Introduction
The carotid artery, a major blood vessel in the
neck, has a crucial role in supplying blood to the brain, neck and
face. Its anatomical positioning and function make it susceptible
to various pathologies, some of which can be life-threatening. One
such rare pathology is dissecting aneurysm of the carotid artery
associated with the hyoid bone. The hyoid bone, a U-shaped bone
situated in the anterior midline of the neck, is unique, as it is
the only bone in the human body that does not articulate with any
other bone. Instead, it is suspended by muscles and ligaments,
giving it mobility that may, in rare instances, lead to mechanical
interference with nearby structures. Dissecting aneurysm of the
carotid artery associated with the hyoid bone is rare. Mechanical
interference between the hyoid bone and the carotid artery has
previously been reported as a cause for stenosis (1,2),
pseudoaneurysm (3) or dissection
(4,5) of the carotid artery. The case
presented in the present study was perhaps the first case of
dissecting an aneurysm of the carotid artery caused by an elongated
hyoid bone.
Case presentation
An 80-year-old man with hypertension, who was taking
amlodipine and irbesartan, presented with right hemiparesis for
>5 h despite preventive therapy with antiplatelets and statins.
The neurologic examination disclosed only right-sided hemiparesis.
The patient was admitted to the Third People's Hospital of Chengdu
(Chengdu, China) in November 2018.
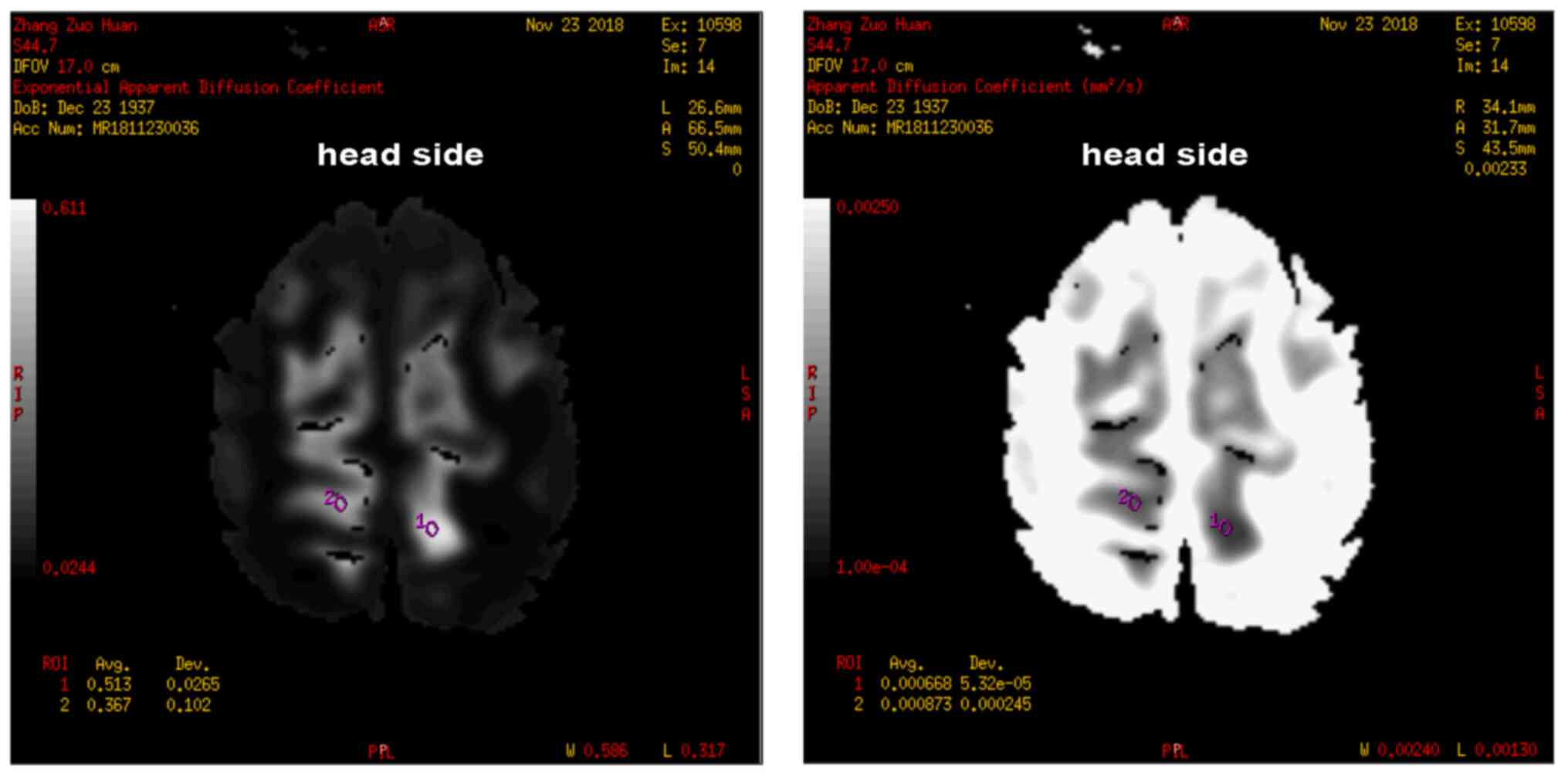
Diffusion-weighted magnetic resonance imaging
revealed acute infarction in the left parietal lobe and magnetic
resonance angiography detected stenosis of both posterior cerebral
arteries (Fig. 1). No responsive
stroke and associated symptoms were found.
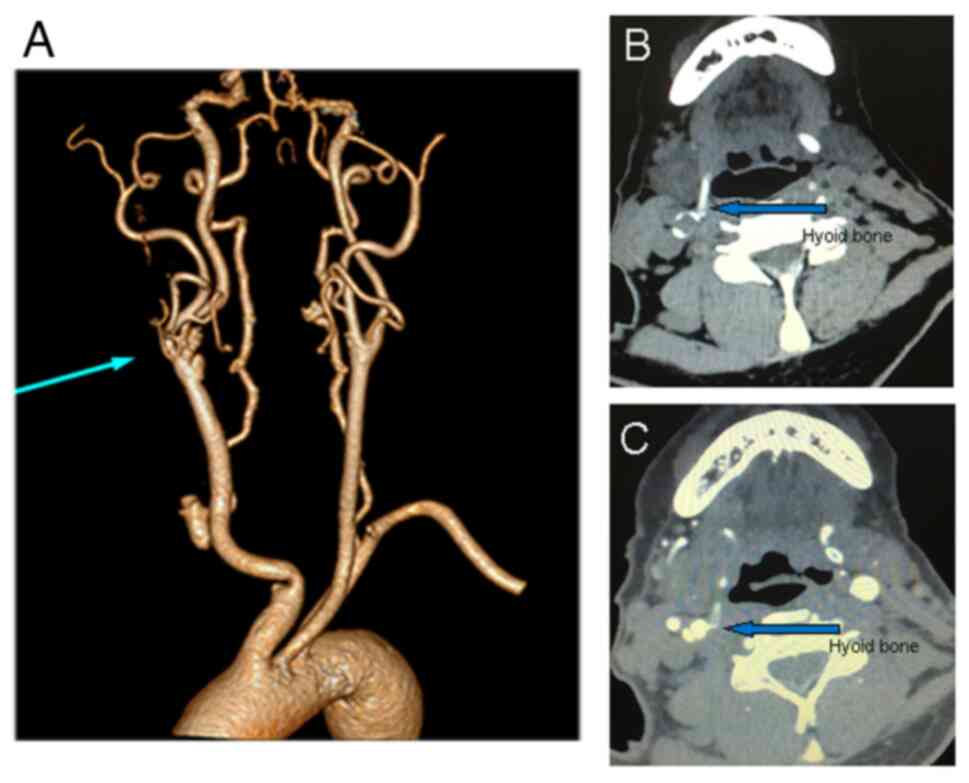
Contrast-enhanced computed tomography revealed two
cysts with some calcification located at the bifurcation of the
right internal carotid artery (ICA) and the right greater horn of
the hyoid bone adjacent to the right ICA (Fig. 2).
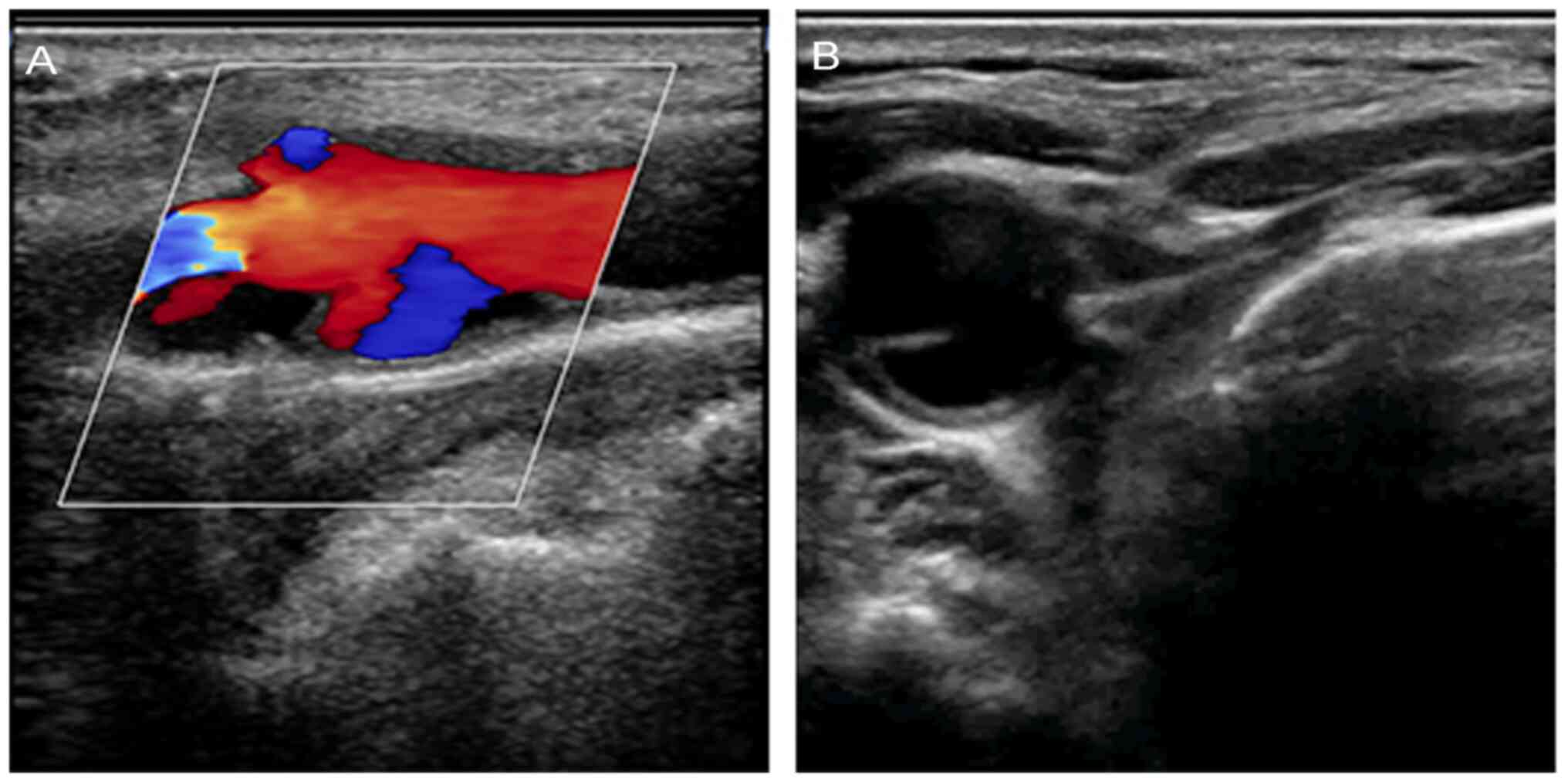
A color duplex scan of the carotid vessels showed
several inhomogeneous plaques in the carotid bifurcation, with
irregular thickening of the vessel walls. Two cysts, in which red
and blue flow signals were detected, communicated with the right
common carotid artery (CCA) and the origin of the right ICA
separately, suggesting dissecting an aneurysm. The right CCA and
the origin of the right ICA were compressed by the hyoid bone
repeatedly when swallowing and speaking (Fig. 3). An ultrasound video also showed
ICA being collapsed by the hyoid bone during swallowing or speech
(Video S1).
The dissecting aneurysm of the carotid artery was
associated with an elongated hyoid bone. The patient was treated
with aspirin (100 mg qd) and clopidogrel (clopidogrel 75 mg) and
symptoms gradually improved. The patient continued to take
clopidogrel and atorvastatin orally after discharge. Follow-ups
were conducted at least every six months post-discharge. The
patient did not experience any further cerebrovascular incidents.
Surgical resection of the hyoid bone was recommended for continuous
mechanical stimulation, but the patient refused.
It is possible that infarction may have been caused
by embolization from a thrombus from a dissecting aneurysm.
Time-of-flight magnetic resonance angiography image (Fig. S1) demonstrated that a right-sided
internal carotid artery lesion does have the potential to cause a
left-sided cerebral infarct lesion.
Discussion
Bony structures around the carotid artery, such as
the styloid process, thyroid cartilage (6) and hyoid bone, can cause dissection,
compression, plaque formation and plaque rupture of the carotid
artery. In 1948, Eagle reported compression and irritation of the
sympathetic plexus close to the ICA, resulting in dysphagia with
facial and neck pain by elongated styloid process (7). This was further reported in other
studies and alternatively called stylocarotid artery syndrome or
Eagle syndrome (8). Kumagai et
al (6) described a case of
symptomatic carotid stenosis caused by mechanical stimulation of
the thyroid cartilage. Similarly, compression and trauma from the
hyoid bone have also been described as rare causes of carotid
stenosis, pseudoaneurysm and dissection. A possible explanation for
carotid vasculopathy is the direct compression of the hyoid bone,
leading to increasing turbulent blood flow and higher shear force,
resulting in endothelial injury (9).
No clear history of head or cervical trauma has been
noted in a majority of patients with carotid dissection. The exact
cause of these so-called spontaneous dissections is unclear.
Recently, certain anatomic characteristics of the hyoid bone (i.e.,
the length and the proximity to the carotid artery) were reported
in only two studies as potential risk factors for carotid
dissection (4,5). However, the case described in this
study was perhaps the first case in which the elongation of the
hyoid bone was diagnosed to be the cause of the dissecting
aneurysm.
In the case described in the present study,
dissecting aneurysm was detected accidentally because of no
responsible ischemic strokes and no associated symptoms or signs
such as neck pain, Horner syndrome, cranial nerve palsy and murmur
of the carotid artery. No other causes of carotid dissection were
found in this case. Computed tomography angiography (CTA) of the
neck may characterize the anatomical association of the carotid
arteries and the hyoid bone. It was hypothesized that a carotid
dissecting aneurysm was related to direct mechanical compression of
the carotid artery by the hyoid bone induced by neck rotation or
swallowing. This diagnosis was confirmed by a dynamic study of
carotid duplex ultrasonography. Swallowing, talking and head
rotation were demonstrated to contribute to the hyoid-related
vessel injury.
No established treatment guidelines exist for hyoid
bone-related carotid artery injury. Anticoagulation and/or
antiplatelet treatment is usually initiated. At present, there is
no established consensus regarding the treatment of this disease.
As will be detailed subsequently, both anticoagulants and
antiplatelet agents are viable options. Following a thorough
discussion with the patient, we opted for antiplatelet therapy. If
the hyoid bone is left untouched, it likely continues to cause
mechanical stimulation. Although no responsible ischemic stroke was
observed in the case reported in the present study, surgical
resection of the hyoid bone was an appropriate treatment option.
Partial hyoid resection is a safe and effective treatment in most
case reports. Therefore, arterial reconstruction combined with
partial hyoid resection was suggested. However, the patient refused
to undergo this surgery and opted for oral antiplatelets.
In summary, despite only a few case reports of hyoid
bone-related dissecting aneurysms, attention should be paid to the
elongated hyoid bone as an underlying factor and treatable cause of
dissecting aneurysm of the carotid artery. CTA of the neck and
carotid duplex ultrasonography are useful treatment modalities.
Partial resection of the hyoid bone is a safe and effective
approach to prevent further ischemia.
Supplementary Material
Supplementary Video
Repeated collisions of the hyoid bone
with the internal carotid artery were seen during the patient’s
swallowing maneuvers.
Time-of-flight magnetic resonance
angiography image shows that a right-sided internal carotid artery
lesion does have the potential to cause a left-sided cerebral
infarct lesion.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed in this study are
included in this published article.
Authors' contributions
QY, YL, HT, QZ and HZ collected patient data. QY and
HL contributed to the study design and manuscript writing. QY and
HZ confirm the authenticity of all the raw data. All authors have
read and approved the final manuscript.
Ethics approval and consent to
participate
The ethics committee of The Affiliated Hospital of
Southwest Jiaotong University and The Third People's Hospital of
Chengdu (Chengdu, China) approved the present study (approval no.
20181123).
Patient consent for publication
The patient provided written consent for the
publication of the case report and images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Abdelaziz OS, Ogilvy CS and Lev M: Is
there a potential role for hyoid bone compression in pathogenesis
of carotid artery stenosis? Surg Neurol. 51:650–653.
1999.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Hong JM, Kim TJ and Lee JS and Lee JS:
Neurological picture. Repetitive internal carotid artery
compression of the hyoid: A new mechanism of golfer's stroke? J
Neurol Neurosurg Psychiatry. 82:233–234. 2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Schneider CG and Kortmann H:
Pseudoaneurysm of the common carotid artery due to ongoing trauma
from the hyoid bone. J Vasc Surg. 45:186–187. 2007.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yukawa S, Yamamoto S and Hara H: Carotid
artery dissection associated with an elongated hyoid bone. J Stroke
Cerebrovasc Dis. 23:e411–e412. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Renard D and Freitag C: Hyoid-related
internal carotid artery dissection. J Neurol. 259:2501–2502.
2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kumagai N, Enomoto Y, Miyai M, Egashira Y,
Nakayama N and Iwama T: A rare case of symptomatic carotid stenosis
caused by mechanical stimulation by thyroid cartilage and frequent
swimming. J Stroke Cerebrovasc Dis. 28:699–701. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Eagle WW: Elongated styloid process;
further observations and a new syndrome. Arch Otolaryngol (1925).
47:630–640. 1948.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Hoffmann E, Rader C, Fuhrmann H and Maurer
P: Styloid-carotid artery syndrome treated surgically with
Piezosurgery: A case report and literature review. J
Craniomaxillofac Surg. 41:162–166. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Renard D, Rougier M, Aichoun I and Labauge
P: Hyoid bone-related focal carotid vasculopathy. J Neurol.
258:1540–1541. 2011.PubMed/NCBI View Article : Google Scholar
|