Introduction
Cardiovascular disease (CVD), which is the leading
cause of death in China (1),
accounted for ~40% of deaths in the Chinese population in
2017(2). Atherosclerotic CVD
(ASCVD), which includes ischemic heart disease and ischemic stroke,
is the main form of CVD (2). In
2016, there were ~2.4 million deaths from ASCVD in China, which
accounted for 61% of all deaths from CVD (2,3). A
monitored atherosclerosis regression study revealed that
quantitative coronary angiographic changes were associated with
cardiovascular events, and optimization of therapies was required
to promote the regression of atherosclerosis (4).
Atherosclerosis is characterized by lipoprotein
retention, foam cell recruitment, vascular smooth muscle cell
proliferation and matrix synthesis (5). The lumen may be occluded when the
plaque is large or prone to rupture and cause thrombosis (5). As ASCVD is a huge health burden,
therapies aiming to reduce the size of atherosclerotic plaque and
open the luminal stenosis have become a popular research focus
(6). Lipid-lowering diets and the
administration of lipid-lowering agents such as statins, have been
revealed to be effective in regressing atherosclerotic plaque
(7). Of these, the lipid-lowering
diet has been the most common non-interventional treatment for
atherosclerosis (8). A number of
trials assessing atherosclerosis do not evaluate diet as an
independent intervention but rather combine it with other lifestyle
changes, such as exercise or quitting smoking (9); this highlights the complex,
multifactorial nature of the influence of lifestyle on
atherosclerosis. Therefore, it is important to clarify the effects
of dietary intervention on atherosclerosis.
A number of studies have demonstrated that switching
from a high-fat or cholesterol-rich diet to a cholesterol-low diet
reduced the plasma lipid levels and caused the regression of
atherosclerotic plaque in rabbits (10-13),
squirrel monkeys (14), rhesus
monkeys (15) and swine (16). However, a previous study using the
rabbit model reported that removing high cholesterol from the diet
did not lead to regression but rather aggravated advanced
atherosclerosis (17). This reason
for this paradoxical response of rabbit arteries to the high
cholesterol withdrawal treatment has not been fully determined, and
is likely due to an inhibiting factor in the reversal of the
atheromatous plaque. The effects of the lipid lowering diet on
plaque requires further elucidation in animal studies.
The stability of plaque serves an essential role in
acute coronary events and mortality (18). In nonhuman primates, the advanced
arterial lesions in cholesterol-fed Rhesus monkeys underwent
remodeling during a subsequent regression period of 40 months when
the animals were switched to low-cholesterol diets (15,19).
In atherosclerotic rabbits with aortic balloon injury, dietary
lipid lowering promoted the stability of plaque via the maturation
of smooth muscle cells (10),
increased collagen content (20)
and reduced endothelial activation (21). Collagen is the main structural
protein of the fibrous cap, and its cross-linking provides
mechanical strength to atherosclerotic lesions and determines the
biomechanical stability of plaque (22). This supports the fact that collagen
cross-linking serves an important role in determining the effect of
a lipid-lowering diet on the stability of plaque. As the
lipoprotein metabolism of rabbits is closer to that of humans than
that of rodents, rabbits fed a simple high cholesterol diet have
become the most popular animal model for the study of
atherosclerosis (23,24). Therefore, the present study
investigated the independent effect of diet intervention on
atherosclerotic plaque and the cross-linking of collagen in
cholesterol-fed rabbits.
Materials and methods
Animal protocol
All animal protocols were approved by the
Institutional Animal Care and Use Committee (IACUC) of the West
China Hospital of Sichuan University. Male New Zealand White
rabbits (n=43; age, 10 weeks) weighing ~2.0 kg were obtained from
Chengdu Dossy Experimental Animals Co., Ltd. The rabbits were
acclimated to the laboratory condition for one week and housed
individually in metal cages in rooms maintained with a 12 h
light/dark cycle, a constant temperature of 22±2°C and
humidity at 50±5%. All animals had access to water at all times and
were fed ad libitum with a regular chow diet or a high-fat
chew diet (100-120 g/day).
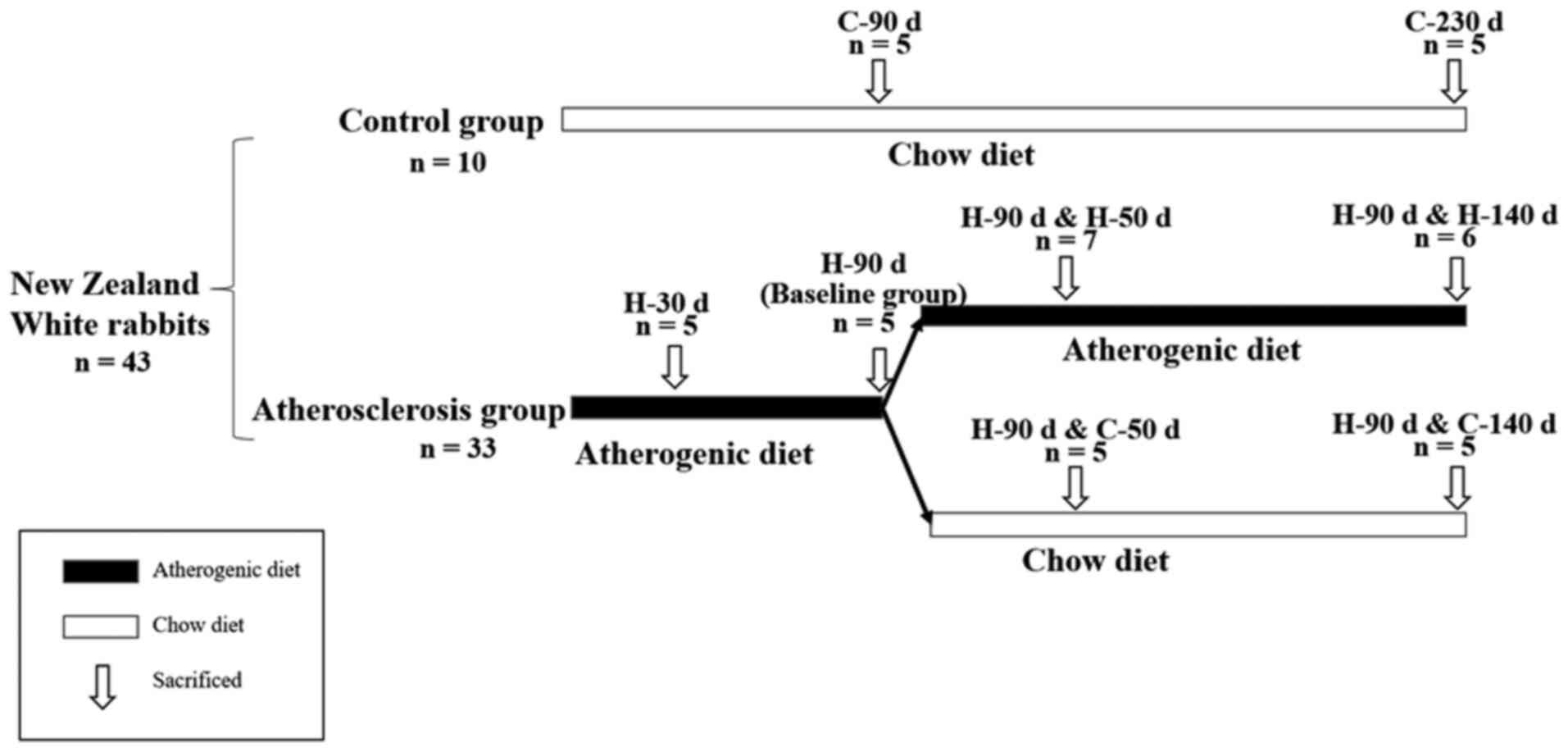
Atherosclerosis was induced using a high cholesterol
diet (HCD) containing 1% (w/w) cholesterol (cat. no.
5915010104; Gen-View Scientific, Inc.). Cholesterol crystals were
dissolved in peroxide-free diethylether, mixed with the chow and
allowed to dry. The atherogenic, high cholesterol diet was given to
rabbits for 30 (H-30 d) or 90 days (H-90 d) to determine whether
plaque formed. A total of five rabbits were euthanized at 30 days
and five rabbits were euthanized at 90 days, and these rabbits
comprised the baseline group. A total of 13 animals continued to
consume the atherogenic diet for 50 (H-90 d & H-50 d; n=7) or
140 more days (H-90 d & H-140 d, n=6). The remaining animals
consumed a chow diet with no added cholesterol for 50 days (H-90 d
& C-50 d; n=5) or 140 days (H-90 d & C-140 d; n=5).
Age-matched rabbits in the control groups were fed a chow diet for
90, and 230 days, respectively. Each control group contained 5
rabbits. The experimental protocol is presented in Fig. 1.
Blood sampling and cholesterol
measurement
Fasting blood was collected weekly via the
left/right marginal ear vein and at the time of harvest after
termination of the experiments in each group. The blood volume was
~1 ml for each rabbit. Blood was centrifuged at 1,123 x g for 15
min at 4˚C. Following centrifugation, ~500 ml plasma could be
obtained from each tube. Plasma samples were stored at -80˚C prior
to analysis. The plasma lipid profiles were determined by the
methods described as follows: Plasma total cholesterol (TC) by
cholesterol oxidase peroxidase (CHOD-POD) method, high-density
lipoprotein cholesterol (HDL-C) and low-density lipoprotein
cholesterol (LDL-C) by the precipitation end point method,
triglycerides (TG) by glycerol-phosphoric acid oxidase peroxidase
(GPO-POD) method using a TC kit (lot no. 141615025), HDL-C kit (lot
no. 142117009), LDL-C kit (lot no. 142016009), and TG kit (lot no.
141716001), respectively (Shenzhen Mindray Bio-Medical Electronics
Co., Ltd.) (25). Each parameter
for each sample was assessed in duplicate. All assays were followed
according to the manufactures' protocol and were analyzed using an
automatic chemistry analyzer (BS-120, Mindray).
Tissue preparation
Following termination of the experiments, the
rabbits were anaesthetized using sodium pentobarbital (30 mg/kg
intravenously; Rhone Merieux, Ltd.) and placed in the supine
position (26,27). The perfusion process and collection
of aortas was performed as previously described (6). An inguinal incision was made to access
the aorta for the insertion of a cannula connected to a perfusion
apparatus. The rabbits were then perfused with isotonic saline from
the left ventricle using a 50 ml syringe needle (at a rate of 100
ml/minute/kg body weight). When the run-off liquid was clear, the
aortas were isolated and cleaned of muscle, adherent fat and
fascia. Finally, the abdominal aorta was cut into three segments
for further analysis. The first segment, which was taken from the
coeliac axis to the left renal artery, was longitudinally opened
along the ventral midline for oil-red O staining to evaluate the
gross atherosclerotic lesion area. The second segment, which was
taken from the 3rd up to the 4th lumbar artery branch point, was
embedded in optimal cutting temperature medium and serially
sectioned at 5-µm thickness for histopathologic examination or
elastic van Gieson (EVG) staining. The remaining arterial tree was
immediately frozen in liquid nitrogen and stored at
-80°C for later use.
Quantification of the atherosclerotic
lesions
Oil-red O staining was used to quantify the en
face atherosclerotic lesion area (6,28). The
first segment of the aorta was fixed with 4% paraformaldehyde for
10 min at 37°C, stained with oil-red O (cat. no.
SLBM4444V; Sigma-Aldrich; Merck KGaA) for 1 h at 37˚C, and pinned
out flat on a wet black cloth with 0.2-mm diameter stainless steel
pins (Fine Science Tools, Inc.). The images of the inner surface of
the aorta were captured using a Ziess digital camera (fiber-optic
CL 1500 ECO cold light source; Carl Zeiss AG) mounted on a Ziess
SteREO Discovery V8 stereo microscope (SteREO Discovery V8; Carl
Zeiss AG). The total aortic surface and atherosclerotic lesion
areas were analyzed en face using computerized quantitative
morphometry by Image Pro Plus software (v6.0, Media Cybernetics,
Inc.). The aortic lesion area was expressed as percentage of the
total aortic area (29).
To quantify the cross-sectional lesion area, the
slices 5-µm from the second segment were stained using EVG
(28,30). Images were captured using a Nikon
DXM 1200/NIS-Elements mounted on a Nikon Eclipse E600 light
microscope (Nikon Corporation) and analyzed using Image Pro Plus
software (v6.0, Media Cybernetics, lnc.).
Quantification of the neutral lipids
and total collagen in plaque
To quantify the neutral lipid content of the plaque,
frozen cross sections of aorta that taken from the 3rd up to the
4th lumbar artery branch point were stained with oil-red O for 30
min at 37˚C, as described previously (28). To determine the total collagen fiber
in the plaque, frozen sections were stained with Sirius red and
fast green for 30 min at room temperature. At least 10 high-power
fields (magnification, x200) were randomly used for each
sample.
Immunohistochemical staining
Immunohistochemical studies were performed on the
luminal aspect of the blood vessel through the plaque to the
elastic lamina (to assess changes that also involved the media).
The detailed procedure has been described previously (6). The 5-µm-thick frozen sections were
fixed in 10% paraformaldehyde solution for 15 min at room
temperature, and then washed with phosphate-buffered saline (PBS)
three times. Sections were blocked with 10% normal goat serum
(Abcam) for 1 h at 37˚C and incubated with primary antibody mouse
anti-rabbit-macrophage monopoly antibody (1:400; CD68; cat. no.
M0633; Dako; Agilent Technologies, Inc.); and primary antibody
mouse anti-rabbit smooth muscle α-actin monopoly antibody (1:50;
HHF-35; cat. no ENZ-C34931; Enzo Life Sciences, Inc.) at
4°C overnight. After incubation, residual antibodies
were removed using three washes with PBS. Subsequently, the tissue
slides were incubated with a secondary antibody Horseradish
Peroxidase (HRP) labeled goat anti-mouse antibody (ready-to-use;
cat. no. 8125; Cell Signaling Technology, Inc.) at 37°C
for 1 h. HRP binding sites were detected using the diaminobenzidine
(DAB) substrate kit per protocol (cat. no. 8059S; Cell Signaling
Technology, Inc.). Tissues were subsequently counterstained with
hematoxylin for 2 min at temperature for microscopic examination.
Negative controls were realized by omission of the primary
antibody. Images were captured with a digital camera (SPOT Flex
Camera; Diagnostic Instruments, Inc.) mounted on a Nikon light
microscope (Nikon Corporation) and analyzed using Image Pro Plus
software (v6.0, Media Cybernetics, Inc.). At least 10 high-power
fields (magnification, x200) were randomly used for each sample.
The area of positive immunohistochemical staining was expressed as
follows: Percentage of the stained area/total plaque area. The
positive immunohistochemical staining of smooth muscle α-actin area
was used to determine the smooth muscle cell (SMC) content of the
plaque.
Evaluation of the stability of the
plaque
The stability of the plaque was evaluated using the
vulnerability index, which was calculated as follows: [Macrophages
staining (%) + lipids staining (%)]/[smooth muscle cells (%) +
total collagen (%)] (31). At least
10 high-power fields (magnification, x200) were selected for each
sample.
Determination of collagen
cross-linking
The cross-linking of the collagen in the plaque was
analyzed using Biocolor S1000 and Biocolor S2000 assay kit
(Biocolor Ltd.). According to the kit, the tissues frozen with
liquid nitrogen were put into a tube with a pepsin concentration of
0.2 mg/ml in 0.5 M acetic acid at 4°C overnight. After
this process, the soluble collagen was released into the solution
and the insoluble collagen was isolated and concentrated using
reagents in the kit. The collagen was then stained by Sircol dye
for 30 min at room temperature and eluted using Alaki Reagent
according to the kit. The eluted solution was analyzed by a
microplate reader under 555-nm wavelength. The insoluble collagen
was analyzed according to the manufacturers protocol. The soluble
collagen and the insoluble collagen were expressed as µg/mg wet
tissue. The cross-linking of the collagen was described as the
ratio of insoluble collagen to soluble collagen, according to the
manufacturers protocol.
Statistical analysis
Data are presented for continuous variables as mean
± SD. Groups that had been fed the atherogenic diet were compared
using one-way ANOVA, followed by Tukey test for multiple
comparisons. All analyses were conducted using SPSS software (IBM
Corp.; version 24.0). P<0.05 was considered to indicate a
statistically significant difference. All figures were constructed
using GraphPad Prism 8.0 Software (GraphPad Software, Inc.).
Results
Changes in the plasma TC, TG, LDL-C,
and HDL-C concentrations after withdrawing the atherogenic
diet
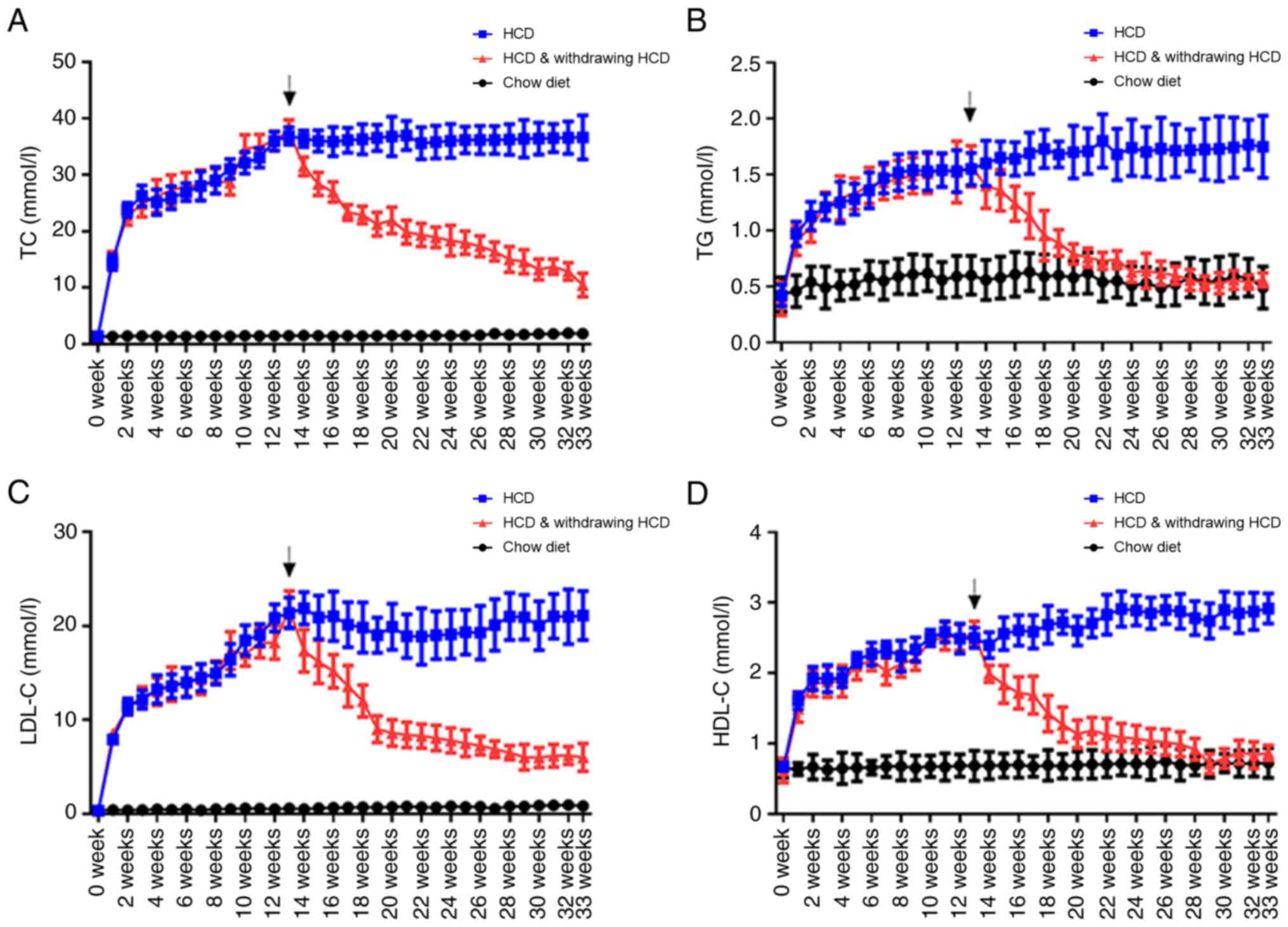
Compared with the control groups, the plasma TC, TG,
LDL-C and HDL-C concentrations markedly increased for 12 weeks and
remained steady during the next 20 weeks of the atherogenic diet.
After withdrawing the atherogenic diet, the plasma TG, LDL-C and
HDL-C concentrations rapidly decreased while the plasma TC
concentration decreased moderately. After 20 weeks of the chow
diet, the plasma TG, and HDL-C concentrations returned to the
baseline levels except for the plasma TC and LDL-C concentration
(Fig. 2A-D).
Changes to the atherosclerotic lesion
areas after withdrawing the atherogenic diet
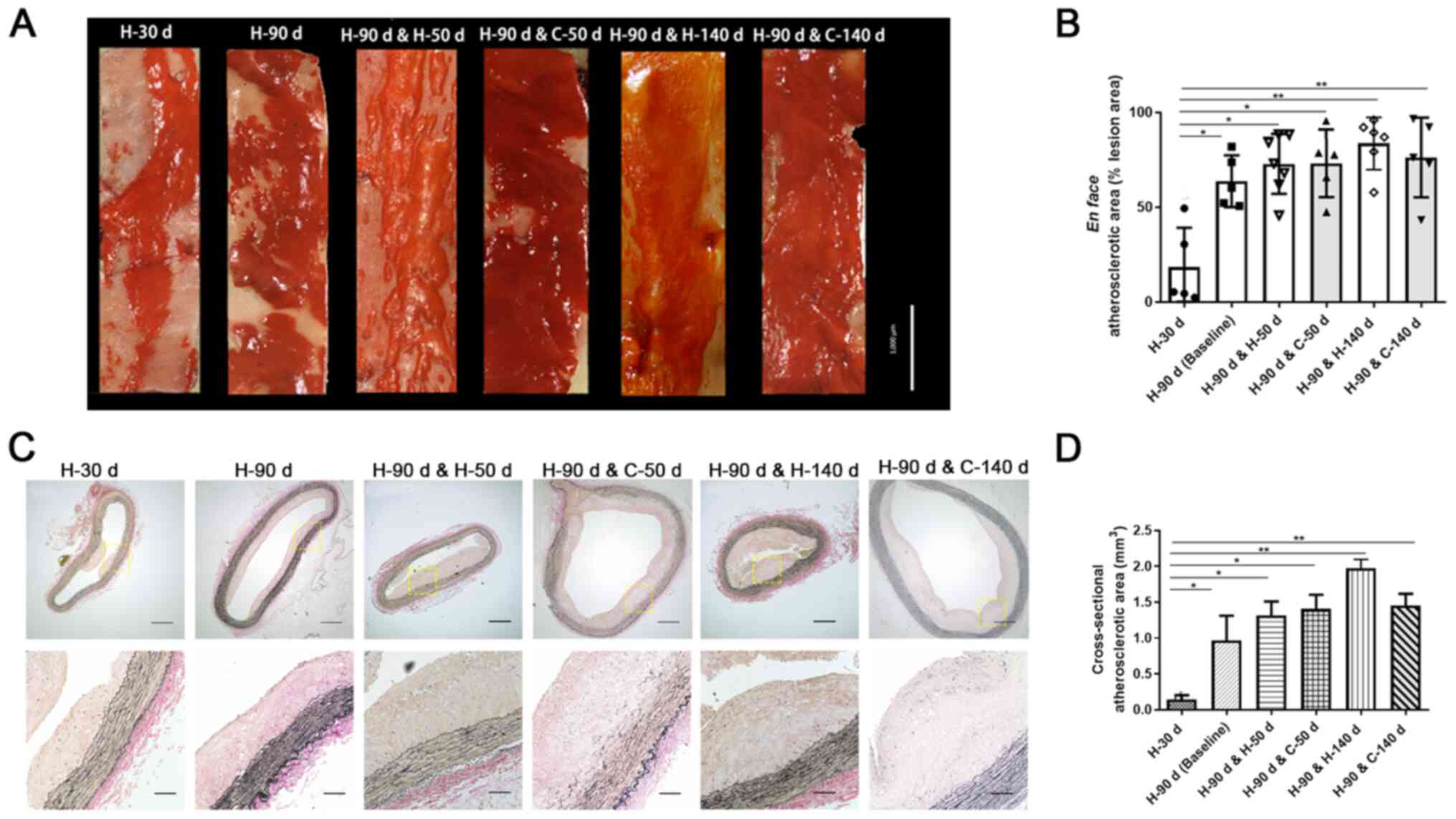
After 30 days of the atherogenic diet (H-30 d),
fatty streaks were induced in the rabbits' aortas. After 90 days of
the atherogenic diet (H-90 d), widespread lesions were induced
(Fig. 3A-D). Fig. 3A and B reveal the en face plaque areas of
the aortas, which are determined by oil-red O staining. There was a
significant difference between H-30 d group and all other groups
(Fig. 3B). En face analysis
of the aortas revealed that the plaque area was significantly
increased from 18.4% in H-30 d group to 63.6% in H-90 d group
(baseline group). When the atherogenic diet was continued, the
en face plaque area increased to 72.6% in H-90 d & H-50
d group and 84.1% in H-90 d & H-140 d group. No significant
differences were observed among the H-90 d group, H-90 d & H-50
d group and the H-90 d & H-140 d group. After the atherogenic
diet was withdrawn for 50 days (H-90 d & C-50 d), the rabbits'
en face lesion area was 71.8%, which was not significantly
lower compared with the baseline group or the atherogenic diet
group. Compared with the atherogenic diet group, the en face
lesion area was reduced to 80.5% in the rabbits that had
cholesterol withdrawn from their diet for 140 days (H-90 d &
C-140 d).
Fig. 3C and D present the cross-sectional plaque areas
of the aortic plaque sections, as determined by EVG staining. There
was a significant difference between H-30 d group and all other
groups (Fig. 3D). The median
cross-sectional plaque area was 0.96 mm2 in the H-90 d
group (baseline group), 1.31 mm2 in H-90 d & H-50 d
group, and 1.97 mm2 in H-90 d & H-140 d group,
respectively. When the atherogenic diet was withdrawn, the
cross-sectional plaque area increased slightly in the rabbits fed
the chow diet for 50 or 140 days compared with the baseline group.
However, compared with the atherogenic diet group (H-90 d &
H-140 d), the cross-sectional plaque area was reduced in rabbits
fed the chow diet for 140 days (H-90 d & C-140 d).
Changes in the plaque components after
withdrawing the atherogenic diet
The changes in the plaque components are presented
in Fig. 4. Fig. 4A and B indicate the changes in the lipid content
of the plaque. Oil-red O staining of the aortic plaque sections
revealed that the lipids content increased during the
atherosclerosis-inducing period. The lipids content was significant
higher in H-90 d & H-50 d, H-90 d & C-50 d, H-90 d &
H-140 d, H-90 d & C-140 d groups than H-30 d or H-90 d group
(Fig. 4B). After withdrawing the
atherogenic diet, the lipid deposition increased for the first 50
days of the chow diet (H-90 d & H-50 d vs. H-90 d & C-50
d). However, the lipid content of the plaque slightly decreased
after 140 days of the chow diet (H-90 d & H-140 d vs. H-90 d
& C-140 d; Fig. 4A and B).
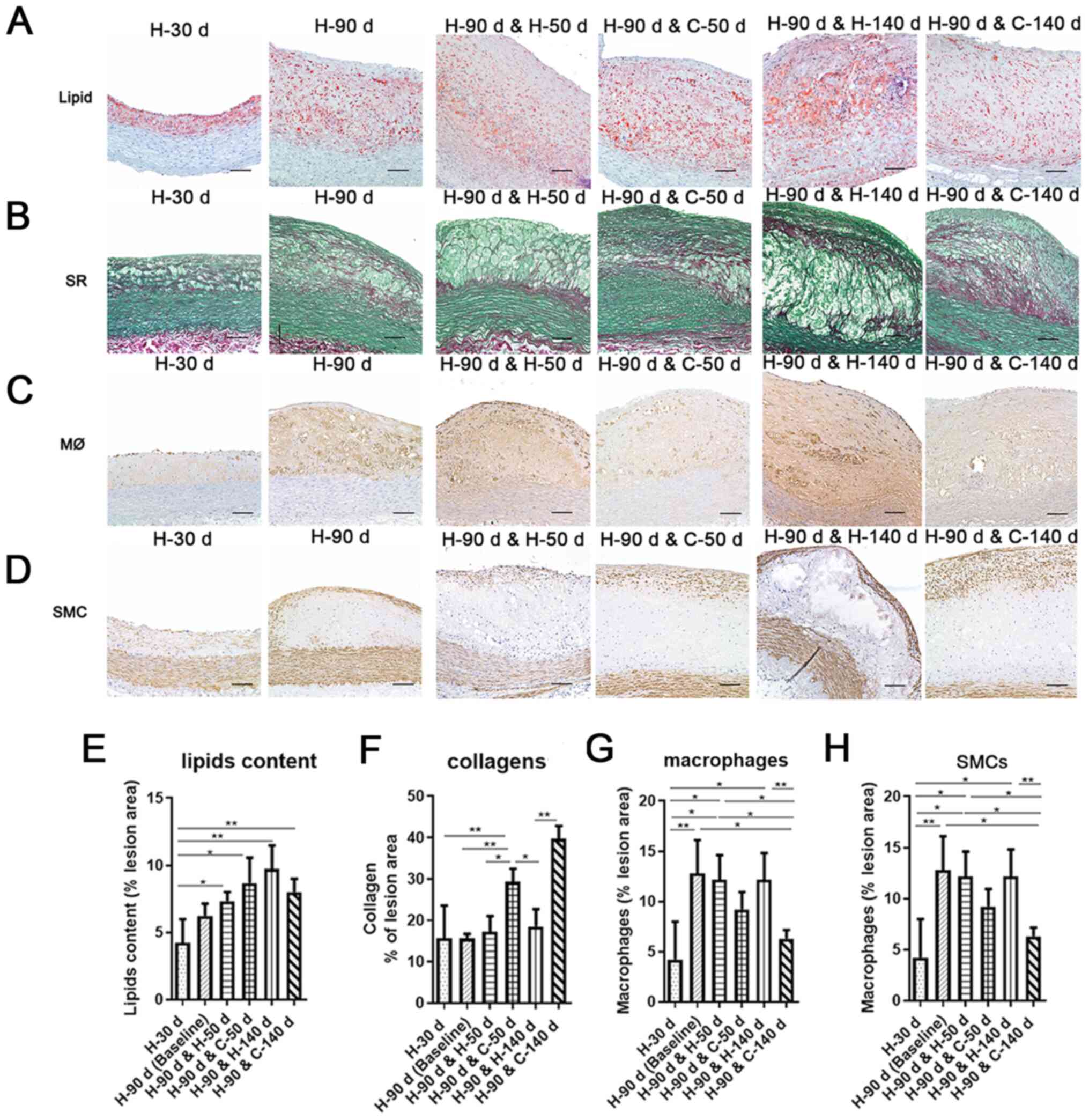 | Figure 4Changes in the plaque components
during the atherogenic diet and after withdrawing the atherogenic
diet. (A) Frozen cross sections were stained using ORO to quantify
the neutral lipids in plaque. x200, bar=100 µm. (B) Frozen cross
sections were stained with SR to quantify the total collagen in
plaques. x200, bar=100 µm. (C) Immunohistochemical staining of
macrophages in plaque. x200, bar=100 µm. (D) Immunohistochemical
staining of SMCs in plaques. x200, bar=100 µm. (E-H) Quantitative
data of the plaque components during the atherogenic diet and after
withdrawing the atherogenic diet. Quantitative data for the
percentage of lipid contents (E), total collagen (F),
macrophage-positive areas (G), and SMC-positive areas (H). All
experimental data were verified in two independent experiments.
Mean ± SD are presented. ORO, oil-red O; SR, Sirius red; SMCs,
smooth muscle cells. *P<0.05;
**P<0.01. |
Sirius red and fast green staining of the aortic
plaques revealed that percentage of the total collagen content of
the plaque did not change significantly in the rabbits fed the
atherogenic diet from day 30 (H-30 d) to day 230 (H-90 d &
H-140 d). However, after withdrawing the atherogenic diet, the
total collagen content of the plaque gradually increased over time
(Fig. 4C and D). The total collagen content of the
plaque was significantly higher in the H-90 d & C-50 d group
and H-90 d & C-140 d group than the other groups (Fig. 4D).
Immunohistochemical analysis of the macrophage
content in the aortic lesions revealed a significant increase in
the macrophage-positive area in the H-90 d group compared with the
H-30 d group. When the rabbits continued to consume the atherogenic
diet, the macrophage content in the plaque remained steady from 90
days of atherogenic diet to 230 days (H-90 d & H-50 d) of
atherogenic diet (H-90 d & H-140 d). However, the
macrophage-positive area in the lesions significantly decreased
compared with the baseline when the diet was replaced with normal
rabbit chow diet for 140 days (H-90 d & C-140 d; Fig. 4E and F).
Immunohistochemical analysis of the SMC content in
atherosclerotic plaque demonstrated that the mean αSMA-positive SMC
area in the atherosclerotic lesions range from 5.48-6.80% during
the atherogenic diet. When the atherogenic diet was shifted to the
chow diet, the mean αSMA-positive SMC area was 6.63% in H-90 d
& C-50 d group and 9.26% in H-90 d & C-140 d group. The
αSMA-positive SMC area was significantly higher in the rabbits
withdrawing from the atherogenic diet for 140 days (H-90 d &
C-140 d) compared with those that continued with the atherogenic
diet for another 140 days (H-90 d & H-140 d) (Fig. 4G and H).
Plaque stability increased after
withdrawing the atherogenic diet
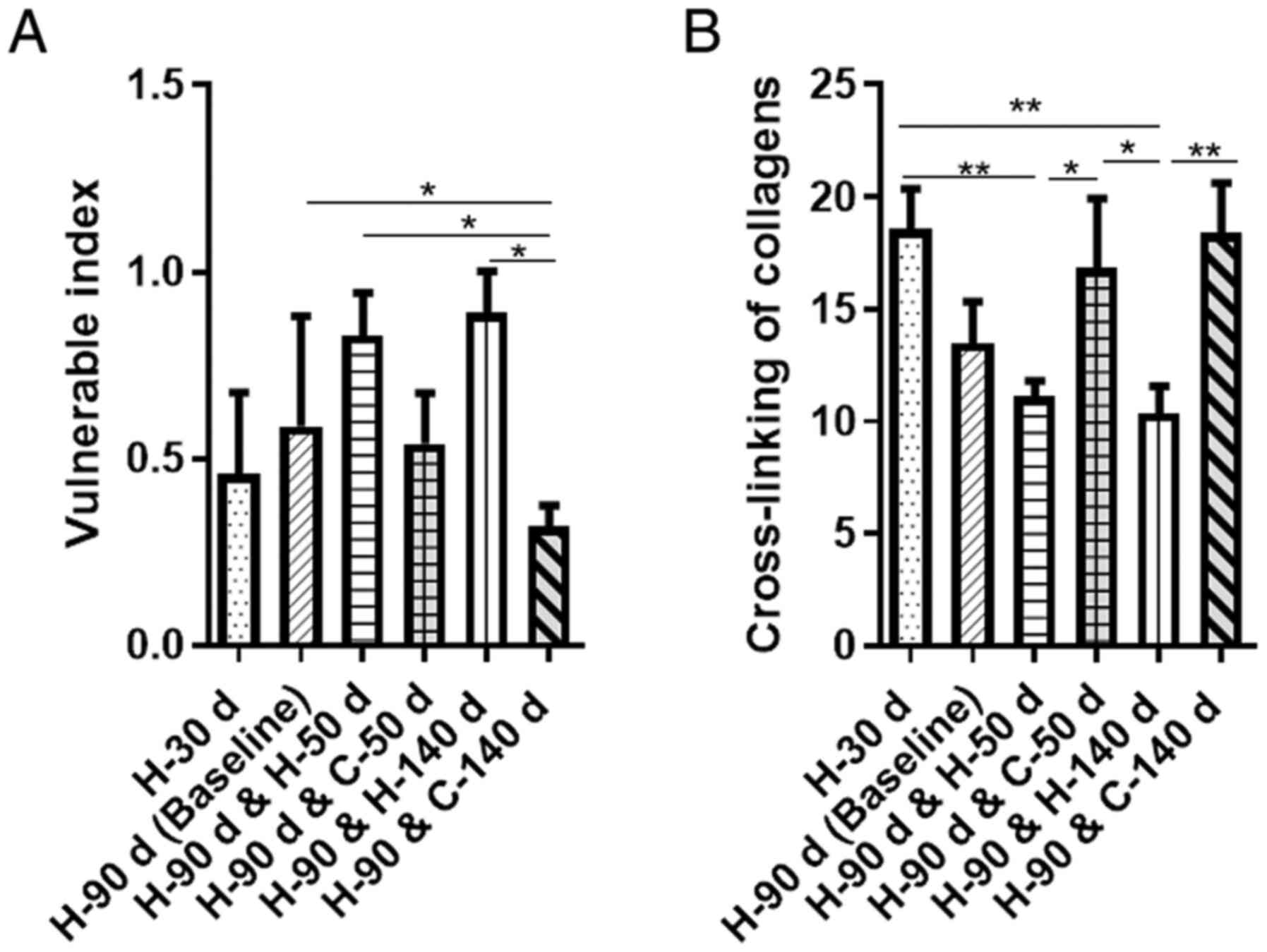
To evaluate the stability of the atherosclerotic
plaque, the vulnerable index was calculated (Fig. 5A). When the rabbits were on the
atherogenic diet, the vulnerable index of the plaque was 0.46 in
the H-30 group, 0.59 in H-90 d group, 0.83 in H-90 d & H-50 d
group, and 0.89 in H-90 d & H-140 d group, respectively. This
result indicating that the formed plaque became more vulnerable
over time. However, the vulnerable index was 0.54 in the H-90 d
& C-50 d group and 0.32 in H-90 d & C-140 d group after
withdrawing the atherogenic diet. The vulnerable index decreased by
8% in H-90 d & C-50 d group compared with the rabbits in H-90 d
group, and decreased by 46% in H-90 d & C-140 d group compared
with the rabbits in the H-90 d & C-50 d group. Compared with
the H-90 d group, the vulnerable index in the H-90 d & C-140 d
group was significantly decreased. Moreover, the vulnerable index
was the lowest in H-90 d & C-140 d group among all groups.
Collagen cross-linking increased after
withdrawing the atherogenic diet
The cross-linking of collagen in the atherosclerotic
plaque was further analyzed in the current study. Compared with the
rabbits in H-30 d group, the cross-linking of collagen decreased
significantly in the rabbits in the H-90 d & H-50 d group or
H-90 d & H-140 d group. Conversely, when given the chow diet
for 50 days or 140 days, the cross-linking of collagen in the
lesions markedly increased compared with the
atherosclerosis-inducing groups (Fig.
5B). The cross-linking of collagen was significantly higher in
H-90 d & C-50 d group or H-90 d & C-140 d group than that
in H-90 d & H-50 d group or H-90 d & H-140 d group.
Discussion
The current study demonstrated that after 90 days of
high cholesterol feeding, the rabbits' aortas exhibited severe
atherosclerotic lesions accompanied by increased amount of lipids
deposition, the accumulation of foam cells, overexpression of the
extracellular matrix and decreased cross-linking of collagen.
Withdrawing cholesterol from the diet did not lead to the
regression of established atherosclerosis but delayed the
progression of lesions compared with the baseline group. However,
the plaque area was moderately reduced after withdrawing
cholesterol from the diet for 140 days (vs. continuation of the
atherogenic diet for 140 more days). Upon removal of the
atherogenic diet for 50 days or 140 days, the lipid deposition,
total collagen content, and SMC content increased in the plaque,
and the macrophages content decreased in the lesions (vs. the
baseline group). Further analysis demonstrated that the vulnerable
index decreased and the cross-linking of collagens increased after
withdrawing the atherogenic diet, which implied that the stability
of the plaque increased.
Atherosclerosis is a lipoprotein-driven disease that
leads to the formation of plaque at specific sites on the arterial
tree with high stress (5). The
plaque is characterized by lipoprotein retention, macrophage
infiltration, smooth muscle cell proliferation and matrix synthesis
(5). During the
atherosclerosis-inducing period of the present study, lipid,
collagen and macrophages were persistently deposited in the aortic
plaque. The rates of macrophage infiltration and lipid deposition
were higher than the total collagen expression rate, which was in
line with the pathophysiology of xanthomas or fatty streaks
(5). Xanthomas have been detected
in fetal aortas and 6-month-old infants, which most likely reflects
risk factors of the mother (32).
However, xanthomas are harmless and fully reversible if the stimuli
that caused their formation dissipate (33). Previous clinical trials indicated
that lipid-lowering drugs (for example, statins and proprotein
convertase subtilisin kexin type 9 inhibitors) and HDL-raising
therapy (for example, the infusion of reconstituted HDL) result in
decreased atheroma volume (34-37).
Experimental agents in preclinical studies, including intravenous
injections of phospholipid liposomes or apoA-I, long-term
administration of L-arginine or anti-inflammatory antibody combined
with or without a normal diet, result in the attenuation of plaque
progression compared with nontreated control animals (38-41).
Nevertheless, lipid-lowering diets have always been the most common
treatment for atherosclerosis.
The American Heart Association provides
recommendations for diet modifications for cardiovascular disease
risk reduction in the general population (42). The concept of regressing
atherosclerosis in nonhuman primates has been reviewed by Malinow
(43) and Feig (44). In the classic studies conducted in
primates, the advanced arterial lesions in cholesterol-fed Rhesus
monkeys underwent shrinkage and remodeling during the 40 months
when their diet was switched to low-fat or linoleate-rich (15,19).
More extensive work by Aikawa et al (10) indicated that cholesterol reduction
by diet alone was able to shrink the plaque size and stabilize
vulnerable plaque in rabbits subjected to balloon injury and
cholesterol feeding (0.3%) for 4 months (10,12,20,21,45,46).
Mice are relatively resistant to the development of
atherosclerosis; Therefore, genetic manipulation of the lipid
metabolism is routinely used in atherosclerosis studies involving
these animals (47). In transgenic
mice, studies on the effects of dietary intervention alone on
atherosclerotic plaques are limited (48), whereas previous evidence has
suggested that aortic transplant, the injection of recombinant
apoA-I or a reconstituted statin-containing HDL particle combined
with a chow diet resulted in a rapid lesion regression in
apoE-/- or Ldlr-/- mice (49). Cessation of cholesterol feeding in
animals demonstrates effectiveness in regressing plaque progression
(17,19). However, in the current study, the
atherosclerotic plaque areas did not shrink but increased slightly
in the rabbits with cessation of the atherogenic diet compared with
the baseline group (H-90 d). The underlying reason for this result
may be related to high cholesterol storage in the liver during the
atherosclerosis-inducing phase. The diet-induced cholesterol
storage supports the long-term persistence of hypercholesterolemia
even after withdrawing cholesterol from the diet (Fig. 2A) (8). Compared with the rabbits that
continued to consume an atherogenic diet, the plaque size was
reduced in the animals from which cholesterol had been withdrawn
for 140 days. Furthermore, the total collagen and αSMC content
increased and the macrophage content decreased, which resulted in
an increased stability of the plaque after switching to a chow diet
for 140 days. These results indicated that removal of cholesterol
from the diet following a cholesterol-rich diet does not always
lead to the regression of lesions but instead results in the
slowing down of the lesion progression and stabilization of the
plaque.
Plaque size and stability are other hallmarks of
atherosclerotic vascular disease (50). Plaque rupture is the most common
cause of coronary thrombosis and leads to ASCVD (51). The majority (~76%) of all fatal
coronary artery thrombi are precipitated by plaque rupture
(52). Ruptured and ruptured-prone
plaque is characterized by a large lipid-rich core, a thin and
collagen-poor fibrous cap, the accumulation of macrophages,
neovascularization and intraplaque hemorrhage (5). Collagen constitutes a major portion of
the extracellular matrix in the plaque, where it contributes to the
strength and integrity of the fibrous cap (53). Previous studies have indicated that
lipid lowering reinforced the fibrous skeleton of the atheroma via
the induction of collagen synthesis and the promotion of the
transition of initial SMCs in atherosclerotic rabbits (10,12,20).
The cross-linking of collagen is a pivotal process that ensures
plaque stability and provides the tensile and elastic
characteristics of connective tissues (22,54).
This process is regulated by lysyl oxidase (LOX), which belongs to
a family of copper-dependent enzymes (55). A previous study reported that LOX is
strongly downregulated in different stages of the atherosclerotic
process (56). In atherosclerotic
plaque from human carotid endarterectomies, higher LOX levels,
which suggest an enhanced cross-linking of collagen, were
associated with a more stable phenotype of the plaque (22). The results from the current study
revealed that the cross-linking of collagens was enhanced, and the
vulnerable index was decreased after withdrawing the atherogenic
diet, indicating that the plaque was becoming more stable.
Therefore, it can be concluded that withdrawing the atherogenic
diet changed the compositions of the plaque, resulting in increased
plaque stability in atherosclerotic rabbits. The current
preclinical study provides evidence for cholesterol restriction
strategies in clinical practice.
Cholesterol-fed rabbits are the classical model for
the study of atherosclerosis. New Zealand White rabbits are
sensitive to dietary cholesterol and rapidly develop severe
hypercholesterolaemia, leading to prominent plaque lesions when fed
an atherogenic diet (1.0-1.5% cholesterol) for a short period time
(about 8 weeks) (23,57). Under the atherogenic diet, plaque
develops in the aortic arch, the thoracic aorta and the abdominal
aorta in these rabbits (24,58).
The data in the current study indicated that after 90 days of an
atherosclerosis-inducing diet, the en face plaque areas of
all aortic arches and thoracic aortas were nearly 100%, whereas the
en face plaque areas of the abdominal aortas fluctuated
between 50 and 80% (Fig. 1B). The
plaque changes in the abdominal aortas are able to be measured
accurately using oil red O staining. In humans, plaque is commonly
located in the abdominal aorta, so the rabbit abdominal aorta is a
suitable atherosclerotic model that closely mimics the human
lesions (59). Therefore, abdominal
aorta tissue in rabbit was selected to investigate the effect of
withdrawing atherogenic diet on atherosclerotic plaque in the
present study.
The evaluation of the stability of plaques using the
vulnerable index was one limitation of this study (31). This method was invasive. A number
invasive and noninvasive novel imaging modalities, such as MRI,
optical coherence tomography, intravascular MRI and intravascular
spectroscopy, have been investigated as being techniques that can
be used to define the specific characteristics of vulnerable plaque
(60). However, the majority of
these techniques are undergoing constant refinement and have
limited reliability in the identification of vulnerable plaque
(60). The vulnerable index is a
simple method and is still widely used for atherosclerosis in
rabbits or transgenic mice (61-65).
In conclusion, the current study demonstrated that
withdrawing the atherogenic diet did not regress the plaque but
slowed the progression of atherosclerosis in the cholesterol-fed
rabbits. Withdrawing the atherogenic diet increased the total
collagen content, alleviated macrophage infiltration, enhanced the
cross-linking of collagen and decreased the vulnerable index of
plaque. These findings support the notion that a healthy diet
should be the fundamental therapy for atherosclerotic
cardiovascular disease in clinical practice (66).
Acknowledgements
Not applicable.
Funding
Funding: The current study was supported by the Popularization
Project of the Science and Technology Project of the Sichuan Health
Planning Committee (grant no. 19PJ250), Postdoctoral Research
Foundation in West China Hospital (grant no. 2019HXBH101), and
Basic Research Project of Sichuan Science and Technology Program
(grant no. 2020YJ0063).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
LZ, SZ, QS and SL conceived and designed the study
and reviewed the manuscript. LZ analyzed the data and interpreted
the results. LZ and SZ drafted the manuscript. SL analyzed and
interpreted data, edited/revised and approved the final version of
the manuscript. LZ, SZ, QS and SL contributed to the discussion of
this manuscript. SL and LZ were responsible for confirming the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
All animal protocols were approved by the
Institutional Animal Care and Use Committee (IACUC) of the West
China Hospital of Sichuan University.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Zhou M, Wang H, Zhu J, Chen W, Wang L, Liu
S, Li Y, Wang L, Liu Y, Yin P, et al: Cause-specific mortality for
240 causes in China during 1990-2013: A systematic subnational
analysis for the Global Burden of Disease Study 2013. Lancet.
387:251–272. 2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Zhao D, Liu J, Wang M, Zhang X and Zhou M:
Epidemiology of cardiovascular disease in China: Current features
and implications. Nat Rev Cardiol. 16:203–212. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Barquera S, Pedroza-Tobias A, Medina C,
Hernández-Barrera L, Bibbins-Domingo K, Lozano R and Moran AE:
Global overview of the epidemiology of atherosclerotic
cardiovascular disease. Arch Med Res. 46:328–338. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Vigen C, Hodis HN, Selzer RH, Mahrer PR
and Mack WJ: Relation of progression of coronary artery
atherosclerosis to risk of cardiovascular events (from the
Monitored Atherosclerosis Regression Study). Am J Cardiol.
95:1277–1282. 2005.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bentzon JF, Otsuka F, Virmani R and Falk
E: Mechanisms of plaque formation and rupture. Circ Res.
114:1852–1866. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Zhao LJ, Xiao Y, Meng X, Wang N and Kang
YJ: Application of a simple quantitative assessment of
atherosclerotic lesions in freshly isolated aortas from rabbits.
Cardiovasc Toxicol. 18:537–546. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Goldberg IJ, Sharma G and Fisher EA:
Atherosclerosis: Making a U Turn. Annu Rev Med. 71:191–201.
2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Chistiakov DA, Myasoedova VA, Revin VV,
Orekhov AN and Bobryshev YV: The phenomenon of atherosclerosis
reversal and regression: Lessons from animal models. Exp Mol
Pathol. 102:138–145. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ornish D, Brown SE, Scherwitz LW, Billings
JH, Armstrong WT, Ports TA, McLanahan SM, Kirkeeide RL, Brand RJ
and Gould KL: Can lifestyle changes reverse coronary heart disease?
The lifestyle heart trial. Lancet. 336:129–133. 1990.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Aikawa M, Rabkin E, Voglic SJ, Shing H,
Nagai R, Schoen FJ and Libby P: Lipid lowering promotes
accumulation of mature smooth muscle cells expressing smooth muscle
myosin heavy chain isoforms in rabbit atheroma. Circ Res.
83:1015–1026. 1998.PubMed/NCBI View Article : Google Scholar
|
|
11
|
McConnell MV, Aikawa M, Maier SE, Ganz P,
Libby P and Lee RT: MRI of rabbit atherosclerosis in response to
dietary cholesterol lowering. Arterioscler Thromb Vasc Biol.
19:1956–1959. 1999.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Aikawa M and Libby P: Lipid lowering
reduces proteolytic and prothrombotic potential in rabbit atheroma.
Ann N Y Acad Sci. 902:140–152. 2000.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Haghjooyjavanmard S, Nematbakhsh M,
Monajemi A and Soleimani M: von Willebrand factor, C-reactive
protein, nitric oxide, and vascular endothelial growth factor in a
dietary reversal model of hypercholesterolemia in rabbit. Biomed
Pap Med Fac Univ Palacky Olomouc Czech Repub. 152:91–95.
2008.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Maruffo CA and Portman OW: Nutritional
control of coronary artery atherosclerosis in the squirrel monkey.
J Atheroscler Res. 8:237–247. 1968.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Armstrong ML, Warner ED and Connor WE:
Regression of coronary atheromatosis in rhesus monkeys. Circ Res.
27:59–67. 1970.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Daoud AS, Jarmolych J, Augustyn JM and
Fritz KE: Sequential morphologic studies of regression of advanced
atherosclerosis. Arch Pathol Lab Med. 105:233–239. 1981.PubMed/NCBI
|
|
17
|
Wissler RW and Vesselinovitch D: Studies
of regression of advanced atherosclerosis in experimental animals
and man. Ann N Y Acad Sci. 275:363–378. 1976.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Libby P, Bornfeldt KE and Tall AR:
Atherosclerosis: Successes, surprises, and future challenges. Circ
Res. 118:531–534. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Armstrong ML: Evidence of regression of
atherosclerosis in primates and man. Postgrad Med J. 52:456–461.
1976.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Aikawa M, Rabkin E, Okada Y, Voglic SJ,
Clinton SK, Brinckerhoff CE, Sukhova GK and Libby P: Lipid lowering
by diet reduces matrix metalloproteinase activity and increases
collagen content of rabbit atheroma: A potential mechanism of
lesion stabilization. Circulation. 97:2433–2444. 1998.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Aikawa M, Sugiyama S, Hill CC, Voglic SJ,
Rabkin E, Fukumoto Y, Schoen FJ, Witztum JL and Libby P: Lipid
lowering reduces oxidative stress and endothelial cell activation
in rabbit atheroma. Circulation. 106:1390–1396. 2002.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ovchinnikova OA, Folkersen L, Persson J,
Lindeman JH, Ueland T, Aukrust P, Gavrisheva N, Shlyakhto E,
Paulsson-Berne G, Hedin U, et al: The collagen cross-linking enzyme
lysyl oxidase is associated with the healing of human
atherosclerotic lesions. J Intern Med. 276:525–536. 2014.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Fan J, Kitajima S, Watanabe T, Xu J, Zhang
J, Liu E and Chen YE: Rabbit models for the study of human
atherosclerosis: From pathophysiological mechanisms to
translational medicine. Pharmacol Ther. 146:104–119.
2015.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Emini Veseli B, Perrotta P, De Meyer GRA,
Roth L, Van der Donckt C, Martinet W and De Meyer GRY: Animal
models of atherosclerosis. Eur J Pharmacol. 816:3–13.
2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Coscia L, Causa P, Giuliani E and Nunziata
A: Pharmacological properties of new neuroleptic compounds.
Arzneimittelforschung. 25:1436–1442. 1975.PubMed/NCBI
|
|
26
|
Gil AG, Silvan G, Illera M and Illera JC:
The effects of anesthesia on the clinical chemistry of New Zealand
White rabbits. Contemp Top Lab Anim Sci. 43:25–29. 2004.PubMed/NCBI
|
|
27
|
Ishikawa N, Kallman CH and Sagawa K:
Rabbit carotid sinus reflex under pentobarbital, urethan, and
chloralose anesthesia. Am J Physiol. 246:H696–H701. 1984.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Lin Y, Bai L, Chen Y, Zhu N, Bai Y, Li Q,
Zhao S, Fan J and Liu E: Practical assessment of the quantification
of atherosclerotic lesions in apoE-/- mice.
Mol Med Rep. 12:5298–5306. 2015.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Zhang WJ, Wei H and Frei B: The iron
chelator, desferrioxamine, reduces inflammation and atherosclerotic
lesion development in experimental mice. Exp Biol Med (Maywood).
235:633–641. 2010.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Zhang C, Zheng H, Yu Q, Yang P, Li Y,
Cheng F, Fan J and Liu E: A practical method for quantifying
atherosclerotic lesions in rabbits. J Comp Pathol. 142:122–128.
2010.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Liu XQ, Mao Y, Wang B, Lu XT, Bai WW, Sun
YY, Liu Y, Liu HM, Zhang L, Zhao YX and Zhang Y: Specific matrix
metalloproteinases play different roles in intraplaque angiogenesis
and plaque instability in rabbits. PLoS One.
9(e107851)2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Napoli C, D'Armiento FP, Mancini FP,
Postiglione A, Witztum JL, Palumbo G and Palinski W: Fatty streak
formation occurs in human fetal aortas and is greatly enhanced by
maternal hypercholesterolemia. Intimal accumulation of low density
lipoprotein and its oxidation precede monocyte recruitment into
early atherosclerotic lesions. J Clin Invest. 100:2680–2690.
1997.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Stary HC: Lipid and macrophage
accumulations in arteries of children and the development of
atherosclerosis. Am J Clin Nutr. 72 (5 Suppl):1297S–1306S.
2000.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Nissen SE, Nicholls SJ, Sipahi I, Libby P,
Raichlen JS, Ballantyne CM, Davignon J, Erbel R, Fruchart JC,
Tardif JC, et al: Effect of very high-intensity statin therapy on
regression of coronary atherosclerosis: The ASTEROID trial. JAMA.
295:1556–1565. 2006.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Stein EA, Mellis S, Yancopoulos GD, Stahl
N, Logan D, Smith WB, Lisbon E, Gutierrez M, Webb C, Wu R, et al:
Effect of a monoclonal antibody to PCSK9 on LDL cholesterol. New
Engl J Med. 366:1108–1118. 2012.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Waksman R, Torguson R, Kent KM, Pichard
AD, Suddath WO, Satler LF, Martin BD, Perlman TJ, Maltais JA,
Weissman NJ, et al: A first-in-man, randomized, placebo-controlled
study to evaluate the safety and feasibility of autologous
delipidated high-density lipoprotein plasma infusions in patients
with acute coronary syndrome. J Am Coll Cardiol. 55:2727–2735.
2010.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Nissen SE, Tsunoda T, Tuzcu EM,
Schoenhagen P, Cooper CJ, Yasin M, Eaton GM, Lauer MA, Sheldon WS,
Grines CL, et al: Effect of recombinant ApoA-I Milano on coronary
atherosclerosis in patients with acute coronary syndromes: A
randomized controlled trial. JAMA. 290:2292–2300. 2003.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Rodrigueza WV, Klimuk SK, Pritchard PH and
Hope MJ: Cholesterol mobilization and regression of atheroma in
cholesterol-fed rabbits induced by large unilamellar vesicles.
Biochim Biophys Acta. 1368:306–320. 1998.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Miyazaki A, Sakuma S, Morikawa W, Takiue
T, Miake F, Terano T, Sakai M, Hakamata H, Sakamoto Y, Natio M, et
al: Intravenous injection of rabbit apolipoprotein A-I inhibits the
progression of atherosclerosis in cholesterol-fed rabbits.
Arterioscler Thromb Vasc Biol. 15:1882–1888. 1995.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Candipan RC, Wang BY, Buitrago R, Tsao PS
and Cooke JP: Regression or progression. Dependency on vascular
nitric oxide. Arterioscler Thromb Vasc Biol. 16:44–50.
1996.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Elhage R, Maret A, Pieraggi MT, Thiers JC,
Arnal JF and Bayard F: Differential effects of interleukin-1
receptor antagonist and tumor necrosis factor binding protein on
fatty-streak formation in apolipoprotein E-deficient mice.
Circulation. 97:242–244. 1998.PubMed/NCBI View Article : Google Scholar
|
|
42
|
American Heart Association Nutrition
Committee. Lichtenstein AH, Appel LJ, Brands M, Carnethon M,
Daniels S, Franch HA, Franklin B, Kris-Etherton P, Harris WS, et
al: Diet and lifestyle recommendations revision 2006: A scientific
statement from the American Heart Association Nutrition Committee.
Circulation. 114:82–96. 2006.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Malinow MR: Experimental models of
atherosclerosis regression. Atherosclerosis. 48:105–118.
1983.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Feig JE: Regression of atherosclerosis:
Insights from animal and clinical studies. Ann Glob Health.
80:13–23. 2014.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Aikawa M and Libby P: Lipid lowering
therapy in atherosclerosis. Semin Vasc Med. 4:357–366.
2004.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Aikawa M, Voglic SJ, Sugiyama S, Rabkin E,
Taubman MB, Fallon JT and Libby P: Dietary lipid lowering reduces
tissue factor expression in rabbit atheroma. Circulation.
100:1215–1222. 1999.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Meir KS and Leitersdorf E: Atherosclerosis
in the apolipoprotein-E-deficient mouse: A decade of progress.
Arterioscler Thromb Vasc Biol. 24:1006–1014. 2004.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Peled M, Nishi H, Weinstock A, Barrett TJ,
Zhou F, Quezada A and Fisher EA: A wild-type mouse-based model for
the regression of inflammation in atherosclerosis. PLoS one.
12(e0173975)2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Feig JE, Rong JX, Shamir R, Sanson M,
Vengrenyuk Y, Liu J, Rayner K, Moore K, Garabedian M and Fisher EA:
HDL promotes rapid atherosclerosis regression in mice and alters
inflammatory properties of plaque monocyte-derived cells. Proc Natl
Acad Sci USA. 108:7166–7171. 2011.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Hafiane A: Vulnerable plaque,
characteristics, detection, and potential therapies. J Cardiovasc
Dev Dis. 6(26)2019.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Zaman AG, Helft G, Worthley SG and Badimon
JJ: The role of plaque rupture and thrombosis in coronary artery
disease. Atherosclerosis. 149:251–266. 2000.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Falk E: Pathogenesis of atherosclerosis. J
Am Coll Cardiol. 47:C7–C12. 2006.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Adiguzel E, Ahmad PJ, Franco C and Bendeck
MP: Collagens in the progression and complications of
atherosclerosis. Vasc Med. 14:73–89. 2009.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Martínez-González J, Varona S, Cañes L,
Galán M, Briones AM, Cachofeiro V and Rodríguez C: Emerging roles
of lysyl oxidases in the cardiovascular system: New concepts and
therapeutic challenges. Biomolecules. 9(610)2019.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Li T, Wu C, Gao L, Qin F, Wei Q and Yuan
J: Lysyl oxidase family members in urological tumorigenesis and
fibrosis. Oncotarget. 9:20156–20164. 2018.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Rodriguez C, Martinez-Gonzalez J, Raposo
B, Alcudia JF, Guadall A and Badimon L: Regulation of lysyl oxidase
in vascular cells: Lysyl oxidase as a new player in cardiovascular
diseases. Cardiovasc Res. 79:7–13. 2008.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Baumgartner C, Brandl J, Münch G and
Ungerer M: Rabbit models to study atherosclerosis and its
complications-Transgenic vascular protein expression in vivo. Prog
Biophys Mol Biol. 121:131–141. 2016.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Getz GS and Reardon CA: Animal models of
atherosclerosis. Arterioscler Thromb Vasc Biol. 32:1104–1115.
2012.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Buchanan JR, Kleinstreuer C, Hyun S and
Truskey GA: Hemodynamics simulation and identification of
susceptible sites of atherosclerotic lesion formation in a model
abdominal aorta. J Biomech. 36:1185–1196. 2003.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Sharif F and Murphy RT: Current status of
vulnerable plaque detection. Catheter Cardiovasc Interv.
75:135–144. 2010.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Dong M, Zhou C, Ji L, Pan B and Zheng L:
AG1296 enhances plaque stability via inhibiting inflammatory
responses and decreasing MMP-2 and MMP-9 expression in
ApoE-/- mice. Biochem Biophys Res Commun. 489:426–431.
2017.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Liang WJ, Zhou SN, Shan MR, Wang XQ, Zhang
M, Chen Y, Zhang Y, Wang SX and Guo T: AMPKα inactivation
destabilizes atherosclerotic plaque in streptozotocin-induced
diabetic mice through AP-2α/miRNA-124 axis. J Mol Med (Berl).
96:403–412. 2018.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Shiomi M, Ito T, Hirouchi Y and Enomoto M:
Fibromuscular cap composition is important for the stability of
established atherosclerotic plaques in mature WHHL rabbits treated
with statins. Atherosclerosis. 157:75–84. 2001.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Wang F, Chen FF, Shang YY, Li Y, Wang ZH,
Han L, Li YH, Zhang L, Ti Y, Zhang W and Zhong M: Insulin
resistance adipocyte-derived exosomes aggravate atherosclerosis by
increasing vasa vasorum angiogenesis in diabetic ApoE mice. Int J
Cardiol. 265:181–187. 2018.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Burke AC, Sutherland BG, Telford DE,
Morrow MR, Sawyez CG, Edwards JY and Huff MW: Naringenin enhances
the regression of atherosclerosis induced by a chow diet in Ldlr
mice. Atherosclerosis. 286:60–70. 2019.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Volgman AS, Palaniappan LS, Aggarwal NT,
Gupta M, Khandelwal A, Krishnan AV, Lichtman JH, Mehta LS, Patel
HN, Shah KS, et al: Atherosclerotic cardiovascular disease in South
Asians in the United States: Epidemiology, risk factors, and
treatments: A scientific statement from the American Heart
Association. Circulation. 138:e1–e34. 2018.PubMed/NCBI View Article : Google Scholar
|