Introduction
Since the COVID-19 pandemic outbreak, medical
systems in all affected countries have tried to identify rapid
solutions to adapt to the arising new challenges (1). Besides management strategies
developed for patients suffering from COVID-19 infection, which
exert an enormous burden on the medical system, critical issues
emerged when trying to find solutions for patients suffering from
other diseases (2,3), including patients diagnosed with head
and neck cancers (HNC). HNC was ranked the sixth most common
malignancy worldwide during the last 5 years, representing ~6% of
all cancer cases (4), and despite
all efforts for early disease detection, up to 70% of the patients
are in advanced stages of the disease at the moment of diagnosis
(5,6). In most cases, these patients are
candidates for extended surgeries, which imply complex
reconstructive solutions using free flap techniques. For the
reconstruction of simple or composite oral defects, current reports
indicate the forearm, anterolateral thigh and fibula as the common
donor sites for free tissue transfer, considered today the golden
standard for this type of defect reconstruction (7,8). The
advances made in microsurgery and reconstructive surgery during the
last decades allowed for numerous medical centers to conduct these
types of surgeries with very high rates of success (9,10).
However, in most cases, patients which undergo head and neck
surgeries with free vascularized flap reconstructions, require
specific postoperative care from several h up to days (11), which represented an enormous
challenge during the last two years since the COVID-19 pandemic
outbreak, due to both lack of available beds in intensive care
units and the deficit of qualified medical staff which was
massively redirected for the treatment and surveillance of COVID-19
patients (12). Unfortunately,
this new context was associated with concerning reports regarding
access to adequate medical care for patients with HNC eligible for
radical surgeries (13). An
increase in avoidable deaths associated with malignancy is expected
in the following years, as a consequence of the limited access to
medical care that patients faced during the last two years of the
COVID-19 pandemic (14).
In this challenging context, surgeons from different
specialties tried to identify timely solutions to treat oncologic
patients (15). These would
usually imply simpler methods of therapy, which could be conducted
without or with the minimal implication of intensive care units.
Management strategies in complex head and neck defects, initially
delayed due to an acute deficit of medical staff specially trained
for perioperative care, were reconsidered and alternative solutions
were identified to provide proper and timely surgical treatment to
patients with resectable HNC, as part of the multimodal oncological
therapy (16). Reconstruction
methods with local and regional flaps, widely used before the
microsurgery era, were reintroduced as valid management
alternatives for large head and neck defect reconstruction.
Techniques using temporalis or pectoralis major muscles, submental
or deltopectoral flaps, for the repair of a variety of oral defects
(17,18), have been reported during the last
years, in this pandemic context, as alternatives for free flap
reconstructive methods (16,19).
In the present study, the clinical case of a patient
diagnosed with locally advanced buccal cancer during the heaviest
wave of COVID-19 pandemic in Romania was presented (when our
medical system was severely challenged), for whom a combination of
two local flaps: temporal and submental flap was used, as an
alternative for a free flap reconstruction technique, in order to
restore the defect resulted after radical tumor resection. The aim
of the present case report is to provide alternative approaches for
the reconstruction of complex head and neck defects in cases were
standard care is not possible, thus assuring the best medical care
for the patients.
Case report
In September 2021, when the fourth wave of the
COVID-19 pandemic heavily hit Romania and an important part of the
medical staff was redirected for the management of COVID-19
patients, a 66-year-old male patient was referred to the Department
of Oral and Maxillofacial surgery of ‘Carol Davila’ Central
University Emergency Military Hospital (Bucharest, Romania), for
specific treatment with a confirmed diagnosis following an
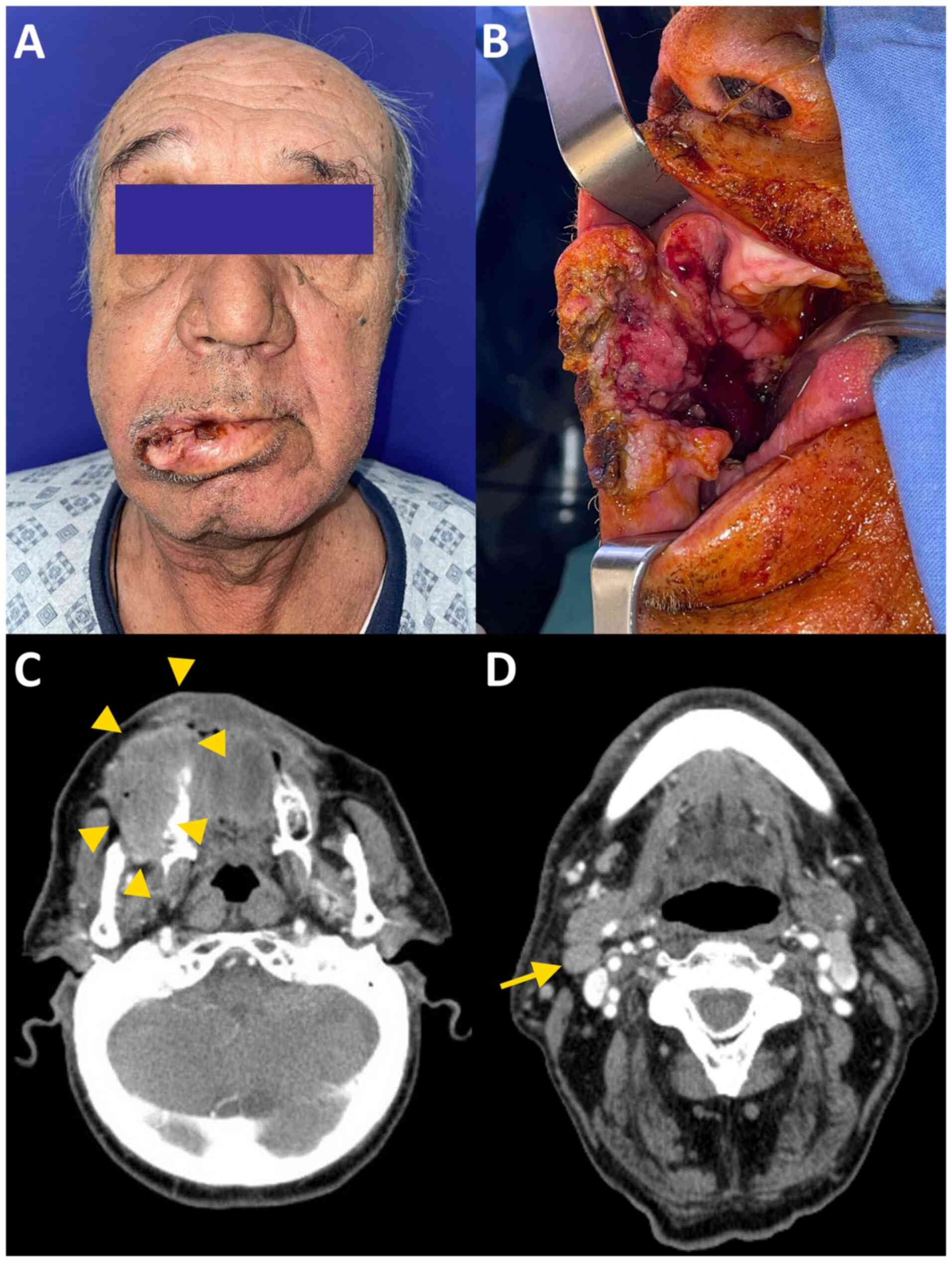
incisional biopsy of an oral squamous cell carcinoma. The clinical
examination revealed an extensive ulcero-infiltrative lesion
involving the entire buccal mucosa on the right side, extended to
the upper vestibulum, right labial commissure and a limited area of
the perioral skin, upper right lip, retromolar region, with a
diameter of ~7/5 cm (Fig. 1A and
B). The mouth opening was
restricted and the patient complained of local pain, oral bleeding,
halitosis and significant eating impairment. The medical history
revealed no significant preexisting conditions except for
hypertension, which was controlled with specific medication. The
patient was a heavy smoker for more than 30 years and had a history
of alcohol abuse. The computed tomography (CT) scan revealed a
contrast-enhancing lesion measuring 6.9/3.9/4.1 cm, involving the
right buccal soft tissues including the buccal muscle, associating
right alveolar bone lysis and lateroanterior maxillary sinus
invasion, inferiorly extended to the vicinity of the right
mandibular ramus, with no cortical bone invasion. The
pterigopalatine fossa was tumor-free. The cervical CT scan
objectified a level IIA lymph node with the largest diameter of 1.3
cm and no other evidence of suspicious nodes in the right cervical
area (Fig. 1C and D). The whole-body CT scan did not reveal
any lesions suggestive of distant metastases.
The indication for urgent radical tumor resection
and immediate defect reconstruction, in order to allow for timely
initiation of the adjuvant therapy, was obvious, but at that
moment, all surgical procedures requiring specialized postoperative
care were restricted due to an acute deficit of medical staff and
available beds in the intensive care units. In our hospital, as in
numerous medical facilities in Romania, other departments were
temporarily adapted to admit COVID-19 patients and medical staff
from other specialties were redirected towards treating COVID-19
hospitalized cases, a situation that was somehow similar to war
conditions. In this context, an alternative procedure was selected
for the defect reconstruction after radical tumor resection, that
would not imply free vascularized tissue transfer and microsurgery,
which according to our protocols should be followed by a temporary
patient transfer to the intensive care unit for specialized
postoperative care, for at least 12 h. Preoperative assessment
included blood tests, electrocardiogram, cardiac and pulmonary
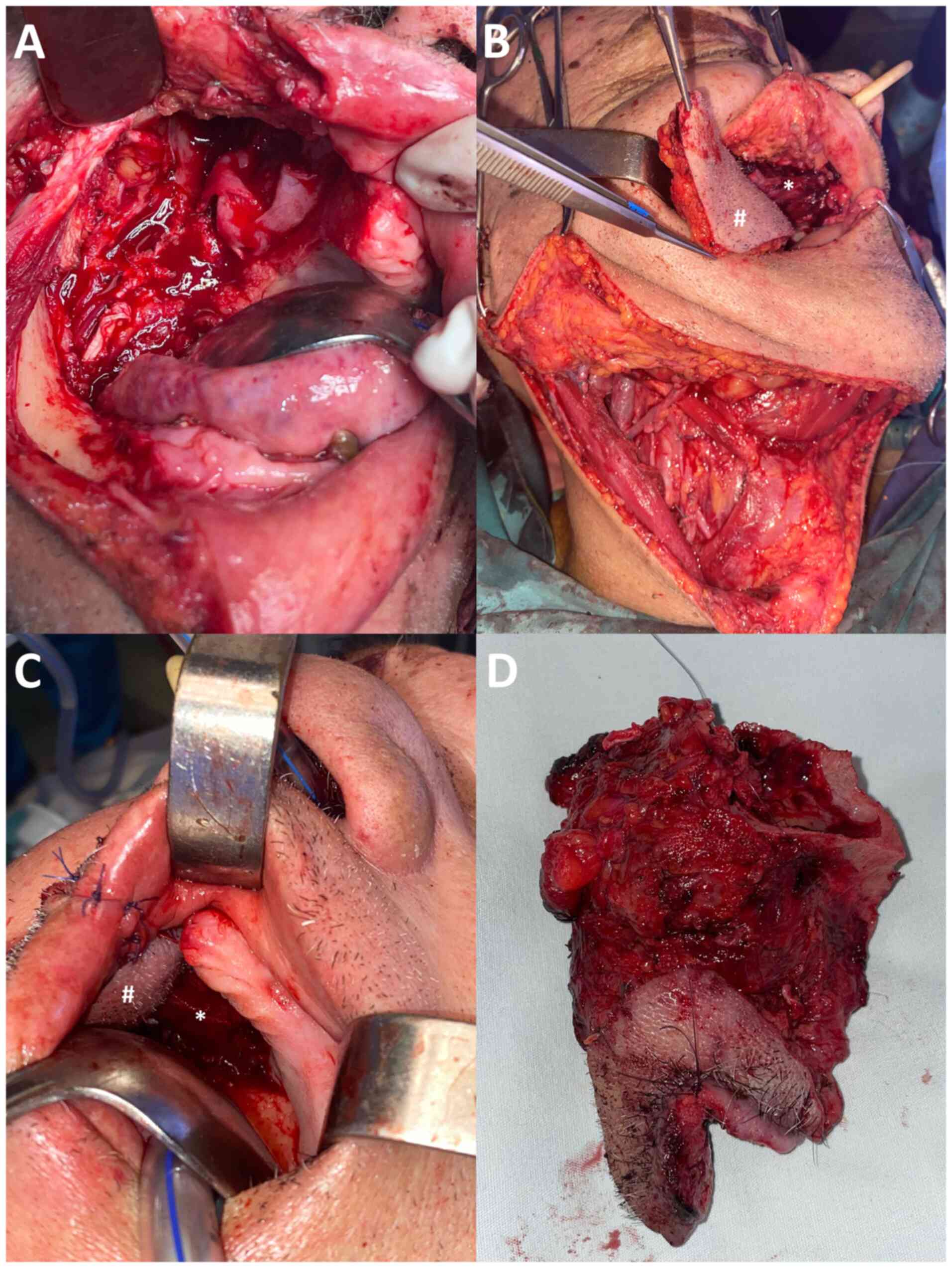
evaluations, with no abnormal findings. The surgical procedure,
conducted under general anesthesia with oro-tracheal intubation,
consisted of radical tumor resection with intraoperative
confirmation of tumor-free margins and concomitant functional
radical neck dissection (type III). The resection specimen included
segments of the lips plus labial commissure, buccal soft tissues
until the subcutaneous layer of genian skin, right hemimaxilla from
the midline, right maxillary sinus, right pterygoid plates with
partial resection of the right pterygoid muscles (Fig. 2), as well as the neck dissection
specimen (lymph node stations 1-5). Defect reconstruction was
conducted through a composite technique, using a right temporal
muscle flap for closure of the oro-antral and oro-nasal fistula and
a submental flap for the reconstruction of the buccal and
retromolar regions. The temporal muscle flap was advanced under the
temporozygomatic arch. No arch osteotomy was required for the
advancement, only the release of the fascia from the arch in order
to obtain a tension-free suture to the recipient site. The
superficial layer of the temporal fascia was preserved and
reinserted in order to prevent the volumetric defect of the donor
temple. The submental flap had a diameter of 5/3 cm, pedicled on
the right facial vessels, advanced to the right inner surface of
the cheek through the floor of the mouth, posterior to the
mylohyoid muscle. The total length of the surgery was 6.5 h. At the
end of the surgery, a nasogastric tube was placed to assist with
feeding during the first postoperative days. Immediately after
surgery, the patient was transferred to the postoperative ward
within our department where the monitoring and treatment were
conducted by the medical staff from the oro-maxillo-facial
department, with no indication for temporary placement in a
specialized care unit or an intensive care unit. Postoperatively,
the patient received intravenous antibiotic therapy [Amoxicilin +
Clavulanic acid 1 g, three times per day (TID)], anti-inflammatory
and analgesic drugs (Paracetamol 10 mg/ml, Metamizole 5 ml TID),
and nutritive support for a total of 5 days. The patient underwent
the standard postoperative care protocol: Daily wound cleaning with
antiseptics, removal of the two draining tubes at 24 and 48 h
(drainage of 20 ccs per tube), and dressing. Postoperative recovery
was optimal, with no significant events or complications. The
length of the hospitalization was of 5 days, which was an important
advantage considering the limited number of beds for non-COVID
patients in our hospital.
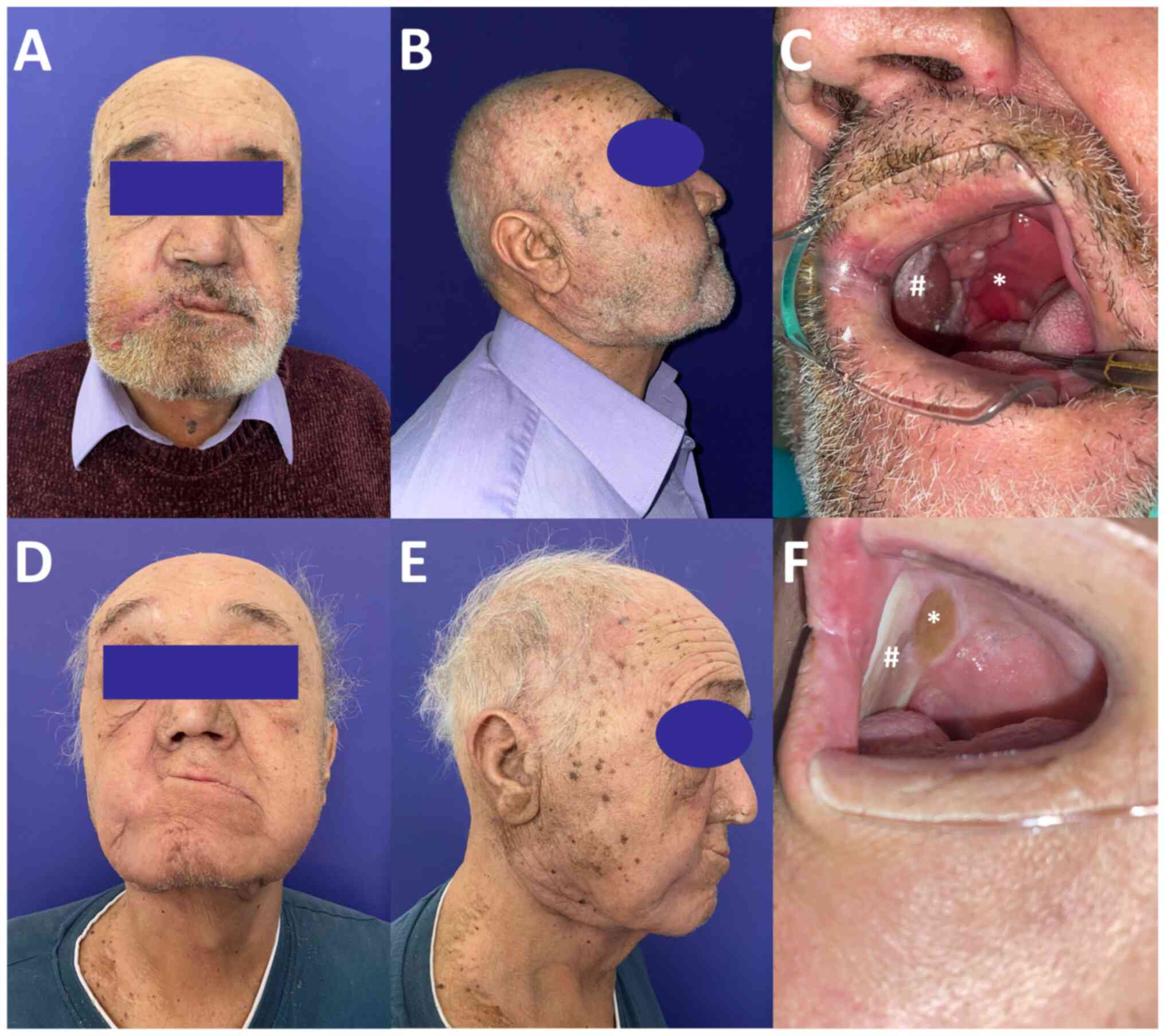
The cutaneous sutures were removed one week after
the surgery. Intraoral wounds were sutured with resorbable sutures.
The patient returned for the first follow-up visit 4 weeks after
surgery, when the normal metaplasia process of the transplanted
tissues was in progress (Fig.
3A-C). The healing was optimal, with no evidence of fistulas or
other complications. The final pathology report described a
poorly-differentiated, keratinizing squamous cell carcinoma, with
bone invasion, positive perineural invasion, and no evidence of
vascular invasion. Intense intratumor and peritumor inflammatory
infiltrate was present. Resection margins, as well as all lymph
nodes within the specimen, were tumor-free. Pathological staging
was pT4aN0Mx. According to national guidelines and based on the
clinical staging and final pathology report the oncology board
proposed adjuvant therapy. Within 6 weeks after surgery, the
patient initiated radiotherapy associated with chemotherapy. At the
first follow-up visit, one month after completion of the adjuvant
treatment, the patient was in a favorable general condition, with
no significant complaints, except for minor microstomia. The oral
and cervical surgical wounds had a normal appearance, with partial
shrinkage of the intraoral flaps secondary to radiotherapy, no
signs of tumor progression or recurrence, and no evidence of
dehiscence or chronic fistulas (Fig.
3D-F). The follow-up contrast CT scan revealed a normal
postoperative/post-irradiation aspect, with no evidence of tumor
progression or recurrence. The patient reported a healthy appetite
and minor weight gain. Furthermore, the patient reported cessation
of smoking and alcohol consumption. The patient is enrolled in a
follow-up program with regular visits and imaging assessments.
Discussion
The COVID-19 pandemic outbreak has shattered the
entire world, challenged the medical systems worldwide, and tested
the speed of reaction of the scientific and medical community when
facing unexpected aggression (20). At certain points, in different
countries, heavy pandemic waves severely affected surgical
departments, which are directly dependent on anesthetists as part
of the medical team and intensive care units for patient management
(12,19). The challenges related to the
reconstruction of head and neck defects emerged once the first
surgical procedures of head and neck tumor resections were
performed (21). This anatomical
region is of great complexity and surgery can have a major impact
on the quality of life of the patient, associated with all the
functional roles attributed to this region-speech, chewing,
swallowing, breathing as well as social reintegration, as the face
represents the projection of one's identity in the society.
Therefore, the perfect reconstruction technique would lead to a
‘restitutio ad integrum’ of the highly specialized noble
structures and is continuously pursued by both researchers and
medical practitioners. Different techniques have been reported and
implemented in clinical practice during the last century, since the
discovery of general anesthesia allowed for an accelerated progress
in surgical procedures (22).
Currently, free flap reconstruction techniques have been accepted
worldwide as the ‘gold standard’ for the reconstruction of wide,
complex head and neck defects (23). In the last decade, these types of
surgeries are conducted in numerous medical facilities with
continuously increasing rates of success, for the great benefit of
patients (24). However,
unexpected local or global events, similar to the pandemic
situation that emerged during the last two years have raised new
challenges, when the sudden acute necessity of intensive care units
and specialized medical staff was redirected to provide specific
medical care for the patients with severe COVID-19 infections
(15). The limited access of
patients to appropriate treatment had negative, occasionally even
dramatic, consequences for patients with other types of diseases,
including patients with HNC (25).
The massive redirection of intensive care equipment and trained
staff for the management of continuously rising number of COVID-19
patients led to a major reduction, and at certain moments even
cessation, of non-emergency surgeries. In this context, complex,
extended surgeries, including free flap reconstructive surgery for
head and neck defects, could not be performed, forcing the
maxillofacial surgeon to look for alternative solutions in order to
provide the best medical care for the patients. Large defects,
routinely reconstructed using free flap techniques, were
reconsidered for reconstructive options with local or regional
flaps, alone or in different combinations (19).
In the present case, regional flaps-temporal muscle
flap and submental flap-were associated as a simpler and reliable
alternative for a composite free flap reconstruction technique of a
large, complex defect of the right hemimaxilla and cheek resulting
after radical tumor excision. Recent studies have reported similar
approaches in the management of patients with HNC during this
pandemic period (16,26). The renewed interest for temporal
muscle flap in the reconstruction of maxillary defects is due to
the advantages of this reconstructive method: a simple and rapid
technique, performed by a single surgeon, with high reliability of
vascular supply and a hidden donor site scar in the hair-bearing
skin, which provides very well matching, thin and pliable tissue
for the immediate closure of oro-antral fistulas resulting after
maxillary resection, with an excellent functional outcome in terms
of speech and swallowing (27).
The main complaint of the patients after using this technique is
the impaired appearance caused by the temple hollowing after
temporal muscle displacement into the oral cavity (28). For our patient, a modification of
the procedure was used, with preservation of the superficial layer
of the temporal fascia, thus allowing for a reconstruction of the
donor site with minimal hollowing, otherwise not reported by the
patient. The initial result was stable at the last follow-up visit,
4 months after surgery and radiotherapy completion. Permanent
facial nerve palsy after flap harvesting is another complication
when raising temporal muscle flap, however, it is uncommon in
experienced hands (28).
The submental flap, used in our patient for the
reconstruction of the buccal and retromolar area, is another flap
that has been reconsidered during the last two years as a valid
alternative for free flap reconstruction techniques (13). This flap was designed and reported
by Martin et al (29) as an
alternative to free flaps for the reconstruction of oral cavity
defects. The donor site for this flap is actually within the
operating field, providing a generous and versatile skin paddle,
with a wide rotation arch and perfectly matching color and texture,
suitable for various cutaneous and oral reconstructions. The major
drawback of this flap is related to the potential risk of
metastatic lymph node transplantation in patients with occult level
I lymph node involvement (30).
Several systematic reviews reported significantly decreased
operating time and hospitalization length, with similar long-term
results for submental flap reconstructive surgeries compared with
free flap reconstruction techniques. However, the size of the
reconstructed defect was smaller and the incidence of partial flap
failure was higher in submental flap groups (31,32).
In the present case, in order to compensate for the limitations
related to the size of the defect, it was chosen to combine two
reconstructive techniques, thus increasing the supply of
transferred tissue, which allowed for an appropriate reconstruction
of the entire defect, with no postoperative complications. In order
to minimize the risk of local recurrence secondary to occult lymph
node metastasis, a careful skeletonisation of the vascular pedicle
during flap harvesting was implemented, with complete removal of
surrounding fatty tissue. Modified techniques, such as the
inclusion of mylohyoid muscle, in order to minimize the risk of
flap loss due to a compromise in vascular supply, are indicated
only in patients with clinically negative necks and primary tumors
with a very low risk of level I lymph node metastasis, which is not
the case for buccal cancer where level 1B lymph node involvement is
more common (33). However, these
modified techniques are useful for training purposes of resident
doctors, increasing their level of confidence when performing
submental flap harvesting (34).
To the best of our knowledge, this is the first report of a
combined technique using these two flaps for the reconstruction of
a composite head defect, resulted after tumor resection. The main
advantages of our proposed approach are related to the simple, fast
and reliable character of the surgical technique, which does not
require any specialized equipment, thus allowing to implement this
reconstructive method in any challenging context, such as a global
pandemic or war. By contrast, microsurgical reconstruction through
free flaps involves complex and lengthy surgeries, which require
highly equipped and specialized facilities, as well as dedicated
postoperative care units. The main limitation of local and regional
flaps in head and neck defect rehabilitation is related to the size
of the reconstructed area. This limitation was overcome through the
use of a combination of two distinct regional flaps-temporal and
submental-thus allowing an optimal primary repair of the wide
defect resulted after tumor resection.
In conclusion, both temporal muscle and submental
flaps are defined by an easy harvesting technique and reduced
surgical time in experienced hands, advantages that become crucial
in historically difficult times. One of the drawbacks of modern
medical training systems is that younger surgeons are mainly
trained in free flap reconstruction techniques and are less
familiar with these alternative methods of reconstruction, thus
excluding them as the option of treatment when making treatment
plans. This aspect emphasizes the importance of a broad program of
surgical training for young surgeons, even if conducted only on
cadaveric specimens, in order to maintain a versatile, flexible
ability of approach in treatment planning. These situations may
become useful not only in severe global situations, such as the
COVID-19 outbreak but also when assessing individual cases. HNC
arises frequently in elderly patients, numerous of whom have other
severe comorbidities, that are not compatible with lengthy,
complex, high-risk surgeries (35,36).
Simple solutions, represented by local flaps, single or in
combination, may be an improved option for these patients.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AC was responsible for conceptualization,
methodology and writing the manuscript. AC, LM, RMC, RSC, TAF, CS,
DOC and CC performed the data analysis, literature research and
original draft preparation. CC was responsible for editing,
critical review of the manuscript and supervision of the project.
AC and CS confirm the authenticity of all the raw data. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved (approval no.
504/1.03.2022) by the Local Ethics Committee of the ‘Carol Davila’
Central Military Emergency University Hospital (Bucharest,
Romania). Written informed consent was obtained from the
patient.
Patient consent for publication
Written informed consent was obtained from the
patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Haldane V, De Foo C, Abdalla SM, Jung AS,
Tan M, Wu S, Chua A, Verma M, Shrestha P, Singh S, et al: Health
systems resilience in managing the COVID-19 pandemic: Lessons from
28 countries. Nat Med. 27:964–980. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Meredith JW, High KP and Freischlag JA:
Preserving elective surgeries in the COVID-19 pandemic and the
future. JAMA. 324:1725–1726. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lee J, Choi JY and Kim MS: Elective
surgeries during the COVID-19 outbreak. Br J Surg.
107(e250)2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Economopoulou P and Psyrri A:
Epidemiology, risk factors and pathogenesis of squamous cell
tumours. In: Head and Neck Cancer: Essentials for Clinicians. 6th
edition. Licitra L and Karamouzis MV (eds). ESMO, Lugano, pp1-6,
2017.
|
|
5
|
Guizard AV, Dejardin OJ, Launay LC, Bara
S, Lapôtre-Ledoux BM, Babin EB, Launoy GD and Ligier KA: Diagnosis
and management of head and neck cancers in a high-incidence area in
France: A population-based study. Medicine (Baltimore).
96(e7285)2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Thompson-Harvey A, Yetukuri M, Hansen AR,
Simpson MC, Adjei Boakye E, Varvares MA and Osazuwa-Peters N:
Rising incidence of late-stage head and neck cancer in the United
States. Cancer. 126:1090–1101. 2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Suh JM, Chung CH and Chang YJ: Head and
neck reconstruction using free flaps: A 30-year medical record
review. Arch Craniofacial Surg. 22:38–44. 2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ragbir M, Brown JS and Mehanna H:
Reconstructive considerations in head and neck surgical oncology:
United Kingdom national multidisciplinary guidelines. J Laryngol
Otol. 130:S191–S197. 2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Dassonville O, Poissonnet G, Chamorey E,
Vallicioni J, Demard F, Santini J, Lecoq M, Converset S, Mahdyoun P
and Bozec A: Head and neck reconstruction with free flaps: A report
on 213 cases. Eur Arch Otorhinolaryngol. 265:85–95. 2008.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Blackwell KE: Unsurpassed reliability of
free flaps for head and neck reconstruction. Arch Otolaryngol Head
Neck Surg. 125:295–299. 1999.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Vincent A, Sawhney R and Ducic Y:
Perioperative care of free flap patients. Semin Plast Surg.
33:5–12. 2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Zaid W and Schlieve T: The early effects
of coronavirus disease-2019 on head and neck oncology and
microvascular reconstruction practice: A national survey of oral
and maxillofacial surgeons enrolled in the head and neck special
interest group. J Oral Maxillofac Surg. 78:1859–1868.
2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kent SL, Kim Y, Perez H, Frank E, Gentry
V, LaTour D and Inman J: Consideration in microvascular
reconstruction during times of social crises: Perspectives on
resource utilization. Facial Plast Surg. 36:768–772.
2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Maringe C, Spicer J, Morris M, Purushotham
A, Nolte E, Sullivan R, Rachet B and Aggarwal A: The impact of the
COVID-19 pandemic on cancer deaths due to delays in diagnosis in
England, UK: A national, population-based, modelling study. Lancet
Oncol. 21:1023–1034. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Stöß C, Steffani M, Kohlhaw K, Rudroff C,
Staib L, Hartmann D, Friess H and Müller MW: The COVID-19 pandemic:
Impact on surgical departments of non-university hospitals. BMC
Surg. 20(313)2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Rashid HU, Rashid M, Khan N, Ansari SS and
Bibi N: Taking a step down on the reconstruction ladder for head
and neck reconstruction during the COVID-19 pandemic. BMC Surg.
21(120)2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Abubaker AO and Abouzgia MB: The
temporalis muscle flap in reconstruction of intraoral defects: An
appraisal of the technique. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod. 94:24–30. 2002.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Amin AA, Sakkary MA, Khalil AA, Rifaat MA
and Zayed SB: The submental flap for oral cavity reconstruction:
Extended indications and technical refinements. Head Neck Oncol.
3(51)2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Pradhan P, Preetam C, Parida PK and Samal
DK: Changing trend in the management of head neck cancers during
the COVID-19 pandemic. Eur Arch Otorhinolaryngol. 279:1453–1460.
2022.PubMed/NCBI View Article : Google Scholar
|
|
20
|
World Health Organization: Third round of
the global pulse survey on continuity of essential health services
during the COVID-19 pandemic. https://www.who.int/publications/i/item/WHO-2019-nCoV-EHS_continuity-survey-2022.1.
Accessed, February 14, 2022.
|
|
21
|
Goldstein JC and Sisson GA Jr: The history
of head and neck surgery. Otolaryngol Head Neck Surg. 115:379–385.
1996.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Keys TE: The History of Surgical
Anesthesia. Robert E (ed). Krieger Publishing Company, Huntington,
1978.
|
|
23
|
Vila PM, Rich JT and Desai SC: Defining
quality in head and neck reconstruction. Otolaryngol Head Neck
Surg. 157:545–547. 2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Hanasono MM: Reconstructive surgery for
head and neck cancer patients. Adv Med. 2014(795483)2014.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Stokes AC, Lundberg DJ, Bor J, Elo IT,
Hempstead K and Preston SH: Association of health care factors with
excess deaths not assigned to COVID-19 in the US. JAMA Netw Open.
4(e2125287)2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Nguyen HL, Nguyen VM and Tran XP:
Temporalis muscle flap for the immediate reconstruction of oral
defects after oncologic resection. Case Rep Oncol. 14:573–579.
2021.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Brennan T, Tham TM and Costantino P: The
temporalis muscle flap for palate reconstruction: Case series and
review of the literature. Int Arch Otorhinolaryngol. 21:259–264.
2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ein L, Daniyan O and Nicolli E: Temporalis
muscle flap. Oper Tech Otolaryngol Head Neck Surg. 30:120–126.
2019.
|
|
29
|
Martin D, Pascal JF, Baudet J, Mondie JM,
Farhat JB, Athoum A, Le Gaillard P and Peri G: The submental island
flap: A new donor site. Anatomy and clinical applications as a free
or pedicled flap. Plast Reconstr Surg. 92:867–873. 1993.PubMed/NCBI
|
|
30
|
Setty CML, Konduru V, Tirkey AJ, Agrawal
M, George P and J R: The submental flap-outcomes and oncologic
safety in head and neck reconstruction. Adv Oral Maxillofac Surg.
3(100082)2021.
|
|
31
|
Mooney SM, Sukato DC, Azoulay O and
Rosenfeld RM: Systematic review of submental artery Island flap
versus free flap in head and neck reconstruction. Am J Otolaryngol.
42(103142)2021.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Jørgensen MG, Tabatabaeifar S, Toyserkani
NM and Sørensen JA: Submental Island flap versus free flap
reconstruction for complex head and neck defects. Otolaryngol Head
Neck Surg. 161:946–953. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Essig H, Warraich R, Zulfiqar G and Rana
M, Eckardt AM, Gellrich NC and Rana M: Assessment of cervical lymph
node metastasis for therapeutic decision-making in squamous cell
carcinoma of buccal mucosa: A prospective clinical analysis. World
J Surg Oncol. 10(253)2012.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Patel UA, Bayles SW and Hayden RE: The
submental flap: A modified technique for resident training.
Laryngoscope. 117:186–189. 2007.PubMed/NCBI View Article : Google Scholar
|
|
35
|
D'Andréa G, Scheller B, Gal J, Chamorey E,
Château Y, Dassonville O, Poissonnet G, Culié D, Koulmann PH,
Hechema R, et al: How to select candidates for microvascular head
and neck reconstruction in the elderly? Predictive factors of
postoperative outcomes. Surg Oncol. 34:168–173. 2020.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Colella G, Rauso R, De Cicco D, Boschetti
CE, Iorio B, Spuntarelli C, Franco R and Tartaro G: Clinical
management of squamous cell carcinoma of the tongue: Patients not
eligible for free flaps, a systematic review of the literature.
Expert Rev Anticancer Ther. 21:9–22. 2021.PubMed/NCBI View Article : Google Scholar
|