Introduction
Pulmonary aspergillosis is a lung disease secondary
to the presence of a ubiquitous germ, Aspergillus fumigatus,
which occurs mainly in immunodeficient individuals. Aspergillus
fumigatus is often the most blamed fungus in Aspergillosis lung
injuries. It is a ubiquitous germ that can be aggressive through
systemic reactions, as well as local or disseminated development.
There are five described anatomo-clinical forms. The allergic
bronchopulmonary form involves the development of the germ in
conditions of asthma or bronchiectasis with the onset of allergic
immunological reactions. Another non-invasive type is the localized
form of pulmonary aspergilloma, which is found in the development
of mycetoma in conditions of localized pulmonary emphysema or
intraparenchymal cavernous lesions, where it finds optimal
conditions for development (humidity, darkness and lack of
ventilation) (1-3).
The extreme form of local invasion is chronic necrotizing
aspergillosis with extensive pleuropulmonary injuries (4-6).
The systemic extensive form in immunosuppressed individuals is
represented by invasive pulmonary aspergillosis (7-9).
A form of hypersensitivity pneumonia caused by inhalation of
aspergillus particles is also described (10).
The localized form of pulmonary or chronic
necrotizing aspergillosis has a high lethal potential outcome, both
by progressively induced respiratory failure and by possible
acute-associated complications, including pulmonary suppuration and
hemoptysis. Aspergilloma usually occurs in old post-tuberculosis
lung cavernous lesions (1-5,11,12).
Through recurrent infections with periods of pulmonary suppuration
and remission, additional parenchyma is recruited with each
exacerbation, functionally excluding new parenchymal areas. In
addition, by releasing endotoxins, the hypertrophy of the local
bronchial vascularization is stimulated until they rupture and
trigger hemoptysis, a complication with high immediate lethal risk
by pulmonary flooding; it exposes the lesion to superinfection
(13-18).
In the case presented in this study, the patient
successfully underwent cavernostomy, a potentially effective and
safe method for cases with life-threatening hemoptysis in which
lung resection is not feasible.
Case report
Approval for the case report was obtained from the
Ethics Committee of ‘Marius Nasta’ National Institute of
Pneumology, Bucharest, Romania (no. 152/2020). Written informed
consent was signed by the patient on 13.05.2020.
A patient with low social status, former smoker with
a history of left pulmonary tuberculosis, cachexia, was admitted
into the Department of Thoracic Surgery, ‘Marius Nasta’ National
Institute of Pneumology, having presented repeated mild hemoptysis
in the previous 3 weeks, bronchial suppurative phenomena and
worsening respiratory failure manifesting through shortness of
breath and hypoxemia.
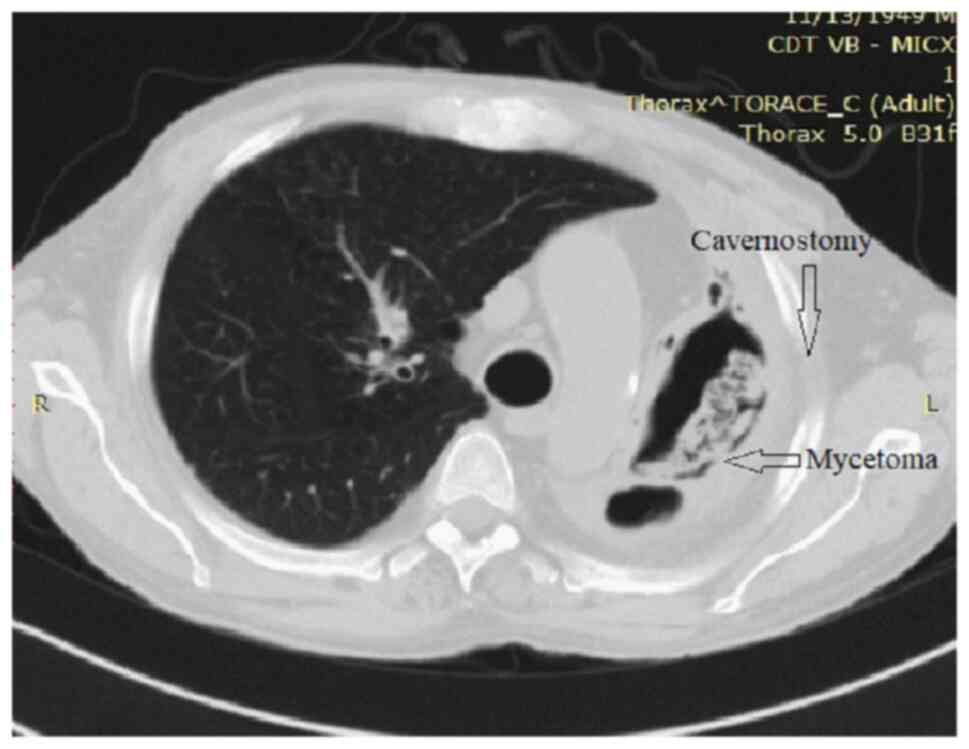
Chest X-ray revealed a left apical pulmonary cavity
(Fig. 1). The chest computed
tomography (CT) showed a culminal cavity surrounded by
consolidation, probably due to aspergillosis infection and
aspiration of blood (Fig. 2).
The bronchoscopy revealed an abnormal structure of
the left upper lobe bronchus, suppurative characteristics and
hemoptysis traces in the culminal bronchus. The bronchoscope
reached the aspergillary cavity; it revealed 9 mm diameter through
the upper left bronchus and culminal bronchus.
The pulmonary function test results indicated: FVC:
2.66 l, 74%, and FEV1: 800 ml after antibiotic treatment. The
arterial blood gas tests indicated a resting hypoxemia of 70 mmHg.
Considering the results, performing lung resection was not possible
due to the extremely high risks involved; therefore, another
procedure was necessary.
Preoperative care included embolization of the
bronchial arteries, in order to avoid hemoptysis in the
perioperative period. Antibiotic and antifungal treatment regarding
the suppurative phenomena was established based on the
antibiogram.
The therapeutic procedure of choice was Monaldi
Cavernostomy, in optimal conditions. The procedure was carried out
in the left axillary region, consisting of 4 lateral sections of
the ribs resected (3-6),
guided by peripheral contact of the cavern with the thoracic wall.
Removal of the adjacent thickened pleura was performed, creating an
opening, followed by removal of the mycetoma, cavity lavage and the
identification of multiple bronchial fistulas inside the cavity
(Fig. 3).
The next step was determined by musculocutaneous
flap to pleuropulmonary edge suture. No per primam suture of the
fistulas was intended. Slightly compressive bandage was performed
to enable aerial drainage of the bronchial fistulas. Subsequently,
daily dressing of the wound was practiced. Antibiotic treatment,
including antifungal treatment, was maintained for 3 weeks.
Furthermore, after 3 months, muscular myoplasty was
necessary in order to fill in the cavity, to favor the closure of
the remaining fistulas and a reopening of the skin stoma, which had
a tendency of closing.
After 1 year, the patient did not present any
episode of hemoptysis or suppurative process and no progressive
degradation of respiratory function. Difficulty in speaking was
present in the first two months after the surgery, being
ameliorated by adducting the upper limb at the level of the skin
stoma, due to major air losses through the bronchial fistulas. The
difficulties of local care, local dressing, initially with betadine
grooming and sterile dressing were overcome in approximately 3
weeks, the patient being independent after this period.
Discussion
The diagnosis of pulmonary aspergillosis is usually
based on imaging, with the typical radiological aspect of
intracavitary mycetoma being the Monod sign, especially in the
context of tuberculosis-related history and clinical manifestations
of recurrent hemoptysis. The bronchoscopy examination often reveals
chronic bronchial alterations and, through bronchial aspiration,
aspergillus fumigatus is identified (19,20).
The antifungal drug treatment is complementary to
the surgical treatment, in order to limit the local suppurative
effects (21-23).
In addition, hemostatic drugs such as lysine derivatives type are
used in order to decrease the postoperative hemorrhagic incidents,
given the increased risk of bleeding by specific pleuropulmonary
adhesions (13,24-26).
The interventional radiology treatment, the
embolization of the hypertrophied bronchial artery, has a temporary
effect (13,27) and it can be used preoperatively to
avoid suppurative or hemoptysis perioperative episodes. Single
embolization has a risk of recurrence of hemoptysis of over 50%
because the environmental conditions that allowed the development
of aspergilloma remain present (13,24).
The treatment of pulmonary aspergilloma in a single,
non-invasive form or in chronic pulmonary aspergillosis, as well as
the invasive form is a combined surgical, radiological and medical
treatment (13,21-28).
The therapeutic strategy is individualized for each patient
(2,24,28).
The ideal treatment is surgical, by removing the pulmonary caverns
or cavities with favorable conditions for fungal development, thus
excluding the maintenance factors of suppurative phenomenon or
recurrent massive hemoptysis (2,28). In
addition, adjusted procedures are recommended as much as possible,
avoiding remnants of affected lung tissue.
Whenever there is a patient with pre-existing
compromised lung function that makes lung resection not possible,
alternative surgical solutions should be considered. The purpose is
to abolish the pathological conditions for the development of this
fungus, such as lung caverns or superinfected air bubbles.
Cavernostomy, which represents the conservative
surgical treatment of invasive pulmonary aspergillosis, should be
considered in cases with a lung function that does not allow
pulmonary resection, but also in patients with comorbidities that
prevent them from benefiting from major lung resections, as in
pre-existing high-risk cardiovascular conditions (17,29-35).
Da Silva et al (36)
identified an indication for cavernostomy as the forms of chronic
invasive pulmonary aspergillosis that require
pleuropneumonectomy-fused intrapleurally with complete pulmonary
destruction or with bilateral forms, usually occurring in
immunocompromised patients or with modified clinical condition.
Therefore, it can be indicated even in those with permissive
respiratory function. The therapeutic objective is to abolish the
conditions that lead to the development of Aspergillus by
performing cavernostomy (34-36).
Cavernostomy is applied in selected cases with
peripherally cavernous lesions colonized with Aspergillus, in close
contact with the chest wall and its structures.
Height recommends closed drainage for 7-10 days,
with intracavitary lavage with antifungals in the preoperative
period (26).
It involves making an ‘H’-shaped skin incision
centered on the cavity or on the pleurotomy orifice of the
previously placed pleural drainage tube. The approach site is
usually axillary to the posterior axillary line for the lesions
found in the Fowler segment, but also interscapular vertebral
approach for posterior and even apical ones. In forms with
significant lung damage and remodeling, cavitary wall exposure
dictates drainage (34,37-39).
Musculocutaneous flaps are harvested and are then
attached to the pleuropulmonary edges of the cavern after the
resection of 2-3 costal segments and after the excision of the
exposed thickened pleura. Careful ligation of the affected
intercostal pedicles and careful hemostasis are practiced, given
the risk of hemorrhage secondary to adhesions and local vascular
hypertrophy.
The cavity is cleaned, removing the mycetoma and
identifying the bronchial fistulas.
The complete excision of the exposed thickened
pleura is performed while avoiding the creation of ‘pockets’, in
order to have a maximum opening and exposure of the pulmonary
cavity.
Subsequently, by daily dressing and cleaning of the
cavernostoma, the granulation and epithelialization of the cavern
will be stimulated. Sometimes, it is necessary to reopen the stoma
due to its tendency of superficially closing. Nakada et al
uses the Alexis wound retractor to avoid this issue (31). Bronchial fistulas may persist for a
long time, but they eventually slowly close. The closure of the
cavernostoma, a secondary therapeutic objective, can be performed
surgically by myoplasty or can occur spontaneously by
epithelialization (31,33,34,40,41).
Under optimal functional conditions, most authors
indicate pulmonary resection as an elective treatment in invasive
pulmonary aspergillosis. Cavernostomy, originally considered for
tuberculosis lesions, was subsequently employed for patients with
invasive pulmonary aspergillosis with borderline lung function, in
whom the anesthetic-surgical risk was too high to perform lung
resection.
Authors found that in the group with conservative
drug treatment in symptomatic forms the results were poor, with a
significant mortality rate at 12 months. Therefore, surgical
treatment was imposed. It is unanimously accepted that in patients
with absolute contraindication to surgery, parenteral treatment is
not sufficient and it is recommended to inject intracavitary
amphotericin, or saline solution, and if possible, draining the
cavity under CT guidance. Complete or temporary remissions can be
obtained (26).
Takahashi et al (42) presented an article of three case
presentations, but all with acceptable lung function (which allowed
a lung resection, i.e., FEV1 over 55%), but all on a postoperative
background of neoplastic context. Patients had developed
aspergillus forms on the remaining pleural cavities, probably air
contaminated postoperatively by parenchymal or bronchial air
fistulas.
The major element of clinics that imposed a
cavernostomy were small-mild, recurrent hemoptysis, less often a
massive episode (30-33,38-43).
Concerning surgical timing, Gebitekin et al
(44) and Da Silva et al
(36) performed the intervention in
conditions of massive hemoptysis, but it is preferable to perform
the intervention in chronic conditions, if possible, after
bronchial artery embolization or after medical treatment with
traxemic acid. Rergkliang et al did the cavernostomy for
massive hemoptysis, but without having a preoperative pulmonary
functional evaluation (44,45).
Cavernostomy is performed where the lesion is
closest to the chest wall. The place of incision is the axillary
area in most cases, but there was also one case in which the
anterior area on the right medioclavicular line was the elected
incision area.
In our group, out of 4 surgical procedures, 3
cavernostomies were performed in the right axillary area and one
interscapuleovertebral on the left hemithorax after resection of
the posterior rib arches 3 and 4. The procedure itself is guided by
the peripheral area of the cavern, usually associated with lesions
of the posterior and apical segments. The approach is limited in
the scapular area if there is an exact overlap.
It is preferable to locate via guidance the
peripheral contact area of the cave under a computed tomography or
radioscopic.
The procedure is performed in a single stage under
general anesthesia. Performing the procedure under local or
regional anesthesia constitutes an exception. Gebitekin et
al (44) simultaneously
mobilized muscle flaps to fill the cavity. This option should be
maintained if there are no major bronchial fistulas. Large flap
muscles of the pectoralis major, serratus anterior or latissimus
dorsi muscles can be used depending on the topography of the
cavern. Shirahashi et al (46) reported a case of two-stage operation
with omentopexy following cavernostomy, for lung abscess arising in
the residual lung after bilobectomy.
The procedure may also involve mobilization of
muscle flaps for filling the remaining cavity, but usually these
should be avoided until the area is granulated and the fistulas
have shrunk or even closed. It can be carried out later, after the
closure of the bronchial fistulas or partially to favor the closure
of the fistulas in case of reintervention for the reopening of the
stoma. Regnard et al (47)
and Sagawa et al (48)
mentioned reinterventions to reopen the superficially closed stoma
to restore communication.
Postoperatively, the authors mention the dressing of
the cavernostoma with gauzes soaked with amphotericin B; however,
daily dressing and cleaning the cavernostoma with sterile gauzes is
sufficient, abolishing the favorable conditions for fungus
development. Systemic antifungal treatment is recommended to
precede the intervention by 2 weeks and to follow it for up to 3
months.
Many authors reported a mortality rate higher than
that seen with pulmonary resection, but that is because the
patients eligible for cavernostomy have a poor general condition or
impaired pulmonary function (41-49).
In a large study, Cesar et al (35) presented 111 cases subjected to
cavernostomy for pulmonary aspergillosis associated with reduced
lung function. The evolution of the patients was similar to the
group in which lung resection was performed. The author found a
higher rate of hemorrhagic complications, probably due to specific
hypervascularization and recurrences, secondary to the tendency of
superficial closure of the stoma or complete non-drainage of the
aspergillary cavities (35).
Overall, the method of cavernostomy remains a good
solution. It is effective and it can be performed in patients with
complex fungal ball with peripheral location, with permanently or
temporarily impaired pulmonary function. In stable patients without
active hemoptysis, it demonstrated to be an easy-to-perform and
low-risk procedure.
In conclusion, lung resection techniques for
invasive pulmonary aspergillosis are of choice if lung function
allows for it and there are no other contraindications. The high
rate of mortality of lung aspergillosis with poor ventilator
function despite medical treatment and arterial embolization demand
a solution with minimal impact. Thus, cavernostomy should remain an
option in selected cases that do not allow large-scale resections
or an additional functional decrease.
Acknowledgements
Professional editing, linguistic and technical
assistance performed by Irina Radu, Individual Service Provider,
certified translator in Medicine and Pharmacy (certificate
credentials: Series E no. 0048).
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
CP, AC, AG, AZ, and CS performed the surgical
procedure. NB, CS, MD, IB, OS, SC, and DC reviewed and analyzed the
literature data. CD performed the preoperative investigation the
patient. IB, NB and CS prepared the draft of the manuscript. CS was
advisor of the surgical procedures. CS and NB reviewed the final
version of the manuscript. CP and CS assessed the authenticity of
all data. The authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Written informed consent was signed by the patient
on 13.05.2020. Approval of the Ethics Committee of ‘Marius Nasta’
National Institute of Pneumology, Bucharest, Romania was obtained
(no 152/2020).
Patient consent for publication
Consent for publication of the patient's data and
images was obtained.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kousha M, Tadi R and Soubani AO: Pulmonary
aspergillosis: A clinical review. Eur Respir Rev. 20:156–174.
2011.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kosmidis C and Denning DW: The clinical
spectrum of pulmonary aspergillosis. Thorax. 70:270–277.
2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Davidsen JR, Rosenvinge FS, Assing K and
Laursen CB: Chronic pulmonary aspergillosis. Ugeskr Laeger.
180(V05170434)2018.PubMed/NCBI(In Danish).
|
|
4
|
Patterson KC and Strek ME: Diagnosis and
treatment of pulmonary aspergillosis syndromes. Chest.
146:1358–1368. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Denning DW, Cadranel J, Beigelman-Aubry C,
Ader F, Chakrabarti A, Blot S, Ullmann AJ, Dimopoulos G and Lange
C: European Society for Clinical Microbiology and Infectious
Diseases and European Respiratory Society. Chronic pulmonary
aspergillosis: Rationale and clinical guidelines for diagnosis and
management. Eur Respir J. 47:45–68. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wilopo BAP, Richardson MD and Denning DW:
Diagnostic aspects of chronic pulmonary aspergillosis: Present and
new directions. Curr Fungal Infect Rep. 13:292–300. 2019.
|
|
7
|
Denning DW, Follansbee SE, Scolaro M,
Norris S, Edelstein H and Stevens DA: Pulmonary aspergillosis in
the acquired immunodeficiency syndrome. N Engl J Med. 324:654–662.
1991.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Gefter WB: The spectrum of pulmonary
aspergillosis. J Thorac Imaging. 7:56–74. 1992.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Binder RE, Faling LJ, Pugatch RD, Mahasaen
C and Snider GL: Chronic necrotizing pulmonary aspergillosis: A
discrete clinical entity. Medicine (Baltimore). 61:109–124.
1982.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Greenberger PA, Bush RK, Demain JG, Luong
A, Slavin RG and Knutsen AP: Allergic bronchopulmonary
aspergillosis. J Allergy Clin Immunol Pract. 2:703–708.
2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Page ID, Byanyima R, Hosmane S, Onyachi N,
Opira C, Richardson M, Sawyer R, Sharman A and Denning DW: Chronic
pulmonary aspergillosis commonly complicates treated pulmonary
tuberculosis with residual cavitation. Eur Respir J.
53(1801184)2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Horvat T, Savu C, Motaş C and Teţu M:
Pneumopericardium-complication of an unknown tuberculosis in a HIV
positive patient. Eur J Cardiothorac Surg. 26(1043)2004.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Walsh TJ, Anaissie EJ, Denning DW,
Herbrecht R, Kontoyiannis DP, Marr KA, Morrison VA, Segal BH,
Steinbach WJ, Stevens DA, et al: Treatment of aspergillosis:
Clinical practice guidelines of the infectious diseases society of
America. Clin Infect Dis. 46:327–360. 2008.PubMed/NCBI View
Article : Google Scholar
|
|
14
|
Shibuya K, Ando T, Hasegawa C, Wakayama M,
Hamatani S, Hatori T, Nagayama T and Nonaka H: Pathophysiology of
pulmonary aspergillosis. J Infect Chemother. 10:138–145.
2004.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Ohba H, Miwa S, Shirai M, Kanai M, Eifuku
T, Suda T, Hayakawa H and Chida K: Clinical characteristics and
prognosis of chronic pulmonary aspergillosis. Respir Med.
106:724–729. 2012.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Soubani AO and Chandrasekar PH: The
clinical spectrum of pulmonary aspergillosis. Chest. 121:1988–1999.
2002.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Zmeili OS and Soubani AO: Pulmonary
aspergillosis: A clinical update. QJM. 100:317–334. 2007.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Izumikawa K, Tashiro T, Tashiro M,
Takazono T, Kosai K, Morinaga Y, Kurihara S, Nakamura S, Imamura Y,
Miyazaki T, et al: Pathogenesis and clinical features of chronic
pulmonary aspergillosis-is it possible to distinguish CNPA and CCPA
clinically? J Infect Chemother. 20:208–212. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Savu C, Melinte A, Posea R, Galie N,
Balescu I, Diaconu C, Cretoiu D, Dima S, Filipescu A, Balalau C and
Bacalbasa N: Pleural solitary fibrous tumors-a retrospective study
on 45 patients. Medicina (Kaunas). 56(185)2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Bruce RA: A case of pulmonary
aspergillosis. Tubercle. 38:203–209. 1957.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Campbell JH, Winter JH, Richardson MD,
Shankland GS and Banham SW: Treatment of pulmonary aspergilloma
with itraconazole. Thorax. 46:839–841. 1991.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Farid S, Mohamed S, Devbhandari M, Kneale
M, Richardson M, Soon SY, Jones MT, Krysiak P, Shah R, Denning DW
and Rammohan K: Results of surgery for chronic pulmonary
aspergillosis, optimal antifungal therapy and proposed high risk
factors for recurrence-a national centre's experience. J
Cardiothorac Surg. 8(180)2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Jhun BW, Jeon K, Eom JS, Lee JH, Suh GY,
Kwon OJ and Koh WJ: Clinical characteristics and treatment outcomes
of chronic pulmonary aspergillosis. Med Mycol. 51:811–817.
2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Stevens DA, Kan VL, Judson MA, Morrison
VA, Dummer S, Denning DW, Bennett JE, Walsh TJ, Patterson TF and
Pankey GA: Practice guidelines for diseases caused by asperillus.
Infectious diseases society of America. Clin Infect Dis.
30:696–709. 2000.PubMed/NCBI View
Article : Google Scholar
|
|
25
|
Flückiger U, Marchetti O, Bille J,
Eggimann P, Zimmerli S, Imhof A, Garbino J, Ruef C, Pittet D,
Täuber M, et al: Treatment options of invasive fungal infections in
adults. Swiss Med Wkly. 136:447–463. 2006.PubMed/NCBI
|
|
26
|
Munk PL, Vellet AD, Rankin RN, Müller NL
and Ahmad D: Intracavitary aspergilloma: Transthoracic percutaneous
injection of amphotericin gelatin solution. Radiology. 188:821–823.
1993.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Suen H, Wright C and Mathisen DJ: Surgical
management of pulmonary aspergillosis. Chest Surg Clin N Am.
3:671–681. 1993.
|
|
28
|
Hargis JL, Bone RC, Stewart J, Rector N
and Hiller FC: Intracavitary amphotereicin B in the treatment of
symptomatic pulmonary aspergillomas. Am J Med. 68:389–394.
1980.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Giron J, Poey C, Fajadet P, Sans N,
Fourcade D, Senac JP and Railhac JJ: CT-guided percutaneous
treatment of inoperable pulmonary aspergillomas: A study of 40
cases. Eur J Radiol. 28:235–242. 1998.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Kasprzyk M, Pieczynski K, Mania K, Gabryel
P, Piwkowski C and Dyszkiewicz W: Surgical treatment for pulmonary
aspergilloma-early and long-term results. Kardiochir
Torakochirurgia Pol. 14:99–103. 2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Nakada T, Akiba T, Inagaki T, Morikawa T
and Ohki T: Simplified cavernostomy using wound protector for
complex pulmonary aspergilloma. Ann Thorac Surg. 98:360–361.
2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Gao Y and Soubani A: Advances in the
diagnosis and management of pulmonary aspergillosis. Adv Respir
Med. 87:231–243. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Lee JG, Lee CY, Park IK, Kim DJ, Chang J,
Kim SK and Chung KY: Pulmonary aspergilloma: Analysis of prognosis
in relation to symptoms and treatment. J Thorac Cardiovasc Surg.
138:820–825. 2009.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Vergeret J, Dabadie P, Dupon M, Maurette
P, Taytard A and Chevais R: Endocavitary drainage (Monaldi's
technic) in the treatment of pulmonary abscess. Rev Fr Mal Respir.
11:201–207. 1983.PubMed/NCBI(In French).
|
|
35
|
Cesar JM, Resende JS, Amaral NF, Alves CM,
Vilhena AF and Silva FL: Cavernostomy x resection for pulmonary
aspergilloma: A 32-year history. J Cardiothorac Surg.
6(129)2011.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Da Silva P, Marsico GA, Araujo MA, Braz
FS, Santos HT, Loureiro GL and Fontes A: Complex pulmonary
aspergilloma treated by cavernostomy. Rev Col Bras Cir. 41:406–411.
2014.PubMed/NCBI View Article : Google Scholar : (In English,
Portuguese).
|
|
37
|
Kelley WO and Pecora DV: The Monaldi
procedure; a report of thirty cases. Am Rev Tuberc. 65:83–87.
1952.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Ratermann KL, Ereshefsky BJ, Fleishaker
EL, Thornton AC, Buch KP and Martin CA: Fulminant invasive
pulmonary aspergillosis after a near-drowning accident in an
immunocompetent patient. Ann Pharmacother. 48:1225–1229.
2014.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Chen JC, Chang YL, Luh SP, Lee JM and Lee
YC: Surgical treatment for pulmonary aspergilloma: A 28 year
experience. Thorax. 52:810–813. 1997.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Kilman JW, Ahn C, Andrews NC and Klassen
K: Surgery for pulmonary aspergillosis. J Thorac Cardiovasc Surg.
57:642–647. 1969.PubMed/NCBI
|
|
41
|
Massard G, Roeslin N, Wihlm JM, Dumont P,
Witz JP and Morand G: Pleuropulmonary aspergilloma: Clinical
spectrum and results of surgical treatment. Ann Thorac Surg.
54:1159–1164. 1992.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Takahashi R, Fujiwara T and Yamakawa H:
Cavernostomy for pulmonary aspergillosis associated with destroyed
lung after surgery for lung cancer: Report of 3 cases. Case Rep
Surg. 2015(614795)2015.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Soltanzadeh H, Wychulis AR, Sadr F,
Bolanowski PJ and Neville WE: Surgical treatment of pulmonary
aspergilloma. Ann Surg. 186:13–16. 1977.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Gebitekin C, Sami Bayram A and Akin S:
Complex pulmonary aspergilloma treated with single stage
cavernostomy and myoplasty. Eur J Cardiothorac Surg. 27:737–740.
2005.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Rergkliang C, Chetpaophan A, Chittithavorn
V and Vasinanukorn P: Surgical management of pulmonary cavity
associated with fungus ball. Asian Cardiovasc Thorac Ann.
12:246–249. 2004.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Shirahashi K, Iuchi K, Matsumura A, Tanaka
H, Tamura M and Goto M: A case of two-stage operation, omentopexy
following cavernostomy, for lung abscess arising in the residual
lung after bilobectomy. J Japan Assoc Chest Surg. 17:691–696.
2003.
|
|
47
|
Regnard JF, Icard P, Nicolosi M, Spagiarri
L, Magdeleinat P, Jauffret B and Levasseur P: Aspergilloma: A
series of 89 surgical cases. Ann Thorac Surg. 69:898–903.
2000.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Sagawa M, Sakuma T, Isobe T, Sugita M,
Waseda Y, Morinaga H and Iuchi K: Cavernoscopic removal of a fungus
ball for pulmonary complex aspergilloma. Ann Thorac Surg.
78:1846–1848. 2004.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Jewkes J, Kay PH, Paneth M and Citron KM:
Pulmonary aspergilloma: Analysis of prognosis in relation to
haemoptysis and survey of treatment. Thorax. 38:572–578.
1983.PubMed/NCBI View Article : Google Scholar
|