Introduction
Neurovascular compression (NVC) is the main cause of
primary trigeminal neuralgia (TN) or hemifacial spasm (HFS), and
frequently occurs at the root entry zone (REZ) of cranial nerves
(1). Microvascular decompression
(MVD) is an effective surgical treatment for TN and HFS caused by
NVC (2,3). However, preoperative detection of NVC
is occasionally difficult. Although MVD is not challenging for
skilled and experienced neurosurgeons, it is not effective for
patients with TN or HFS not caused by NVC (4). Therefore, an accurate preoperative
diagnosis of NVC is crucial in deciding whether to perform MVD.
Magnetic resonance imaging (MRI) has been used to
detect NVC prior to MVD for numerous years; however, it does have
certain disadvantages. Routine MRI sequences cannot clearly and
accurately display the relationship between nerves and blood
vessels at the REZ (4). Since the
1990s, 3D time-of-flight magnetic resonance angiography (3D TOF
MRA) has gradually become a common MRI sequence for detecting NVC.
3D TOF MRA is able to selectively image fast-flowing blood and
clearly display nerves and blood vessels (5). However, the 3D TOF MRA sequence
demonstrates a poor ability to visualize blood vessels with a slow
blood flow, such as veins and arterioles (6). With the development of MRI
technology, the appearance of high resolution T2-weighted imaging
(HR T2WI) brings new options for NVC detection. HR T2WI may
adequately demonstrate the anatomical structure in the
cerebellopontine angle (CPA) against the background of
cerebrospinal fluid (CSF) signal and aid in justifying a diagnosis
of NVC, which may be obtained by different technologies, including
3D balanced steady state gradient echo and 3D fast turbo spin echo
(5). Different manufacturers use
different names for these technologies, such as constructive
interference steady state (CISS), fast imaging employing
steady-state acquisition (FIESTA), balanced fast field echo (bFFE),
sampling perfection with application-optimized contrasts using
different flip angle evolutions (SPACE), balanced steady-state free
precession and turbo spin echo driven equilibrium. However, it is
difficult for HR T2WI to distinguish the relationship between
nerves and blood vessels when they are in close contact or there is
a lack of CSF signal contrast around them. In that case, another
MRI sequence is needed to assist with the diagnosis (6). Due to their advantages and
disadvantages, they are frequently used together to detect NVC.
Although the combination of the two sequences may make up for
certain shortcomings, both display two-dimensional images, and the
spatial structure of CPA cannot be displayed intuitively and
dynamically. Therefore, it is necessary to identify more accurate
imaging or post-processing technology to improve imaging
quality.
Multimodal image fusion (MIF) may combine two or
more images from the same or different modalities and reconstruct a
3D model, which allows the operator to observe anatomical details
more clearly from different angles (7). Therefore, the MIF technique combined
with these MRI sequences is considered to be an accurate method for
the preoperative diagnosis of NVC. 3D MIF based on 3D TOF MRA
combined with HR T2WI may accurately display the precise anatomical
structures at the REZ and indicate the relationship between cranial
nerves and blood vessels (8,9).
However, there remains a lack of large-scale clinical trials to
analyze its clinical application value in the preoperative
diagnosis of NVC.
The present meta-analysis was designed to evaluate
the value of 3D MIF based on 3D TOF MRA combined with HR T2WI in
the preoperative judgment of NVC in patients with TN and HFS, and
thus to evaluate its clinical application value in the preoperative
evaluation of MVD.
Materials and methods
Manuscript preparation
The whole study was conducted according to the
PRISMA 2020 statement (10) and
the manuscript was prepared and revised according to the PRISMA
2020 Checklist.
Search strategy and selection
criteria
PubMed (https://pubmed.ncbi.nlm.nih.gov/), Embase (https://www.embase.com), Web of Science (https://www.webofscience.com), Scopus (https://www.scopus.com), China National Knowledge
Infrastructure (https://www.cnki.net) and the
Cochrane Library (https://www.cochranelibrary.com/) were systematically
searched. The medical subject heading terms or Emtree terms were
‘Magnetic Resonance Angiography’ and ‘Microvascular Decompression
Surgery’. The search query was ‘((Microvascular Decompression
Surgery) OR (Decompression Surgeries, Microvascular) OR
(Decompression Surgery, Microvascular) OR (Microvascular
Decompression Surgeries) OR (Surgeries, Microvascular
Decompression) OR (Surgery, Microvascular Decompression) OR
(Microvascular Decompression) OR (Decompression, Microvascular) OR
(Decompressions, Microvascular) OR (Microvascular Decompressions))
AND ((Magnetic Resonance Angiography) OR (MRI Angiography) OR
(Angiographies, MRI) OR (Angiography, MRI) OR (MRI Angiographies)
OR (MRI Angiographies) OR (Angiographies, Magnetic Resonance) OR
(Magnetic Resonance Angiographies) OR (Perfusion Magnetic Resonance
Imaging) OR (Perfusion Weighted MRI) OR (MRI, Perfusion Weighted)
OR (time-of-flight))’. Articles published from the inception of
each database to September 2022 were retrieved.
After deleting duplicate publications, reasonable
inclusion and exclusion criteria were developed to review the
remaining studies. The inclusion criteria were as follows: i) The
study used 3D MIF technology based on 3D TOF MRA combined with HR
T2WI to judge NVC in patients with TN or HFS; ii) the study design
was prospective or retrospective; and iii) the intraoperative
findings were used as the reference standard for NVC diagnosis. The
exclusion criteria were as follows: i) Reviews, case reports,
editorials, correspondences, comments or meeting abstracts/meeting
minutes; ii) 3D MIF technology was not used in the study, or 3D TOF
MRA combined with HR T2WI was not used to fuse the multimodal
image; iii) the patients in the study received only preoperative
evaluation but not MVD; and iv) studies without sufficient data to
construct the 2x2 contingency table.
Data extraction
A total of two investigators (BZ and RL)
independently extracted the data, including the quality assessment
of the retrieved studies. Discrepancies were resolved in a
consensus meeting, or if no agreement could be reached, such as
regarding the methodological quality of the included studies, they
were resolved by referral to a third investigator (SG). The
extracted data included the following: i) Basic research
information, including the name of the first author, publication
year, country of the first author, sample size and type of research
design; ii) the characteristics of the participants, including the
age of the patients and their diagnosis; iii) the MRI sequences
used in the study; iv) the 3D fusion software used in the study;
and v) the research results, including the number of true
positives, false positives, false negatives, true negatives,
sensitivity and specificity.
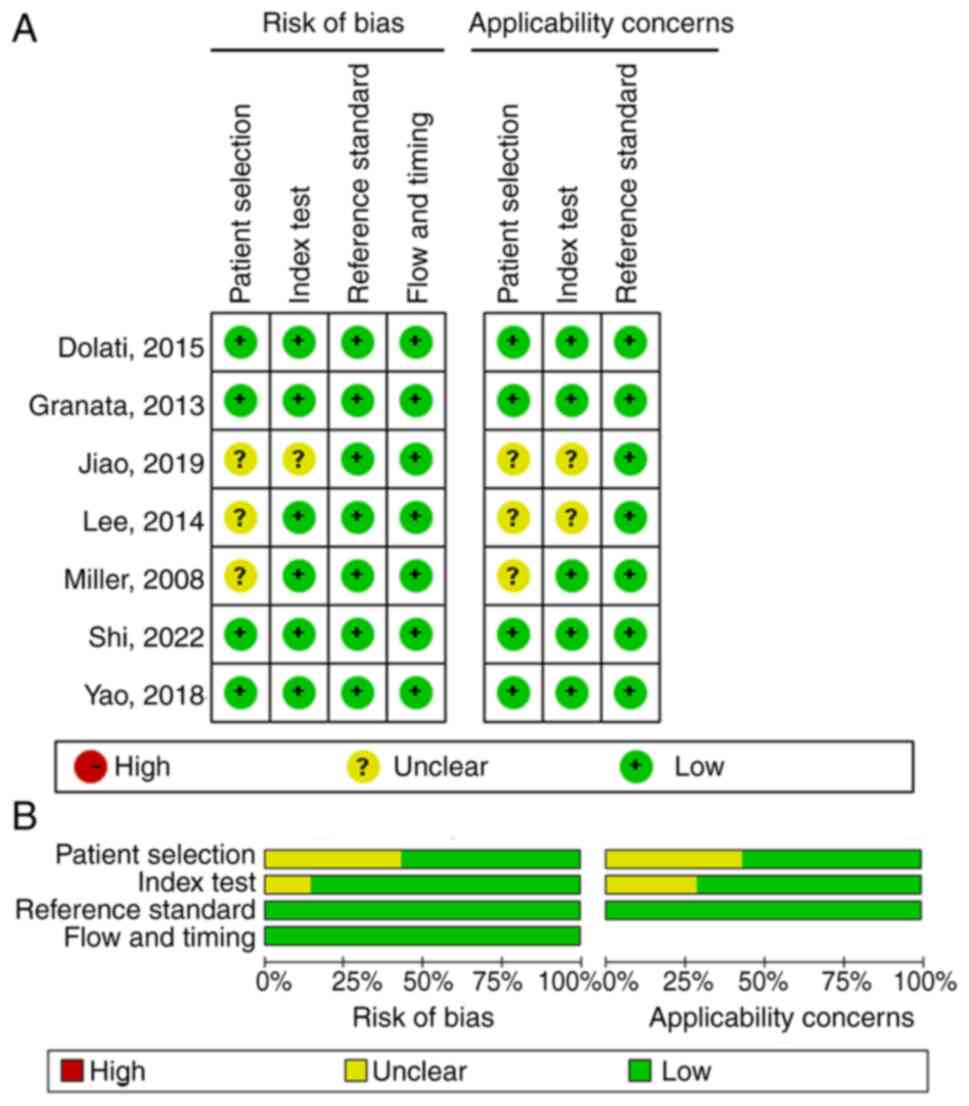
Literature quality assessment
The methodological quality of the included studies
was assessed by two researchers on the basis of the Quality
Assessment of Diagnostic Accuracy Studies (QUADAS) checklist
(11). Review Manager 5.4.1
software (The Cochrane Collaboration) was used to generate a
methodological quality graph and methodological quality graph
summary.
Statistical analysis
An exact binomial rendition of the bivariate
mixed-effects regression model was used to synthesize data. The
data analysis was performed using the meta-analytical integration
of diagnostic test accuracy studies (MIDAS) module of Stata 16.0
software (StataCorp LP). The pooled sensitivity, specificity,
positive likelihood ratio (PLR), negative likelihood ratio (NLR),
diagnostic odds ratio (DOR), area under the receiver operating
characteristic curve (AUROC) and 95% CIs were calculated. The I²
and Q-test were used to assess heterogeneity. The publication bias
of the included literature was examined by Deeks' test using Stata
16.0. The clinical application value of 3D MIF based on 3D TOF MRA
combined with HR T2WI for the diagnosis of NVC was evaluated by
Fagan nomogram and likelihood ratio (LR) scatter plot. Graphs were
produced using the MIDAS module for Stata 16.0 and Review Manager
5.4.1 software.
Results
Included articles
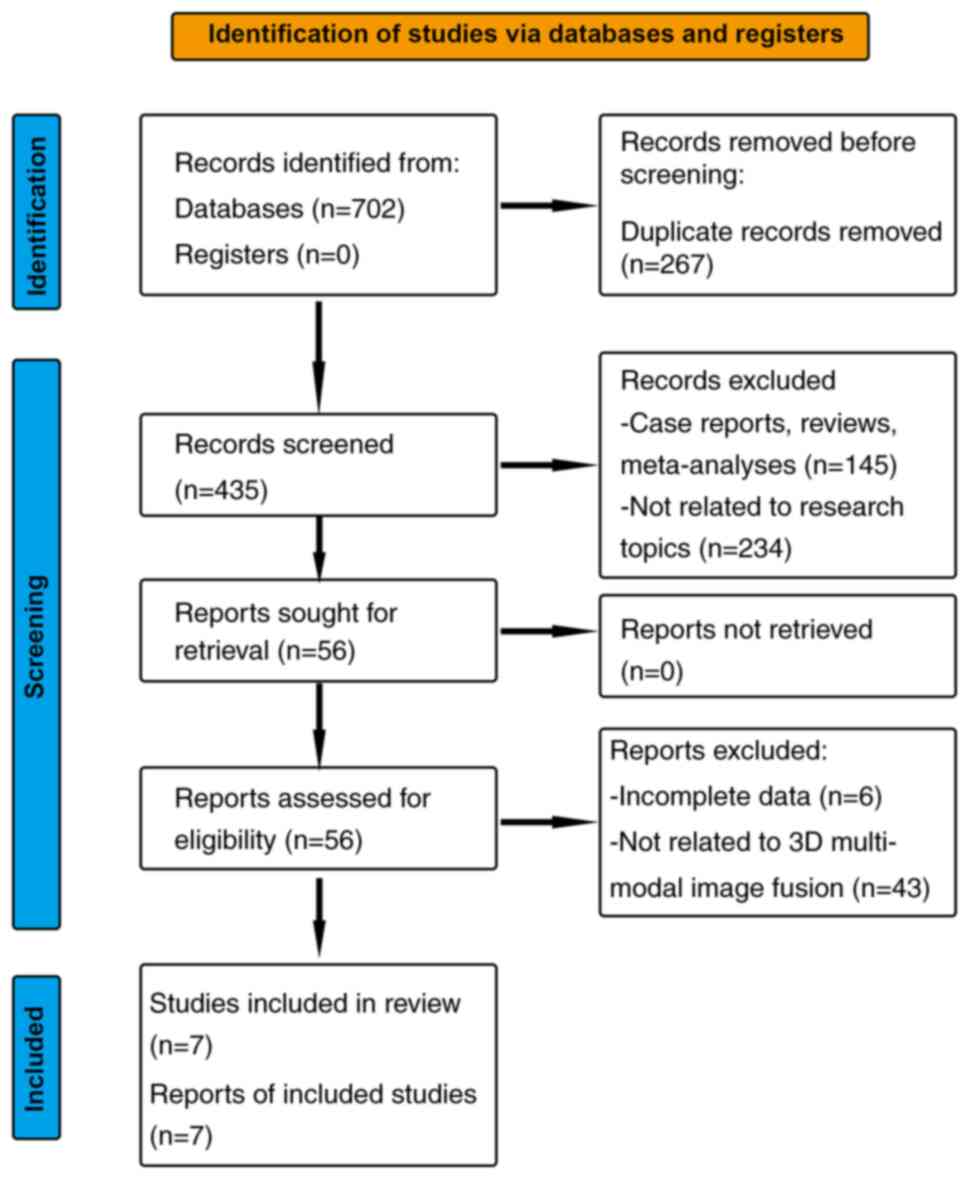
In the search, 702 articles were identified, with
435 articles remaining after discarding duplicate records. A
full-text analysis was performed on the 56 articles that remained
following screening by titles and abstracts, of which 6 articles
did not have complete data and 43 articles were not related to 3D
MIF or 3D TOF MRA combined with HR T2WI, and were therefore
excluded. Finally, 7 articles were included in the present analysis
(Fig. 1).
Basic characteristics of the included
studies
The basic characteristics of the studies included in
the present meta-analysis are presented in Table I. A total of 390 patients were
included in the seven studies. Among them, three studies (12-14)
focused on TN, one (8) on HFS and
three (9,15,16)
on both. A total of two (8,12) of
the seven studies performed 3D TOF MRA combined with the 3D FIESTA
sequence, two (9,15) performed 3D TOF MRA combined with
the 3D SPACE sequence, one (13)
performed 3D TOF MRA combined with bFFE sequence, one (14) performed 3D TOF MRA combined with
bFFE and 3D Gd-enhanced spoiled gradient recalled sequence, and one
(16) performed 3D TOF MRA
combined with the 3D CISS sequence. A total of three (8,9,12) of
the seven studies used 3D-slicer software (17) for 3D MIF, two (13,14)
used OsiriX 2.5.1 software (Pixmeo SARL), and the remaining two
used iPlan Net (Brainlab AG) (15)
software and Leonardo™ (Siemens AG) software (16), respectively. A total of four
studies (9,14-16)
were performed as prospective studies and the remaining three as
retrospective studies. According to the methodological quality
graph (Fig. 2A) and the
methodological quality summary (Fig.
2B), the quality of the literature included in the present
study was acceptable.
 | Table IBasic characteristics of the included
studies. |
Table I
Basic characteristics of the included
studies.
| First author,
year | Country | Sample size | Age, years | Diagnosis | Research type | MRI sequences | 3D fusion
software | True-pos | False-pos | False-neg | True-neg | Sensitivity | Specificity | (Refs.) |
|---|
| Shi, 2022 | China | 40 | 49.6 (24-66) | HFS | Retrospective | 3D TOF MRA + 3D
FIESTA | 3D-slicer | 38 | 1 | 0 | 1 | 1.00 | 0.50 | (8) |
| Jiao, 2019 | China | 48 | ND | TGN | Retrospective | 3D TOF MRA + 3D
FIESTA | 3D-slicer | 46 | 0 | 1 | 1 | 0.98 | 1.00 | (12) |
| Yao, 2018 | China | 42 | 51.2±11.6
(22-76) | TGN/HFS | Prospective | 3D TOF + 3D
SPACE | 3D-slicer | 40 | 0 | 1 | 1 | 0.98 | 1.00 | (9) |
| Dolati, 2015 | USA | 14 | 65±10 | TGN | Prospective | 3D TOF + 3D
SPACE | iPlan Net | 19 | 0 | 0 | 1 | 1.00 | 1.00 | (15) |
| Dolati, 2015 | USA | 6 | 61±7 | HFS | | | | | | | | | | (15) |
| Lee, 2014 | USA | 190 | 56±14.2 | TGN | Retrospective | 3D TOF + bFFE | OsiriX | 148 | 5 | 6 | 31 | 0.96 | 0.86 | (13) |
| Miller, 2008 | USA | 18 | 52.9 (26-80) | TGN | Prospective | 3D TOF + bFFE + 3D
Gd-enhanced SPGR | OsiriX | 15 | 0 | 1 | 2 | 0.94 | 1.00 | (14) |
| Granata, 2013 | Italy | 32 | 42±7 (23-68) | TGN/HFS | Prospective | 3D TOF + 3D
CISS | Leonardo | 21 | 0 | 0 | 11 | 1.00 | 1.00 | (16) |
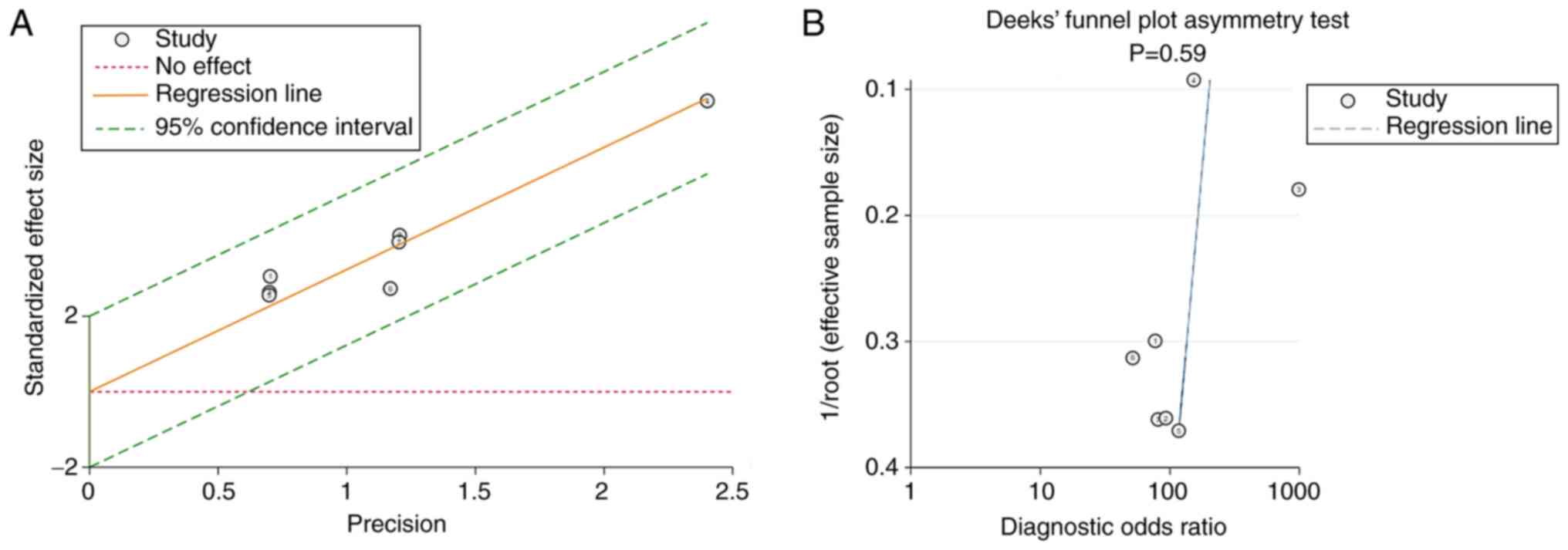
Meta-analysis results. Heterogeneity
of the meta-analysis
The I2 and Q-test were used to assess the
heterogeneity of the studies. The results indicated that the
studies in the present meta-analysis had no substantial
heterogeneity (I2=0; Q=0.000; P=0.50). The same result
was observed from the Galbraith plot (Fig. 3A).
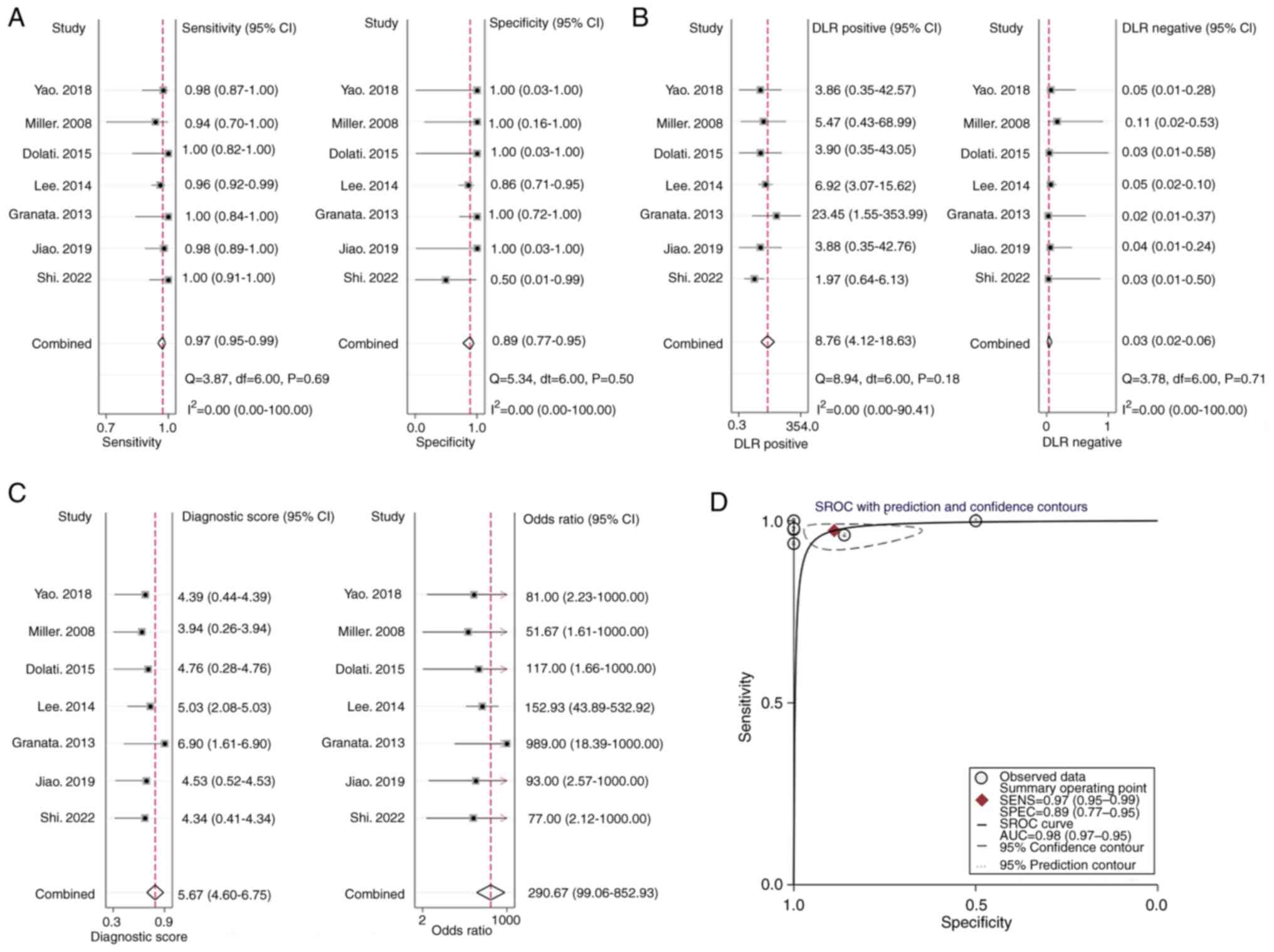
Summary effect size
Bivariate analysis yielded that the pooled
sensitivity and specificity of 3D MIF based on 3D TOF MRA combined
with HR T2WI for detecting NVC were 0.97 (95% CI, 0.95-0.99) and
0.89 (95% CI, 0.77-0.95), respectively (Fig. 4A). The pooled PLR was 8.8 (95% CI,
4.1-18.6), the pooled NLR was 0.03 (95% CI, 0.02-0.06; Fig. 4B) and the pooled DOR was 291 (95%
CI, 99-853; Fig. 4C). The AUROC
was 0.98 (95% CI, 0.97-0.99; Fig.
4D).
Publication bias
The Deeks' funnel plot asymmetry test was used to
evaluate the publication bias of the studies in the current
meta-analysis, with P=0.59 indicating no significant publication
bias in the included studies (Fig.
3B).
Sensitivity analysis
Sensitivity analysis was carried out by deleting
each included study one by one and calculating the respective
summary effect size. The pooled sensitivity and AUROC were used as
evaluation indicators. The results suggested that excluding any
study did not significantly change the pooled sensitivity and AUROC
(Table II), indicating that the
results of the present meta-analysis were robust and reliable.
| Table IISensitivity analysis. |
Table II
Sensitivity analysis.
| First author of
excluded study, year | Pooled sensitivity
(95% CI) | Pooled AUROC (95%
CI) | (Refs.) |
|---|
| Shi, 2022 | 0.97
(0.93-0.99) | 0.98
(0.97-0.99) | (8) |
| Jiao, 2019 | 0.97
(0.95-0.99) | 0.98
(0.97-0.99) | (12) |
| Yao, 2018 | 0.97
(0.95-0.99) | 0.98
(0.97-0.99) | (9) |
| Dolati, 2015 | 0.97
(0.95-0.99) | 0.98
(0.97-0.99) | (15) |
| Lee, 2014 | 0.98
(0.95-1.00) | 0.99
(0.98-1.00) | (13) |
| Miller, 2008 | 0.97
(0.95-0.99) | 0.98
(0.97-0.99) | (14) |
| Granata, 2013 | 0.97
(0.95-0.99) | 0.98
(0.96-0.99) | (16) |
Evaluation of clinical application
value
The LR scatter plot based on summary PLR and NLR was
in the lower left quadrant (Fig.
5A). According to the data of the present meta-analysis, the
incidence rate of NVC in patients with TN and HFS was estimated to
be 86.15%, which was consistent with the reported results (18). Therefore, with a pretest
probability of 0.86, the Fagan nomogram indicated that the positive
post-test probability was 98% and the negative post-test
probability 16% (Fig. 5B).
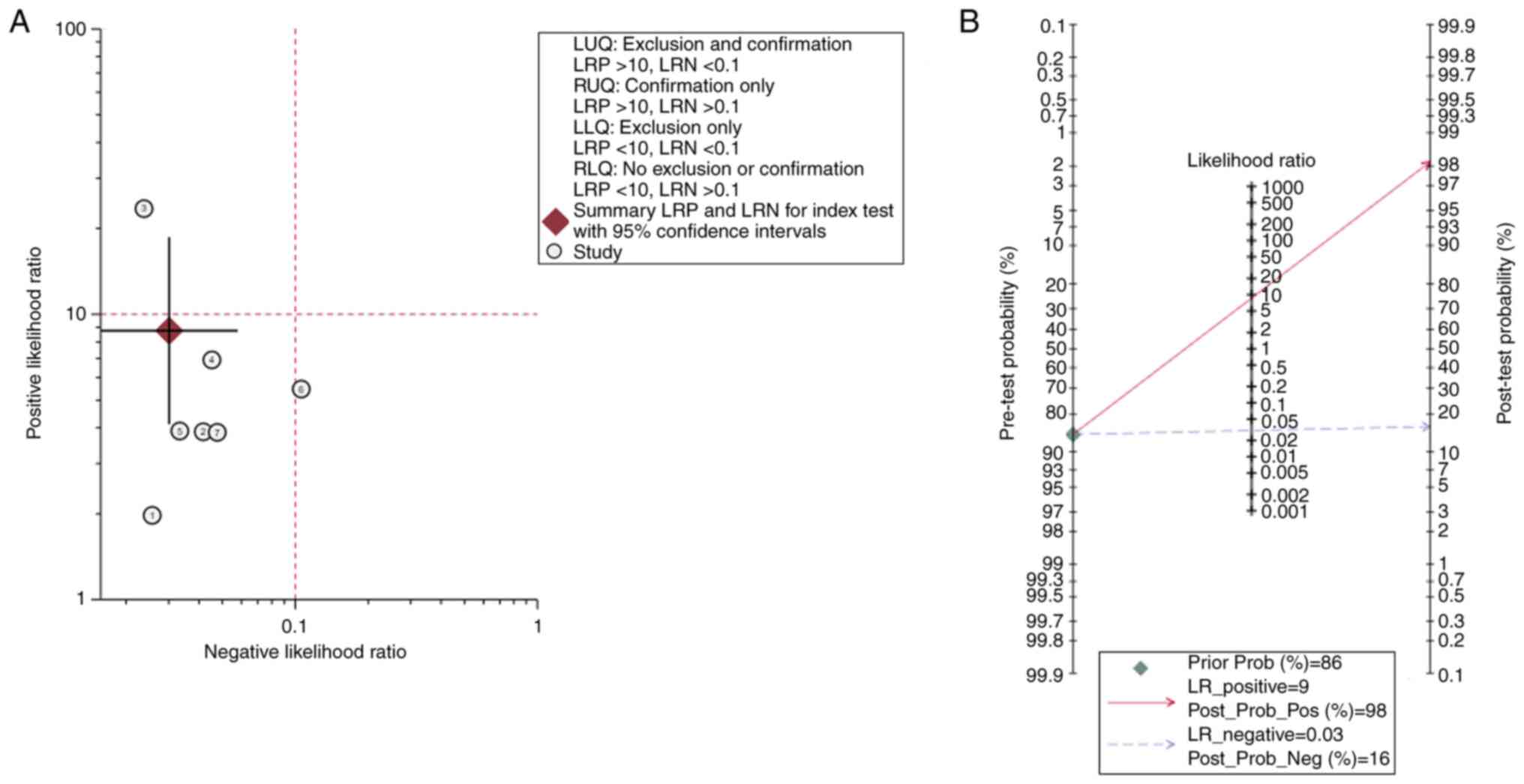 | Figure 5Assessment of the clinical application
value of 3D multimodal image fusion based on time-of-flight
magnetic resonance angiography combined with high-resolution
T2-weighted imaging. (A) Likelihood ratio scatter plot. (B) Fagan
nomogram showing the post-test probability. LUQ, left upper
quadrant; LRP, likelihood ratio positive; LRN, likelihood ratio
negative; RUQ, right upper quadrant; LLQ, left lower quadrant; RLQ,
right lower quadrant; LR, likelihood ratio; Prob, probability; Pos,
positive; Neg, negative. |
Discussion
In the present meta-analysis, the sensitivity,
specificity, PLR, NLR, DOR and AUROC of 3D MIF based on 3D TOF MRA
combined with HR T2WI for detecting NVC were examined. The results
demonstrated a high diagnostic ability of this technology with high
sensitivity and specificity. As mentioned above, 3D TOF MRA is a
widely used MRI sequence for detecting NVC, which is frequently
used as a standard MRI-based method to compare with other methods.
In a previous meta-analysis, the authors reported that 3D TOF MRA
exhibited a sensitivity of 0.95 (95% CI, 0.93-0.96) and specificity
of 0.77 (95% CI, 0.66-0.86) in correctly identifying NVC in
patients with TN (19). According
to the present results, when using 3D MIF technology, the
sensitivity and specificity in diagnosing NVC was able to be
improved. In a previous report, the DOR and AUROC of 3D TOF MRA in
diagnosing NVC were 52.92 (95% CI, 26.39-106.11) and 0.97 (95% CI,
0.95-0.99), respectively (19).
Compared with 3D TOF MRA, the DOR of 3D MIF technology based on 3D
TOF MRA combined with HR T2WI reached 291 (95% CI, 99-853) and the
AUROC was 0.98 (95% CI, 0.97-0.99). These results suggested that
compared with 3D TOF MRA, 3D MIF technology based on 3D TOF MRA
combined with HR T2WI appears to have more advantages in diagnosing
NVC in terms of diagnostic accuracy. In addition, whether 3D MIF is
able to actually improve the effectiveness of 3D TOF MRA combined
with HR T2 in the diagnosis of NVC is also of great concern. In
another meta-analysis, the sensitivity and specificity of 3D TOF
MRA combined with HR T2WI in diagnosing NVC were 0.96 (95% CI,
0.92-0.98) and 0.92 (95% CI, 0.74-0.98), respectively, and the DOR
and AUROC were 283 (95% CI, 50-1,620) and 0.98 (95% CI 0.97-0.99),
respectively (20). Compared with
the results of the present study, the sensitivity and DOR of the
diagnosis of NVC appear to be improved after the combination of 3D
MIF technology. However, it is not accurate to evaluate the
diagnostic effectiveness of different methods by directly comparing
the values of different meta-analysis results. In a network
meta-analysis, different NVC diagnostic methods were evaluated by
constructing statistical models, and the results indicated that 3D
MIF based on 3D TOF MRA combined with HR T2WI did have a higher
superiority index in diagnosing NVC compared with the simple
combination of the aforementioned MRI sequences without 3D MIF
(21). These results suggested
that 3D MIF technology may indeed improve the efficiency of NVC
diagnosis.
To date, to the best of our knowledge, no
meta-analysis has been published on HR T2WI as another type of MRI
sequence commonly used in the detection of NVC. Therefore, there
are no indicators that may accurately reflect the ability of HR
T2WI to detect NVC, such as the pooled sensitivity, specificity,
PLR, NLR, DOR and AUROC. According to existing clinical studies,
the range of sensitivity and specificity of HR T2 WI in the
detection of NVC are 86.17-100 and 71.47-100%, respectively
(22-25).
The results of different studies vary widely, which may be due to
the use of different HR T2WI techniques and study designs. The
value of HR T2WI in detecting NVC requires to be evaluated by
further meta-analyses or large-scale clinical studies. Current data
cannot be used to directly compare the ability of HR T2WI and 3D
MIF based on 3D TOF MRA combined with HR T2WI to detect NVC.
Furthermore, the post-test probabilities are also
associated with the clinical diagnostic ability of the diagnostic
test (26). In the present study,
the post-test probability for a positive test result was 98%,
indicating the high clinical application value of 3D MIF based on
3D TOF MRA combined with HR T2WI in diagnosing NVC. The LR scatter
plot is a qualitative effect size rating approach for diagnostic
test accuracy, which divides the effect rating of diagnostic tests
by quadrant (27). The LR scatter
plot based on summary PLR and NLR was in the lower left quadrant.
This meant that 3D MIF based on 3D TOF MRA combined with HR T2WI
has the ability to exclude the diagnosis of NVC and that the
diagnostic accuracy of this test has a ‘moderate’ effect rating. In
combination, the above two results suggested that 3D MIF based on
3D TOF MRA combined with HR T2WI had a good clinical application
value in diagnosing NVC.
For 3D MIF, the selection of MR sequences for fusion
also affects the final diagnostic effect. Since the combination of
3D TOF MRA and HR T2WI has several advantages in detecting NVC
(28,29), it may add to the advantages of 3D
MIF technology. In fact, this is also the most commonly used
combination of MRI sequences in 3D MIF clinical studies to detect
NVC (8,9,12-16).
There are currently few studies on the use of other MRI sequence
combinations for 3D MIF in the detection of NVC (30). However, with the development of MR
technology, other more suitable MRI sequence combinations may
appear.
The present meta-analysis had certain limitations:
i) NVC may also cause glossopharyngeal neuralgia (GN), but due to
the lack of relevant clinical research data, patients with GN were
not included in the current meta-analysis; ii) due to the limited
number of cases, subgroup analyses were not performed for different
diseases, T2 sequences or 3D fusion software; iii) of the seven
included studies, three were retrospective studies, which have more
potential sources of bias and confounding than prospective
studies.
In conclusion, the present results suggested that 3D
MIF based on 3D TOF MRA combined with HR T2WI has excellent
sensitivity and specificity for detecting NVC in patients with TN
or HFS. This method should serve a key role in the preoperative
evaluation of MVD.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by a grant from the Key
Research and Development Plan of Shaanxi Province, China (grant no.
2021SF-298).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CL was responsible for writing the main manuscript
and data analysis. CL and LY contributed to the study design. BZ,
SG and RL contributed to the literature search, data extraction and
quality assessment. CL and SG confirm the authenticity of all the
raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Broggi M, Acerbi F, Ferroli P, Tringali G,
Schiariti M and Broggi G: Microvascular decompression for
neurovascular conflicts in the cerebello-pontine angle: which role
for endoscopy? Acta Neurochir (Wien). 155:1709–1716.
2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Cui Z and Ling Z: Advances in
microvascular decompression for hemifacial spasm. J Otol. 10:1–6.
2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Sade B and Lee JH: Microvascular
decompression for trigeminal neuralgia. Neurosurg Clin N Am.
25:743–749. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Montano N, Conforti G, Di Bonaventura R,
Meglio M, Fernandez E and Papacci F: Advances in diagnosis and
treatment of trigeminal neuralgia. Ther Clin Risk Manag.
11:289–299. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Chen SR: Neurological Imaging for
Hemifacial Spasm. Int Ophthalmol Clin. 58:97–109. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Donahue JH, Ornan DA and Mukherjee S:
Imaging of Vascular Compression Syndromes. Radiol Clin North Am.
55:123–138. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Huang B, Yang F, Yin M, Mo X and Zhong C:
A Review of multimodal medical image fusion techniques. Comput Math
Methods Med. 2020(8279342)2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Shi H, Li Y, Wang Y, Guo W, Zhang K, Du Y,
Shi H and Qian T: The preoperative evaluation value of 3D-slicer
program before microsurgical vascular decompression in patients
with hemifacial spasm. Clin Neurol Neurosurg.
217(107241)2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Yao S, Zhang J, Zhao Y, Hou Y, Xu X, Zhang
Z, Kikinis R and Chen X: Multimodal image-based virtual reality
presurgical simulation and evaluation for trigeminal neuralgia and
hemifacial spasm. World Neurosurg. 113:e499–e507. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. BMJ. 372(n71)2021.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
Whiting PF, Rutjes AW, Westwood ME,
Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA, Bossuyt PM
and QUADAS-2 Group: QUADAS-2: A revised tool for the quality
assessment of diagnostic accuracy studies. Ann Intern Med.
155:529–536. 2011.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Jiao Y, Duan F, Yan Z, Meng Q and Feng Y:
The value of 3D-TOF-MRA and 3D-FIESTA fusion three-dimensional
images in judgment of offending vessel in primary trigeminal
neuralgia. Chin J Neurosurg. 35:928–932. 2019.
|
|
13
|
Lee A, McCartney S, Burbidge C, Raslan AM
and Burchiel KJ: Trigeminal neuralgia occurs and recurs in the
absence of neurovascular compression Clinical article. J Neurosurg.
120:1048–1054. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Miller J, Acar F, Hamilton B and Burchiel
K: Preoperative visualization of neurovascular anatomy in
trigeminal neuralgia. J Neurosurg. 108:477–482. 2008.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Dolati P, Golby A, Eichberg D, Abolfotoh
M, Dunn IF, Mukundan S, Hulou MM and Al-Mefty O: Pre-operative
image-based segmentation of the cranial nerves and blood vessels in
microvascular decompression: Can we prevent unnecessary
explorations? Clin Neurol Neurosurg. 139:159–165. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Granata F, Vinci SL, Longo M, Bernava G,
Caffo M, Cutugno M, Morabito R, Salamone I, Tomasello F and Alafaci
C: Advanced virtual magnetic resonance imaging (MRI) techniques in
neurovascular conflict: Bidimensional image fusion and virtual
cisternography. Radiol Med. 118:1045–1054. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Fedorov A, Beichel R, Kalpathy-Cramer J,
Finet J, Fillion-Robin JC, Pujol S, Bauer C, Jennings D, Fennessy
F, Sonka M, et al: 3D Slicer as an image computing platform for the
quantitative imaging network. Magn Reson Imaging. 30:1323–1341.
2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Bašić Kes V and Zadro Matovina L:
Accommodation to diagnosis of trigeminal neuralgia. Acta Clin
Croat. 56:157–161. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Cai J, Xin ZX, Zhang YQ, Sun J, Lu JL and
Xie F: Diagnostic value of 3D time-of-flight MRA in trigeminal
neuralgia. J Clin Neurosci. 22:1343–1348. 2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Liang C, Yang L, Zhang BB, Guo SW and Li
RC: Three-dimensional time-of-flight magnetic resonance angiography
combined with high resolution T2-weighted imaging in preoperative
evaluation of microvascular decompression. World J Clin Cases.
10:12594–12604. 2022.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Liang C, Yang L, Reichardt W, Zhang B and
Li R: Different MRI-based methods for the diagnosis of
neurovascular compression in trigeminal neuralgia or hemifacial
spasm: A network meta-analysis. J Clin Neurosci. 108:19–24.
2022.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Xia H, Kong M, Lu H, Luo S, Xu D and Zhang
J: Value of MR 3D FLASH-WE combined with 3D SPACE sequences applied
in cranial nerve diseases. Chin Comput Med Imaging. 21:505–509.
2015.(In Chinese).
|
|
23
|
Jia JM, Guo H, Huo WJ, Hu SW, He F, Sun XD
and Lin GJ: Preoperative evaluation of patients with hemifacial
spasm by three-dimensional time-of-flight (3D-TOF) and
three-dimensional constructive interference in steady state
(3D-CISS) sequence. Clin Neuroradiol. 26:431–438. 2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Ruiz-Juretschke F, Guzmán-de-Villoria JG,
García-Leal R and Sañudo JR: Predictive value of magnetic resonance
for identifying neurovascular compressions in trigeminal neuralgia.
Neurologia. 34:510–519. 2019.PubMed/NCBI View Article : Google Scholar : (In English,
Spanish).
|
|
25
|
Yang D, Shen J, Xia X, Lin Y, Yang T, Lin
H, Jin Y, Zhou K and Li Y: Preoperative evaluation of neurovascular
relationship in trigeminal neuralgia by three-dimensional fast low
angle shot (3D-FLASH) and three-dimensional constructive
interference in steady-state (3D-CISS) MRI sequence. Br J Radiol.
91(20170557)2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Gogtay NJ: Statistical evaluation of
diagnostic tests-part 2 (pre-test and post-test probability and
odds, likelihood ratios, receiver operating characteristic curve,
Youden's index and diagnostic test biases). J Assoc Physicians
India. 65:86–91. 2017.PubMed/NCBI
|
|
27
|
Rubinstein ML, Kraft CS and Parrott JS:
Determining qualitative effect size ratings using a likelihood
ratio scatter matrix in diagnostic test accuracy systematic
reviews. Diagnosis. 5:205–214. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Singhal S and Danks RA: Radiologic and
neurosurgical diagnosis of arterial neurovascular conflict on
magnetic resonance imaging for trigeminal neuralgia in routine
clinical practice. World Neurosurg. 157:e166–e172. 2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Wei Sheng C, Yu R, Meng Q and Qu C:
Efficacy of microvascular decompression in patients with trigeminal
neuralgia with negative neurovascular relationship shown by
magnetic resonance tomography. Clin Neurol Neurosurg.
197(106063)2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Ogiwara M and Shimizu T: Surface rendered
three-dimensional MR imaging for the evaluation of trigeminal
neuralgia and hemifacial spasm. J Clin Neurosci. 11:840–844.
2004.PubMed/NCBI View Article : Google Scholar
|