Introduction
The most common arrhythmia is atrial fibrillation
(AF), which can increase certain morbidities, such as heart failure
and stroke, and also increase mortality rates, due to stroke and
other cardiovascular diseases (1,2). The
incidence and prevalence of AF in the elderly has increased
significantly from 2004-2016. The prevalence of atrial fibrillation
was 0.95%, and the incidence of AF ranges between 0.21 and 0.41 per
1,000 person/years in the elderly over 70 years or older (3,4). As
common triggers of AF have been observed to be originated from
pulmonary veins, and pulmonary vein (PV) isolation (PVI) with
catheter ablation has been established as an effective treatment
for AF and is recommended by current guidelines (1,3).
With the aging of the general population, more
elderly people need to receive catheter ablation for AF. The
elderly population are more likely to be diagnosed with coronary
artery disease, type 2 diabetes, hypertension, stroke, a higher
risk of thrombo-embolic events, renal insufficiency and other
chronic diseases, which can greatly increase the incidence of
intraoperative complications (4).
Additionally, catheter ablation for AF and long operation and
sedation time increases the incidence of intraoperative
complications in the elderly (5).
The relatively simple learning curve of cryoballoon ablation and
short intraoperative operation time associated with this treatment,
may be more suitable for the treatment of AF in the elderly.
Studies have confirmed that cryoballoon ablation had
comparable efficacy compared with catheter ablation (4,5). The
success rate of catheter ablation in elderly patients with AF has
been revealed to be promising in several studies (6,7).
Although there have been some studies on cryoballoon
ablation in elderly patients with AF, most studies lacked
controlled studies with young people and the number of included
cases was small (8,9), to the best of the authors' knowledge,
there has been no systematic review or meta-analysis on this
subject. Therefore, it was decided to perform a systematic review
and meta-analysis on this important subject.
Materials and methods
Protocol
The Preferred Reporting Items for Systematic Reviews
and Meta-Analyses guidelines were used in conducting the review
(10).
Data sources and literature
search
A total of four databases (PubMed https://pubmed.ncbi.nlm.nih.gov/, Embase
https://www.embase.com/, Cochrane Library
https://www.cochranelibrary.com/ and Web
of Science https://www.webofscience.com/) were searched until
February 2023. A comprehensive search was performed to identify
published articles or studies on the efficacy and safety of
cryoballoon ablation in elderly patients with AF (such as procedure
time, fluoroscopy time, success rate and complications). Medical
Subject Heading terms were used in PubMed, EMTREE terms in Embase,
and keyword search terms for cryoballoon ablation, elderly and
atrial fibrillation were used in all four databases with the use of
following search terms as single or complex terms in titles,
abstracts and keywords: (aged OR elderly OR aged 80 and over OR
oldest old OR centenarian OR supercentenarian OR
semi-supercentenarians OR octogenarian OR nonagenarian) AND
(cryoablation OR cryoballoon OR cryosurgery) AND (atrial
fibrillation OR auricular fibrillation OR persistent Atrial
Fibrillation OR familial Atrial Fibrillation OR paroxysmal Atrial
Fibrillation). No language limitations were applied.
Study selection and inclusion
criteria
All articles were screened independently by two
reviewers according to the following inclusion criteria: i)
Full-text and relevant data could be acquired; ii) controlled
clinical trials involving cryoballoon ablation; iii) comparing
efficacy and safety of cryoballoon ablation in the elderly and the
young population; iv) minimum follow-up time of 12 months.
Articles such as reviews, abstracts or summaries
presented in meetings were excluded. Disagreements between
reviewers were resolved by discussion.
Quality assessment and data
extraction
Data of study characteristics such as sample size,
follow-up period, age and sex were independently extracted by the
two reviewers according to the predefined protocol. The quality of
the included studies was assessed using the Newcastle-Ottawa Scale
(NOS) for observational studies (7). Studies were scored according to
selection of study groups (four points), comparability of groups
(two points), and ascertainment of exposure and outcomes (three
points) for case-control and cohort studies.
Statistical analysis
Stata (version 14.0; StataCorp LLC) was used to
perform the primary statistical analyses. Data are presented as the
mean difference and were pooled using the inverse variance for
continuous outcome measures. For dichotomous outcomes, data are
presented as the odds ratio (OR) and were pooled using the
Mantel-Haenszel random effects model. The 95% CI was used to
express procedural and long-term outcomes of the two groups,
respectively. Heterogeneity was quantified using I2.
Random effect models were applied to assess the
studies regardless of the heterogeneity (I2). P<0.05
was considered to indicate a statistically significant
difference.
Results
Search results
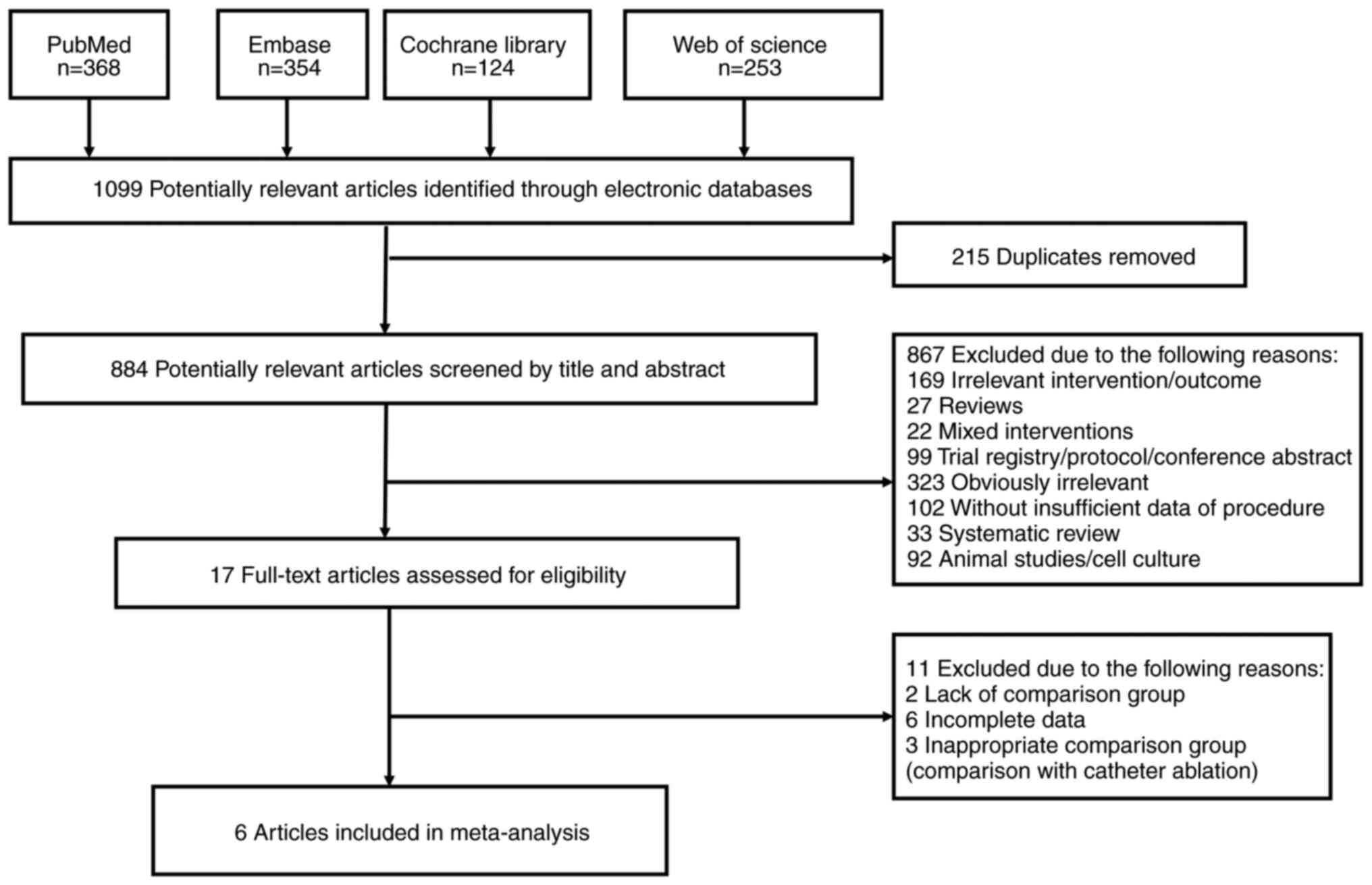
Based on the search strategy, 1,099 studies were
identified in the Cochrane library, Embase, PubMed and Web of
Science databases. Finally, six studies (8-13)
that met the inclusion criteria were identified (Fig. 1).
Characteristics of the included
studies and quality assessment
The characteristics of the included studies are
shown in Table I. Studies were
performed in Germany (n=3), Italy (n=1), China (n=1), Belgium (n=1)
and Japan (n=1). Most trials were single-center studies (n=4) and
all the included trials (n=6) were of high quality (NOS score of
8-9). Of the six studies, five (12-16)
included elderly patients ≥75 years old, but one (17) included elderly patients ≥80 years
old. The follow-up time was 12 months for five studies and 11.8±5.4
months for one study. Two studies included patients with paroxysmal
AF only (Table I).
 | Table ICharacteristics of trials included in
the meta-analysis. |
Table I
Characteristics of trials included in
the meta-analysis.
| | Sample size | |
|---|
| First author/s,
year | Country | Type | Age of elderly
group, years | Elderly group,
n | Control group,
n | Follow-up,
months | PAF, n (%) | NOS score | (Refs.) |
|---|
| Abdin et al,
2019 | Germany | Single-center,
controlled | ≥75 | 55 | 183 | 11.8±5.4 | 91 (38.2) | 8 | (16) |
| Abugattas et
al, 2017 | Belgium and
Italy | Two-center,
controlled | ≥75 | 53 | 106 | 12 | 159(100) | 8 | (15) |
| Heeger et
al, 2019 | Germany | Multi-center,
controlled | ≥75 | 104 | 104 | 12 | 119 (57.2) | 9 | (14) |
| Kanda et al,
2019 | Japan | Single-center,
controlled | ≥80 | 49 | 241 | 12 | 290(100) | 8 | (17) |
| Tscholl et
al, 2018 | Germany | Single-center,
controlled | ≥75 | 40 | 40 | 12 | 37 (46.25) | 9 | (12) |
| Zhang et al,
2019 | China | Single-center,
controlled | ≥75 | 127 | 550 | 12 | 603 (89.1) | 8 | (14) |
A total of 1,652 patients (936 male patients;
56.66%) were enrolled in the studies (428 patients in the elderly
group and 1,224 patients in the control group), with a mean age of
66.61 years. The mean left ventricular ejection fraction was 60.4%
(Table II). The left atrial size
was not significantly different between the two groups (42 mm in
the elderly group compared with 41 mm in the young group;
P=0.58).
| Table IIBaseline characteristics of the
included studies. |
Table II
Baseline characteristics of the
included studies.
| | Age, years | P-value | Male patients,
n | P-value | LVEF, % | P-value | CHA2DS2-vasc | P-value | HASBLED | P-value | LA diameter,
mm | P-value | |
|---|
| First author/s,
year | Elderly | Control | <0.01 | Elderly | Control | <0.01 | Elderly | Control | 0<0.01 | Elderly | Control | 0<0.01 | Elderly | Control | <0.01 | Elderly | Control | 0.58 | (Refs.) |
|---|
| Abdin et al,
2019 | 78± 2.8 | 60.8± 9.5 | <0.01 | 25 | 120 | <0.01 | 51.6± 8.3 | 52.5± 8.0 | 0.47 | 4.0± 1.3 | 2.0± 1.3 | <0.01 | 2.2± 0.89 | 1.2± 0.97 | <0.01 | 40.9± 5.5 | 40.8± 6.6 | 0.92 | (16) |
| Abugattas et
al, 2017 | 78.19± 2.7 | 58.97± 8.5 | <0.01 | 24 | 62 | 0.12 | 59.2± 5.2 | 59.9± 6.4 | 0.49 | NA | NA | NA | NA | NA | NA | 41.4± 7.2 | 40.9± 6.6 | 0.66 | (15) |
| Heeger et
al, 2019 | 77.5± 3.7 | 63± 13.3 | <0.01 | 52 | 54 | 0.78 | NA | NA | NA | 3.8± 1.1 | 2.1± 1.3 | <0.01 | NA | NA | NA | 44.5± 5.6 | 44.5± 5.6 | >0.99 | (14) |
| Kanda et al,
2019 | 84±3 | 66±10 | <0.01 | 24 | 145 | 0.15 | 66±10 | 65±10 | 0.52 | 3.8±0.9 | 2.2±1.4 | <0.01 | NA | NA | NA | 40±6 | 38±6 | 0.03 | (17) |
| Tscholl et
al, 2018 | 77.0± 2.2 | 65.5± 9.4 | <0.01 | 20 | 26 | 0.17 | 63±4.4 | 65±7.4 | 0.15 | 4±0.74 | 2±1.48 | <0.01 | 2±0.74 | 2±1.48 | >0.99 | NA | NA | | (12) |
| Zhang et al,
2019 | 79.2± 3.1 | 63.8± 7.6 | <0.01 | 57 | 327 | <0.01 | 58.7± 9.0 | 61.5± 6.5 | 0 | 4.8±1.6 | 2.6± 1.7 | <0.01 | 2.0±0.8 | 1.8±0.8 | 0.01 | 41.0± 5.3 | 41.3± 5.6 | 0.58 | (13) |
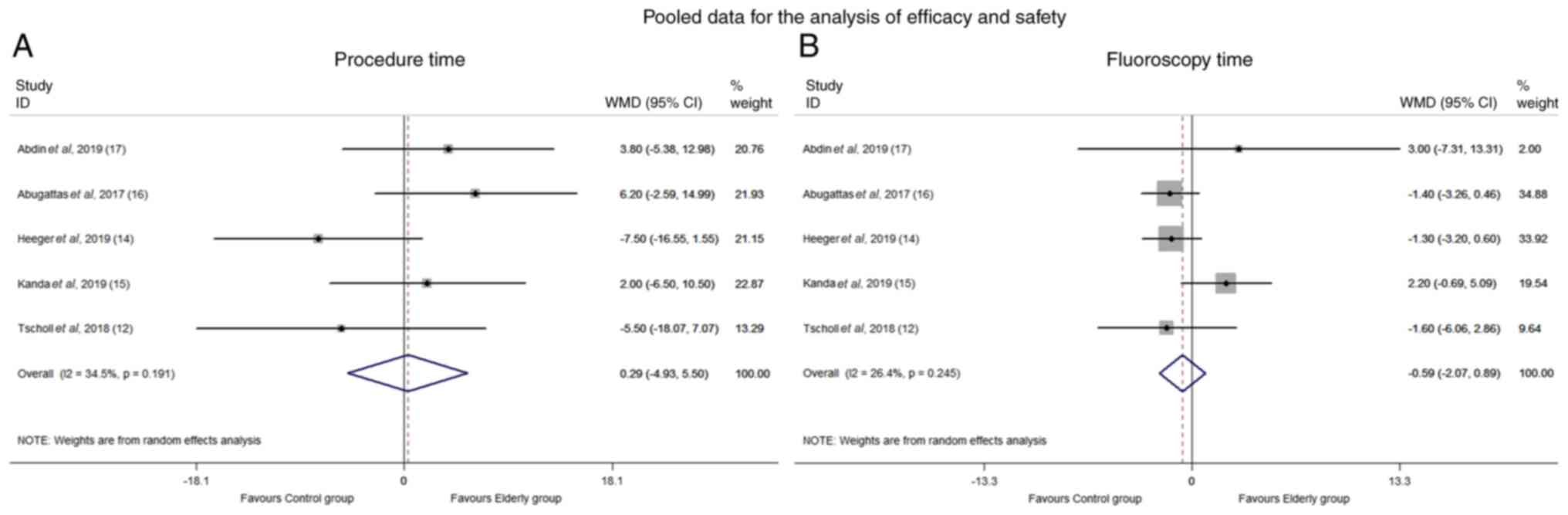
Procedural time
The procedural time was reported in five studies.
The heterogeneity was moderate (I2=34.5%). The
difference in procedural time between the two groups was not
significant (mean difference, 0.29; 95% CI, -4.93 to 5.50; P=0.91;
Fig. 2A).
Fluoroscopy time
The fluoroscopy time was systematically reported in
five studies. There was moderate heterogeneity among these trials
(I2=26.4%). The fluoroscopy time in the elderly group
was not significantly different compared with the younger group
(mean difference, -0.59; 95% CI, -2.07 to 0.89; P=0.43; Fig. 2B).
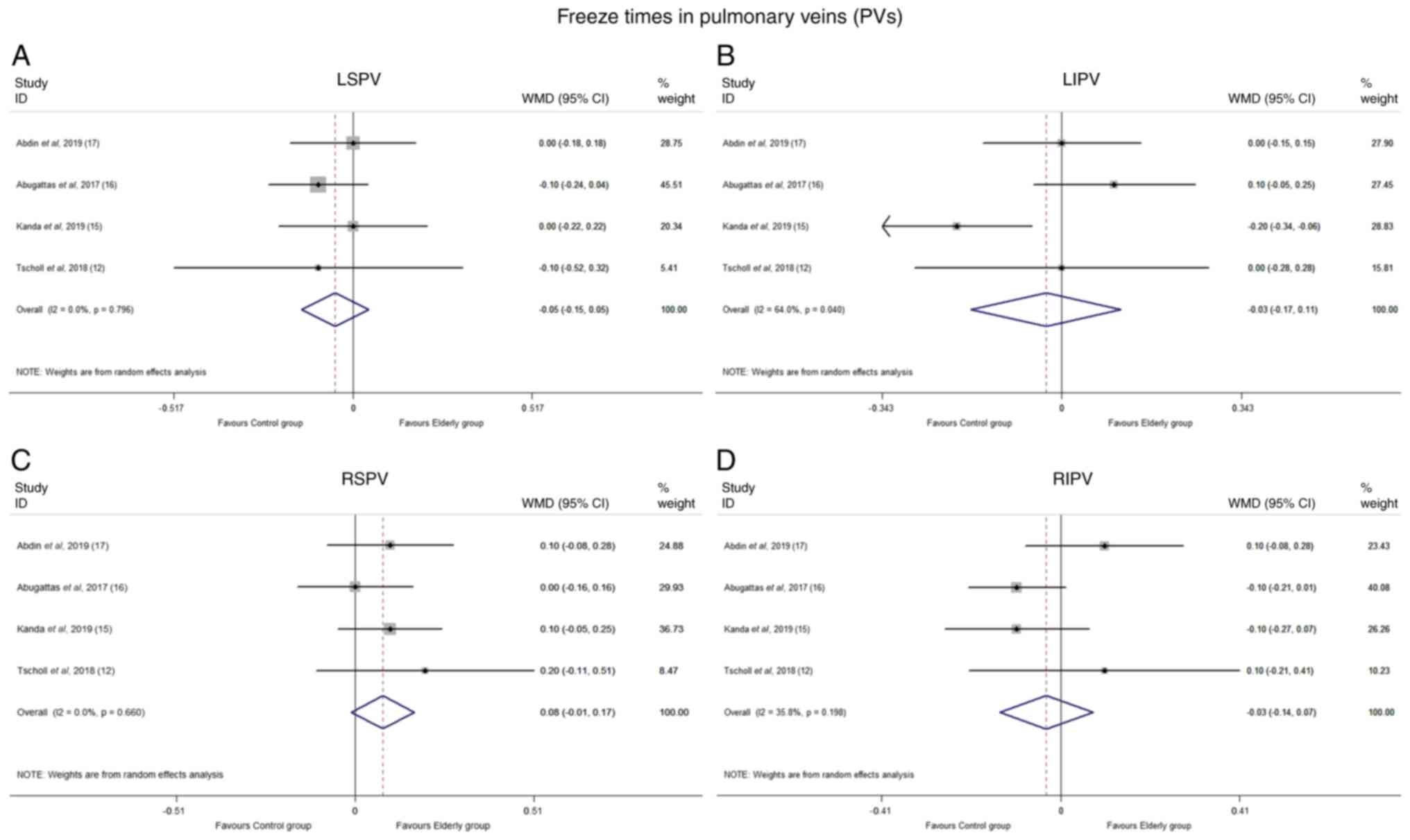
Freeze times in PVs
Data for freeze times in four PVs were available for
four studies (12,15-17).
The I2 index for left superior PVs (LSPVs), left
inferior PVs (LIPVs), right superior PVs (RSPVs) and right inferior
PVs (RIPVs) was 0.0, 64.0, 0.0 and 35.8%, respectively. There was
no significant difference between the elderly and control group in
terms of freeze times of LSPVs (mean difference, -0.051; 95% CI,
-0.148 to 0.046; P=0.303), LIPVs (mean difference, -0.03; 95% CI,
-0.17 to 0.11; P=0.36), RSPVs (mean difference, 0.079; 95% CI,
-0.012 to 0.169; P=0.088) and RIPVs (mean difference, -0.033; 95%
CI, -0.14 to 0.07; P=0.55; Fig.
3). When a sensitivity test was performed, the removal of any
individual study did not affect the point estimate or confidence
interval of the results (data not shown).
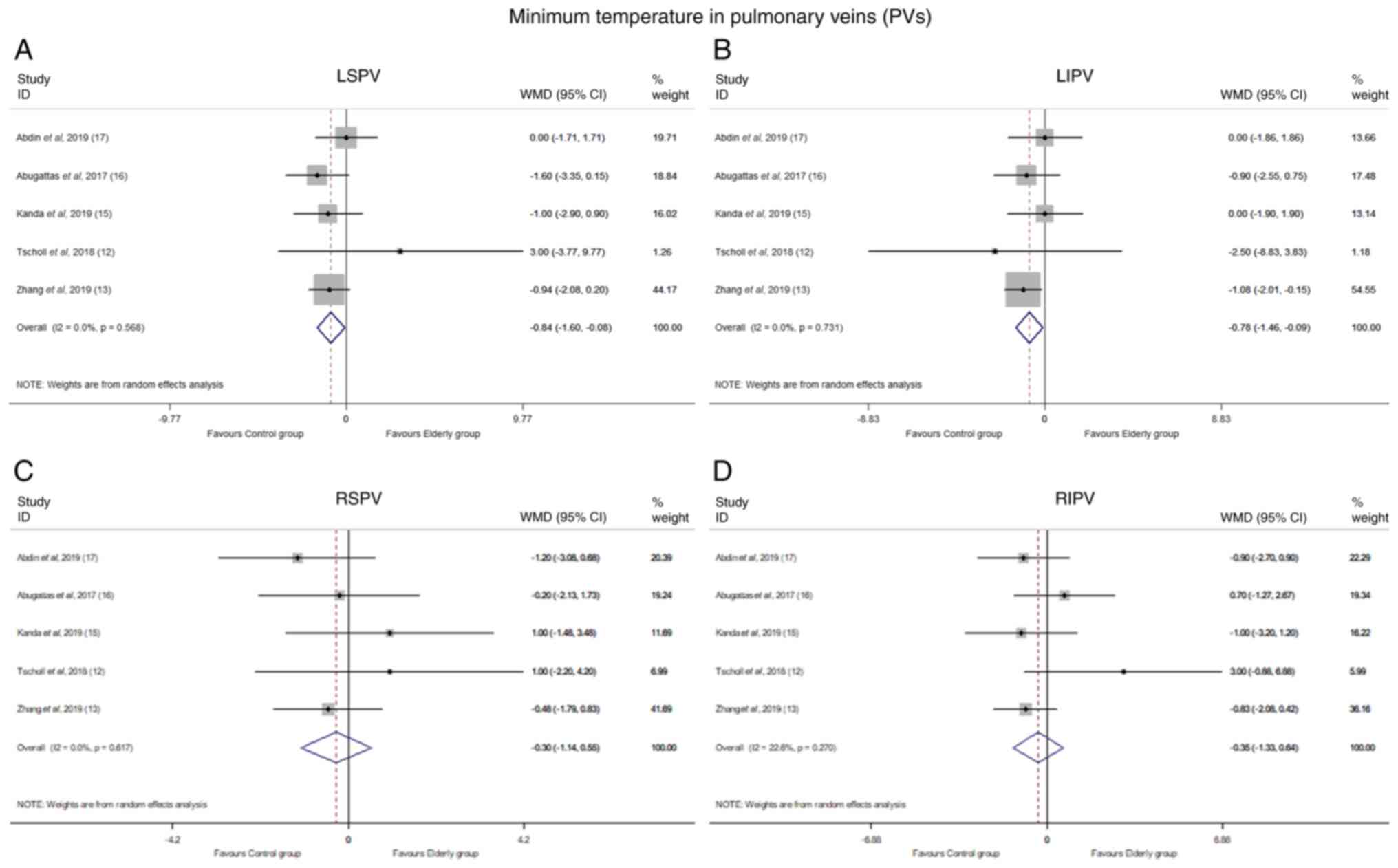
Minimum temperature in PVs
A total of five trials reported the minimum
temperature in PVs during the procedure. Cryoballoon freezing was
associated with a significantly lower temperature in the elderly
compared with the control group during the ablation of LSPVs (mean
difference, -0.84; 95% CI, -1.60 to -0.08; P=0.03) and LIPVs (mean
difference, -0.78; 95% CI, -1.46 to -0.09; P=0.03). In addition,
there was no heterogeneity (I2=0.0%).
There was no significant difference between the two
groups during the cryoablation process of the RSPVs (mean
difference, -0.30; 95% CI, -1.14 to 0.55; P=0.49) and RIPVs (mean
difference, -0.35; 95% CI, -1.33 to 0.64; P=0.49). In addition,
there was no heterogeneity for RSPVs (I2=0.0%) and low
heterogeneity for RIPVs (I2=22.6%) (Fig. 4).
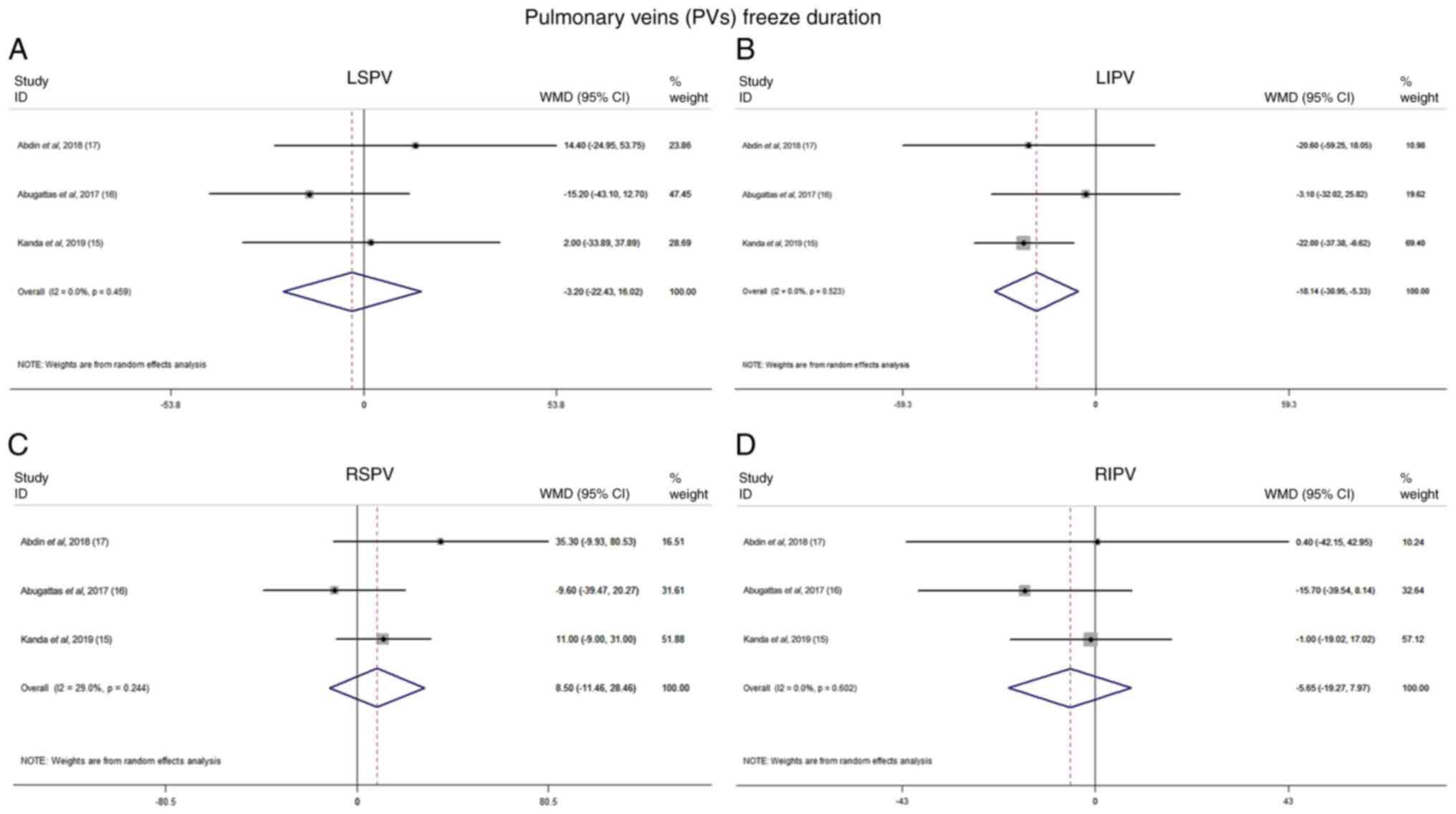
PV freeze duration
Data on PV freeze duration were available for three
studies. There were no significant differences in freeze durations
of LSPVs, RSPVs and RIPVs between the two groups. However, LIPV of
the elderly group was characterized by longer freeze duration (mean
difference, -18.14; 95% CI, -30.95 to -5.33; P=0.006). There was no
heterogeneity between the two groups (I2=0.0%; Fig. 5).
Success rate
All the included studies systematically reported the
success rate. The heterogeneity in both groups was low
(I2=2.1%). There was no difference in the success rate
between the elderly and younger individuals (OR, 0.981; 95% CI,
0.72 to 1.34; P=0.903; Fig.
S1).
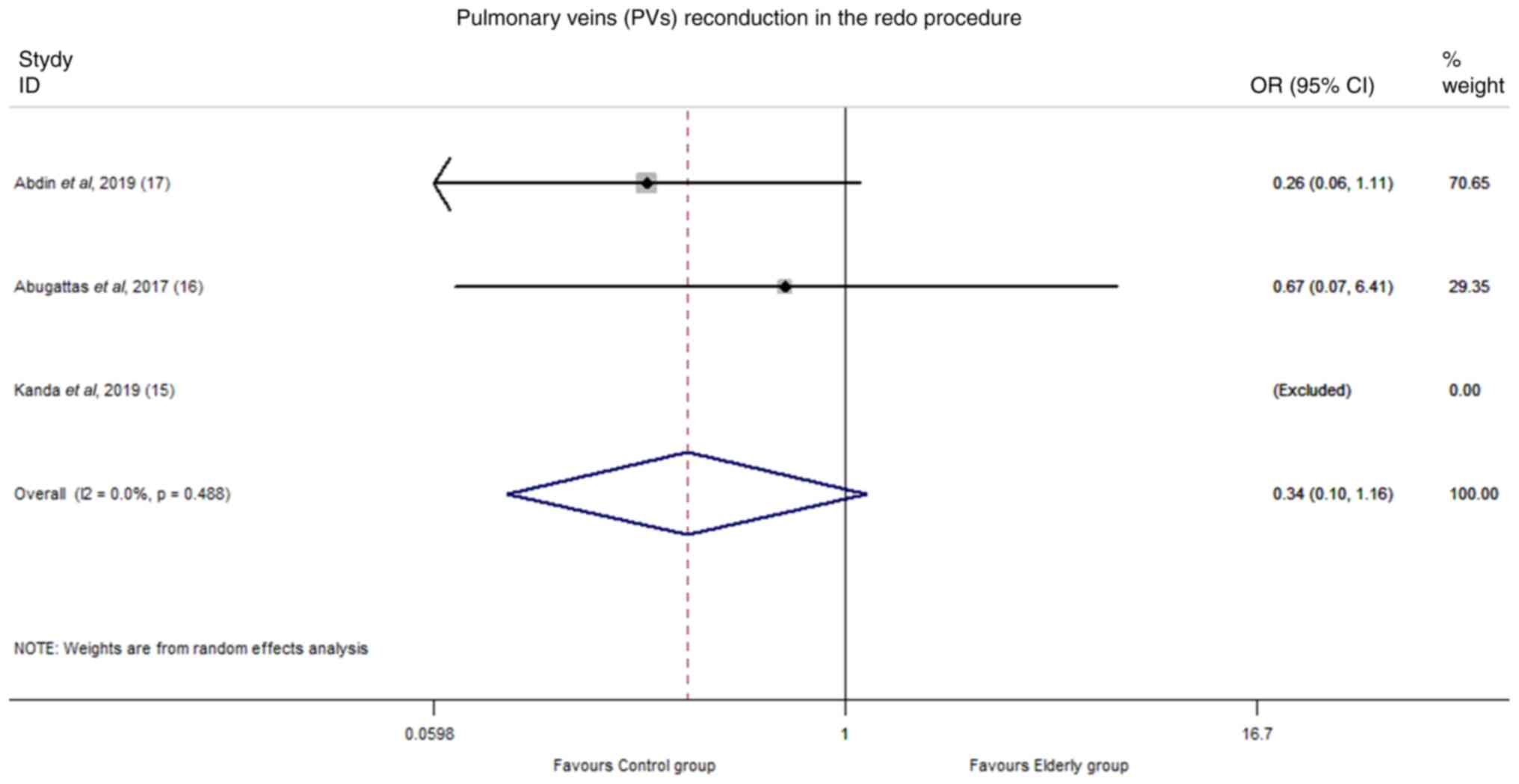
In addition, three trials reported the PV
reconduction in the redo procedure. There was no significant
heterogeneity (I2=0.0%). The difference in PV
reconduction between the elderly and control group was not
significant (OR, 0.34; 95% CI, 0.10 to 1.16; P=0.08; Fig. 6).
Transient phrenic nerve palsy
(tPNP)
The results of tPNP were reported in all included
studies. However, one study (17)
reported tPNP in all patients, and was not included in the
analysis. The heterogeneity was low (I2=0.0%). There was
no difference in the rate of tPNP between the two groups (mean
difference, 0.96; 95% CI, 0.45 to 2.02; P=0.90; Fig. S2). Other complications of the
procedure are shown in Table
III. There was no significant difference between the two
groups.
| Table IIIComplications in the included
studies. |
Table III
Complications in the included
studies.
| | Persistent PNP,
n | Atrio-esophageal
fistula, n | Groin
complications, n | Tamponade, n | Mortality, n | MI, n | Stroke/TIA, n | Pericardial
effusion, n | |
|---|
| First author/s,
year | Elderly | Control | Elderly | Control | Elderly | Control | Elderly | Control | Elderly | Control | Elderly | Control | Elderly | Control | Elderly | Control | (Refs.) |
|---|
| Abdin et al,
2019 | 0 | 0 | 0 | 0 | 2 | 4 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | (16) |
| Abugattas et
al, 2017 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | NA | NA | (15) |
| Heeger et
al, 2019 | 0 | 0 | 0 | 0 | 4 | 4 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | (14) |
| Kanda et al,
2019 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | (17) |
| Tscholl et
al, 2018 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | (12) |
| Zhang et al,
2019 | 0 | 0 | 0 | 0 | NA | NA | 0 | 1 | 0 | 2 | 0 | 2 | 1 | 5 | 1 | 3 | (13) |
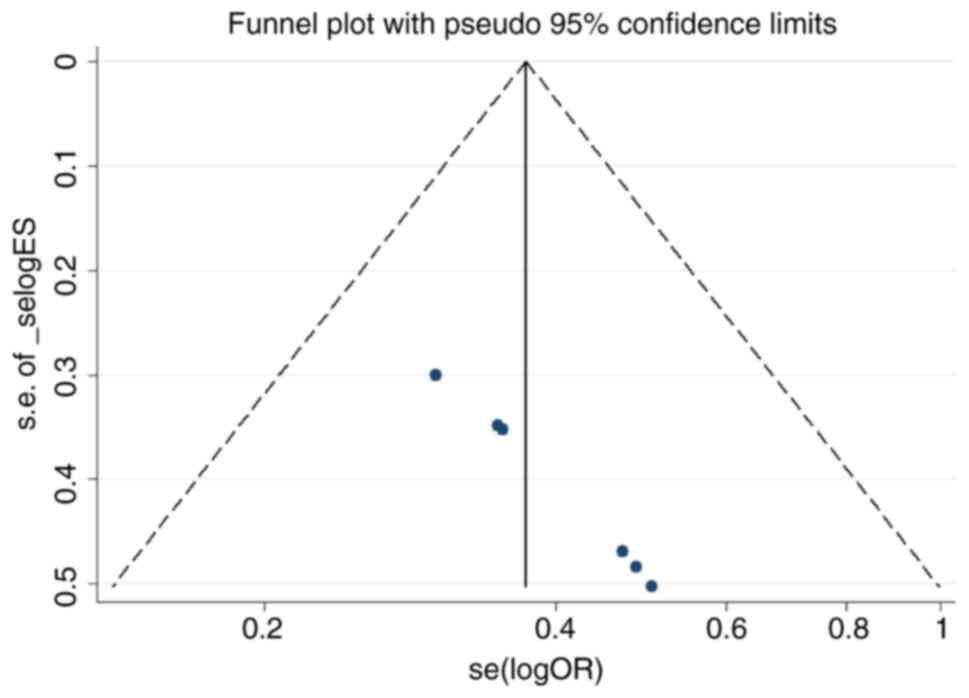
Risk of bias and sensitivity
analysis
All trials included were nonrandomized controlled
studies. A funnel plot of studies including procedural time was
highly symmetrical, six dots were contained in the large triangle
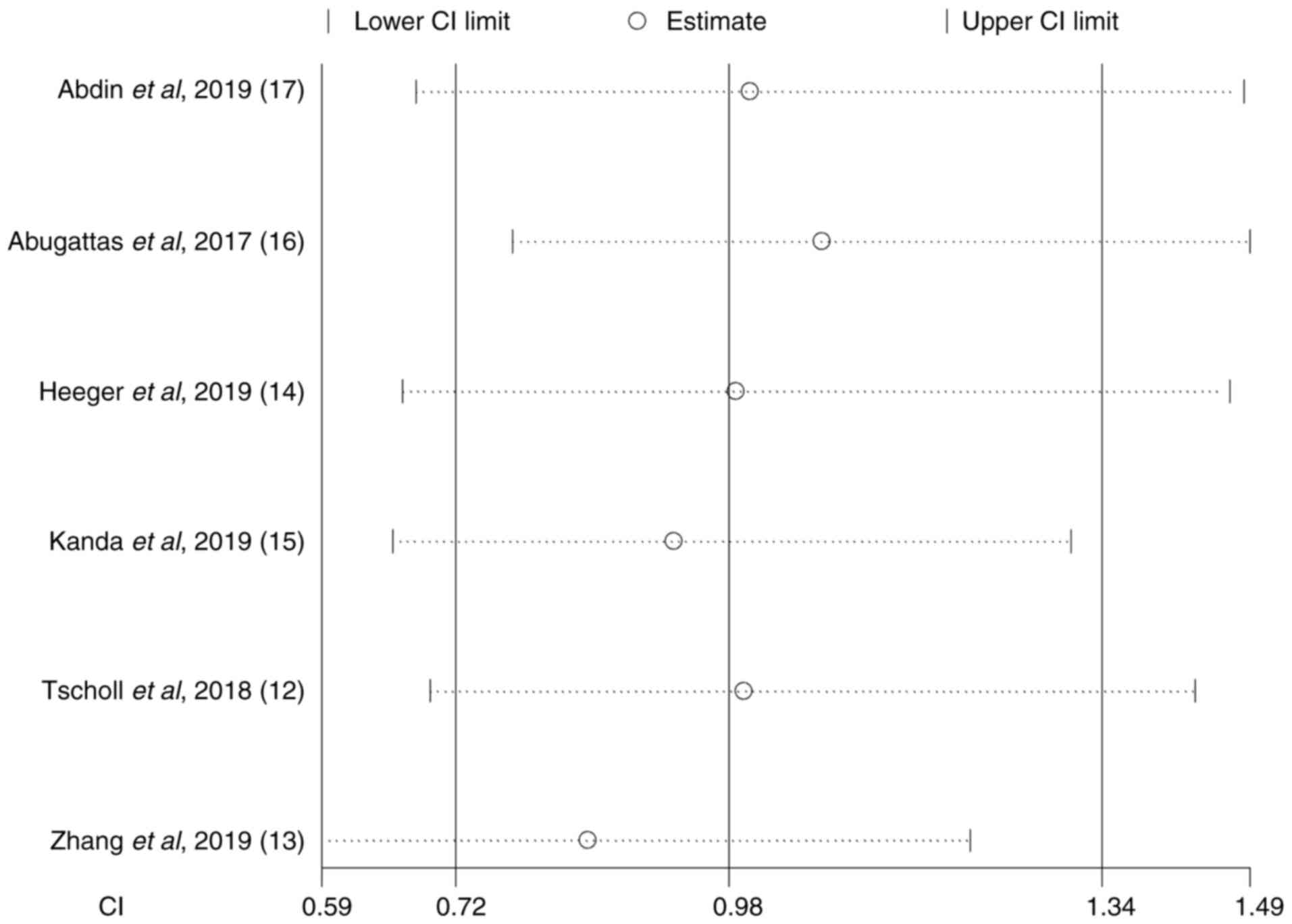
and no evidence of publication bias was identified (Fig. 7). A sensitive analysis showed that
the direction and magnitude of combined estimates of fluoroscopy
time did not vary markedly with the removal of any study,
indicating that the meta-analysis had good reliability and the
results were not overly influenced by each individual study
(Fig. 8). However, it should be
noted that the elderly patients were >80 years old in the study
by Kanda et al (17), while
the patients were >75 years old in the other five studies, which
might be a source of bias.
Discussion
To the best of our knowledge, the present study was
the first meta-analysis to systematically evaluate the efficacy and
safety of the cryoballoon ablation procedure in elderly patients
with AF. The main finding of the present study was that the
cryoballoon ablation procedure was as effective and safe in the
elderly as in the younger patients with AF. Cryoballoon freezing
was associated with a significantly lower temperature in the
elderly compared with the control group during the ablation of
LSPVs.
Since the study by Haïssaguerre et al
(18) reported that triggers from
the PVs initiated AF, PVI has been recommended as the cornerstone
of ablation approaches for the treatment of AF (19). The efficacy and safety have been
uniformly demonstrated in multiple trials (20,21).
At present, it has been shown that cryoablation can have a similar
effect to radiofrequency ablation (4,5). A
number of studies have established that the prognosis of AF is
worse in patients aged ≥75 years, and the rates of mortality and
major adverse cardiac events are higher (22-25).
As the remodeling and fibrosis of the atrium increase with aging,
the success rate of PVI is supposed to be lower in the elderly
population (15). Therefore, a
number of clinical trials, such as the STOP-AF and RAAFT-2 trials,
did not include elderly patients (26,27).
However, some non-randomized clinical trials have reported that the
results of catheter ablation in elderly patients with AF are
promising (28,29). Furthermore, the risk of surgery is
higher due to the poor physical conditions and more complications
in the elderly. Compared with radiofrequency ablation, cryoablation
has a shorter left atrial operation time, which seems to be more
suitable for elderly patients (4,5).
The present meta-analysis focused on a comparison of
cryoablation between older and young adults. The results were
consistent with the observations from the aforementioned studies
(12-17).
In the present study, the procedural data and success rate for the
efficacy analysis were pooled. No significant difference was
observed between the procedural time (mean difference, 0.29; 95%
CI, -4.93 to 5.50; P=0.91; Fig.
2A) and fluoroscopy time (mean difference, -0.59; 95% CI, -2.07
to 0.89; P=0.43; Fig. 2B). No
significant difference was observed for the success rate (OR,
0.981; 95% CI, 0.72 to 1.34; P=0.903; Fig. S1).
Generally, it has been assumed that the elderly
cannot endure long operations as can the young, which may affect
the efficacy of the procedure (8,9).
However, there was no difference between the two groups in the
efficacy of the procedure. The cryoballoon ablation procedure takes
a short time, which might be a possible explanation. Freeze times
of PVs could be performed safely in the elderly as with the young.
However, it should be noted that freezing energy could produce a
lower temperature on LSPV and LIPV in the elderly compared with the
control group in the present study. Nevertheless, in the present
study, there was no significant difference between the left
pulmonary veins and right pulmonary veins, although the mechanism
is unclear. In addition, the LIPV freezing time was longer in the
elderly. Therefore, it also suggested that doctors should be more
careful in the process of LPV freezing in the elderly. The
complication rates of the catheter ablation procedure in elderly
patients with AF reported in some trials are inconsistent (30,31).
A number of studies have indicated that the rate of complication of
catheter ablation was higher in elderly patients with AF compared
with the young population (32,33).
Compared with catheter ablation, some studies have reported that
there were fewer serious complications for the cryoballoon ablation
procedure (34,35).
In addition to complications such as pericardial
effusions or tamponades, PV stenosis may occur in rare instances
(36). Phrenic nerve palsy is the
most common complication for the cryoballoon procedure, and can be
prevented by phrenic nerve pacing in the procedure (35). tPNP results were reported by all
the included trials and it was identified that there was no
significant difference in the rate of tPNP between the two groups
(mean difference, 0.96; 95% CI, 0.45 to 2.02; P=0.90) and the
heterogeneity was low. There was no significant difference for
other complications such as atrio-esophageal fistula, tamponade and
mortality (Table III).
Therefore, the incidence of complications of the
cryoballoon procedure in the elderly was similar to that in the
young. The data of some recurrent cases were also analyzed in the
present study. It was found that there was no significant
difference in PV reconduction between the two groups, which further
verified that the effect of cryoablation in the elderly was not
inferior to that in the young.
The trials included in the present meta-analysis
were non-randomized trials, which might cause bias and yield
limited meaningful results. Additionally, more high-quality
randomized controlled trials are required to analyze the efficacy
and safety of cryoballoon ablation in the elderly. Patients aged
>80 years old were included in the Tscholl et al
(12) trial, while patients were
>75 years old in other trials. This could be a source of
heterogeneity. The heterogeneity was low or moderate in the present
study.
In conclusion, cryoballoon ablation was as safe and
effective in elderly patients with AF as in young patients. The
cryoballoon operation of the left pulmonary veins in the elderly
requires more attention.
Supplementary Material
Success rate.
Transient phrenic nerve palsy.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by a grant from the
Natural Science Foundation of Shandong Province (grant no.
ZR2022MH253).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
XL and QZ conceived and designed the study. LY, JG
and HBT performed the statistical analysis of the data. XL and JG
drafted and wrote the paper. All authors reviewed and edited the
manuscript. Data authentication is not applicable. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kirchhof P, Benussi S, Kotecha D, Ahlsson
A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks
J, et al: 2016 ESC Guidelines for the management of atrial
fibrillation developed in collaboration with EACTS. Europace.
18:1609–1678. 2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Feinberg WM, Blackshear JL, Laupacis A,
Kronmal R and Hart RG: Prevalence, age distribution, and gender of
patients with atrial fibrillation. Analysis and implications. Arch
Intern Med. 155:469–473. 1995.PubMed/NCBI
|
|
3
|
Go AS, Hylek EM, Phillips KA, Chang Y,
Henault LE, Selby JV and Singer DE: Prevalence of diagnosed atrial
fibrillation in adults: national implications for rhythm management
and stroke prevention: the AnTicoagulation and risk factors in
atrial fibrillation (ATRIA) study. JAMA. 285:2370–2375.
2001.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Zoni-Berisso M, Lercari F, Carazza T and
Domenicucci S: Epidemiology of atrial fibrillation: European
perspective. Clin Epidemiol. 6:213–220. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kuck KH, Brugada J, Fürnkranz A, Metzner
A, Ouyang F, Chun KR, Elvan A, Arentz T, Bestehorn K, Pocock SJ, et
al: Cryoballoon or radiofrequency ablation for paroxysmal atrial
fibrillation. N Engl J Med. 374:2235–2245. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Lioni L, Letsas KP, Efremidis M, Vlachos
K, Giannopoulos G, Kareliotis V, Deftereos S and Sideris A:
Catheter ablation of atrial fibrillation in the elderly. J Geriatr
Cardiol. 11:291–295. 2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kawamura I, Aikawa T, Yokoyama Y, Takagi H
and Kuno T: Catheter ablation for atrial fibrillation in elderly
patients: Systematic review and a meta-analysis. Pacing Clin
Electrophysiol. 45:59–71. 2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ikenouchi T, Nitta J, Nitta G, Kato S,
Iwasaki T, Murata K, Junji M, Hirao T, Kanoh M, Takamiya T, et al:
Propensity-matched comparison of cryoballoon and radiofrequency
ablation for atrial fibrillation in elderly patients. Heart Rhythm.
16:838–845. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Xing Y, Xu B, Sheng X, Xu C, Peng F, Sun
Y, Wang S and Guo H: Efficacy and safety of uninterrupted
low-intensity warfarin for cryoballoon ablation of atrial
fibrillation in the elderly: A pilot study. J Clin Pharm Ther.
43:401–407. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Moher D, Liberati A, Tetzlaff J and Altman
DG: PRISMA Group. Preferred reporting items for systematic reviews
and meta-analyses: The PRISMA statement. J Clin Epidemiol.
62:1006–1012. 2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lo CK, Mertz D and Loeb M:
Newcastle-Ottawa Scale: Comparing reviewers' to authors'
assessments. BMC Med Res Methodol. 14(45)2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Tscholl V, Lin T, Lsharaf AK, Bellmann B,
Nagel P, Lenz K, Landmesser U, Roser M and Rillig A: Cryoballoon
ablation in the elderly: One year outcome and safety of the
second-generation 28 mm cryoballoon in patients over 75 years old.
Europace. 20:772–777. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Zhang J, Ren Z, Wang S, Zhang J, Yang H,
Zheng Y, Meng W, Zhao D and Xu Y: Efficacy and safety of
cryoballoon ablation for Chinese patients over 75 years old: A
comparison with a younger cohort. Journal Of Cardiovascular
Electrophysiology. 30:2734–2742. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Heeger CH, Bellmann B, Fink T, Bohnen JE,
Wissner E, Wohlmuth P, Rottner L, Sohns C, Tilz RR, Mathew S, et
al: Efficacy and safety of cryoballoon ablation in the elderly: A
multicenter study. Int J Cardiol. 278:108–113. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Abugattas JP, Iacopino S, Moran D, De
Regibus V, Takarada K, Mugnai G, Ströker E, Coutiño-Moreno HE,
Choudhury R, Storti C, et al: Efficacy and safety of the second
generation cryoballoon ablation for the treatment of paroxysmal
atrial fibrillation in patients over 75 years: A comparison with a
younger cohort. Europace. 19:1798–1803. 2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Abdin A, Yalin K, Lyan E, Sawan N, Liosis
S, Meyer-Saraei R, Elsner C, Lange SA, Heeger CH, Eitel C, et al:
Safety and efficacy of cryoballoon ablation for the treatment of
atrial fibrillation in elderly patients. Clin Res Cardiol.
108:167–174. 2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kanda T, Masuda M, Kurata N, Asai M, Iida
O, Okamoto S, Ishihara T, Nanto K, Tsujimura T, Okuno S, et al:
Efficacy and safety of the cryoballoon-based atrial fibrillation
ablation in patients aged ≥80 years. J Cardiovasc Electrophysiol.
30:2242–2247. 2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Haïssaguerre M, Jaïs P, Shah DC, Takahashi
A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Métayer P and
Clémenty J: Spontaneous initiation of atrial fibrillation by
ectopic beats originating in the pulmonary veins. N Engl J Med.
339:659–666. 1998.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Calkins H, Kuck KH, Cappato R, Brugada J,
Camm AJ, Chen SA, Crijns HJ, Damiano RJ Jr, Davies DW, DiMarco J,
et al: 2012 HRS/EHRA/ECAS expert consensus statement on catheter
and surgical ablation of atrial fibrillation: Recommendations for
patient selection, procedural techniques, patient management and
follow-up, definitions, endpoints, and research trial design: A
report of the heart rhythm society (HRS) task force on catheter and
surgical ablation of atrial fibrillation. Developed in partnership
with the European heart rhythm association (EHRA), a registered
branch of the European society of cardiology (ESC) and the European
cardiac arrhythmia society (ECAS); and in collaboration with the
American college of cardiology (ACC), American heart association
(AHA), the Asia pacific heart rhythm society (APHRS), and the
society of thoracic surgeons (STS). Endorsed by the governing
bodies of the American college of cardiology foundation, the
American heart association, the European cardiac arrhythmia
society, the European heart rhythm association, the society of
thoracic surgeons, the Asia pacific heart rhythm society, and the
heart rhythm society. Heart Rhythm. 9:632–696.e21. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Jaïs P, Cauchemez B, Macle L, Daoud E,
Khairy P, Subbiah R, Hocini M, Extramiana F, Sacher F, Bordachar P,
et al: Catheter ablation versus antiarrhythmic drugs for atrial
fibrillation: The A4 study. Circulation. 118:2498–2505.
2008.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Wilber DJ, Pappone C, Neuzil P, De Paola
A, Marchlinski F, Natale A, Macle L, Daoud EG, Calkins H, Hall B,
et al: Comparison of antiarrhythmic drug therapy and radiofrequency
catheter ablation in patients with paroxysmal atrial fibrillation:
A randomized controlled trial. JAMA. 303:333–340. 2010.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Wazni OM, Marrouche NF, Martin DO, Verma
A, Bhargava M, Saliba W, Bash D, Schweikert R, Brachmann J, Gunther
J, et al: Radiofrequency ablation vs antiarrhythmic drugs as
first-line treatment of symptomatic atrial fibrillation: A
randomized trial. JAMA. 293:2634–2640. 2005.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Hiasa KI, Kaku H, Inoue H, Yamashita T,
Akao M, Atarashi H, Koretsune Y, Okumura K, Shimizu W, Ikeda T, et
al: Age-related differences in the clinical characteristics and
treatment of elderly patients with atrial fibrillation in
Japan-insight from the ANAFIE (All Nippon AF In Elderly) registry.
Circ J. 84:388–396. 2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Shao XH, Yang YM, Zhu J, Zhang H, Liu Y,
Gao X, Yu LT, Liu LS, Zhao L, Yu PF, et al: Comparison of the
clinical features and outcomes in two age-groups of elderly
patients with atrial fibrillation. Clin Interv Aging. 9:1335–1342.
2014.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Zakeri R, Chamberlain AM, Roger VL and
Redfield MM: Temporal relationship and prognostic significance of
atrial fibrillation in heart failure patients with preserved
ejection fraction: A community-based study. Circulation.
128:1085–1093. 2013.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Packer DL, Kowal RC, Wheelan KR, Irwin JM,
Champagne J, Guerra PG, Dubuc M, Reddy V, Nelson L, Holcomb RG, et
al: Cryoballoon ablation of pulmonary veins for paroxysmal atrial
fibrillation: First results of the North American arctic front
(STOP AF) pivotal trial. J Am Coll Cardiol. 61:1713–1723.
2013.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Morillo CA, Verma A, Connolly SJ, Kuck KH,
Nair GM, Champagne J, Sterns LD, Beresh H, Healey JS and Natale A:
RAAFT-2 Investigators. Radiofrequency ablation vs antiarrhythmic
drugs as first-line treatment of paroxysmal atrial fibrillation
(RAAFT-2): A randomized trial. JAMA. 311:692–700. 2014.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Corrado A, Patel D, Riedlbauchova L, Fahmy
TS, Themistoclakis S, Bonso A, Rossillo A, Hao S, Schweikert RA,
Cummings JE, et al: Efficacy, safety, and outcome of atrial
fibrillation ablation in septuagenarians. J Cardiovasc
Electrophysiol. 19:807–811. 2008.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Zado E, Callans DJ, Riley M, Hutchinson M,
Garcia F, Bala R, Lin D, Cooper J, Verdino R, Russo AM, et al:
Long-term clinical efficacy and risk of catheter ablation for
atrial fibrillation in the elderly. J Cardiovasc Electrophysiol.
19:621–626. 2008.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Haegeli LM, Duru F, Lockwood EE, Lüscher
TF, Sterns LD, Novak PG and Leather RA: Ablation of atrial
fibrillation after the retirement age: Considerations on safety and
outcome. J Interv Card Electrophysiol. 28:193–197. 2010.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Baman TS, Jongnarangsin K, Chugh A,
Suwanagool A, Guiot A, Madenci A, Walsh S, Ilg KJ, Gupta SK,
Latchamsetty R, et al: Prevalence and predictors of complications
of radiofrequency catheter ablation for atrial fibrillation. J
Cardiovasc Electrophysiol. 22:626–631. 2011.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Deshmukh A, Patel NJ, Pant S, Shah N,
Chothani A, Mehta K, Grover P, Singh V, Vallurupalli S, Savani GT,
et al: In-hospital complications associated with catheter ablation
of atrial fibrillation in the United States between 2000 and 2010:
Analysis of 93 801 procedures. Circulation. 128:2104–2112.
2013.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Cappato R, Calkins H, Chen SA, Davies W,
Iesaka Y, Kalman J, Kim YH, Klein G, Natale A, Packer D, et al:
Updated worldwide survey on the methods, efficacy, and safety of
catheter ablation for human atrial fibrillation. Circ Arrhythm
Electrophysiol. 3:32–38. 2010.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Thomas D, Katus HA and Voss F:
Asymptomatic pulmonary vein stenosis after cryoballoon catheter
ablation of paroxysmal atrial fibrillation. J Electrocardiol.
44:473–476. 2011.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Rottner L, Fink T, Heeger CH, Schlüter M,
Goldmann B, Lemes C, Maurer T, Reißmann B, Rexha E, Riedl J, et al:
Is less more? Impact of different ablation protocols on
periprocedural complications in second-generation cryoballoon based
pulmonary vein isolation. Europace. 20:1459–1467. 2018.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Tokutake K, Tokuda M, Ogawa T, Matsuo S,
Yoshimura M and Yamane T: Pulmonary vein stenosis after
second-generation cryoballoon ablation for atrial fibrillation.
HeartRhythm Case Rep. 3:36–39. 2017.PubMed/NCBI View Article : Google Scholar
|