cyst is a type of odontogenic cyst and
accounts for 20-24% of all jaw cysts (1). There are two types of dentigerous
cysts: one of developmental origin, associated with impacted teeth
(2) and the other one, of
inflammatory origin, associated with non-vital primary teeth
(3,4). Inflammatory dentigerous cysts are only
found in the mixed dentition and they generally involve mandibular
premolars (3,5).
A dentigerous cyst encloses the crown of an
unerupted tooth by expansion of its follicle and is attached to the
tooth along the cervical region (6). Dentigerous cysts are often
asymptomatic and they are usually detected during routine
radiographic examination, X-rays taken for orthodontic reasons or
in order to find the reason for delayed eruption (2,7,8). In
the radiographic examination, dentigerous cyst lesion shows a
well-demarcated unilocular radiolucency with a sclerotic border,
surrounding the crown of an unerupted tooth (3,9).
The cyst may cause swelling, tooth displacement,
tooth mobility and sensitivity if it reaches a size larger than 2
cm in diameter (7).
Odontogenic keratocyst, unicystic ameloblastoma,
central giant cell granuloma and a large radicular cyst must be
considered in the differential diagnosis of a dentigerous cyst.
Radiograph alone cannot differentiate the above-mentioned lesions,
thus a histopathological examination can help accurate diagnosis
(1,3).
Histologically, dentigerous cysts consist of a
fibrous wall containing variable amounts of myxoid tissue and
odontogenic remnants. The cyst is lined with nonkeratinized
stratified squamous epithelium consisting of muco-sebaceous,
ciliated and, rarely, sebaceous cells. The epithelial-connective
tissue interface is typically flattened, but becomes highly
irregular when associated with inflammation (10). Pseudoepitheliomatous hyperplasia
with thicker epithelium and acute and chronic inflammatory
infiltrate are frequently found (8).
Extraction of non-vital primary teeth and
marsupialization represent the best strategy to conserve teeth
affected by a dentigerous cyst and to permit their eruption,
especially in young patients (1,3,5). When
unerupted third molars are involved, coronectomy (intentional
partial odontectomy) can be a solution (11,12).
There are currently more published reports on odontogenic cysts
found in adults than in pediatric patients (4).
This report presents two clinical cases of children
with dentigerous cysts of inflammatory origin. The two cases were
managed differently due to the associated medical condition of one
of the patients who had autism, which limited patient cooperation
under common dental office circumstances.
Case reports
Case 1
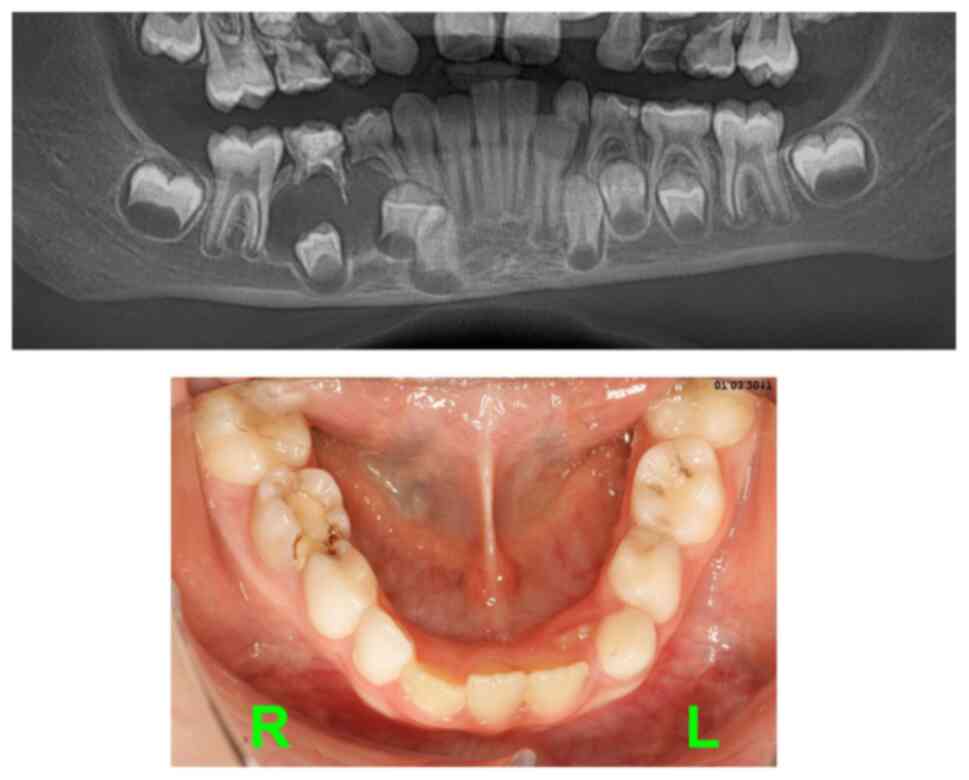
A boy aged 7 years 11 months was referred by a
fellow surgeon for a second opinion for the treatment of an
odontogenic cyst on the right side of the mandible (Fig. 1). General examination and anamnesis
confirmed that the patient was healthy, with no significant medical
history. Clinical intraoral examination revealed a right lower
first permanent molar (46) with untreated caries, while the second
primary molar in the same quadrant (85) was mobile, with a large
composite restoration. According to anamnesis, 85 had been treated
endodontically a few months before. Radiographic examination showed
a large unilocular radiolucent area surrounding the crown of the
mandibular second premolar (45). The roots of the non-vital second
primary molar exhibited accelerated resorption and appeared to
project into the lumen of the cystic cavity.
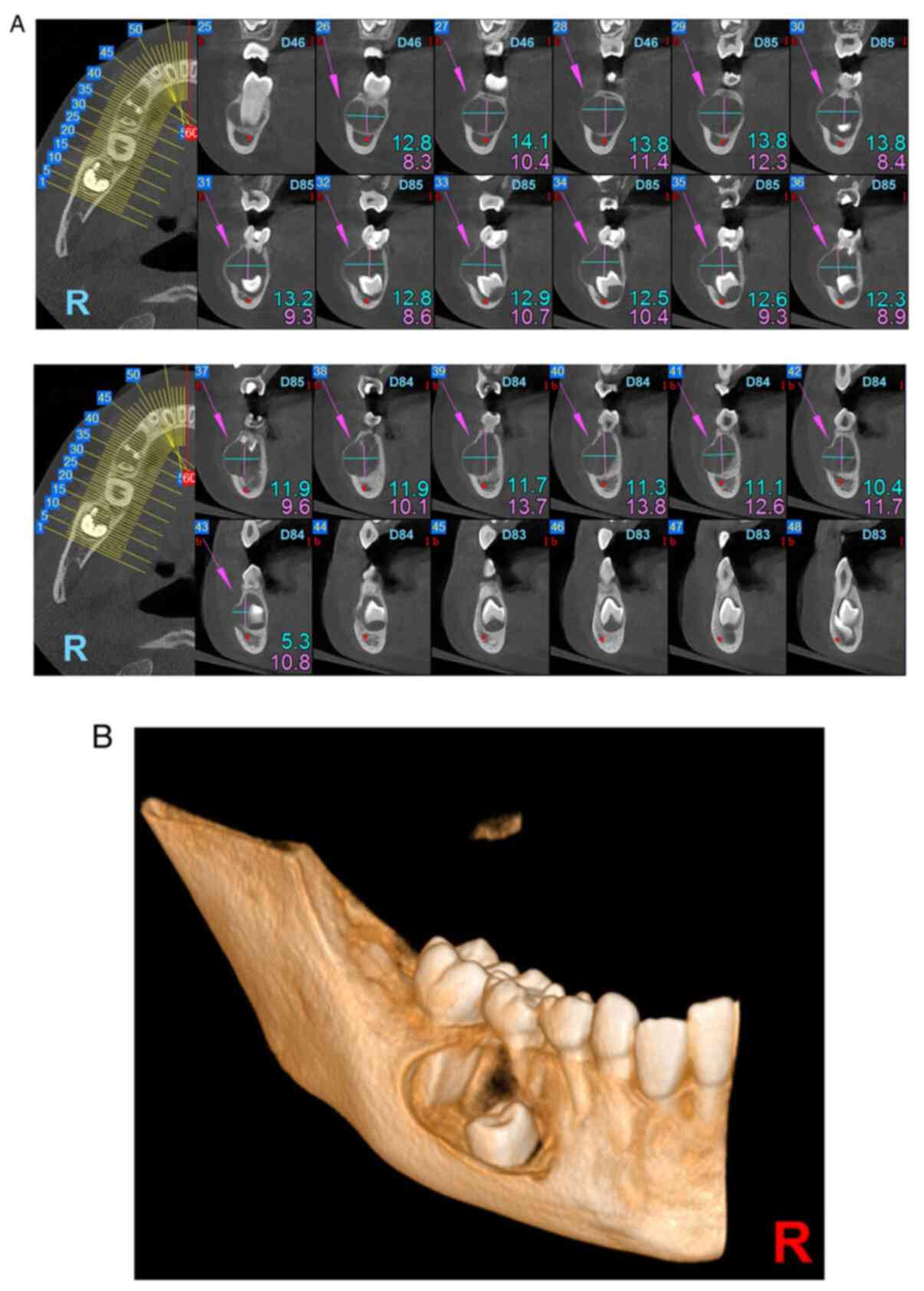
The computed tomography (CT) examination previously
recommended by the referring colleague (Fig. 2A and B) revealed a large cystic cavity (14x12
mm), enclosing the crown of unerupted 45 and displacing medially
the crown of unerupted 44. The second premolar was shifted to the
lower edge of the mandible.
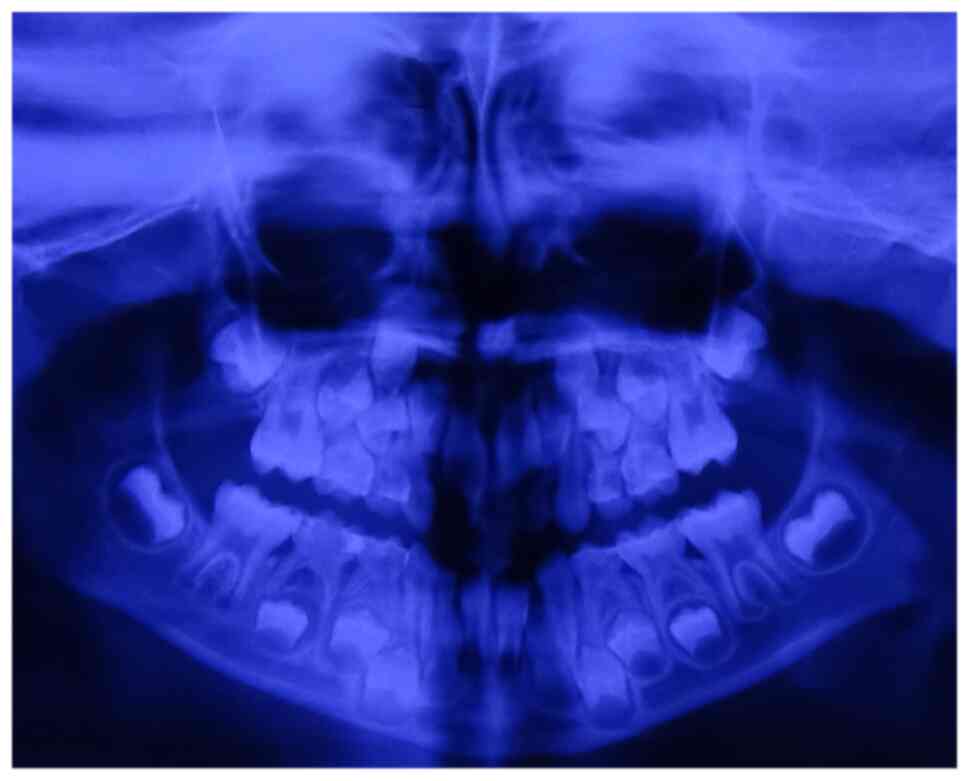
A previous panoramic X-ray, taken 14 months before
referral (Fig. 3), showed deep
untreated caries on both lower primary molars on the right
side.
Treatment
As a first step, an alginate impression of the lower
arch was taken. Teeth 84 and 85 were removed from the cast and a
removable lower appliance was custom-made, with a space maintainer
corresponding to the removed primary molars. Extractions were
scheduled to be performed under inhalation sedation due to the high
level of dental anxiety of the child (initial level 2 of
cooperation on Frankl scale).
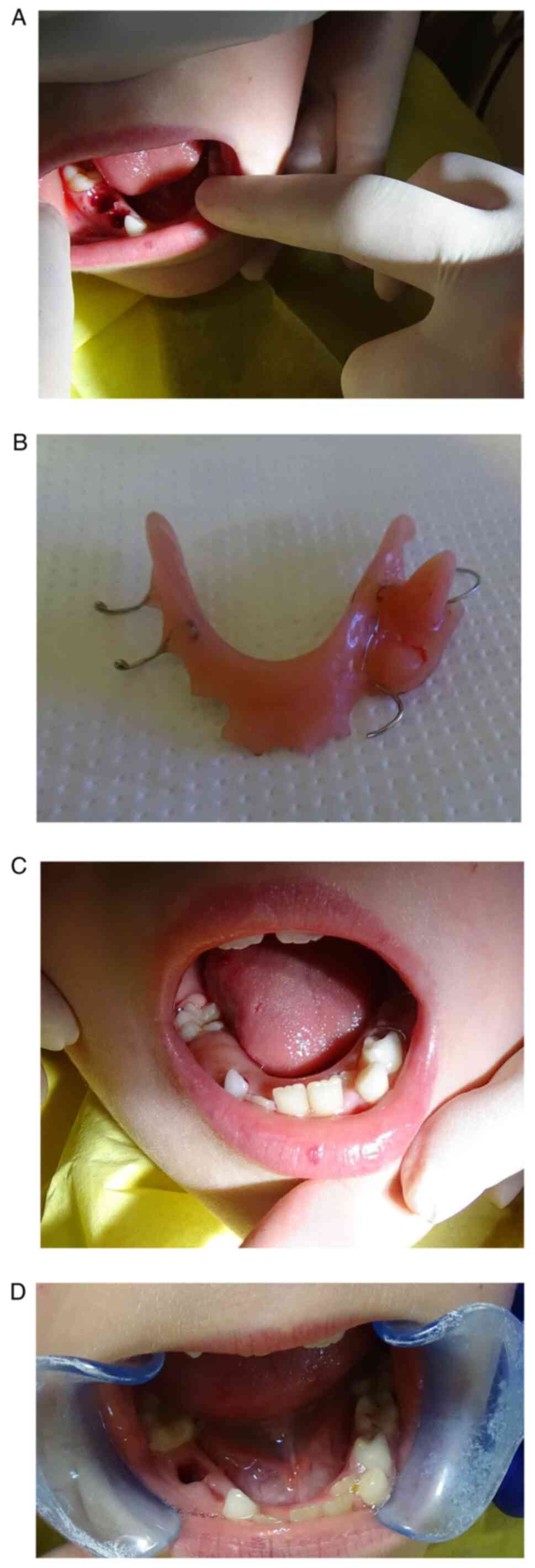
Extraction of both primary molars on the right side
and marsupialization of the cyst were performed under nitrous
sedation and local infiltration anesthesia. The removable appliance
was adapted on site, with an acrylic piece fitted into the socket
(Fig. 4A-D).
Parents were instructed to daily irrigate the
operative site with saline after the extraction for the next week.
Patient was instructed to wear the appliance at all times and was
recalled after 7 days and then every 2 weeks.
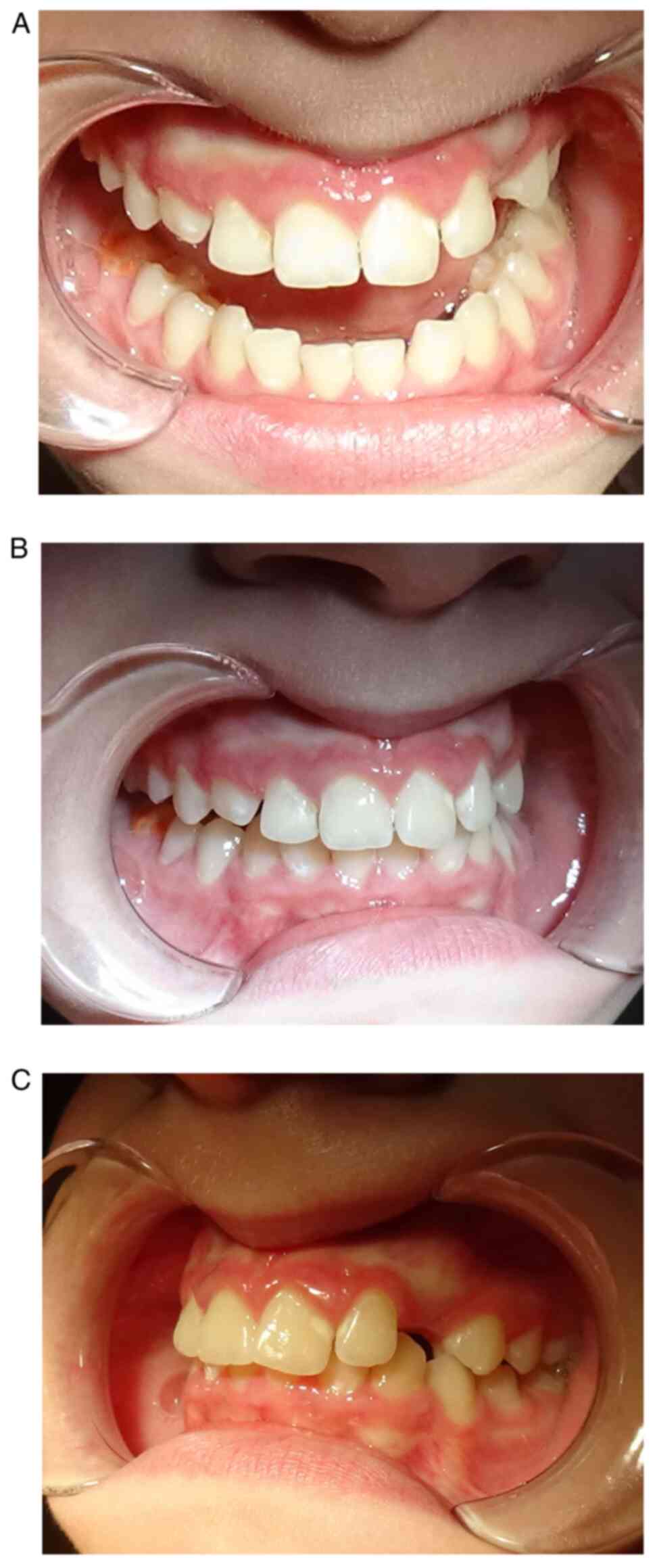
Follow-up
The in-socket piece was progressively reduced as the
cystic cavity was shrinking. After 2 months, 44 regained its upward
position and 45 moved towards correct eruption (Fig. 5A and B).
Orthodontic treatment with removable appliances was
then initiated due to crowding. Twenty months after surgery, both
premolars on the right side were sound and correctly erupted, while
on the left side of the mandible deciduous molars were still in
place. The right lower first permanent molar remained unaffected
despite its proximity to the cyst (Figs. 6 and 7).
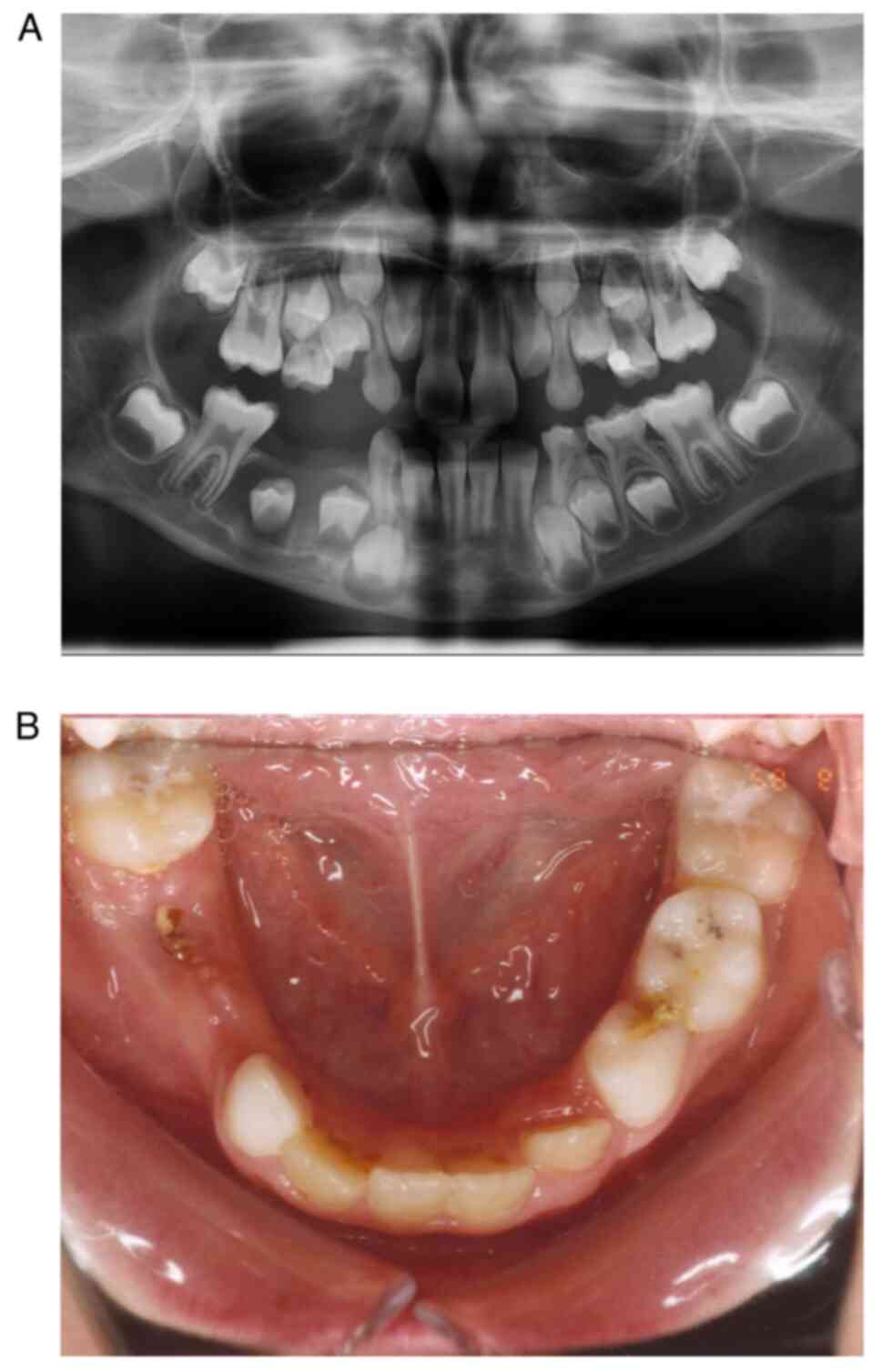
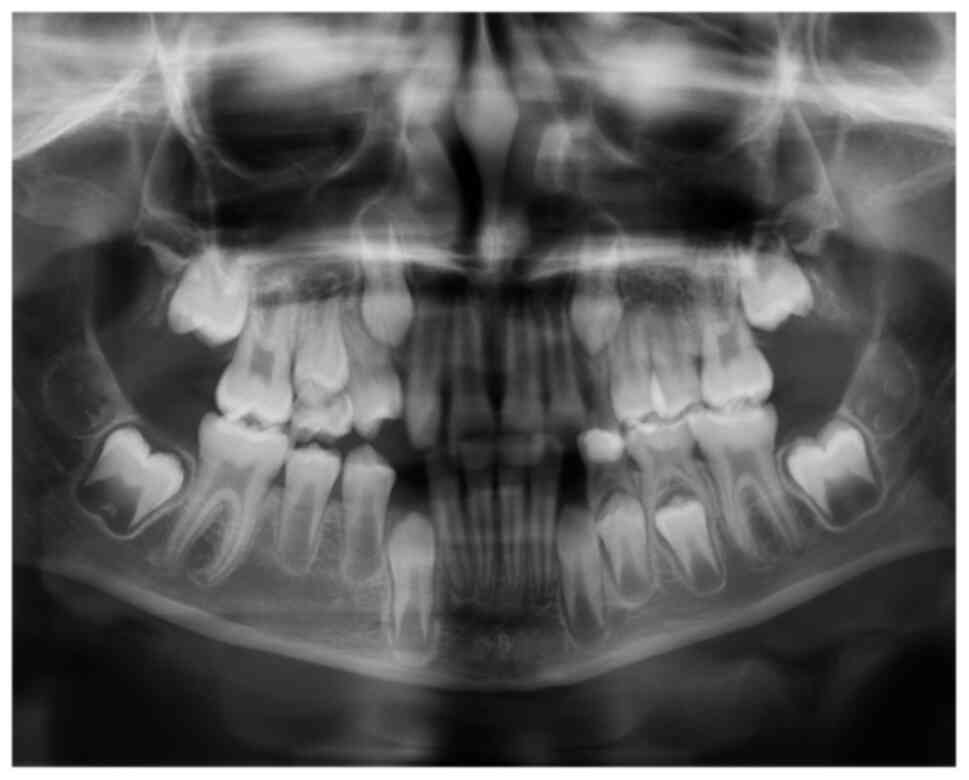
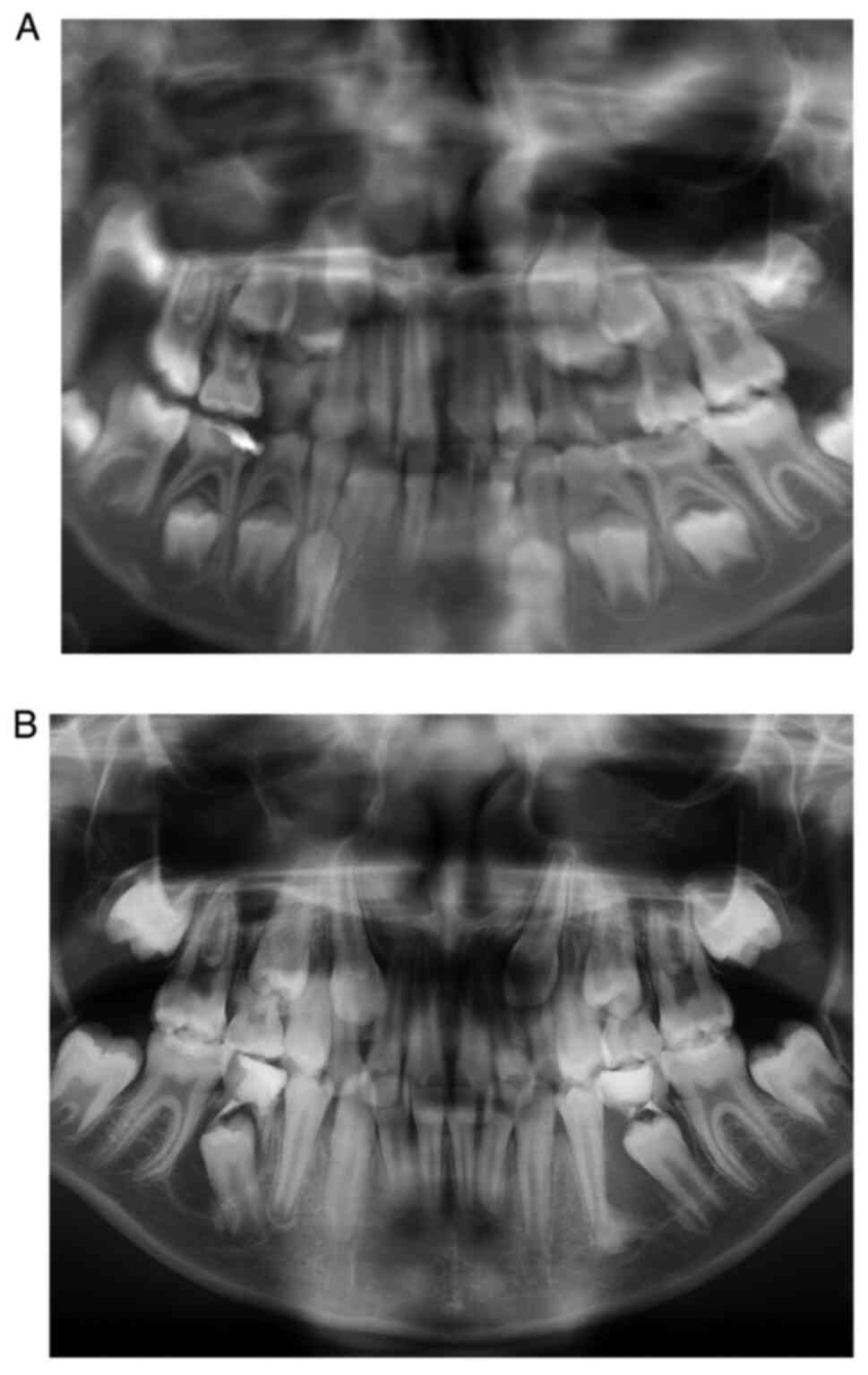
Case 2
In January 2018, bilateral inflammatory follicular
cysts were diagnosed during a routine dental check-up in an
autistic girl aged 10 years 9 months, treated and followed in our
clinic. The vestibular bone plate was slightly deformed. The
patient did not exhibit any manifestations that might have
suggested pain and there were no clinical signs of inflammation
around the lesion. Panoramic X-ray showed bilateral large
dentigerous cysts enclosing the crowns of the lower second
premolars on both sides (Fig. 8B).
No other investigations were performed. According to the dental
records of the child, endodontic treatment on 75 and 85 had been
performed under general anesthesia 33 months before, due to
extensive caries (Figs. 8A and
9A and B).
Treatment
Teeth 75 and 85 (together with other 4 primary
teeth: 53, 55, 63 and 65) were extracted under general anesthesia
(Fig. 10), leaving large bone
defects. Given the developmental stage of the lower second
premolars, an appliance with an in-socket piece was not considered
necessary. Despite some estimated risk for mesial tilting of the
lower first permanent molars, the patients' general pathology ruled
out space maintainers as well.
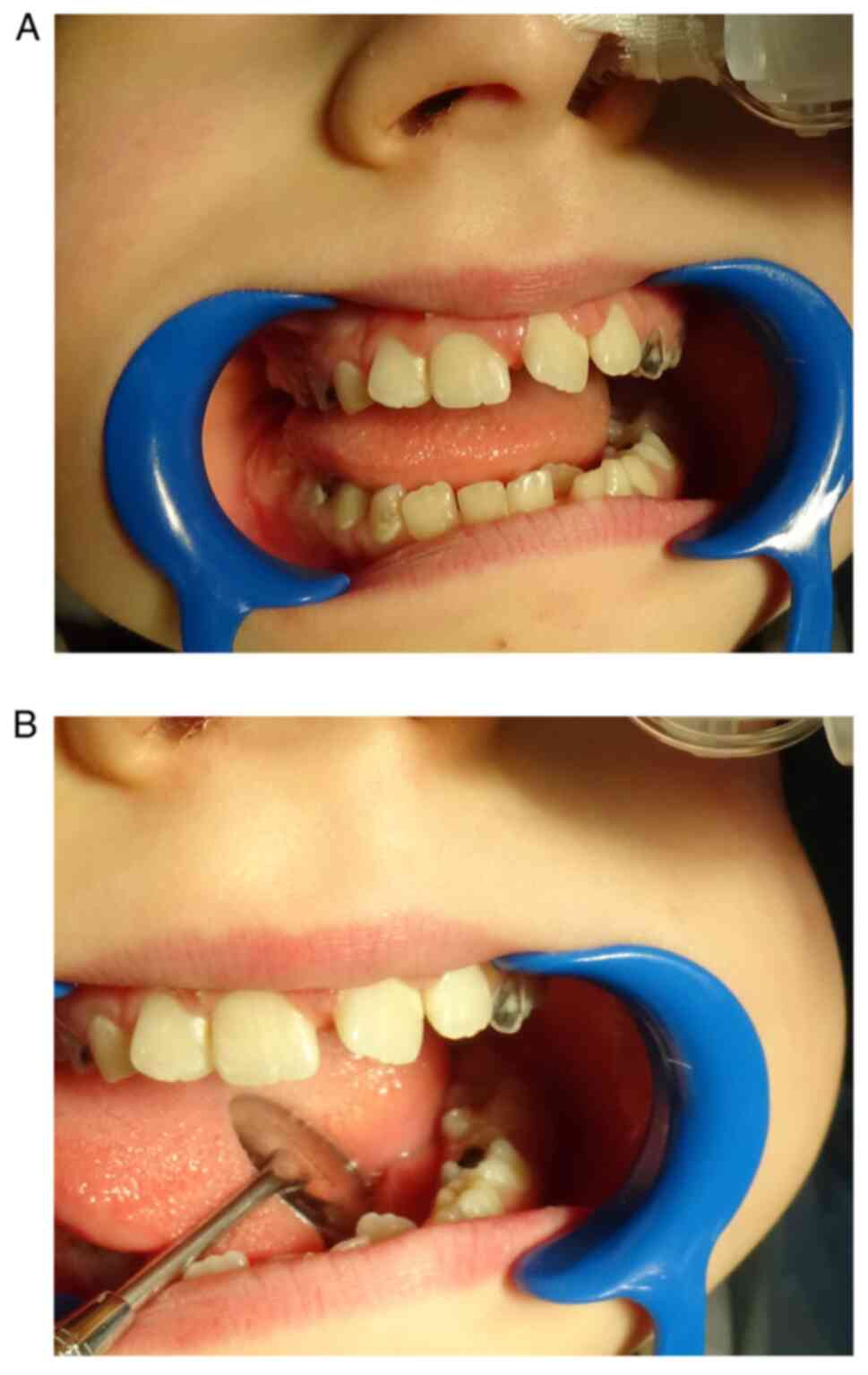
Follow-up
Clinical evolution was good. Thirteen months after
extraction, lower second premolars were fully erupted and sound,
while 36 and 46 remained in fairly good position (Fig. 11A-C). No further X-rays were taken
due to difficulties in obtaining the patient's cooperation, as well
as to questionable objective reasons to insist.
Discussion
Inflammatory follicular cysts occur most frequently
in the premolar region, after primary molars affected by deep
caries become non-vital. Inflammatory follicular cysts occur more
frequently in boys than girls and are 10 times more likely to occur
in the lower jaw than in the upper (3).
The pathogenesis of dentigerous cysts is still
controversial. Benn and Altini (13) proposed three possible mechanisms for
cyst histogenesis. The first hypothesis suggests that the
developmental dentigerous cyst might form from a dental follicle,
secondarily inflamed from a non-vital tooth as a source of
inflammation. The second proposed explanation would be the
formation of a radicular cyst at the apex of a non-vital deciduous
tooth, followed by eruption of its permanent successor into the
radicular cyst, thus resulting in a dentigerous cyst of
extrafollicular origin. They also suggested that the follicle of a
permanent successor might get secondarily infected from other
sources than the non-vital deciduous predecessor, leading to a
dentigerous cyst formation. Available evidence in both our cases
indicated that infection of the predecessors (second primary
molars) could have been the source of inflammation of the
dentigerous cysts.
Pulp treatment cannot prevent the development of
these cysts as they have been noted to occur both after pulp
treatment and in the absence of it (3). In our cases, inflammatory dentigerous
cysts occurred in primary molars with endodontic treatment.
Modern imaging [such as cone-beam computed
tomography (CBCT)] can provide useful information for the
diagnostic and clinical management of dentigerous cysts, especially
for large ones, with displacement of adjacent teeth (7). In our first clinical case, the CT
investigation recommended by the referring colleague was very
helpful for quick diagnostic and efficient decision-taking.
However, careful evaluation of the benefits and need for such
investigations compared with the potential risks of exposure to
ionizing radiation is extremely important in pediatric patients.
The European Academy of Paediatric Dentistry's guidelines for
prescribing radiographs in children and adolescents clearly point
out that CBCT examination can be justified only when it results in
a substantial net gain of information which directly influences the
decision-making (14). Besides the
age of the patient and the expected diagnostic benefits, the
child's capacity to cooperate for complex imaging (needing a longer
acquisition time) is also to be taken into account when indicating
such investigations, especially when general conditions (e.g.,
intellectual challenge) are present (14).
Both of our clinical cases provide information on
the growth rate of inflammatory dentigerous cysts: In the first
case, the cyst reached a diameter of 1.4 cm in 14 months, while in
the second case cysts with diameters >1 cm developed over a
period of ~3 years. Shear (6)
reported radiological findings showing that dentigerous cysts of
4-5 cm in diameter may develop in 3-4 years. Early recognition of
dentigerous cysts, often as incidental findings, and prompt
treatment limit the extent of jaw bone destruction (4). Uneventful healing with spontaneous
gradual filling of the residual cavities, without any graft
material, can be obtained even in large cysts after
marsupialization if the cavity is sufficiently surrounded by bony
walls (15).
Although rarely, untreated dentigerous cysts may
sometimes develop into an odontogenic tumor or a malignancy such as
squamous cell carcinoma (1).
Therefore, early diagnosis and treatment of a dentigerous cyst
lesion is important for the prevention of development into more
destructive lesions.
It is generally accepted that extraction of a
non-vital primary tooth and marsupialization will allow rapid
healing of the lesion and eruption of the permanent tooth, provided
that these procedures are performed at the normal time of eruption
(3). However, opinions that the
treatment plan for dentigerous cysts should consider extraction of
the involved permanent tooth are not completely ruled out. In this
respect, removal of the associated permanent tooth along with cyst
enucleation may be necessary if it shows arrested development, is
severely displaced or if the lesion is extensive (3,5).
By extracting the infected primary teeth,
marsupialization of the cyst and ensuring continuous drainage, it
is possible to achieve spontaneous eruption of the involved
permanent teeth even if they are badly dislocated. Healing and
ossification of the bony defect can take place simultaneously with
the eruption of the permanent teeth. The reparatory process is
completed in one to two years, depending on the dimensions of the
bone defect (15).
In our first case, drainage was maintained with a
custom-made removable appliance (modified Howley plate), which also
played the role of a space maintainer, prevented food impaction and
allowed access for regular cleansing. The same method has been
successfully used in previous reports (16).
No evidence of recurrence was noted on follow-up
radiography after marsupialization. These results are consistent
with previous studies, which have shown that recurrence is rare
after total lesion removal or when the involved tooth erupts after
marsupialization (1,15-17).
In conclusion, conservative treatment of large
inflammatory dentigerous cysts in young patients provides good
results with minimal invasion, ensures preservation and physiologic
development of teeth and proper bone healing. Modern imaging can
substantially help diagnostic and clinical decisions, but
indications for high radiation investigations must be carefully
evaluated. Patients must be followed-up until full eruption of the
displaced permanent teeth and bony consolidation of the cyst.
Acknowledgements
Not applicable.
Funding
Funding: This study was supported by Erasmus+ Project
2019-1-RO01-KA202-063820-OSCAR (Oscar Special Care Academic
Resources).
Availability of data and materials
All patient data mentioned in the article are
available from the corresponding author on reasonable request.
Authors' contributions
AV and AB provided clinical management of the
patients. AV, AM and AD contributed in all the stages of the
article preparation, from literature research to revising the
manuscript for important intellectual content. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written consent for the publication of the images
was obtained from the patients' parents before paper
submission.
Competing interests
The authors declare that they have no competing
interests.
Authors' information
Arina Vinereanu: https://orcid.org/0000-0001-9745-1315.
References
|
1
|
Kirtaniya BC, Sachdev V, Singla A and
Sharma AK: Marsupialization: A conservative approach for treating
dentigerous cyst in children in the mixed dentition. J Indian Soc
Pedod Prev Dent. 28:203–208. 2010.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Sindi AM: Bilateral mandibular dentigerous
cysts presenting as an incidental finding: A case report. Am J Case
Rep. 20:1148–1151. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Koželj V and Sotošek B: Inflammatory
dentigerous cysts of children treated by tooth extraction and
decompression-report of four cases. Br Dent J. 187:587–590.
1999.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Rajendra Santosh AB: Odontogenic cysts.
Dent Clin North Am. 64:105–119. 2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Shetty RM and Dixit U: Dentigerous cyst of
inflammatory origin. Int Clin J Pediatr Dent. 3:195–198.
2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Shear M: Cysts of the oral regions. 3rd
edition. Blackwell Munksgaard Publishers, Oxford Wright, pp75-89,
1992.
|
|
7
|
Bodner L, Woldenberg Y and Bar-Ziv J:
Radiographic features of large cysts lesion of jaws in children.
Pediatr Radiol. 33:3–6. 2003.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Huang G, Moore L, Logan RM and Gue S:
Histological analysis of 41 dentigerous cysts in a paediatric
population. J Oral Pathol Med. 48:74–78. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ziccardi VB, Eggleston TI and Schnider RE:
Using fenestration technique to treat a large dentigerous cyst. J
Am Dent Assoc. 128:201–205. 1997.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Tüzüm MS: Marsupialization of a cyst
lesion to allow tooth eruption: A case report. Quintessence Int.
28:283–284. 1997.PubMed/NCBI
|
|
11
|
Henien M, Sproat C, Kwok J, Beneng K and
Patel V: Coronectomy and dentigerous cysts: A review of 68
patients. Oral Surg Oral Med Oral Pathol Oral Radiol. 123:670–674.
2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Patel V, Sproat C, Samani M, Kwok J and
McGurk M: Unerupted teeth associated with dentigerous cysts and
treated with coronectomy: Mini case series. Br J Oral Maxillofac
Surg. 51:644–649. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Benn A and Altini M: Dentigerous cysts of
inflammatory origin. A clinicopathologic study. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod. 81:203–209. 1996.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kühnisch J, Anttonen V, Duggal MS,
Spyridonos ML, Rajasekharan S, Sobczak M, Stratigaki E, Van Acker
JWG, Aps JKM, Horner K and Tsiklakis K: Best clinical practice
guidance for prescribing dental radiographs in children and
adolescents: An EAPD policy document. Eur Arch Paediatr Dent.
21:375–386. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Chacko R, Kumar S, Paul A and Arvind
: Spontaneous bone regeneration after enucleation of large
jaw cysts: A digital radiographic analysis of 44 consecutive cases.
J Clin Diagn Res. 9:ZC84–ZC89. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Nohra J, Kassir AR, Akel H and Dagher M:
Treatment of dentigerous cysts with a modified Hawley plate in
children: Report of two cases with radiographic results. Br J Oral
Maxillofac Surg. 58:102–104. 2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Koca H, Esin A and Aycan K: Outcome of
dentigerous cysts treated with marsupialization. J Clin Pediatr
Dent. 34:165–168. 2009.PubMed/NCBI View Article : Google Scholar
|