Introduction
Camrelizumab is an anti-programmed cell death-1
(PD-1) antibody that is uniquely associated with the
treatment-related adverse event of reactive cutaneous capillary
endothelial proliferation (RCCEP) (1-3).
Most RCCEPs occur in the skin (2),
where the incidence rate may be as high as 85.7%, as found in one
study on patients treated with camrelizumab (4). Although RCCEP is self-limited, it may
persist in certain patients with continuous drug use, and only
after drug withdrawal, spontaneous atrophy or necrosis may occur
and the lesions fall off. RCCEP is classified into five levels by
the Chinese National Medical Products Administration (5), namely ‘red-nevus-like’, ‘pearl-like’,
‘mulberry-like’, ‘patch-like’ and ‘tumor-like’. This condition
manifests as bleeding nodules and may seriously affect a person's
self-image and quality of life. Although there have been numerous
studies on the treatment of RCCEP using methods such as laser or
surgical resection (5), the
lesions may be scattered and numerous, rendering local treatment
insufficient. It was previously reported that the incidence of
RCCEP is lower in patients receiving anti-angiogenic drugs;
however, this notion remains controversial (6). As such, the development of effective
treatment regimens for patients with RCCEP is an urgent unmet
medical need in the era of immunotherapy.
Thalidomide is a synthetic glutamate derivative that
has potential anti-angiogenic and anti-neoplastic effects, although
its mechanisms of action in this regard have remained elusive. It
may reduce the expression of interleukin (IL)-6, IL-1β, tumor
necrosis factor-α (TNF-α), basic fibroblast growth factor (bFGF),
vascular endothelial growth factor (VEGF) or cell surface adhesion
molecules in stromal cells (7).
Furthermore, thalidomide is able to immunomodulate T cells, enhance
anti-plasma cell cytotoxicity of natural killer cells, inhibit
cyclooxygenase-2 and induce an anti-angiogenic effect that may
potentially lead to appreciable anti-tumor activity (8). A series of studies have indicated
that thalidomide has encouraging anti-angiogenic activities in
several types of cancer, including prostate cancer and multiple
myeloma (9-11).
Recently, Song et al (12)
reported that thalidomide prevents camrelizumab-induced RCCEP.
Providing further evidence in support of these findings, the
present study reported on a patient with RCCEP who successfully
responded to low-dose oral thalidomide (100 mg administered every
night).
Case report
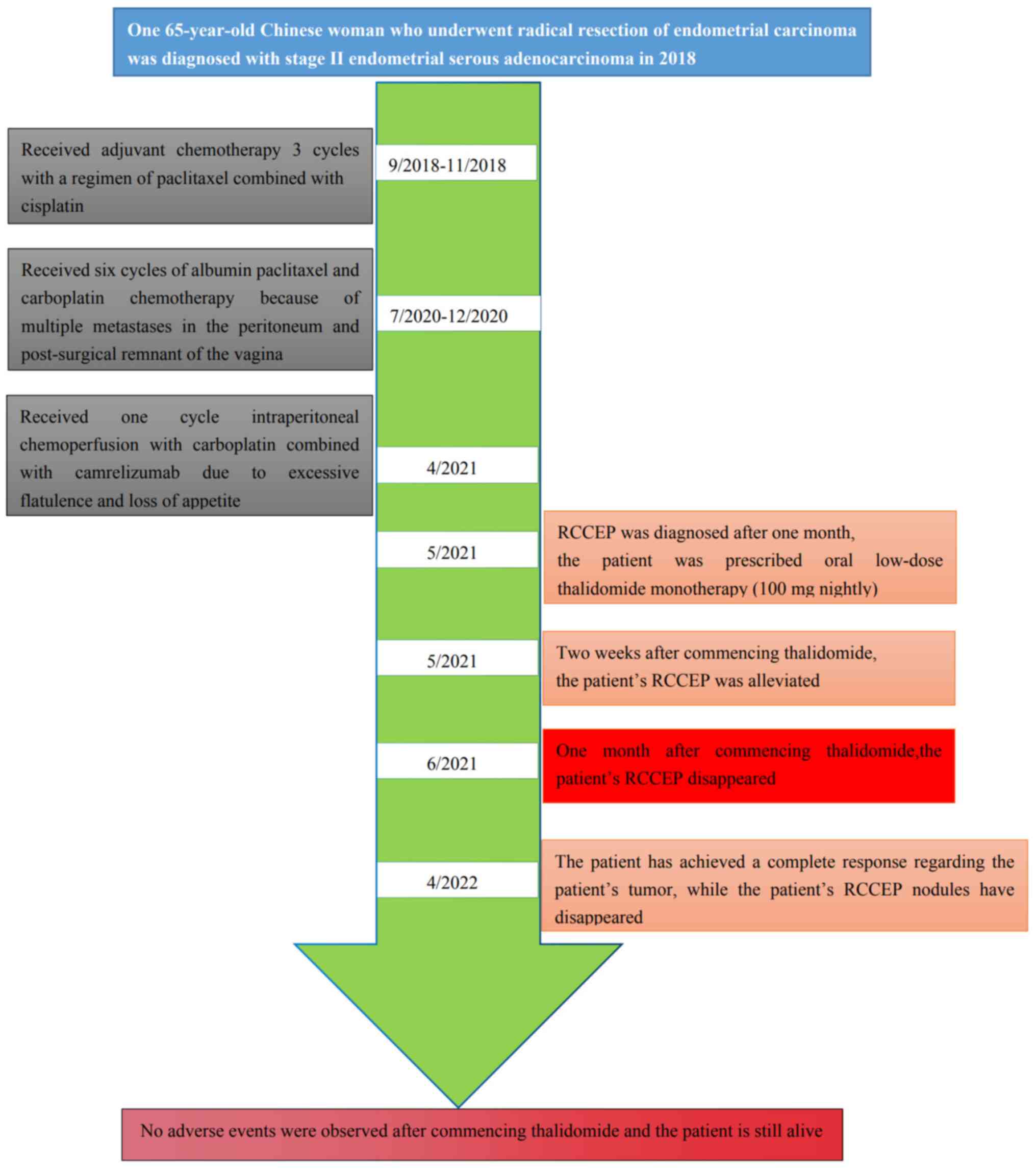
In September 2018, a 65-year-old Chinese female
underwent radical resection of endometrial carcinoma at the First
People's Hospital of Yibin (Yibin, China). The pathological
diagnosis was International Federation of Gynecology and Obstetrics
stage II endometrial serous adenocarcinoma. At two weeks after the
surgery, the patient received chemotherapy comprising paclitaxel
combined with cisplatin (three cycles) as adjuvant therapy. In July
2020, multiple metastases in the peritoneum and post-surgical
remnant of the vagina were detected by magnetic resonance imaging
and computed tomography (CT). The patient then received six cycles
of albumin paclitaxel and carboplatin chemotherapy. The patient
also underwent radiotherapy (volumetric modulated arc therapy; 60
Gy via 25 fractions of 2.4 Gy each), including vaginal
brachytherapy (30 Gy via 5 fractions of 6 Gy each). In April 2021,
the patient complained of excessive flatulence and loss of
appetite; upon examination, adenocarcinoma cells were found in the
seroperitoneum. Given this recurrence, the patient underwent
intraperitoneal chemoperfusion with carboplatin after having
refused intravenous chemotherapy for systemic treatment. At the
same time, the patient was prescribed camrelizumab after it was
discovered that the tumor was positive for PD-1. After one month,
the flatulence and loss of appetite subsided; however, the patient
complained that the skin of her face and torso was scattered with
several punctured vascular nodules ~1-2 mm in size. The patient's
medical timeline is presented in Fig.
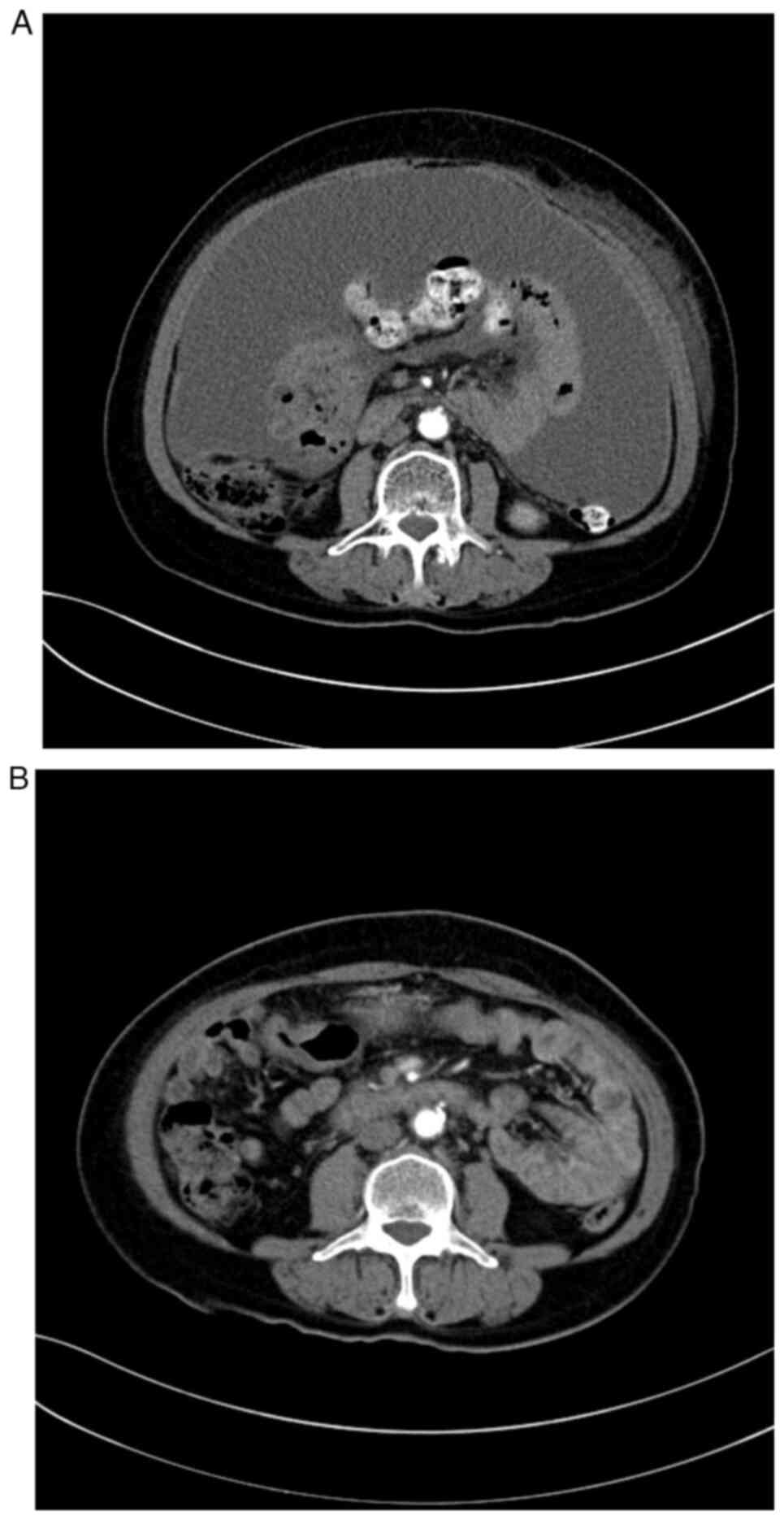
1. The CT images prior to and after the treatment for the
recurrence are presented in Fig.
2A and B, respectively.
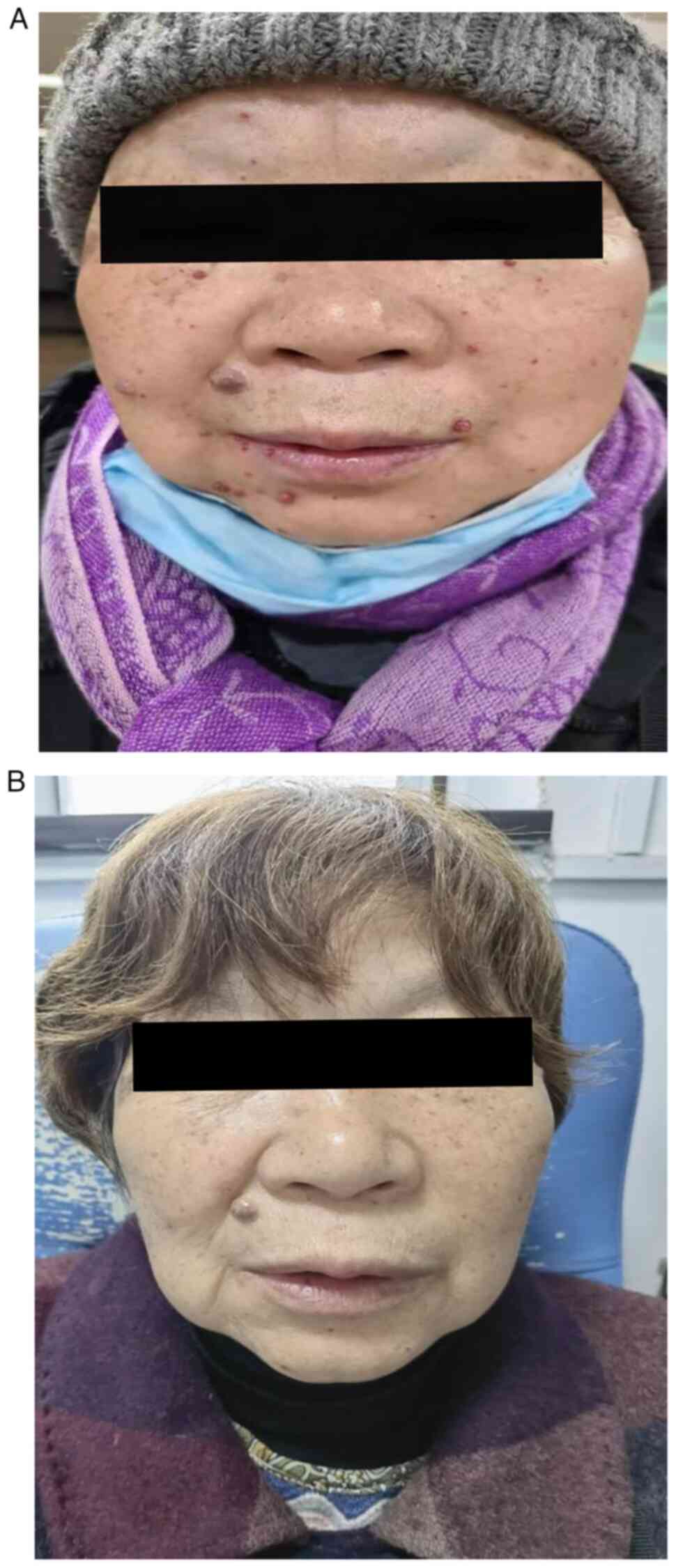
The size and number of angio-proliferations
increased during subsequent treatment, with certain nodules
erupting when touched (Fig. 3A).
Nodules ranged from 1-2 mm in size. Multiple nodules were fused
into a pearl of ~3x5 mm and were bright red, soft and hemorrhaging.
The patient was therefore diagnosed with RCCEP. There was no
obvious improvement despite the patient avoiding scratching or
rubbing the nodules and protecting them from any contact. It was
decided to prescribe oral thalidomide (100 mg every night). After
one month, the RCCEP disappeared (Fig.
3B). Therefore, no discontinuation or dose reduction of
camrelizumab was necessary. In May 2021, 1 month after treatment
for a second recurrence, the patient's performance status had also
improved under a combination of camrelizumab and thalidomide. In
April 2022, The patient achieved a complete tumor response and the
RCCEP nodules disappeared.
Discussion
Immune checkpoint inhibitors (ICIs), particularly
monoclonal antibodies targeting PD-1 or its ligand PD-L1, have
produced marked anti-tumor results when used to treat a variety of
malignancies (13-16).
Despite their effectiveness, however, ICIs are also associated with
adverse events. RCCEP is a common side effect of camrelizumab
(17-19)
that usually occurs on the skin; even low-grade conditions may
easily cause bleeding, affecting the patients' appearance and
quality of life. Reactive capillary endothelial proliferation has
been reported to occur in the oral mucosa (20,21),
but there has been no evidence of its occurrence in visceral
organs. At present, there are global standards for the
classification of adverse reactions of the skin, such as National
Comprehensive Cancer Network and European Society for Medical
Oncology, but RCCEP is the most common side effect of camrelizumab,
which was independently developed in China. Certain other mAb, such
as ramucirumab, Tanibirumab, Nivolumab and Pembrolizumab, have also
been reported to be associated with cutaneous capillary endothelial
proliferation, which is not unique to Cam but varies in terms of
the presentation and incidence of RCCEP (22). Therefore, there is only a Chinese
standard for the classification of RCCEP. The relationship between
immune-related adverse events (irAEs) to immunotherapy and ICI
effectiveness is gradually becoming clearer after certain clinical
trials found that immunotherapy is more effective in patients who
experience such reactions. However, the relationship between
cutaneous irAEs and efficacy is elusive or controversial. For
instance, Huang et al (23)
found that, among 228 patients with advanced and metastatic
esophageal squamous cell carcinoma treated with camrelizumab, the
median survival time of those with RCCEP (n=182) was 10.1 months,
while that of patients without RCCEP (n=46) was only 2.5 months.
Aso et al (24) analyzed
the clinical data of 155 patients with advanced non-small-cell lung
cancer who were treated with nivolumab or pembrolizumab monotherapy
and found that those with adverse skin reactions (n=51) had a
higher objective tumor response rate (57 vs. 19%, P<0.01) and
longer progression-free survival (12.9 vs. 3.5 months, P<0.01)
than those with no such reactions. The patient with RCCEP described
in the present study is still alive and in complete clinical
remission. For this reason, it may be hypothesized that patients
with RCCEP caused by immunotherapy may be expected to have a better
outcome, which aligns with the findings of these other studies.
RCCEP may be related to immunotherapeutic efficacy, and even if it
occurs in patients who are benefitting from treatment, it is not
recommended that immunotherapy is discontinued unless the lesions
bleed profusely and affect a person's appearance, as such
occurrences may seriously affect a patient's quality of life. It is
necessary to increase the immunotherapy compliance rate and avoid
interruptions to gain the maximum benefit; as such, the development
of effective treatments for RCCEP in the era of immunotherapy is an
urgent unmet medical need.
The mechanism of RCCEP remains elusive. It may be
caused by over-activation of immune function due to therapy, which
interferes with the balance between pro- and anti-angiogenic
factors in the skin. CD4+ T-cell activation may be
another mechanism; such activation increases Th2 cytokine IL-4
levels, which in turn stimulates the differentiation of
CD163+ M2 macrophages and promotes vascular
proliferation by releasing VEGF-A (25-27).
It has been hypothesized that the inhibition of angiogenic factors
is able to reduce the occurrence of RCCEP. Combining ICIs with
molecularly targeted drugs such as bevacizumab and apatinib has
also been reported to reduce the incidence of RCCEP, indicating
that blocking the VEGF ligand-receptor signaling pathway and
inhibiting endothelial cell proliferation sufficiently decreases
capillary density to prevent the adverse event (28). However, it remains elusive whether
anti-angiogenic drugs are able to reverse RCCEP that has already
manifested. Furthermore, ICI monotherapy and immunochemotherapy are
currently the most widely used regimens (13-16),
whereas combining anti-angiogenic agents with ICIs is not yet
mainstream and the use of anti-angiogenic drugs to prevent RCCEP
remains controversial. At the same time, anti-angiogenic agents
should not be routinely used to prevent RCCEP, as this may increase
the patient's burden and side effects. Therefore, it may not be
reasonable to prescribe expensive anti-angiogenic drugs to treat
RCCEP and there is an urgent need for non-invasive and inexpensive
drug therapies that may effectively treat RCCEP. To that end, the
patient of the present study demonstrated that low-dose thalidomide
appears to have a curative effect on RCCEP.
Thalidomide is a synthetic glutamate derivative with
two optical isomers, R (dextral) and S (left-handed), at
physiological pH, which inhibit VEGF, bFGF and capillary formation
in a dose-dependent manner; as such, it exerts an anti-angiogenic
effect without changing VEGF-A levels or disturbing the microvessel
density in the dermis (29).
Thalidomide is able to regulate the secretion of other cytokines
induced by TNF-α, thus regulating the immune status of the body
(30). Song et al (12) reported that thalidomide may prevent
camrelizumab-induced RCCEP. The use of anti-angiogenic drugs for
RCCEP prevention remains controversial. At the same time,
anti-angiogenic drugs should not be routinely used for RCCEP
prevention, as they may increase the burden on the patient and side
effects. Consequently, the use of expensive anti-angiogenic drugs
in the treatment of RCCEP may not be reasonable. At present, a
non-invasive and inexpensive drug therapy is urgently needed to
effectively treat RCCEP. Therefore, it is posited that thalidomide
may be used to treat RCCEP. In the present study, it was also found
that RCCEP nodules shrank in size and decreased in number after
thalidomide treatment, and this evidence suggests that blocking
angiogenesis is an important mechanism for RCCEP treatment. In
addition, the surfaces of the nodules became hard and dark after
treatment, indicating reduced hemorrhage; this may indicate that
thalidomide helped ameliorate the abnormal activity of immune cells
against the epidermis and dermis and ultimately reduced dermal
fibrous tissue hyperplasia (31).
In conclusion, low-dose thalidomide monotherapy had
excellent efficacy against RCCEP; the possible mechanism of its
action appears to be angiogenesis blockade and immune regulation.
Preclinical and clinical studies should be developed to further
explore the mechanism, efficacy and appropriate dose of thalidomide
when treating patients with RCCEP.
Acknowledgements
Not applicable.
Funding
Funding: This study was funded by the Sichuan Medical
Association Youth Innovation Project (grant no. Q16082).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request
Authors' contributions
SW conceived and designed the present study. SW and
CW wrote the original draft. KL and YJ performed the analysis and
interpretation of data. ZJ provided administrative, technical and
material support, prepared the figures and edited the manuscript.
All authors have read and approved the final manuscript. CW and KL
confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
The study on a human participant was approved by the
Medical Ethics Committee of the Second People's Hospital of Yibin
(Yibin, China; approval no. 2021-037-01).
Patient consent for publication
The patient provided written informed consent for
the publication of the study and the associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fang W, Yang Y, Ma Y, Hong S, Lin L, He X,
Xiong J, Li P, Zhao H, Huang Y, et al: Camrelizumab (SHR-1210)
alone or in combination with gemcitabine plus cisplatin for
nasopharyngeal carcinoma: Results from two single-arm, phase 1
trials. Lancet Oncol. 19:1338–1350. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mo H, Huang J, Xu J, Chen X, Wu D, Qu D,
Wang X, Lan B, Wang X, Xu J, et al: Safety, anti-tumour activity,
and pharmacokinetics of fixed-dose SHR-1210, an anti-PD-1 antibody
in advanced solid tumours: A dose-escalation, phase 1 study. Br J
Cancer. 119:538–545. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Teng Y, Guo R, Sun J, Jiang Y and Liu Y:
Reactive capillary hemangiomas induced by camrelizumab (SHR-1210),
an anti-PD-1 agent. Acta Oncol. 58:388–389. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Chen X, Ma L, Wang X, Mo H, Wu D, Lan B,
Qu D, Zhang H, Huang J and Xu BH: Reactive capillary hemangiomas: A
novel dermatologic toxicity following anti-PD-1 treatment with
SHR-1210. Cancer Biol Med. 16:173–181. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Chinese Society of Clinical Oncology
(CSCO): Management of Immune Checkpoint Inhibitor-Related Toxicity,
1. People's Health Publishing House, Beijing, 2020.
|
|
6
|
Rispoli M, Savastano MC and Lumbroso B:
Quantitative vascular density changes in choriocapillaris around
CNV after anti-VEGF treatment: Dark halo. Ophthalmic Surg Lasers
Imaging Retina. 49:918–924. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Vacca A, Scavelli C, Montefusco V, Di
Pietro G, Neri A, Mattioli M, Bicciato S, Nico B, Ribatti D,
Dammacco F and Corradini P: Thalidomide downregulates angiogenic
genes in bone marrow endothelial cells of patients with active
multiple myeloma. J Clin Oncol. 23:5334–5346. 2005.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Keifer JA, Guttridge DC, Ashburner BP and
Baldwin AS Jr: Inhibition of NF-kappa B activity by thalidomide
through suppression of IkappaB kinase activity. J Biol Chem.
276:22382–22387. 2001.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Melchert M and List A: The thalidomide
saga. Int J Biochem Cell Biol. 39:1489–1499. 2007.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Raje N and Anderson KC: Thalidomide and
immunomodulatory drugs as cancer therapy. Curr Opin Oncol.
14:635–640. 2002.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Yuan JH, Yang F, Wang F, Ma JZ, Guo YJ,
Tao QF, Liu F, Pan W, Wang TT, Zhou CC, et al: A long noncoding RNA
activated by TGF-β promotes the invasion-metastasis cascade in
hepatocellular carcinoma. Cancer Cell. 25:666–681. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Song G, Zhang FF and Cheng HD: Thalidomide
for prevention of camrelizumab-induced reactive cutaneous capillary
endothelial proliferation. Australas J Dermatol. 63:217–221.
2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Li Q, Zhou Y, He W, Ren X, Zhang M, Jiang
Y, Zhou Z and Luan Y: Platelet-armored nanoplatform to harmonize
janus-faced IFN-γ against tumor recurrence and metastasis. J
Control Release. 338:33–45. 2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Zhang M, Qin X, Zhao Z, Du Q, Li Q, Jiang
Y and Luan Y: A self-amplifying nanodrug to manipulate the
Janus-faced nature of ferroptosis for tumor therapy. Nanoscale
Horiz. 7:198–210. 2022.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Bhardwaj M, Chiu MN and Pilkhwal Sah S:
Adverse cutaneous toxicities by PD-1/PD-L1 immune checkpoint
inhibitors: Pathogenesis, treatment, and surveillance. Cutan Ocul
Toxicol. 41:73–90. 2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Qin S, Ren Z, Meng Z, Chen Z, Chai X,
Xiong J, Bai Y, Yang L, Zhu H, Fang W, et al: Camrelizumab in
patients with previously treated advanced hepatocellular
carcinoma:A multicentre,open-label, parallel-group, randomised,
phase 2 trial. Lancet Oncol. 21:571–580. 2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Mok TSK, Wu YL, Kudaba I, Kowalski DM, Cho
BC, Turna HZ, Castro G Jr, Srimuninnimit V, Laktionov KK,
Bondarenko I, et al: Pembrolizumab versus chemotherapy for
previously untreated, PD-L1-expressing, locally advanced or
metastatic non-small-cell lung cancer(KEYNOT-042):A randomised,
open-label, controlled, phase 3 trail. Lancet. 393:1819–1830.
2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Si L, Zhang X, Shu Y, Pan H, Wu D, Liu J,
Lou F, Mao L, Wang X, Wen X, et al: A phase Ib study of
Pembrolizumab as second-line therapy for Chinese patients with
advanced or metastatic melanoma(KEYNOTE-151). Transl Oncol.
12:828–835. 2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Song Y, Wu J, Chen X, Lin T, Cao J, Liu Y,
Zhao Y, Jin J, Huang H, Hu J, et al: A single-arm, multicenter,
phase II study of camrelizumab in relapsed or refractory classical
hodgkin lymphoma. Clin Cancer Res. 25:7363–7369. 2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wang F, Qin S, Sun X, Ren Z, Meng Z, Chen
Z, Chai X, Xiong J, Bai Y, Yang L, et al: Reactive cutaneous
capillary endothelial proliferation in advanced hepatocellular
carcinoma patients treated with camrelizumab:data derived from a
multicenter phase 2 trial. J Hematol Oncol. 13(47)2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Yu Q and Wang WX: Camrelizumab (SHR-1210)
leading to reactive capillary hemangioma in the gingiva:A case
report. World J Clin Cases. 8:624–629. 2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Qin SK and Wang F: Camrelizumab induced
cutaneous capillary endothelial proliferation Clinical expert
consensus. Chin Clin Oncol. 25:840–846. 2020.(In Chinese).
|
|
23
|
Huang J, Xu J, Chen Y, Zhuang W, Zhang Y,
Chen Z, Chen J, Zhang H, Niu Z, Fan Q, et al: Camrelizumab versus
investigator's choice of chemotherapy as second-line therapy for
advanced or metastatic oesophageal squamous cell carcinoma
(Escort):A multicentre, randomised, open-label, phase 3 study.
Lancet Oncol. 21:832–842. 2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Aso M, Toi Y, Sugisaka J, Aiba T, Kawana
S, Saito R, Ogasawara T, Tsurumi K, Ono K, Shimizu H, et al:
Association between skin reaction and clinical benefit in patients
treated with anti-programmed cell death 1 monotherapy for advanced
non-small cell lung cancer. Oncologist. 25:e536–e544.
2022.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Spratlin JL, Mulder KE and Mackey JR:
Ramucirumab (IMC-1121B):A novel attack on angiogenesis. Future
Oncol. 6:1085–1094. 2010.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lee SJ, Lee SY, Lee WS, Yoo JS, Sun JM,
Lee J, Park HS, Park JO, Ahn MJ, Lim HY, et al: Phase I trial and
pharmacokinetic study of tanibirumab, a fully human monoclonal
antibody to vascular endothelial growth factor receptor 2, in
patients with refractory solid tumors. Invest New Drugs.
35:782–790. 2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ton NC, Parker GJ, Jackson A, Mullamitha
S, Buonaccorsi GA, Roberts C, Watson Y, Davies K, Cheung S, Hope L,
et al: Phase I evaluation of CDP791, a pegylated di-Fab' conjugate
that binds vascular endothelial growth factor receptor2. Clin
Cancer Res. 13:7113–7118. 2007.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Zhou C, Gao G, Wang YN, Zhao J, Chen G,
Liu Z, Gu K, Huang M, He J, Chen J, et al: Efficacy of PD-1
monoclonal antibody SHR-1210 plus Apatinib in patients with
advanced non-squamous NSCLC with wild-type EGFR and ALK. J Clin
Oncol. 35(9112)2019.
|
|
29
|
Salemi M, Mohammadi S, Ghavamzadeh A and
Nikbakht M: Anti-vascular endothelial growth factor targeting by
curcumin and thalidomide in acute myeloid leukemia cells. Asian Pac
J Cancer Prev. 18:3055–3061. 2017.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Bodera P and Stankiewicz W:
Immunomodulatory Properties of Thalidomide Analogs: Pomalidomide
and lenalidomide, experimental and therapeutic applications. Recent
Pat Endocr Metab Immune Drug Discov. 5:192–196. 2011.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Bai YZ, Wang Q, Guo BS, Wang Ax, Zhang LH,
Xue F, Li SY and Li YP: Effects of Thalidomide on the Expression of
Collagen IA1 and Regulatory Factor in Histamine-activated Human
Dermal Fibroblasts. Chin J Derm Venereol. 36:1253–1255. 2022.(In
Chinese).
|