Introduction
Bladder cancer (BC) is one of the most common
malignancies of the genitourinary system (1). Despite the established risk factors,
such as age, smoking and family history, there is an absence of
early detection strategies (2).
Biomarkers have potential for the diagnosis, staging, prognosis,
and treatment of BC (3). However,
the biomarkers currently used for BC present several limitations,
such as PD-L1 immunohistochemistry lacking standard uniformity and
definitions for PD-L1 testing, with the major concern being the
lack of a common method for assessment and interpretation of IHC
staining (4). Thus, it is important
to identify novel BC biomarkers with high specificity and
sensitivity.
Human cytosolic sulfotransferases (SULTs) are phase
II detoxification enzymes that catalyze the biotransformation of
several endogenous and exogenous substrates (5). In most cases, this reaction renders
the substrate more water-soluble, resulting in excretion (6). However, in some instances, the
sulfation of a molecule results in bioactivation, which induces
carcinogenesis; one example is the aromatic compounds from
cigarette smoke and occupational exposures, the principal exogenous
risk factors for BC (7,8). By influencing DNA adduct formation,
Sulfotransferase Family 1A Member 2 (SULT1A2) has been reported to
induce the mutagenicity and carcinogenicity of substrates,
including nitrotoluenes, 3-nitrobenzanthrone, aristolochic acids,
aromatic hydroxylamine and polycyclic aromatic hydrocarbons
(9-11).
Several studies have demonstrated that SULT1A2 plays a role in the
chemical carcinogenesis of these substrates if it is expressed as a
functional protein (12,13). In addition, SULT1A2 is considered
one of the five major genes associated with BC (2). Although SULT1A2 RNA has been detected
in several tissues, Nowell et al (12) demonstrated that SULT1A2 protein
expression in human tissues, including bladder tumors, was poorly
detected using a SULT1A2-specific antibody. However, the expression
of SULT1A2 may be misleading since the protein may be induced under
certain physiological states to achieve bioactivation by sulfation.
Only a few studies have investigated the tissue distribution and
regulatory mechanism of SULT1A2(12). Thus, it is important to determine
whether SULT1A2 is expressed in human bladder tissues, and clarify
how SULT1A2 participates and affects the occurrence and development
of BC.
To the best of our knowledge, the present study was
the first to demonstrate that SULT1A2 expression is upregulated in
BC cells and tissues compared with normal bladder cells and
tissues. The aim of the current study was to explore the
feasibility of SULT1A2 as an effective biomarker for the staging
and determining the prognosis of patients with BC.
Materials and methods
Clinical samples
A total of 100 formalin-fixed, paraffin-embedded
(FFPE) BC tissues, and 12 frozen BC tissues and corresponding
adjacent normal bladder tissues (ANBTs; >5 cm from the tumor)
were collected from patients with BC who underwent radical
resection, without preoperative chemotherapy or radiotherapy, at
the First Affiliated Hospital of Sun Yat-sen University between
February 2015 and October 2018. According to BC histopathology
(14), the tissue samples were
divided into non-muscle invasive cancer (NMIBC) and muscle invasive
cancer (MIBC). NMIBC includes Ta stage (tumor is confined to the
bladder mucosa), Tis stage (carcinoma in situ) and T1 stage
(tumor manifests as invasion of the subepithelial connective
tissue). MIBC includes T2 stage (tumor invades the muscle layer),
T3 stage (tumor invades the adjacent bladder tissues) and T4 stage
(tumor invades other tissues or organs). Immunohistochemistry (IHC)
analysis was performed using FFPE BC tissues stored at 4˚C
including 41 NMIBC and 59 MIBC samples, and corresponding ANBTs.
Reverse transcription-quantitative (RT-q)PCR and western blot
analyses were performed using the 12 frozen BC tissues stored at
-80˚C, including six NMIBC and six MIBC samples, and corresponding
ANBTs. The present study was approved by the Institutional Ethics
Committee for Clinical Research and Animal Trials of the First
Affiliated Hospital of Sun Yat-sen University, Guangzhou, China
[approval no. (2016)067]. Written informed consent was provided by
all patients prior to the study start.
Cell culture
The human uroepithelial SV-HUC-1 cell line was
purchased from the American Type Culture Collection and maintained
in F-12K medium (Gibco, Thermo Fisher Scientific, Inc.). The human
T24 and 5637 BC cell lines were purchased from the Institute of
Cell Biology, Chinese Academy of Sciences (https://www.cellbank.org.cn). T24 cells were
maintained in RPMI-1640, while 5637 cells were maintained in
minimum essential medium (both purchased from Gibco; Thermo Fisher
Scientific, Inc.). All media were supplemented with 10% fetal
bovine serum (Gibco; Thermo Fisher Scientific, Inc.) and cultured
at 37˚C, with 5% CO2.
IHC
BC tissues and ANBTs were fixed in 4% formalin
solution for 24 h at room temperature, then embedded in paraffin
and sectioned (5-µm-thick). Paraffin sections were heated at 55˚C
for 2 h. Prior to immunostaining, slides were dewaxed in xylene and
rehydrated in alcohol, and antigen retrieval was performed by
microwaving the slides in citric saline (Wuhan Promoter Biological
Co., Ltd.). The slides were subsequently incubated with 3% hydrogen
peroxide to inhibit endogenous peroxidase activity for 15 min at
room temperature and blocked with 3% goat serum (Sigma-Aldrich;
Merck KGaA) for 10 min at 37˚C. For IHC staining, the slides were
incubated with primary antibody against SULT1A2 (cat. no.
HPA051051; 1:200; Sigma-Aldrich; Merck KGaA) overnight at 4˚C, and
subsequently incubated with secondary antibody [GTVision I; 1:500;
Gene Science and Technology (Shanghai) Co., Ltd.] for 1 h at room
temperature. SULT1A2 expression was detected using a DAB detection
system [Gene Science and Technology (Shanghai) Co., Ltd.]. The
slides were visualized and captured at x400 magnification (Axio
Imager. Z2 fluorescence microscope; ZEISS).
IHC staining was assessed using a semi-quantitative
scoring method (15) by recording
both the area of positive staining and the staining intensity. The
area of positive staining was scored as follows: 0, 0%; 1, 1-25%;
2, 26-50%; 3, 51-75% and 4, >75%. The staining intensity was
defined as follows: 0, no staining; 1, weak staining; 2, moderate
staining and 3, strong staining. The immunoreactivity score (IHS)
was calculated by multiplying the positive area score by the
staining intensity score. An IHS <8 was classified into the low
expression group, while an IHS ≥8 was classified into the high
expression group.
Tissue microarray
A tissue microarray from FFPE tissues containing 55
BC tissue spots (item no. HBlaU066Su01; Shanghai Xinchao Biological
Technology Co., Ltd.) was used to detect SULT1A2 protein expression
via IHC analysis.
RT-qPCR
Total RNA was extracted from tissues or cells using
TRIzol® reagent (Thermo Fisher Scientific, Inc.),
according to the manufacturer's protocol, and reverse transcribed
into cDNA using the TransScript All-in-One First-Strand cDNA
Synthesis SuperMix (TransGen Biotech Co., Ltd.) according to the
manufacturer's protocol. qPCR was subsequently performed using the
Fast SYBR Green PCR Master Mix on a Step-One Fast Real-time PCR
System (both purchased from Thermo Fisher Scientific, Inc.). qPCR
conditions were as follows: 95˚C for 30 sec, followed by 40 cycles
at 95˚C for 5 sec, 60˚C for 34 sec and 95˚C for 15 sec. The primer
sequences used for qPCR are listed in Table I. Each sample was run in triplicate.
The average CT values of each target gene are then compared to the
internal reference gene GAPDH CT values. The formulas were used in
relative quantitative analysis: Change Fold=2-∆∆CT;
∆∆CT=∆CT test-∆CT con (16).
 | Table IPrimer sequences used for quantitative
PCR. |
Table I
Primer sequences used for quantitative
PCR.
| Gene | Forward primer
(5'-3') | Reverse primer
(5'-3') |
|---|
| SULT1A2 |
TACTTTGCAGAGGCACTGGG |
CGCCCTGGTAGATCATGTCC |
| GAPDH |
TGTGGGCATCAATGGATTTGG |
ACACCATGTATTCCGGGTCAAT |
Western blotting
Both frozen tissues and cells were used for Western
blotting. Total protein was extracted using RIPA buffer (cat. no.
R0278; Sigma-Aldrich; Merck KGaA). Total protein was quantified
using the BCA Protein Quantitation Assay kit (Takara Bio, Inc.) and
40 µg protein/lane was separated by 10% SDS-PAGE. The separated
proteins were subsequently transferred onto PVDF membranes
(Sigma-Aldrich; Merck KGaA) and blocked with 5% bovine serum
albumin (Sigma-Aldrich; Merck KGaA) in Tris-buffered saline
containing 0.1% Tween-20 for 1 h at room temperature. The membranes
were incubated with primary antibodies against SULT1A2 (HPA051051;
1:200; Sigma-Aldrich; Merck KGaA) and β-actin (cat. no. 4970;
1:1,000; Cell Signaling Technology, Inc.) overnight at 4˚C.
Membranes were washed with Tris-buffered saline containing 0.1%
Tween-20 for 30 min and subsequently incubated with Anti-rabbit
IgG, HRP-conjugated secondary antibodies (cat. no. 7074; 1:1,000;
Cell Signaling Technology, Inc.) for 1 h at room temperature.
Membranes were re-washed with TBST for 30 min, and protein bands
were visualized using the ECL western blotting detection system
(Bio-Rad Laboratories, Inc.). Protein bands were analyzed using
ImageJ software (version 1.51e; National Institutes of Health).
High-throughput data processing
The RNA-Seq data and clinical data for the BC
samples were downloaded from The Cancer Genome Atlas (TCGA;
http://gdc.cancer.gov) database. The microarray
data based on the Affymetrix platform were downloaded from the Gene
Expression Omnibus (GEO) database (http://www.ncbi.nlm.nih.gov/geo/; GSE3167: Tumor,
n=46; normal, n=14 and GSE68020: Tumor, n=30; normal, n=20;
GSE3167: NMIBC, n=33; MIBC, n=13 and GSE120736: NMIBC, n=84; MIBC,
n=61) (17,18). The data from TCGA database were log2
transformed, and the results were analyzed using Microsoft Excel
2019 (Microsoft Corporation) and GraphPad Prism 6 software
(GraphPad Software, Inc.).
Detection of biological pathways and
internal mechanism
‘ClusterProfiler’ R language packages (version 3.8;
http://www.bioconductor.org) and ‘DOSE’
R language packages (version 3.5; http://www.bioconductor.org) were used to perform
pathway enrichment analysis and Disease Ontology (DO) annotation to
investigate the pathways and biological parameters associated with
SULT1A2, respectively. The samples in the GSE3167 dataset were
separated into high and low expression groups, according to median
SULT1A2 expression. Differentially expressed genes were determined
using the ‘limma’ R package (version 3.12; http://www.bioconductor.org), and an adjusted
P<0.05 was selected as the threshold for enriched terms. To
determine the function of SULT1A2 in BC, gene set enrichment
analysis (GSEA; version 2.2.4 jar software; http://software.broadinstitute.org/gsea/downloads.jsp)
was performed to identify pathways that were associated with
SULT1A2. The gene sets with normalized using an enrichment score of
>1, P-value <0.05 and false discovery rate value <0.25,
which were regarded as significantly enriched gene sets. The Kyoto
Encyclopedia of Genes and Genomes (KEGG) database (http://www.genome.ad.jp/kegg/kegg2.html)
was used to identify biological pathways and DO annotation was
performed to assess the associations between genes and diseases.
Gene Ontology (GO) enrichment analysis was also performed to
determine the biological functions in BC, and the associated
biological processes, molecular functions and cellular components
were identified.
Statistical analysis
Statistical analysis was performed using SPSS 17.0
software (SPSS, Inc.), GraphPad Prism 6 software (GraphPad
Software, Inc.) and R 3.5.0 software (https://www.r-project.org). The ‘survminer’ R package
(version 0.4.8; http://www.sthda.com/english/rpkgs/survminer/) was
used to draw survival curves. The Kaplan-Meier method and log-rank
test were used to assess overall survival (OS) rate of patients in
the high and low expression groups. Each experiment was repeated in
triplicate. Data are presented as the mean ± standard error of the
mean or standard deviation. Paired Student's t-test was used to
compare differences between two groups, while one-way ANOVA
followed by Tukey's post hoc test was used to compare differences
between multiple groups. P<0.05 was considered to indicate a
statistically significant difference.
Results
SULT1A2 is highly expressed in BC
tissues and cells compared with normal bladder tissues and
cells
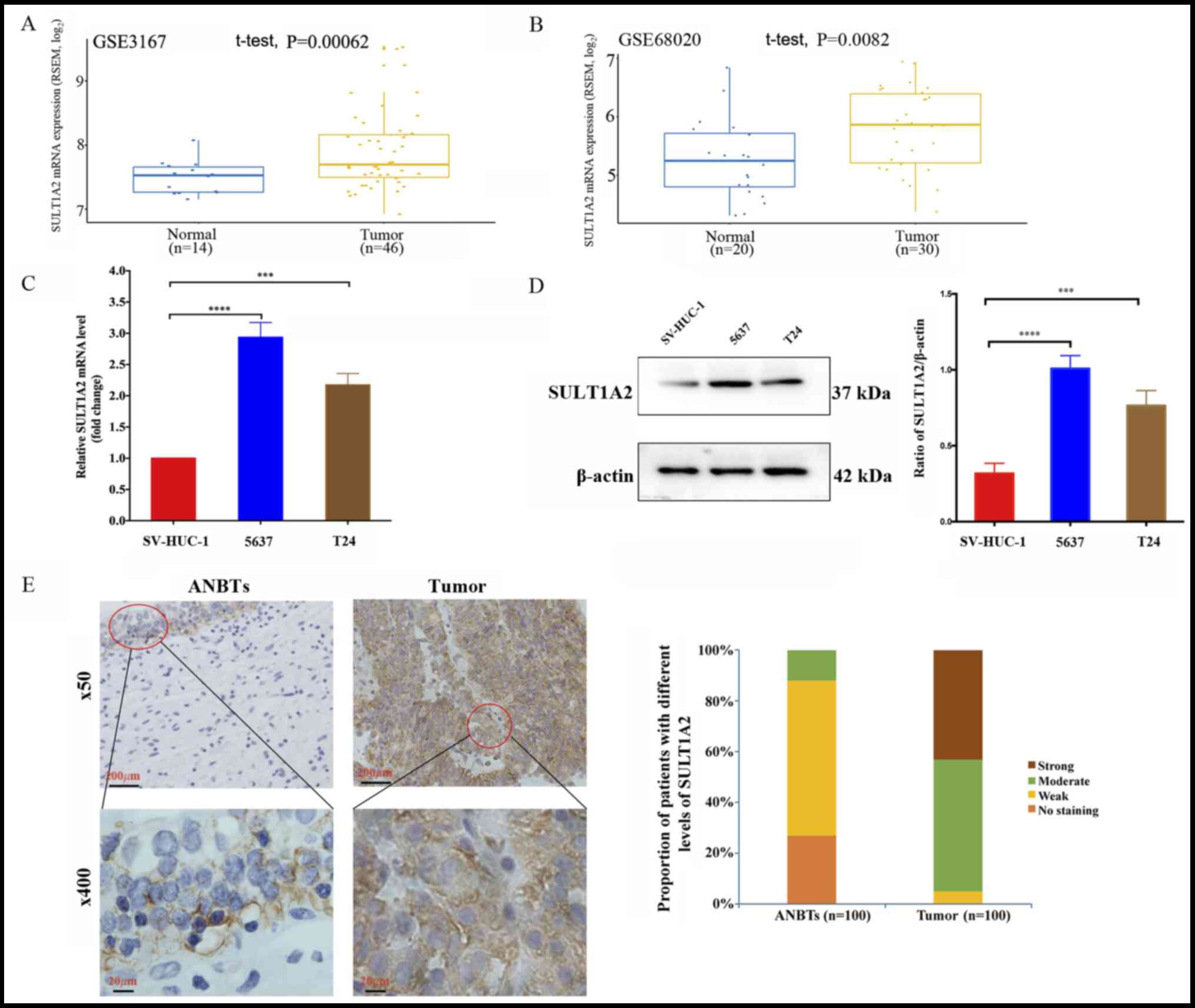
To determine the clinical significance of SULT1A2 in
BC, datasets from the GEO database were used to assess SULT1A2
expression. The results demonstrated that SULT1A2 expression was
significantly higher in BC tissues compared with normal bladder
tissues (Fig. 1A, P<0.001 and
1B, P<0.01). RT-qPCR and western
blot analyses were subsequently performed to detect SULT1A2 mRNA
and protein expression levels in BC cells and normal bladder cells,
respectively. The results demonstrated that SULT1A2 expression was
significantly higher in BC cells compared with normal bladder cells
(Fig. 1C, P<0.001 and 1D, P<0.001). IHC analysis was performed
to detect SULT1A2 expression in FFPE BC tissues (n=100) and
corresponding ANBTs (n=100). SULT1A2 was prominently located in the
cytoplasm and was moderately or highly expressed in most FFPE BC
tissues, whereas it was undetected or weakly expressed in the
majority of ANBTs (Fig. 1E).
Collectively, these results suggest that SULT1A2 is highly
expressed in BC tissues and cells compared with normal bladder
tissues and cells.
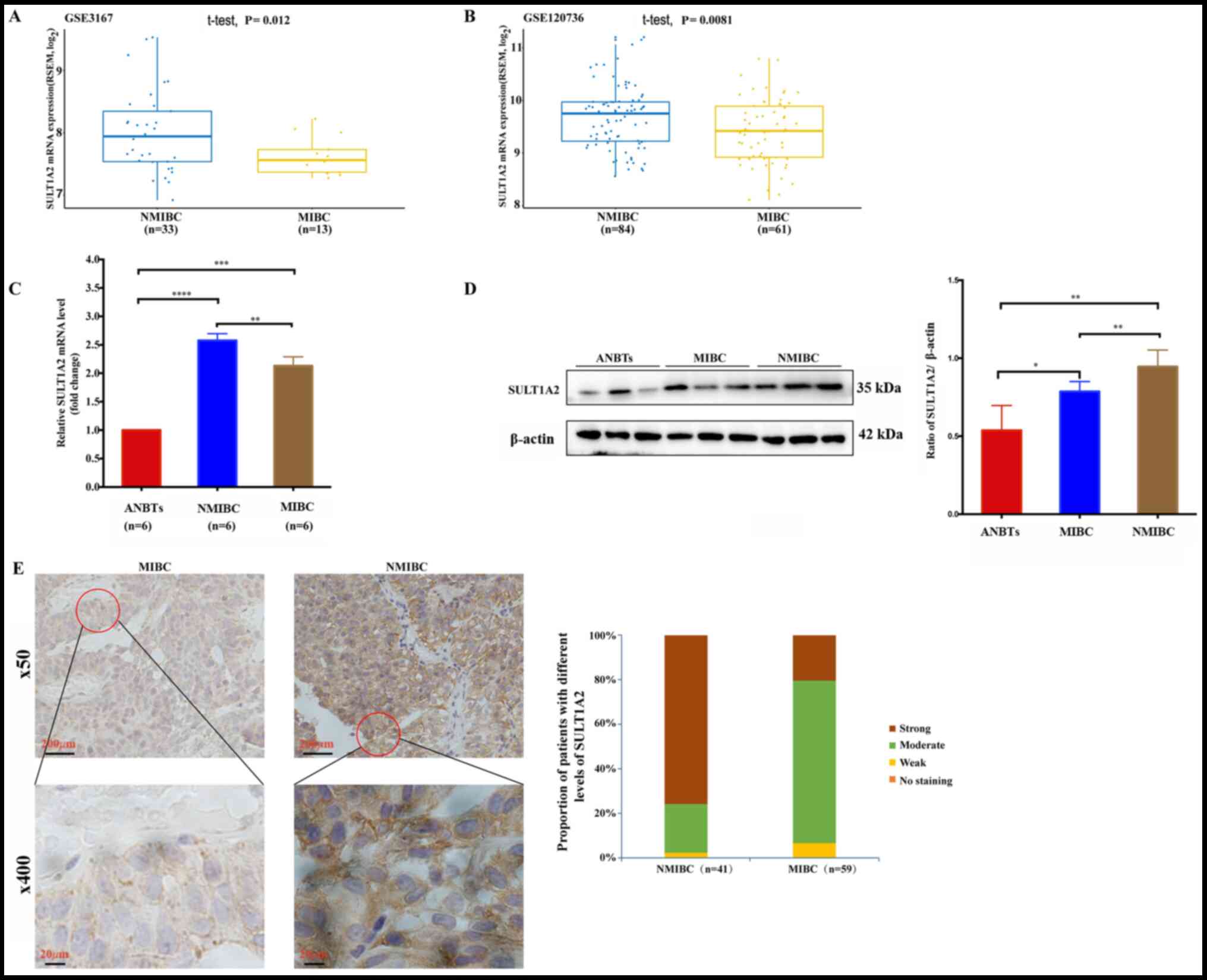
SULT1A2 is associated with the staging
of BC
Our studies demonstrate that SULT1A2 expression is
significantly higher in BC tissues and cells compared with ANBTs
and cells. Data from the GEO database was further analyzed to
investigate the association between SULT1A2 expression and the
clinicopathological characteristics of BC. The results demonstrated
that SULT1A2 mRNA expression was significantly higher in NMIBC
tissues compared with MIBC tissues (Fig. 2A, P<0.05 and 2B, P<0.01). Subsequently, reverse
transcription-quantitative PCR and western blot analyses were
performed to detect SULT1A2 mRNA and protein expression levels at
different stages of frozen BC tissues (n=12) and corresponding
ANBTs (n=6). The results demonstrated that SULT1A2 mRNA and protein
expression levels were significantly higher in frozen BC tissues
compared with ANBTs, and SULT1A2 expression levels were
significantly elevated in NMIBC tissues compared with MIBC tissues
(Fig. 2C, P<0.01 and 2D, P<0.05). IHC analysis was performed
to detect SULT1A2 expression in FFPE BC tissues, with NMIBC and
MIBC. The results demonstrated that SULT1A2 protein expression was
significantly higher in NMIBC tissues compared with MIBC tissues
(Fig. 2E, P<0.01). Taken
together, these results suggest that SULT1A2 expression is
associated with BC stages.
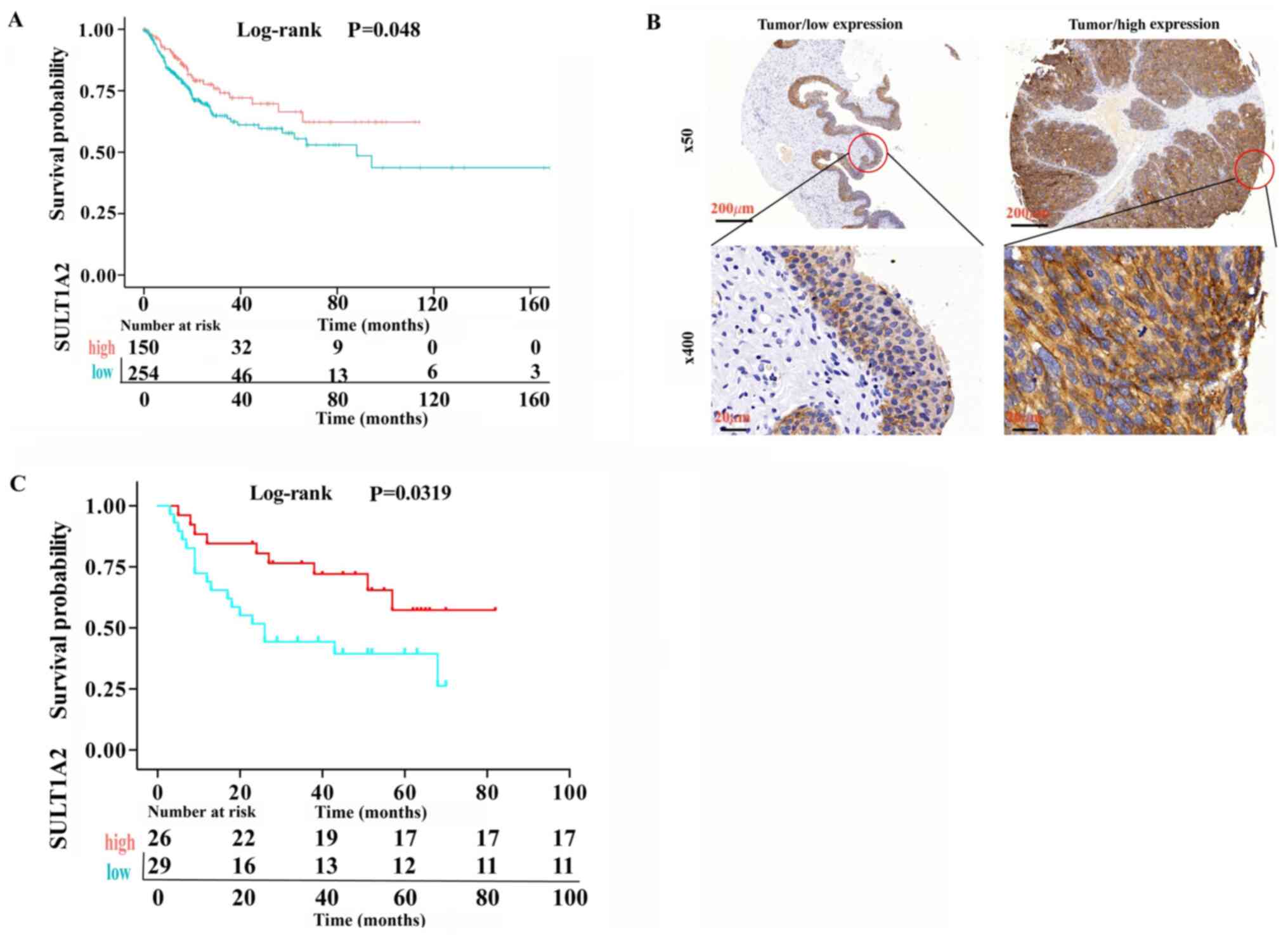
High SULT1A2 expression predicts
better prognosis in patients with BC
Patients in TCGA dataset were divided into two
groups (high and low expression groups), based on median SULT1A2
expression. Kaplan-Meier OS curves were constructed and the
log-rank test was used to determine statistical significance. The
results demonstrated that patients with high SULT1A2 expression had
a better prognosis for long-term survival (Fig. 3A, P<0.05). IHC analysis was
performed using the BC tissue microarray (n=55) to validate the
results and determine the prognostic value of SULT1A2 in patients
with BC. The results demonstrated that SULT1A2 was highly expressed
in 26/55 BC tissues, and patients with high SULT1A2 expression had
a better prognosis for long-term survival (Fig. 3B and C, P<0.05), which was consistent with
TCGA analysis. Collectively, these results suggest that SULT1A2
expression is positively associated with survival in patients with
BC.
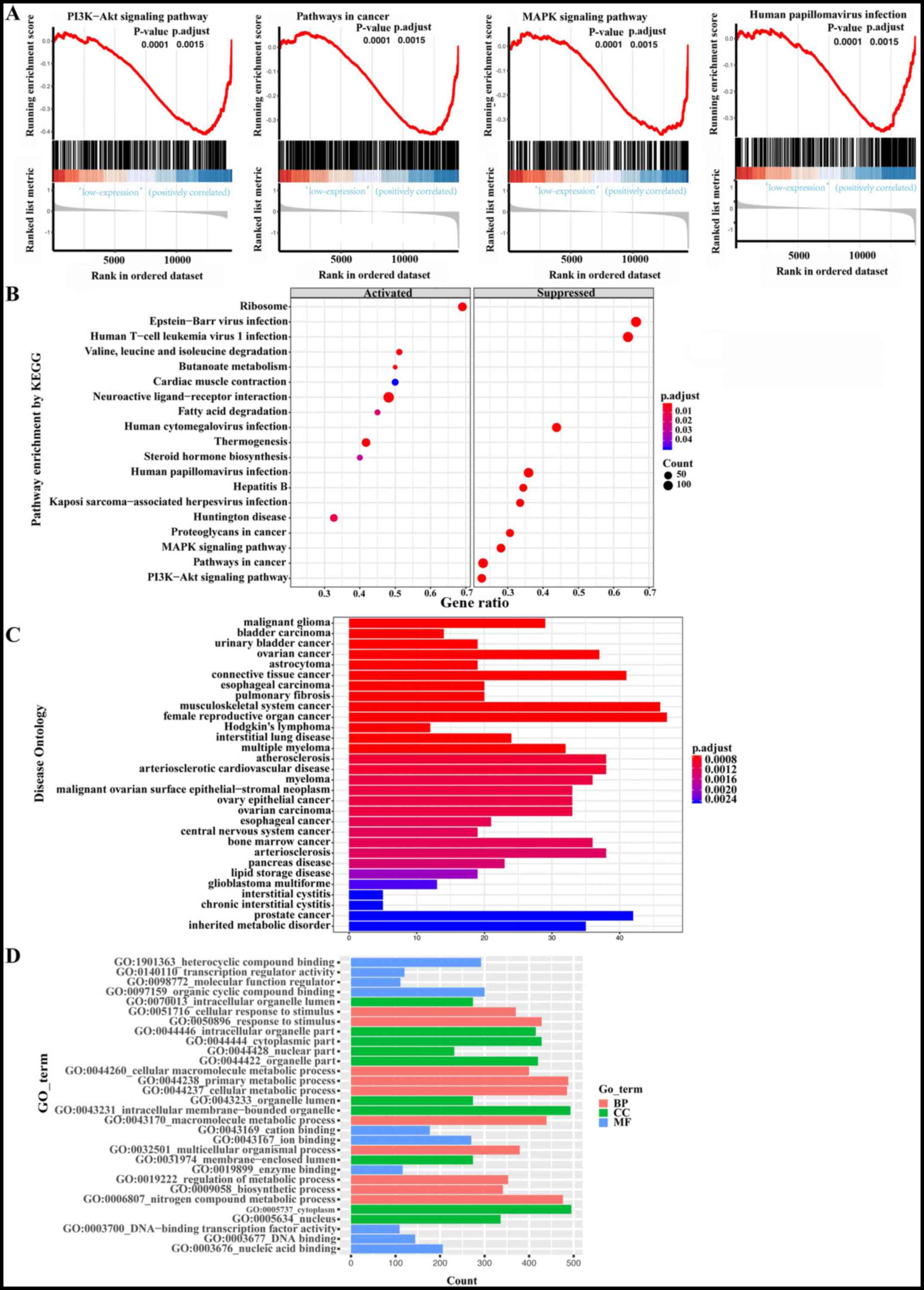
Functional analysis of SULT1A2
To determine the function of SULT1A2 in BC, gene set
enrichment analysis was performed to identify pathways that are
associated with SULT1A2. BC-related pathways were associated with
SULT1A2, including the PI3K-Akt signaling pathway (P=0.000141804),
pathways in cancer (P=0.000132979), the MAPK signaling pathway
(P=0.000145243) and human papillomavirus (HPV) infection
(P=0.000144092) (Fig. 4A). Previous
studies have demonstrated that these pathways are closely
associated with the occurrence and development of BC (19,20).
In addition, other important pathways associated with SULT1A2 were
also discovered (Fig. 4B). To
further confirm the molecular functions of SULT1A2, enriched DO and
GO terms were identified. DO analysis demonstrated that BC is one
of the most closely associated diseases to SULT1A2 (Fig. 4C). GO analysis demonstrated that
SULT1A2 variation in BC results in changes in biosynthetic
processes (P<0.001), the regulation of the metabolic processes
(P<0.001), the nucleus (P<0.001) and DNA binding (P<0.05)
(Fig. 4D).
Discussion
Although SULT1A2 can catalyze the bioactivation of
several procarcinogens (12), a
previous study has suggested that the SULT1A2 transcript has a
splicing defect that may prevent it from becoming translated into
protein (21), in which case
SULT1A2 is considered a pseudogene. Another study has screened
several cytosolic fractions from different tissues, including
tumors, and SULT1A2 expression was undetected (12). In addition, a molecular
epidemiological study has concluded that SULT1A2 has no association
with the risk of liver, colon, lung, oral, gastric, renal, cervical
or breast cancer (22). SULT1A2
does not appear to play a role in carcinogenesis and cancer
development; however, it is associated with the early onset of
breast cancer and mediated biotransformation in the breast
(12). Ongoing research conducted
by the present authors has demonstrated that SULT1A2 expression
significantly changes in BC, but not in other SULT isoforms (data
not shown). The present study aimed to investigate the role of
SULT1A2 in BC using cancer cells, FFPE cancer tissues and frozen
cancer tissues. The results demonstrated that SULT1A2 mRNA and
protein expression levels were significantly higher in BC cells and
tissues compared with normal bladder cells and corresponding ANBTs.
In addition, SULT1A2 expression levels were significantly higher in
NMIBC tissues compared with MIBC tissues. Notably, patients with
high SULT1A2 protein expression have a good prognosis for long-term
survival. Analyses using TCGA and GEO databases indicated that
SULT1A2 mRNA expression was higher in early stage BC compared with
advanced stage BC, and patients with high SULT1A2 mRNA expression
had a better prognosis for long-term survival than those with low
SULT1A2 expression. These results confirm that SULT1A2 is expressed
in human bladder tissues, particularly in BC tissues, and SULT1A2
expression is associated with the classification and prognosis of
BC.
The results of the present study demonstrated that
SULT1A2 is activated during all phases of BC and that activation of
SULT1A2 is a frequent event in tumor progression and metastasis.
Given that metastatic disease is the principal cause of mortality
in patients with cancer (23), a
better understanding of tumor invasion and metastasis is essential
to identify novel therapeutic targets. Increasing evidence suggest
that the pathways in cancer not only have a direct role in tumor
invasion by degrading extracellular matrix protein, but they also
play an important role in maintaining the tumor microenvironment,
thus promoting tumor growth (24,25). A
previous study demonstrated that PI3K and MAPK signaling, belonging
to the pathways in cancer, are one of the three main pathways
frequently dysregulated in BC (1).
Activation of the PI3K/Akt and MAPK signaling pathways mediates BC
invasion (26). A previous study
has implicated that the p38 MAPK and PI3K/AKT signaling pathways
may be responsible for MMP-2/-9 expression regulating the
migratory/invasive capacity of BC cells (27). The MAPK signaling pathway also
affects the invasive ability of human BC cells via the downstream
signal AP-1, impeding the transition of cells from the
G1 phase to the S phase, and mediating
epithelial-to-mesenchymal transition (28,29).
Whole-genome and RNA sequencing identified potential therapeutic
targets in 69% of BCs, including 42% with targets in the PI3K/AKT
pathway and 45% with targets in the MAPK pathway (1). Activation of the epidermal growth
factor receptor (EGFR) and downstream signaling pathways, including
PI3K/Akt and MAPK, induces resistance to EGFR-targeted therapy in
BC (26). Although chromosomal
alterations involved in the PI3K/AKT signaling pathway play a major
role in the effectiveness of targeted therapy (30), targeting the two major signaling
pathways remains an important therapeutic approach for BC.
The results of the present study suggest that the
pathways in cancer, the MAPK signaling pathway, and the PI3K/Akt
signaling pathway have a negative association with the SULT1A2 gene
in BC, which indicates that SULT1A2 may be a protector by
decreasing the proliferation and metastasis of cancer cells via
downregulation of these signaling pathways. GO enrichment and KEGG
pathway analyses were performed to elucidate the carcinogenesis and
progression of BC. SULT1A2 may have two roles in BC by affecting
biosynthetic processes, metabolic process, the nucleus and DNA
binding through the pathways of cancer, including the MAPK and
PI3K/Akt signaling pathways. The current study speculated that when
SULT1A2 expression increases to a certain threshold, carcinogenesis
is activated; if it sufficiently increases to reach another
threshold, a protective effect is activated. This can explain the
upregulated expression of SULT1A2 in BC, in which SULT1A2
expression is higher in the early/noninvasive stage compared with
the advanced/invasive stage. Given that the early stage of BC
recurs in 50-70% of patients, the effective therapeutic control of
cancer recurrence is required at an early stage (31). Thus, SULT1A2 may be used as a novel
therapeutic target in early BC.
The results of the present study demonstrated that
SULT1A2 is associated with HPV infection. HPV is a risk factor for
penile cancer; however, its role in BC remains unclear. High-risk
HPVs are the primary causative agents of carcinomas (32). The prevalence of high-risk HPV in BC
varies, particularly in Moroccan patients, with the highest
prevalence of 52.4% (33). However,
clinical trials have reported that HPV is not associated with the
risk of BC (34,35). Recently, Weinstein et al
(36) identified that high-risk HPV
may play a role in the development of a small percentage of BCs. It
was demonstrated that only one BC tissue expressed HPV16, a
high-risk HPV (36), in 122 cases;
however, the HPV16 virus integrated into an apoptosis-regulating
gene (BCL2L1) and induced it to be amplified and significantly
overexpressed (1). Moonen et
al (37) demonstrated a
positive association between cancer stage and high-risk HPV DNA.
Given that SULT1A2 is closely associated with BC, it was speculated
that SULT1A2 may be involved in the development of BC via HPV
infection. However, further studies are required to verify this
assumption.
The present study is not without limitations. First,
SULT1A2 expression was assessed in 100 FFPE BC tissues and
corresponding ANBTs at the protein level but not the genomic level.
If high-throughput data processing were used in the 100 samples and
corresponding ANBTs, the results would be more reliable. Secondly,
the present study failed to exhibit the results of some of the
SULT1A2 regulatory pathways. The research is ongoing (data not
shown), which will be time consuming and require additional
financial resources. Based on the present study, SULT1A2 plays a
protective role in the development of BC; however, the cell
phenotype was not verified. In addition, further studies are
required to assess the effect of overexpressing SULT1A2 on the
proliferation and invasion of BC cells.
In conclusion, the results of the present study
demonstrated that SULT1A2 was highly expressed in BC tissues and
significantly associated with the staging of BC. In addition, high
SULT1A2 expression was significantly associated with overall
survival of patients with BC, and SULT1A2 was associated with
BC-related pathways and biosynthetic processes. Thus, SULT1A2 may
act as an oncogene in BC, and serve as a biomarker for tumor
staging and prognosis in patients with BC.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Youth Program of
The National Natural Science Foundation of China (No.
81900092).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JS designed the present study. YC performed the
experiments. YC and QO acquired and analyzed the data. YC drafted
and revised the manuscript for important intellectual content. All
authors have read and approved the final manuscript. JS and YC
confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Ethics Committee for Clinical Research and Animal Trials of the
First Affiliated Hospital of Sun Yat-sen University [approval no.
(2016)067, Guangzhou, China]. Written informed consent was provided
by all patients prior to the study start.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cancer Genome Atlas Research Network.
Comprehensive molecular characterization of urothelial bladder
carcinoma. Nature. 507:315–322. 2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Figueroa JD, Malats N, García-Closas M,
Real FX, Silverman D, Kogevinas M, Chanoc S, Welch R, Dosemeci M,
Lan Q, et al: Bladder cancer risk and genetic variation in AKR1C3
and other metabolizing genes. Carcinogenesis. 29:1955–1962.
2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Schulster M: Bladder cancer academy 2019
selected summaries. Rev Urol. 21:23–28. 2019.PubMed/NCBI
|
|
4
|
Vlachostergios PJ and Faltas BM: The
molecular limitations of biomarker research in bladder cancer.
World J Urol. 37:837–848. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Dong D, Ako R and Wu B: Crystal structures
of human sulfotransferases: Insights into the mechanisms of action
and substrate selectivity. Expert Opin Drug Metab Toxicol.
8:635–646. 2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kauffman FC: Conjugation-deconjugation
reactions in drug metabolism and toxicity. Fed Proc. 46:2434–2445.
1987.PubMed/NCBI
|
|
7
|
Cole P, Monson RR, Haning H and Friedell
GH: Smoking and cancer of the lower urinary tract. N Engl J Med.
284:129–134. 1971.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Cole P, Hoover R and Friedell GH:
Occupation and cancer of the lower urinary tract. Cancer.
29:1250–1260. 1972.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Sabbioni G, Jones CR, Sepai O, Hirvonen A,
Norppa H, Järventaus H, Glatt H, Pomplun D, Yan H, Brooks LR, et
al: Biomarkers of exposure, effect, and susceptibility in workers
exposed to nitrotoluenes. Cancer Epidemiol Biomarkers Prev.
15:559–566. 2006.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Arlt VM, Stiborova M, Henderson CJ,
Osborne MR, Bieler CA, Frei E, Martinek V, Sopko B, Wolf CR,
Schmeiser HH and Phillips DH: Environmental pollutant and potent
mutagen 3-nitrobenzanthrone forms DNA adducts after reduction by
NAD(P)H:quinone oxidoreductase and conjugation by
acetyltransferases and sulfotransferases in human hepatic cytosols.
Cancer Res. 65:2644–2652. 2005.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Sidorenko VS, Attaluri S, Zaitseva I, Iden
CR, Dickman KG, Johnson F and Grollman AP: Bioactivation of the
human carcinogen aristolochic acid. Carcinogenesis. 35:1814–1822.
2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Nowell S, Green B, Tang YM, Wiese R and
Kadlubar FF: Examination of human tissue cytosols for expression of
sulfotransferase isoform 1A2 (SULT1A2) using a SULT1A2-specific
antibody. Mol Pharmacol. 67:394–399. 2005.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Svendsen C, Meinl W, Glatt H, Alexander J,
Knutsen HK, Hjertholm H, Rasmussen T and Husøy T: Intestinal
carcinogenesis of two food processing contaminants,
2-amino-1-methyl-6-phenylimidazo[4,5-b]pyridine and
5-hydroxymethylfurfural, in transgenic FVB min mice expressing
human sulfotransferases. Mol Carcinog. 51:984–992. 2012.PubMed/NCBI View
Article : Google Scholar
|
|
14
|
Sanli O, Dobruch J, Knowles MA, Burger M,
Alemozaffar M, Nielsen ME and Lotan Y: Bladder cancer. Nat Rev Dis
Primers. 3(17022)2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Situ DR, Hu Y, Zhu ZH, Wang J, Long H and
Rong TH: Prognostic relevance of β-catenin expression in T2-3N0M0
esophageal squamous cell carcinoma. World J Gastroenterol.
16:5195–5202. 2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Regier N and Frey B: Experimental
comparison of relative RT-qPCR quantification approaches for gene
expression studies in poplar. BMC Mol Biol. 11(57)2010.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Song Y, Jin D, Ou N, Luo Z, Chen G, Chen
J, Yang Y and Liu X: Gene expression profiles identified novel
urine biomarkers for diagnosis and prognosis of high-grade bladder
urothelial carcinoma. Front Oncol. 10(394)2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Huang YD, Shan W, Zeng L and Wu Y:
Screening of differentially expressed genes related to bladder
cancer and functional analysis with DNA microarray. Asian Pac J
Cancer Prev. 14:4553–4557. 2013.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Heidegger I, Borena W and Pichler R: The
role of human papilloma virus in urological malignancies.
Anticancer Res. 35:2513–2519. 2015.PubMed/NCBI
|
|
20
|
Kachrilas S, Dellis A, Papatsoris A,
Avgeris S, Anastasiou D, Gavriil A, Horti M, Tseleni Balafouta S,
Livadas K, Stravopodis DJ, et al: PI3K/AKT pathway genetic
alterations and dysregulation of expression in bladder cancer. J
BUON. 24:329–337. 2019.PubMed/NCBI
|
|
21
|
Liu J, Li H, Shen S, Sun L, Yuan Y and
Xing C: Alternative splicing events implicated in carcinogenesis
and prognosis of colorectal cancer. J Cancer. 9:1754–1764.
2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Peng CT, Chen JC, Yeh KT, Wang YF, Hou MF,
Lee TP, Shih MC, Chang JY and Chang JG: The relationship among the
polymorphisms of SULT1A1, 1A2 and different types of cancers in
Taiwanese. Int J Mol Med. 11:85–89. 2003.PubMed/NCBI
|
|
23
|
McGowan PM, Kirstein JM and Chambers AF:
Micrometastatic disease and metastatic outgrowth: Clinical issues
and experimental approaches. Future Oncol. 5:1083–1098.
2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Ahmad A, Wang Z, Kong D, Ali S, Li Y,
Banerjee S, Ali R and Sarkar FH: FoxM1 down-regulation leads to
inhibition of proliferation, migration and invasion of breast
cancer cells through the modulation of extra-cellular matrix
degrading factors. Breast Cancer Res Treat. 122:337–346.
2010.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Liguori M, Solinas G, Germano G, Mantovani
A and Allavena P: Tumor-associated macrophages as incessant
builders and destroyers of the cancer stroma. Cancers (Basel).
3:3740–3761. 2011.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Kassouf W, Dinney CP, Brown G, McConkey
DJ, Diehl AJ, Bar-Eli M and Adam L: Uncoupling between epidermal
growth factor receptor and downstream signals defines resistance to
the antiproliferative effect of Gefitinib in bladder cancer cells.
Cancer Res. 65:10524–10535. 2005.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Kumar B, Koul S, Petersen J, Khandrika L,
Hwa JS, Meacham RB, Wilson S and Koul HK: p38 mitogen-activated
protein kinase-driven MAPKAPK2 regulates invasion of bladder cancer
by modulation of MMP-2 and MMP-9 activity. Cancer Res. 70:832–841.
2010.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Zhao L, Zhang T, Geng H, Liu ZQ, Liang ZF,
Zhang ZQ, Min J, Yu DX and Zhong CY: MAPK/AP-1 pathway regulates
benzidine-induced cell proliferation through the control of cell
cycle in human normal bladder epithelial cells. Oncol Lett.
16:4628–4634. 2018.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Sun X, Zhang T, Deng Q, Zhou Q, Sun X, Li
E, Yu D and Zhong C: Benzidine induces epithelial-mesenchymal
transition of human bladder cancer cells through activation of ERK5
pathway. Mol Cells. 41:188–197. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Houédé N and Pourquier P: Targeting the
genetic alterations of the PI3K-AKT-mTOR pathway: Its potential use
in the treatment of bladder cancers. Pharmacol Ther. 145:1–18.
2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Khadjavi A, Mannu F, Destefanis P,
Sacerdote C, Battaglia A, Allasia M, Fontana D, Frea B, Polidoro S,
Fiorito G, et al: Early diagnosis of bladder cancer through the
detection of urinary tyrosine-phosphorylated proteins. Br J Cancer.
113:469–475. 2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Douglawi A and Masterson TA: Updates on
the epidemiology and risk factors for penile cancer. Transl Androl
Urol. 6:785–790. 2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Berrada N, Al-Bouzidi A, Ameur A, Abbar M,
El-Mzibri M, Ameziane-El-Hassani R, Benbacer L, Khyatti M, Qmichou
Z, Amzazi S and Attaleb M: Human papillomavirus detection in
Moroccan patients with bladder cancer. J Infect Dev Ctries.
7:586–592. 2013.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Alexander RE, Hu Y, Kum JB, Montironi R,
Lopez-Beltran A, Maclennan GT, Idrees MT, Emerson RE, Ulbright TM,
Grignon DG, et al: p16 expression is not associated with human
papillomavirus in urinary bladder squamous cell carcinoma. Mod
Pathol. 25:1526–1533. 2012.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Polesel J, Gheit T, Talamini T, Shahzad N,
Lenardon O, Sylla B, La Vecchia C, Serraino D, Tommasino M and
Franceschi S: Urinary human polyomavirus and papillomavirus
infection and bladder cancer risk. Br J Cancer. 106:222–226.
2012.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Weinstein SJ, Ziegler RG, Selhub J, Fears
TR, Strickler HD, Brinton LA, Hamman RF, Levine RS, Mallin K and
Stolley PD: Elevated serum homocysteine levels and increased risk
of invasive cervical cancer in US women. Cancer Causes Control.
12:317–324. 2001.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Moonen PM, Bakkers JM, Kiemeney LA,
Schalken JA, Melchers WJ and Witjes JA: Human papilloma virus DNA
and p53 mutation analysis on bladder washes in relation to clinical
outcome of bladder cancer. Eur Urol. 52:464–468. 2007.PubMed/NCBI View Article : Google Scholar
|