Introduction
Oral cancer is defined as a group of cancers
originating from the oral cavity or lip and represents one of the
most common malignancies worldwide (1). In 2020, a total of 377,713 new cases
were diagnosed globally, and 177,757 patients succumbed to this
disease (2). Oral squamous cell
carcinoma is the most common pathological type of oral cancer; it
represents more than 90% of the cases (3). Some modifiable risk factors have been
reported to contribute to the development of oral cancer, including
tobacco smoking, alcohol consumption, betel quid, human
papillomavirus infection, and poor oral hygiene (4). The overall 5-year survival rate for
oral cancer is 75–90% for stage I and 10–22% for stage IV (5). Currently, the standard treatment for
oral cancer includes surgical resection, radiotherapy, and
chemotherapy with molecular-targeted therapy and immunotherapy
using immune checkpoint inhibitors. These treatments are associated
with various adverse events, and many patients develop drug
resistance during treatment. Thereby, local and regional
recurrences are reported in 90% of oral cancers after surgery and
radiotherapy (6,7). At present, clinical trials for head
and neck squamous cell carcinoma (HNSCC) treated with immune
checkpoint inhibitors are ongoing. Anti-PD-1 antibodies, such as
nivolumab and pembrolizumab, have been approved by the US Food and
Drug Administration for patients with relapsed or metastatic HNSCC,
as well as cisplatin-resistant tumors (8). Anti-epidermal growth factor receptor
(EGFR) antibodies, such as cetuximab, have been approved for use in
combination with radiation therapy in patients with HNSCC (9). Despite these developments, efficacy
remains limited, and adverse events have been reported. Therefore,
further development of novel therapeutic strategies, such as
personalized therapies based on cancer biomarkers and novel
molecular-targeted therapies with no or low side effects in
patients with oral cancer, are needed.
To identify molecular targets for the diagnosis and
treatment of cancer, a genome-wide expression profile analysis and
subsequent tissue microarray analysis with solid tumor tissues and
normal tissues were performed. Several oncoantigens involved in the
development and/or progression of solid cancers were isolated
(10–36). This systematic strategy identified
Opa interacting protein 5 (OIP5) as a candidate molecular target
overexpressed in the majority of oral cancers.
OIP5 encodes a 25-kDa protein and was initially
identified in a yeast two-hybrid system (37). OIP5 contains a Yippee domain
(38) and a coiled-coil domain
(39), suggesting that it has a
role in cell proliferation and mitosis-associated processes. OIP5
is a component of the Mis18 complex, which consists of three
subcomplexes: Mis18α, Mis18β (OIP5), and Mis18BP1. OIP5 interacts
with Holliday junction recognition protein (HJURP) and mediates the
loading of newly synthesized centromeric protein A (CENP-A) on the
centromere by the Mis18 complex, which is required for accurate
chromosome segregation (40,41).
Previous findings indicate that OIP5 is overexpressed in various
types of human cancers, such as lung and esophageal carcinomas
(29), bladder cancer (42), gastric cancer (43), and glioblastoma (44); however, its role in oral
carcinogenesis and the clinical significance of OIP5 protein as a
tissue biomarker for oral cancer has yet to be clarified.
In the present study, the aim was to determine
whether OIP5 plays a significant role in the development of oral
cancer and is a putative cancer biomarker and therapeutic
target.
Materials and methods
Oral cancer cell lines and clinical
tissue samples
The following oral cancer cell lines were used in
this study: four tongue squamous cell carcinoma cell lines (SCC9,
CAL 27, HSC3, and HSC4), one pharynx squamous cell carcinoma
(FaDu), one mouth squamous cell carcinoma (HSC2), and one gingival
squamous cell carcinoma (Ca9-22). The human oral mucosa
keratinocyte (HOMK) cell line, used as a normal control, was
purchased from the Cell Research Corporation (Singapore). The
histology of the cell lines and resources are summarized in
Table I. All cells were grown in
monolayer in an appropriate medium. The oral cancer cell lines were
cultured at 37°C in a humidified atmosphere with 5% CO2
in a medium containing 10% fetal bovine serum (FBS) and antibiotics
(Thermo Fisher Scientific, Inc.). HOMK cells were grown in a medium
supplemented with EpiLife Defined Growth Supplement. In total, 13
oral squamous cell cancer tissue samples (5 females, 8 males;
median age, 63 years; age range, 45–74 years) were obtained from
ProteoGenex (Inglewood, USA), and a normal tongue tissue was
obtained from Clontech (USA). A total of 164 existing
formalin-fixed primary oral cancer tissue samples and adjacent
normal tissue samples obtained from patients with oral cancer who
had undergone surgery between 2004 and 2012 and treated with
adjuvant or neoadjuvant chemotherapy at Kumamoto University were
used in this study. The clinical stage of the tumor samples was
judged according to the Union for International Cancer Control TNM
classification (7th Edition of UICC; http://www.inen.sld.pe/portal/documentos/pdf/educacion/13072015_TNM%20Classification.pdf).
 | Table I.List of oral cancer cells and oral
mucosa keratinocytes used in the present study. |
Table I.
List of oral cancer cells and oral
mucosa keratinocytes used in the present study.
| Cell line | Histology | Resource | Catalog no. |
|---|
| FaDu | Squamous cell
carcinoma of the pharynx | ATCC | HTB-43 |
| SCC9 | Squamous cell
carcinoma of the tongue | ATCC | CRL-1629 |
| CAL 27 | Squamous cell
carcinoma of the tongue | ATCC | CRL-2095 |
| Ca9-22 | Gingival squamous
cell carcinoma | RIKEN BRC | RCB1976 |
| HSC2 | Squamous cell
carcinoma of the mouth | RIKEN BRC | RCB1945 |
| HSC3 | Squamous cell
carcinoma of the tongue | RIKEN BRC | RCB1975 |
| HSC4 | Squamous cell
carcinoma of the tongue | RIKEN BRC | RCB1902 |
| HOMK | Human oral mucosa
keratinocyte | Cell Research
Corporation Pte Ltd. | hOMK100 |
The study protocol and the use of existing clinical
materials were approved by the Ethics Committees [Kumamoto
University; Shiga University of Medical Science (no. G2009-163)]
based on the national ethical guidelines for human subjects. It was
confirmed that this study was fully ethically compliant, and that
informed consent was waived by the ethics committee due to the
retrospective nature of the study and the national ethical
guidelines.
Real-time PCR
Total RNA was extracted from cultured oral cancer
cells and oral cancer tissues using the Maxwell 16 LEV Simply RNA
purification kit (Promega Corp.) according to the manufacturer's
protocol. The RNA was reverse-transcribed into cDNA using the
PrimeScript RT Master Mix (Takara Bio Inc.). Gene expression was
measured by real-time PCR using TaqMan Universal Master Mix II and
TaqMan assays on a StepOnePlus thermocycler (Applied Biosystems;
Thermo Fisher Scientific, Inc.) according to the manufacturer's
instructions. The reaction conditions were as follows: initial
denaturation for 2 min at 50°C and 10 min at 95°C, followed by 40
cycles of 95°C for 1 sec and 60°C for 20 sec. Each experiment was
performed in triplicate. ACTB (Hs01060665_g1) as an internal
control and OIP5 (Hs00944000_g1) primers (Applied
Biosystems) were used for the PCR reaction. Relative OIP5
mRNA expression was calculated using the 2−ΔΔCt method
(45).
Western blot analysis
To prepare whole cell lysates, the cells were lysed
on ice in Pierce RIPA buffer (Thermo Fisher Scientific, Inc.)
supplemented with 1% protease inhibitor cocktail (Thermo Fisher
Scientific, Inc.). After homogenization, the cell lysates were
incubated on ice for 30 min and centrifuged at 14,000 × g for 15
min to separate the supernatant from the cellular debris. The
concentration of total protein was estimated using the Qubit
Protein Assay Kit (Thermo Fisher Scientific, Inc.), and the
proteins were mixed with SDS sample buffer, boiled at 100°C for 5
min, and incubated at room temperature for 5 min before loading
into 12% Mini-Protean® TGX gels (Bio-Rad Laboratories).
After electrophoresis at 200 V for 30 min, the proteins were
transferred to Trans-Blot® Turbo 0.2 µm PVDF membranes
(Bio-Rad Laboratories). The membranes were blocked with 5% nonfat
milk in TBST at room temperature for 1 h. A commercially available
rabbit polyclonal antibody to human OIP5 (dilution, 1:1,000; cat.
no. 12142-1-AP; ProteinTech Group) was incubated with the membrane
at room temperature for 1.5 h, followed by incubation with
horseradish peroxidase (HRP)-conjugated secondary antibodies (GE
Healthcare, UK) for 1 h at room temperature. Protein bands were
visualized by enhanced chemiluminescence using the Fusion Solo S
system (Vilber Lourmat, France).
Immunocytochemistry
The cultured cells were seeded into Lab-Tek II
chamber slides (Nalge Nunc Int.). After fixation in 4% formaldehyde
solution for 15 min at room temperature, the cells were washed
twice with PBS, and the upper part of the well was then removed. To
render the cells permeable, PBS containing 0.1% Triton X-100 was
added for 2 min at room temperature. The cells were covered with 3%
bovine serum albumin (BSA) for 30 min at room temperature to block
nonspecific binding. Then, the membrane was incubated with rabbit
anti-OIP5 antibody (ca. no. 12142-1-AP; ProteinTech Group) in PBS
containing 1% BSA and 0.1% Tween-20 at 4°C overnight in a wet box.
After washing with PBS, a goat anti-rabbit secondary antibody
conjugated to Alexa 488 (Thermo Fisher Scientific, Inc.) was added
for 1 h at room temperature in a wet box in the dark. Nuclei were
stained with Vectashield Mounting Medium containing DAPI (Vector
Laboratories). OIP5 antibody staining was visualized using
fluorescence microscopy (BZ-X710, Keyence, Japan).
Immunohistochemistry and tissue
microarray analysis
Tumor tissue microarrays were constructed according
to previously published procedures using 164 formalin-fixed primary
oral cancer tissues that were surgically resected (63 patients
treated with curative surgery and neoadjuvant chemotherapy, and 101
patients treated with curative surgery and adjuvant chemotherapy).
The tissue areas selected for sampling were determined by visual
alignment with the corresponding hematoxylin and eosin
(H&E)-stained sections on the slides. Three, four, or five
tissue cores (diameter, 0.6 mm; height, 3–4 mm) taken from donor
tumor blocks were placed into recipient paraffin blocks using a
tissue microarrayer (Beecher Instruments Inc.). A core of normal
oral epithelial tissue was punched in each case, and 5-µm sections
of the resulting microarray blocks were used for
immunohistochemical analysis.
Tissue microarray slides were deparaffinized in
xylene and rehydrated in graded concentrations of ethanol. For
antigen retrieval, the slides were boiled in Target Retrieval
Solution (pH 6.0) (Dako; Agilent Technologies, Inc.). A rabbit
polyclonal anti-OIP5 antibody (cat. no. 12142-1-AP; ProteinTech
Group) was added to each slide and incubated overnight after
blocking endogenous peroxidase activity in a 0.3% hydrogen
peroxide/methanol mixed solution and nonspecific protein binding
sites in protein blocking buffer (cat. no. X0909; Dako Cytomation).
After primary antibody incubation, sections were incubated with an
HRP-labeled anti-rabbit IgG secondary antibody (Dako Cytomation)
for 30 min. Chromogen substrate was added to visualize labeled
protein, and the specimens were counterstained with H&E.
Because the intensity of staining within each tumor tissue core was
mostly homogeneous, positivity for OIP5 was assessed
semi-quantitatively by three independent investigators without
prior knowledge of the clinicopathological data, each of whom
recorded staining intensity as positive or negative. Cases were
accepted as positive if at least two investigators independently
scored them as such.
Cell growth assay
The SCC9 and HSC2 cell lines that did not express
endogenous OIP5 were plated at 0.8×106 cells/100-mm dish
and transfected with OIP5-expressing plasmid (pCMV6-Entry-Myc-DDK,
OriGene, USA) or mock plasmids by FuGENE 6 (Promega Corp.). Cell
viability was assessed using MTT assay (Cell Counting Kit-8;
Dojindo Laboratories, Japan) 5 days after plasmid transfection.
RNA interference assay
To investigate the biological function of OIP5 in
oral cancer cells, small interfering RNAs (siRNAs) (Sigma-Aldrich;
Merck KGaA) were transfected into Ca9-22 and CAL 27 cells using
Lipofectamine 2000 reagent (Invitrogen; Thermo Fisher Scientific,
Inc.) according to the manufacturer's instructions. The sequences
targeting each gene were as follows: si-OIP5-#1,
5′-GGUUCACUCAAAGGCAGUA-3′; si-OIP5-#2,
5′-CUAUUUACCUUUAGGCUGA-3′; control 1: si-LUC,
5′-CGUACGCGGAAUACUUCGA-3′; and control 2: si-EGFP,
5′-GAAGCAGCACGACUUCUUC-3′. Cell numbers and viability were measured
by colony formation and MTT assays using Cell Counting Kit-8
solution (Dojindo Laboratories) 6 days after transfection.
Flow cytometry
Cell cycle analysis was performed using a Cycletest
Plus DNA reagent kit (BD Biosciences). Ca9-22 and CAL 27 cells, for
measuring DNA ploidy, were harvested by trypsinization 72 h after
si-OIP5-#2 or si-LUC transfection and suspended at a concentration
of 1×106 cells/ml. The sample was filtered through a
50-µm nylon mesh, kept on ice, and protected from light. Cell cycle
analysis was conducted within 3 h using a flow cytometer (BD
FACSCanto™ II. The DNA content was measured in cells selected from
at least 20,000 ungated cells.
Live-cell imaging
The Ca9-22 and CAL 27 cells transfected with
si-OIP5-#2 or si-LUC were seeded on 35-mm glass
dishes in an appropriate culture medium containing 10% FBS. The
Evos FL Auto Cell Imaging System (Life Technologies; Thermo Fisher
Scientific, Inc.) time-lapse microscopy was used to monitor changes
in cell morphology and death after transfection with OIP5 siRNA.
Live-cell imaging was initiated 72 h after si-LUC and
si-OIP5 transfection, and images were captured every 15 min
for 24 h up to 96 h.
Senescence assay
The cells were plated into 35-mm-diameter culture
dishes up to 5 days after siRNA transfection into Ca9-22 and CAL 27
cells and stained with the senescence β-Galactosidase Staining Kit
#9860 (Cell Signaling Technology, Inc.). The plates were incubated
overnight at 37°C in a non-CO2 containing dry incubator.
The percentage of senescence-associated β-galactosidase (SA-β-gal)
positivity per 50 cells observed under a light microscope was
calculated. Senescence-associated heterochromatic foci (SAHF) were
detected by DAPI staining 96 h after siRNA transfection.
Statistical analysis
Statistical analyses were performed using the
StatView 5.0 Statistical Program (SAS Institute, Inc.). The
significance test analyzing the difference between two groups of
cell-based assays was performed using the Student's t-test. One-way
ANOVA followed by Tukey's post hoc test was performed to compare
the means of each group with those of every other group when
performing multiple comparisons. Results are presented as mean ±
standard deviation. Each experiment was performed in triplicate. We
used contingency tables to analyze the relationship between OIP5
expression and clinicopathological variables (e.g., sex, age,
primary tumor region, and pathological TNM stage) in patients with
oral cancer. Tumor-specific survival curves were generated on the
date of surgery to the time of death from oral cancer or last
follow-up observation. Kaplan-Meier curves were calculated for each
relevant variable and OIP5 expression in oral tumors. The
differences in survival times among the patient subgroups were
analyzed using the log-rank test. Univariate and multivariate
analyses were performed using the Cox proportional hazard
regression model to determine the association between
clinicopathological variables and cancer-related mortality. First,
we analyzed associations between death and possible prognostic
factors, including OIP5 positivity, age, sex, primary region, pT
factor, pN factor, and treatment (curative surgery with adjuvant
chemotherapy vs. curative surgery with neoadjuvant chemotherapy).
Second, a multivariate Cox analysis was performed in a stepwise
fashion in which OIP5 positivity was forced into the model along
with each significant variable. As significant prognostic factors
were continually added to the model, P<0.05 was considered
statistically significant and an independent factor.
Database analysis
The gene expression and signal pathways related to
OIP5 were screened using the ONCOMINE database (https://www.oncomine.org/resource/login.html), Gene
Set Enrichment Analysis (GSEA) database (https://www.gsea-msigdb.org/gsea/msigdb/search.jsp),
BioGPS database (http://biogps.org/#goto=welcome), and UALCAN database
(http://ualcan.path.uab.edu/). Mutational
status of the OIP5 gene was screened using cBioPortal for
Cancer Genomics database (http://www.cbioportal.org/).
Results
Expression of OIP5 in oral cancer
cells and tissues
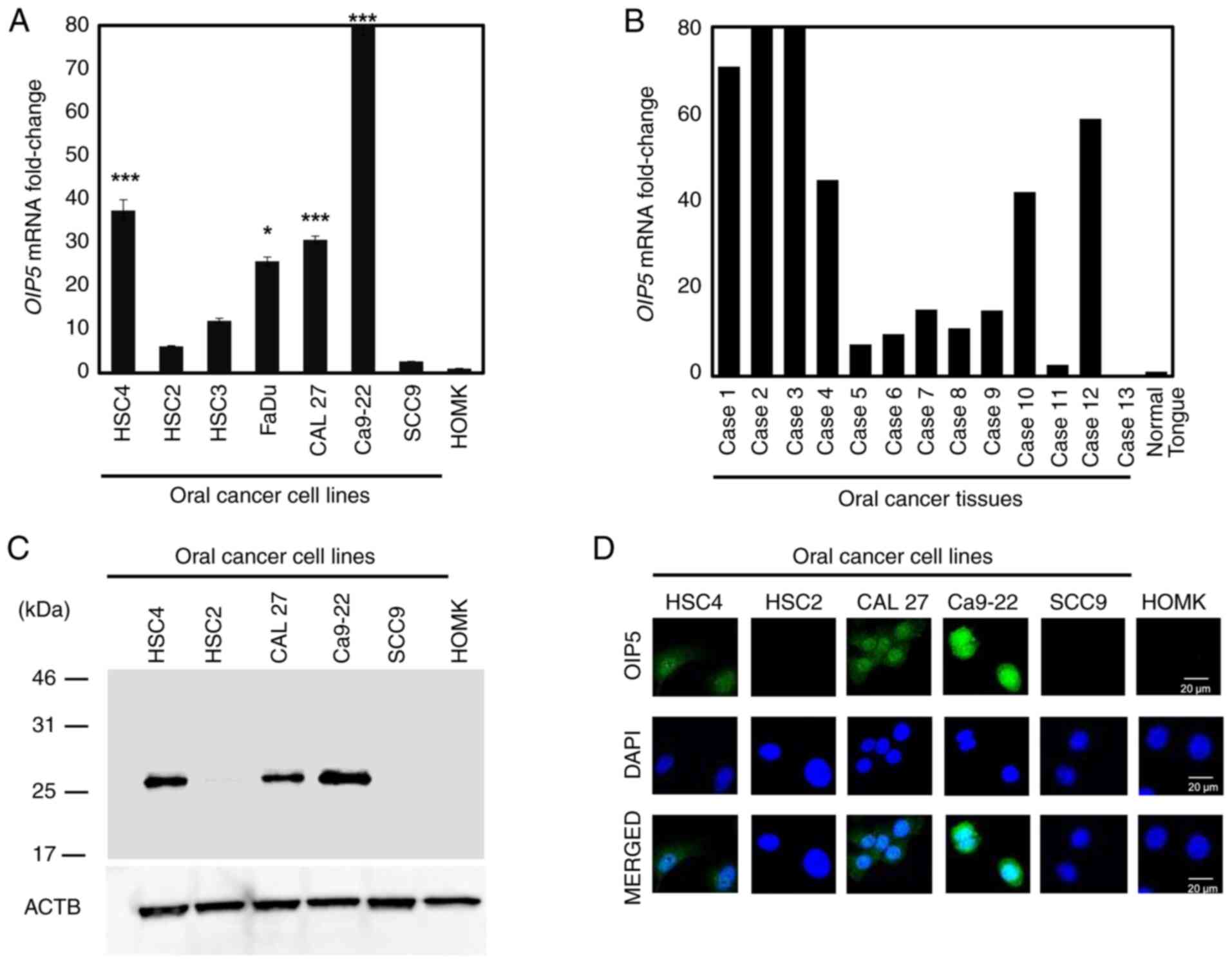
We first confirmed that OIP5 mRNA was
frequently and significantly overexpressed in many of the oral
cancer cell lines, while it was barely detectable in the HOMKs
(Fig. 1A). Additionally,
OIP5 mRNA was frequently overexpressed in most of the oral
cancer tissues, while its expression was hardly detectable in
healthy tongue tissues (Fig. 1B).
Western blotting revealed that OIP5 protein was expressed in many
oral cancer cell lines; however, no expression was detected in the
HOMK cells (Fig. 1C).
Immunocytochemical analysis revealed that OIP5 protein was
localized in the nucleus and cytoplasm of oral cancer cells
(Fig. 1D).
Correlation of OIP5 expression with
poor clinical outcome for patients with oral cancer
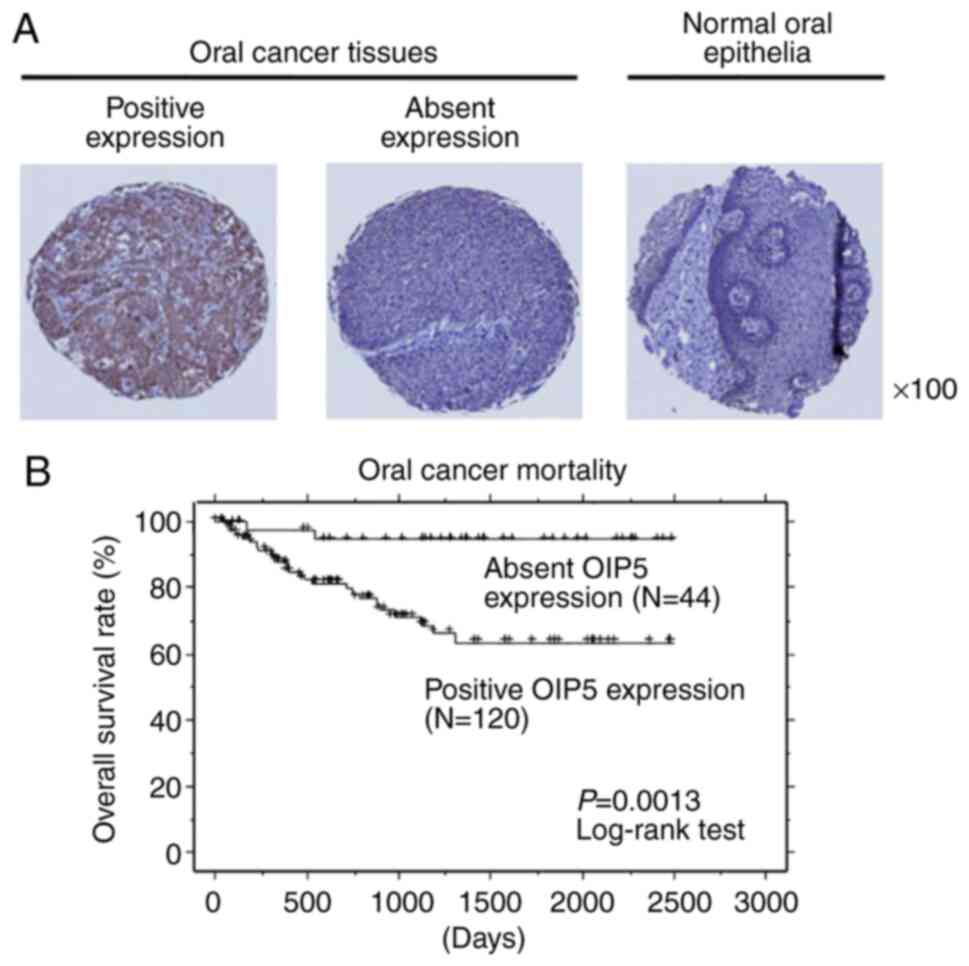
To verify the biological and clinicopathological
significance of OIP5 in oral cancer tissues, we examined the
expression of OIP5 protein using tissue microarrays containing oral
cancer tissues from 164 patients who underwent radical resection.
Immunohistochemical staining using anti-OIP5 antibody demonstrated
that OIP5 expression was detectable in 120 of 164 (73.2%) oral
cancer cases; however, it was barely detectable in the surrounding
normal tissues (Fig. 2A). Next, we
assessed the association between OIP5 protein expression and
clinical parameters. Sex (higher in females; P=0.0202 using
Fisher's exact test) and region (higher in the gingiva, buccal
mucosa, and others; P=0.0029 using Fisher's exact test) were
significantly associated with positive OIP5 expression (Table II). Furthermore, the positivity of
OIP5 protein expression was also significantly related to poorer
prognosis for patients with oral cancer (P=0.0013 using log-rank
test; Fig. 2B). In addition, we
also performed univariate analysis to determine the correlation
between patient prognosis and other clinicopathological factors,
including age (<65 vs. ≥65 years), sex (male vs. female), region
(tongue vs. others), pT classification (T1-T2 vs. T3-T4), pN
classification (N0 vs. N1-N2), treatment (curative surgery with
adjuvant chemotherapy vs. curative surgery with neoadjuvant
chemotherapy), and OIP5 expression status (absent vs. positive). Of
these parameters, positive OIP5 expression (P=0.0061) and advanced
pN stage (P=0.0029) were significantly associated with poor
prognosis. Furthermore, multivariate analysis showed that positive
OIP5 expression (P=0.0086) and advanced pN factor (P=0.0068) were
independent prognostic factors (Table
III).
| Table II.Association between OIP5 protein
expression in oral cancer tissues and patient characteristics
(N=164). |
Table II.
Association between OIP5 protein
expression in oral cancer tissues and patient characteristics
(N=164).
| Parameters | Total | Positive OIP5
expression | Negative OIP5
expression | P-value (positive
vs. negative) |
|---|
| Total number of
specimens | 164 | 120 | 44 |
|
| Treatment |
|
|
| 0.8566 |
|
Neoadjuvant | 63 | 47 | 16 |
|
|
Adjuvant | 101 | 73 | 28 |
|
| Sex |
|
|
| 0.0202a |
|
Male | 94 | 62 | 32 |
|
|
Female | 70 | 58 | 12 |
|
| Age (years) |
|
|
| 0.4733 |
|
<65 | 66 | 46 | 20 |
|
|
≥65 | 98 | 74 | 24 |
|
| Region |
|
|
| 0.0029a |
|
Tongue | 80 | 50 | 30 |
|
|
Othersb | 84 | 70 | 14 |
|
| pT factor |
|
|
| 0.2747 |
|
T1-T2 | 103 | 72 | 31 |
|
|
T3-T4 | 61 | 48 | 13 |
|
| pN
factor |
|
|
| 0.3225 |
| N0 | 120 | 85 | 35 |
|
|
N1-N2 | 44 | 35 | 9 |
|
| Table III.Cox proportional hazards model
analysis of prognostic factors in the patients with oral
cancer. |
Table III.
Cox proportional hazards model
analysis of prognostic factors in the patients with oral
cancer.
| Variables | HR | 95% CI |
Unfavorable/Favorable | P-value |
|---|
| Univariate
analysis |
|
|
|
|
| OIP5
expression | 7.482 | 1.773-31.577 |
Positive/Negative | 0.0061a |
| Age
(years) | 1.979 | 0.904-4.331 | ≥65/<65 | 0.0877 |
|
Sex | 1.831 | 0.893-3.755 | Female/Male | 0.0986 |
|
Region | 1.538 | 0.745-3.176 | Othersb/Tongue | 0.2443 |
| T
factor | 1.461 | 0.709-3.011 | T3-T4/T1-T2 | 0.3035 |
| N
factor | 2.977 | 1.451-6.108 | N1-N2/N0 | 0.0029a |
|
Treatment | 1.122 | 0.587-2.532 |
Neoadjuvant/Adjuvant chemotherapy | 0.5957 |
| Multivariate
analysis |
|
|
|
|
| OIP5
expression | 6.907 | 1.634-29.204 |
Positive/Negative | 0.0086a |
| N
factor | 2.699 | 1.315-5.542 | N1-N2/N0 | 0.0068a |
Enforced OIP5 expression promotes oral
cancer cell growth
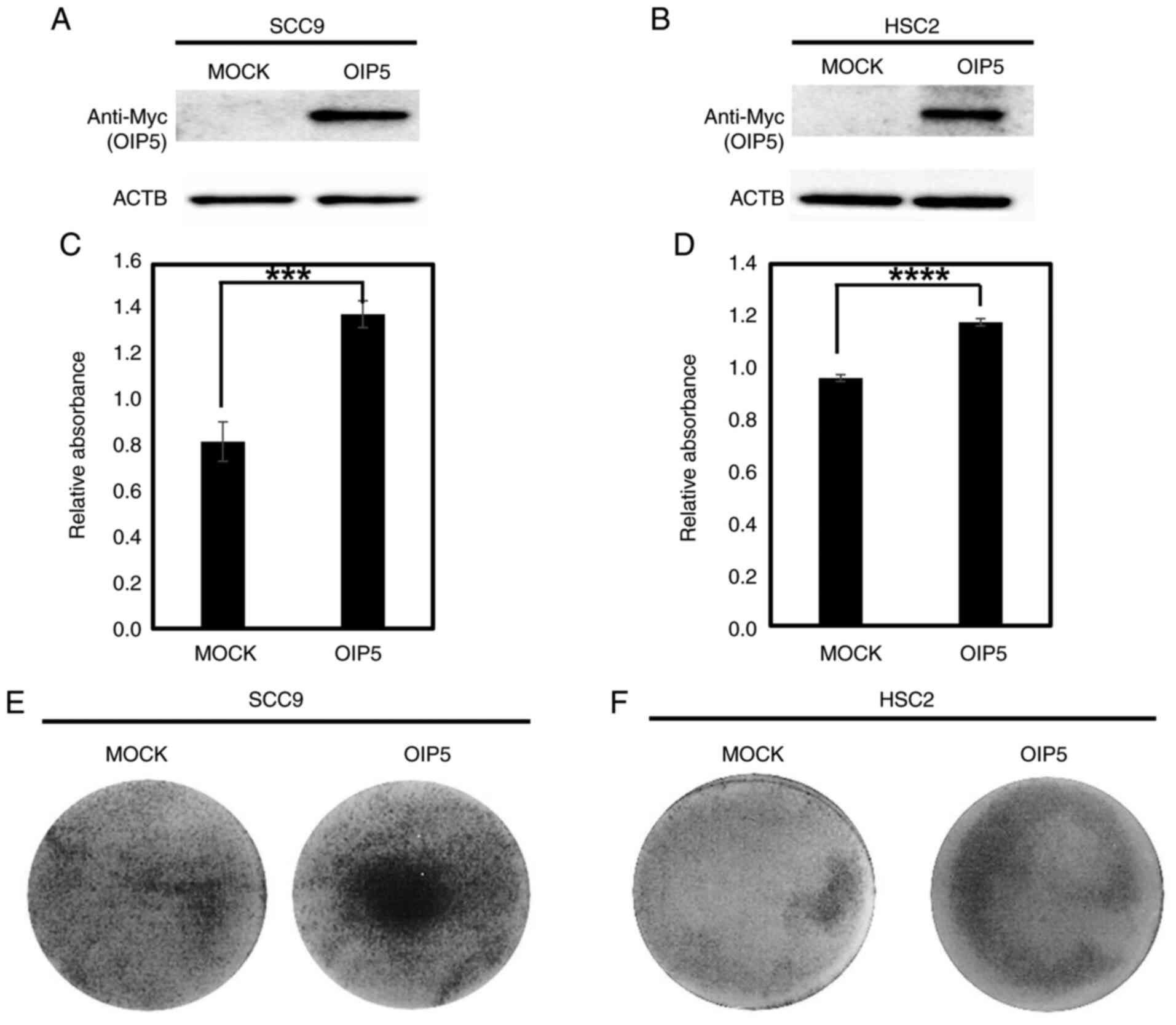
To evaluate the potential role of OIP5 in
tumorigenesis, plasmids expressing OIP5 or mock plasmids
were transfected into SCC9 and HSC2 cells that did not express
endogenous OIP5. After confirmation of exogenous OIP5 expression by
western blot analysis (Fig. 3A and
B), cell viability was examined using MTT assay. It was found
that the viability of OIP5-overexpressing cells was significantly
higher compared than the viability of the cells transfected with
the mock vectors (Fig. 3C and D).
The colony formation assay also showed that OIP5 overexpression
increased the numbers of SCC9 and HSC2 cells (Fig. 3E and F).
Inhibition of oral cancer cell growth
by suppression of OIP5 expression
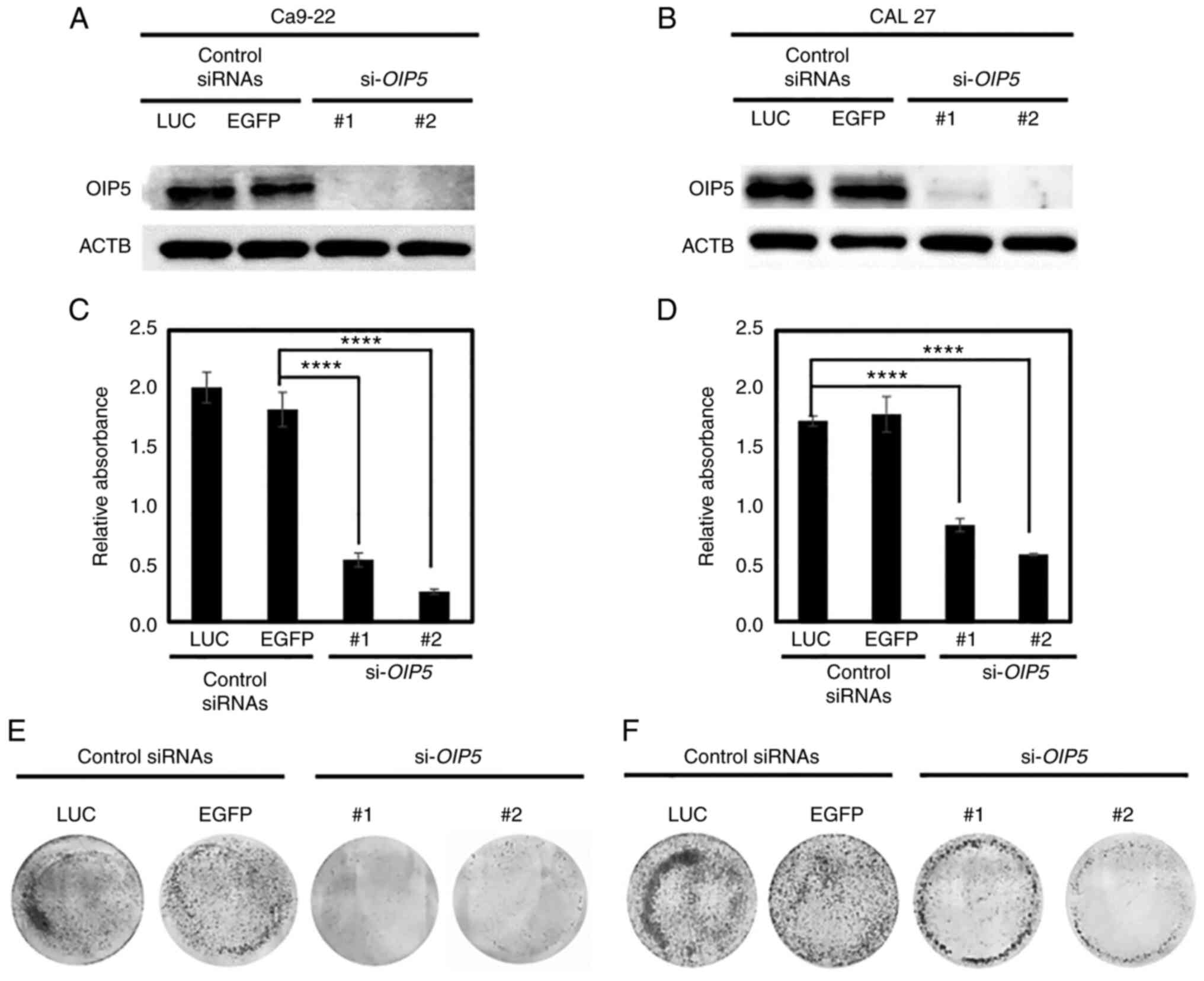
To further assess the role of OIP5 in oral cancer
development and progression, siRNAs against OIP5
(si-OIP5-#1 and si-OIP5-#2) along with control siRNAs
(si-LUC and si-EGFP) were transfected into oral
cancer cell lines (Ca9-22 and CAL 27). After confirming the
reduction of OIP5 protein levels using western blot analysis
(Fig. 4A and B), we continually
performed an MTT assay and colony formation assay to examine the
role of OIP5 in tumor proliferation. The MTT assay showed that the
suppression of endogenous OIP5 expression by si-OIP5 effectively
inhibited oral cancer cell viability (P<0.0001) in the
si-OIP5-transfected Ca9-22 and CAL 27 cells compared with
si-controls (Fig. 4C and D). In
addition, colony formation assays demonstrated that the suppression
of OIP5 expression inhibited the growth of Ca9-22 and CAL 27 cells
compared with controls (Fig. 4E and
F).
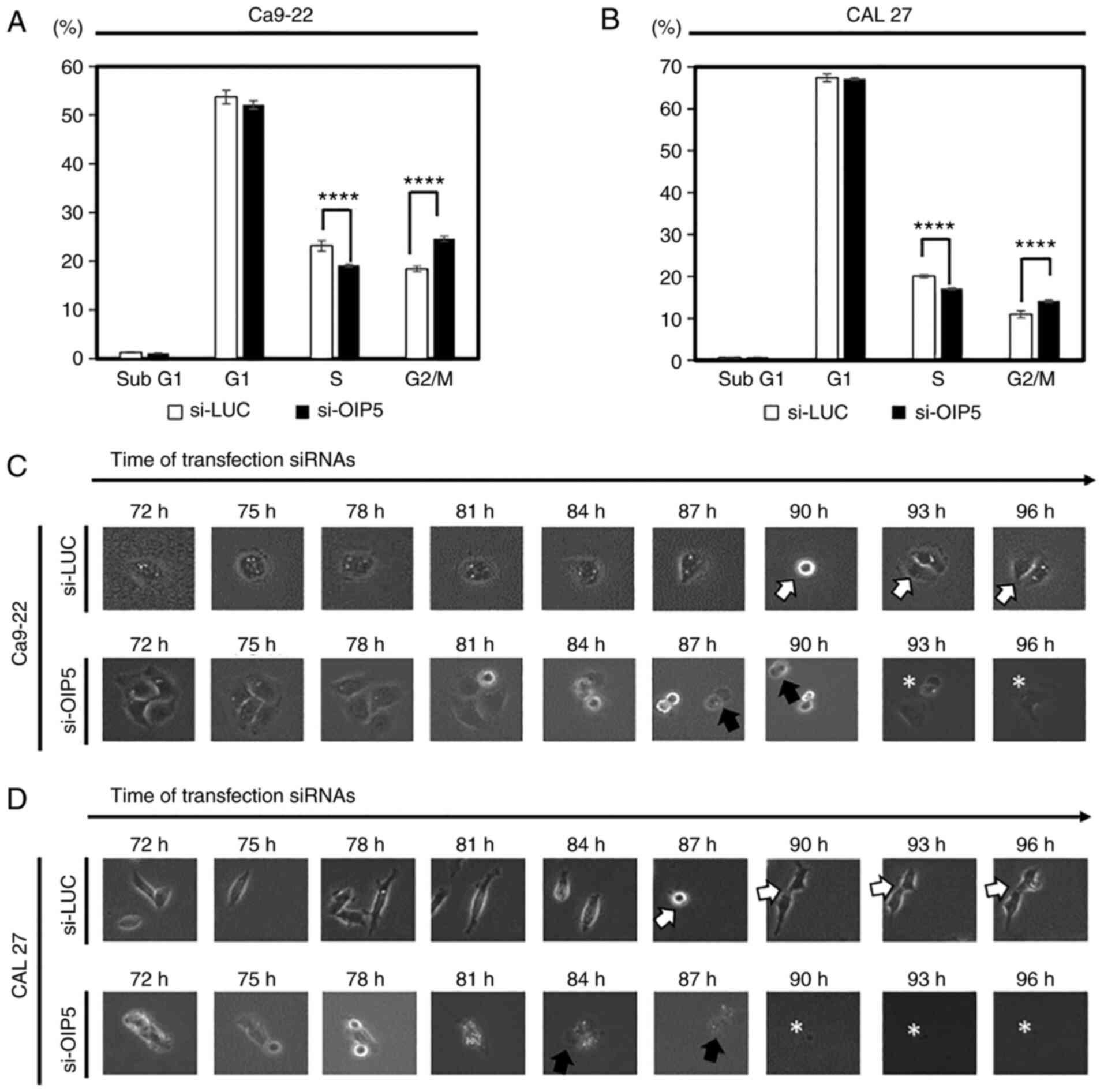
Cell cycle arrest by inhibition of
OIP5 expression
To examine the effect of OIP5 on cell cycle, flow
cytometric analyses of Ca9-22 and CAL 27 cells 72 h after siRNA
transfection was performed. Following OIP5 knockdown, we observed
that the cell population at the G2/M phase was significantly
increased (P<0.0001; Figs. 5A and
B and S1). To further clarify
the effect of OIP5 suppression on cellular morphology and cell
cycle, live-cell imaging of the Ca9-22 and CAL 27 cells was carried
out after si-OIP5 or control siRNA transfection. Time-lapse
microscopy revealed that the cells were normally divided in control
siRNA-transfected cells, whereas the cells failed to divide and
subsequently died in si-OIP5-transfected cells (Fig. 5C and D).
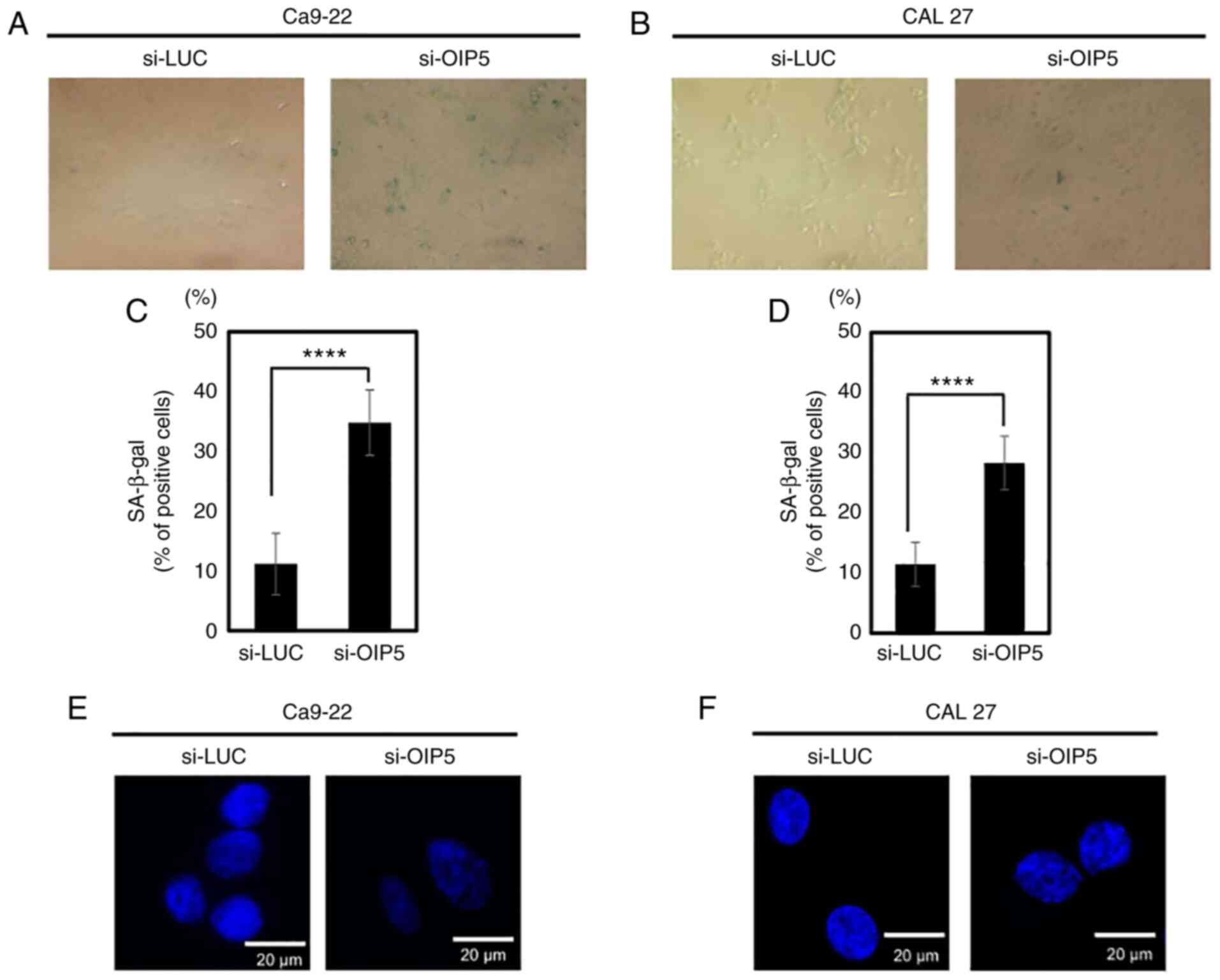
Suppression of OIP5 expression induces
cellular senescence
To examine whether OIP5 regulates the immortality of
oral cancer cells, senescence analysis was performed using acidic
β-galactosidase (SA-β-Gal) staining. OIP5 knockdown by
si-OIP5 significantly increased the number of cells stained
with senescent cell markers of SA-β-gal compared with the controls
(P<0.0001) (Fig. 6A-D). In
addition, SAHF in the nucleus were also detected in
si-OIP5-transfected oral cancer cells (Fig. 6E and F). The results indicate that
OIP5 is likely an important molecule for the immortality of oral
cancer cells.
Database analysis of OIP5 expression,
mutation, and its related pathways
To validate the expression of OIP5 in HNSCC
and normal tissues, we investigated the OIP5 data using
databases. BioGPS database analysis showed OIP5 mRNA
expression in testis is nearly 20 times higher than in other normal
tissues. UALCAN database showed among 520 cases of primary HNSCC
and 44 cases of normal tissues, OIP5 expression is significantly
higher in tumors than in normal tissues, and the methylation levels
of OIP5 promotor are likely to be lower in HNSCC tissues compare
with that in normal tissues. To examine the mechanism of oncogenic
OIP5 activation in oral cancer, we investigated the
OIP5 data using the cBioPortal for Cancer Genomics database.
Among 523 cases of HNSCC, mutations and deep deletions of
OIP5 were detected in only two cases (0.38%) and one case
(0.19%), respectively; however, no amplification of OIP5 was
observed. To screen the biological role of OIP5, we referred the
OIP5 data using pathway analysis. GSEA database revealed that OIP5
expression was associated with cell cycle and chromosome
maintenance, as well as the deposition of new CENP-A-containing
nucleosomes at the centromere. To examine the importance of the
functional association of OIP5 with CENP-A in oral cancer, we
confirmed the co-expression of OIP5 protein with CENP-A in HNSCC
using the ONCOMINE database (GSE12452 and GSE9844 datasets with
co-expression correlation coefficients of 0.818 and 0.663,
respectively).
Discussion
Oral cancer is highly malignant and shows resistance
to anticancer treatment. Despite progression following oral cancer
treatment, only a 5% improvement in overall survival has been
achieved over the last 2 decades (46). Targeting specific molecules involved
in oral cancer development may be an effective therapeutic approach
that exhibits high efficacy and less toxicity if the molecular
mechanisms of oral cancer proliferation and survival are well
defined. In the present study, a high level of OIP5 expression was
detected in most oral cancer cells and tissues, but low or no
detectable expression of OIP5 was observed in normal oral cells and
tissues. A gene expression database suggested that, except for the
testes, OIP5 is expressed at minimal levels in normal
tissues and organs, indicating that it is a candidate target for
the development of new diagnostics and therapeutics. In addition,
OIP5 expression is significantly increased in HNSCC, and the
methylation levels of OIP5 promotor are likely to be lower
in HNSCC tissues compare with that in normal tissues. Genetic
mutation and amplification of OIP5 are not frequent in
HNSCC. Therefore, OIP5 overexpression may be caused by an
epigenetic mechanism in oral cancer cells. Further analysis of the
transcriptional regulation of OIP5 is warranted.
Tissue microarray analysis showed that OIP5
expression was associated with poor clinical outcomes for patients
with oral cancer. We found that there was no significant
association between the type of oral cancer treatment (neoadjuvant
cases and adjuvant cases) and OIP5 protein expression level in oral
cancer tissues (positive vs. negative; P=0.8566), thus confirming
that neoadjuvant chemotherapy did not affect OIP5 expression. In
addition, multivariate analysis showed that positive OIP5
expression was an independent prognostic factor, indicating that
OIP5 expression in oral cancer tissues may represent a clinical
prognostic indicator that warrants further study in patients
receiving chemotherapy for oral cancer.
The exogenous expression of OIP5 in oral cancer cell
lines that did not normally express endogenous OIP5 enhanced cell
growth. In contrast, OIP5 knockdown led to G2/M cell cycle arrest
and subsequent cell death and/or cellular senescence in oral cancer
cells, as monitored by live-cell imaging and senescence assays;
this suggests that OIP5 may play a role in cell cycle and cellular
senescence. Therefore, targeting OIP5 and its pathway with
selective small molecule inhibitors and/or gene therapy may be a
therapeutic strategy for oral cancer.
Using the database, we found that OIP5 expression
was associated with cell cycle and chromosome maintenance as well
as the deposition of new CENP-A-containing nucleosomes at the
centromere. The old CENP-A nucleosome recruits CENP-C through their
interaction. In addition, CENP-C recruits the Mis18 complex
containing OIP5 as a component at late anaphase when CDK1 activity
is markedly reduced. Thereby, the Mis18 complex recruits the
prenucleosomal CENP-A complex through the direct binding of Mis18β
and HJURP (41). Previous reports
have demonstrated that the centromere recruitment of newly
synthesized CENP-A was rapidly abolished by the suppression of OIP5
expression in HeLa cells, followed by defects, such as misaligned
chromosomes, anaphase missegregation, and interphase micronuclei
(40). Those cell defects could
support our results that depletion of OIP5 inhibits oral cancer
cell proliferation. To examine the importance of the functional
association of OIP5 with CENP-A in oral cancer, we confirmed the
co-expression of OIP5 protein with CENP-A using the database. To
identify novel pathways related to OIP5 overexpression, further
investigation of downstream signaling of OIP5 is important for
clarifying the role of OIP5 in oral cancer development.
In summary, OIP5 is likely to function as an
oncoprotein in oral cancer and may play an important role in oral
cancer proliferation and survival. OIP5 is a putative biomarker
that may predict the prognosis of patients with oral cancer.
Therefore, targeting OIP5 may be useful for developing novel
treatments, including immunotherapies and molecular-targeted
therapies, which may exert strong biological effects with minimal
adverse effects.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This research study was supported in part by a Grant-in-Aid for
Scientific Research (B), Grant-in-Aid for Challenging Research
(Exploratory), and Grant-in-Aid for Scientific Research on
Innovative Areas from the Japan Society for the Promotion of
Science (JSPS KAKENHI, grant nos. 15H04761, 19H03559, 21K19444 and
16H06277). YD is a member of the Shiga Cancer Treatment Project
supported by Shiga Prefecture (Japan) and the International Joint
Research Project (FY2016-2021) of the Institute of Medical Sciences
(The University of Tokyo).
Availability of data and materials
All data generated or analyzed in this study are
included in the published paper.
Authors' contributions
MZ, AT, and YD conceptualized and designed the
study. MZ, AT, and YD developed the study methodology. YY, MS, and
YD acquired the data (acquiring and managing patients and providing
facilities). MZ, AT, BT, and YD analyzed and interpreted the data
(statistical analysis, biostatistics, and computational analysis)
and confirmed the accuracy. MZ, AT, and YD wrote, reviewed, and/or
revised the manuscript. MZ, AT, and YD were involved in
administrative, technical, or material support (reporting or
organizing data and constructing databases). YD supervised the
study. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committees (Kumamoto University; Shiga University of Medical
Science).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
BSA
|
bovine serum albumin
|
|
EGFR
|
epidermal growth factor receptor
|
|
FBS
|
fetal bovine serum
|
|
H&E
|
hematoxylin and eosin
|
|
HJURP
|
Holliday junction recognition
protein
|
|
HNSCC
|
head and neck squamous cell
carcinoma
|
|
HOMKs
|
human oral mucosa keratinocytes
|
|
OIP5
|
opa interacting protein 5
|
|
SAHF
|
senescence-associated heterochromatic
foci
|
|
SaS
|
StatView statistical
|
References
|
1
|
Montero PH and Patel SG: Cancer of the
oral cavity. Surg Oncol Clin N Am. 24:491–508. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dumache R, Rogobete AF, Andreescu N and
Puiu M: Genetic and epigenetic biomarkers of molecular alterations
in oral carcinogenesis. Clin Lab. 61:1373–1381. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Oji C and Chukwuneke F: Poor oral hygiene
may be the sole cause of oral cancer. J Maxillofac Oral Surg.
11:379–383. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
da Silva SD, Hier M, Mlynarek A, Kowalski
LP and Alaoui-Jamali MA: Recurrent oral cancer: Current and
emerging therapeutic approaches. Front Pharmacol. 3:1492012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kareemaghay S and Tavassoli M: Clinical
immunotherapeutic approaches for the treatment of head and neck
cancer. Int J Oral Maxillofac Surg. 48:419–436. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Carvalho ALKL, Kowalski LP, Agra IM,
Pontes E, Campos OD and Pellizzon AC: Treatment results on advanced
neck metastasis (N3) from head and neck squamous carcinoma.
Otolaryngol Head Neck Surg. 132:862–868. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ferris RL, Blumenschein G Jr, Fayette J,
Guigay J, Colevas AD, Licitra L, Harrington K, Kasper S, Vokes EE,
Even C, et al: Nivolumab for recurrent squamous-cell carcinoma of
the head and neck. N Engl J Med. 375:1856–1867. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cripps C, Winquist E, Devries MC,
Stys-Norman D and Gilbert R; Head Neck Cancer Disease Site Group, :
Epidermal growth factor receptor targeted therapy in stages III and
IV head and neck cancer. Curr Oncol. 17:37–48. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Daigo Y and Nakamura Y: From cancer
genomics to thoracic oncology: Discovery of new biomarkers and
therapeutic targets for lung and esophageal carcinoma. Gen Thorac
Cardiovasc Surg. 56:43–53. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Daigo Y, Takano A, Teramoto K, Chung S and
Nakamura Y: A systematic approach to the development of novel
therapeutics for lung cancer using genomic analyses. Clin Pharmacol
Ther. 94:218–223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ishikawa N, Daigo Y, Takano A, Taniwaki M,
Kato T, Hayama S, Murakami H, Takeshima Y, Inai K, Nishimura H, et
al: Increases of amphiregulin and transforming growth factor-alpha
in serum as predictors of poor response to gefitinib among patients
with advanced non-small cell lung cancers. Cancer Res.
65:9176–9184. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ishikawa N, Daigo Y, Yasui W, Inai K,
Nishimura H, Tsuchiya E, Kohno N and Nakamura Y: ADAM8 as a novel
serological and histochemical marker for lung cancer. Clin Cancer
Res. 10:8363–8370. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kakiuchi S, Daigo Y, Ishikawa N, Furukawa
C, Tsunoda T, Yano S, Nakagawa K, Tsuruo T, Kohno N, Fukuoka M, et
al: Prediction of sensitivity of advanced non-small cell lung
cancers to gefitinib (Iressa, ZD1839). Hum Mol Genet. 13:3029–3043.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kato T, Daigo Y, Hayama S, Ishikawa N,
Yamabuki T, Ito T, Miyamoto M, Kondo S and Nakamura Y: A novel
human tRNA-dihydrouridine synthase involved in pulmonary
carcinogenesis. Cancer Res. 65:5638–5646. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kikuchi T, Daigo Y, Katagiri T, Tsunoda T,
Okada K, Kakiuchi S, Zembutsu H, Furukawa Y, Kawamura M, Kobayashi
K, et al: Expression profiles of non-small cell lung cancers on
cDNA microarrays: Identification of genes for prediction of
lymph-node metastasis and sensitivity to anti-cancer drugs.
Oncogene. 22:2192–2205. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Suzuki C, Daigo Y, Ishikawa N, Kato T,
Hayama S, Ito T, Tsuchiya E and Nakamura Y: ANLN plays a critical
role in human lung carcinogenesis through the activation of RHOA
and by involvement in the phosphoinositide 3-kinase/AKT pathway.
Cancer Res. 65:11314–11325. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kakiuchi S, Daigo Y, Tsunoda T, Yano S,
Sone S and Nakamura Y: Genome-wide analysis of organ-preferential
metastasis of human small cell lung cancer in mice. Mol Cancer Res.
1:485–499. 2003.PubMed/NCBI
|
|
19
|
Taniwaki M, Daigo Y, Ishikawa N, Takano A,
Tsunoda T, Yasui W, Inai K, Kohno N and Nakamura Y: Gene expression
profiles of small-cell lung cancers: Molecular signatures of lung
cancer. Int J Oncol. 29:567–575. 2006.PubMed/NCBI
|
|
20
|
Oshita H, Nishino R, Takano A, Fujitomo T,
Aragaki M, Kato T, Akiyama H, Tsuchiya E, Kohno N, Nakamura Y and
Daigo Y: RASEF is a novel diagnostic biomarker and a therapeutic
target for lung cancer. Mol Cancer Res. 11:937–951. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hayama S, Daigo Y, Yamabuki T, Hirata D,
Kato T, Miyamoto M, Ito T, Tsuchiya E, Kondo S and Nakamura Y:
Phosphorylation and activation of cell division cycle associated 8
by aurora kinase B plays a significant role in human lung
carcinogenesis. Cancer Res. 67:4113–4122. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ishikawa N, Daigo Y, Takano A, Taniwaki M,
Kato T, Tanaka S, Yasui W, Takeshima Y, Inai K, Nishimura H, et al:
Characterization of SEZ6L2 cell-surface protein as a novel
prognostic marker for lung cancer. Cancer Sci. 97:737–745. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kato T, Sato N, Hayama S, Yamabuki T, Ito
T, Miyamoto M, Kondo S, Nakamura Y and Daigo Y: Activation of
Holliday junction recognizing protein involved in the chromosomal
stability and immortality of cancer cells. Cancer Res.
67:8544–8553. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Suzuki C, Takahashi K, Hayama S, Ishikawa
N, Kato T, Ito T, Tsuchiya E, Nakamura Y and Daigo Y:
Identification of Myc-associated protein with JmjC domain as a
novel therapeutic target oncogene for lung cancer. Mol Cancer Ther.
6:542–551. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Takahashi K, Furukawa C, Takano A,
Ishikawa N, Kato T, Hayama S, Suzuki C, Yasui W, Inai K, Sone S, et
al: The neuromedin U-growth hormone secretagogue receptor
1b/neurotensin receptor 1 oncogenic signaling pathway as a
therapeutic target for lung cancer. Cancer Res. 66:9408–9419. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Taniwaki M, Takano A, Ishikawa N, Yasui W,
Inai K, Nishimura H, Tsuchiya E, Kohno N, Nakamura Y and Daigo Y:
Activation of KIF4A as a prognostic biomarker and therapeutic
target for lung cancer. Clin Cancer Res. 13:6624–6631. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yamabuki T, Takano A, Hayama S, Ishikawa
N, Kato T, Miyamoto M, Ito T, Ito H, Miyagi Y, Nakayama H, et al:
Dikkopf-1 as a novel serologic and prognostic biomarker for lung
and esophageal carcinomas. Cancer Res. 67:2517–2525. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fujitomo T, Daigo Y, Matsuda K, Ueda K and
Nakamura Y: Identification of a nuclear protein, LRRC42, involved
in lung carcinogenesis. Int J Oncol. 45:147–156. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Koinuma J, Akiyama H, Fujita M, Hosokawa
M, Tsuchiya E, Kondo S, Nakamura Y and Daigo Y: Characterization of
an Opa interacting protein 5 involved in lung and esophageal
carcinogenesis. Cancer Sci. 103:577–586. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Nguyen MH, Koinuma J, Ueda K, Ito T,
Tsuchiya E, Nakamura Y and Daigo Y: Phosphorylation and activation
of cell division cycle associated 5 by mitogen-activated protein
kinase play a crucial role in human lung carcinogenesis. Cancer
Res. 70:5337–5347. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hayama S, Daigo Y, Kato T, Ishikawa N,
Yamabuki T, Miyamoto M, Ito T, Tsuchiya E, Kondo S and Nakamura Y:
Activation of CDCA1-KNTC2, members of centromere protein complex,
involved in pulmonary carcinogenesis. Cancer Res. 66:10339–10348.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Takano A, Ishikawa N, Nishino R, Masuda K,
Yasui W, Inai K, Nishimura H, Ito H, Nakayama H, Miyagi Y, et al:
Identification of nectin-4 oncoprotein as a diagnostic and
therapeutic target for lung cancer. Cancer Res. 69:6694–6703. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kobayashi Y, Takano A, Miyagi Y, Tsuchiya
E, Sonoda H, Shimizu T, Okabe H, Tani T, Fujiyama Y and Daigo Y:
Cell division cycle-associated protein 1 overexpression is
essential for the malignant potential of colorectal cancers. Int J
Oncol. 44:69–77. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Thang PM, Takano A, Yoshitake Y, Shinohara
M, Murakami Y and Daigo Y: Cell division cycle associated 1 as a
novel prognostic biomarker and therapeutic target for oral cancer.
Int J Oncol. 49:1385–1393. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Daigo K, Takano A, Thang PM, Yoshitake Y,
Shinohara M, Tohnai I, Murakami Y, Maegawa J and Daigo Y:
Characterization of KIF11 as a novel prognostic biomarker and
therapeutic target for oral cancer. Int J Oncol. 52:155–165.
2018.PubMed/NCBI
|
|
36
|
Nakamura M, Takano A, Thang PM, Tsevegjav
B, Zhu M, Yokose T, Yamashita T, Miyagi Y and Daigo Y:
Characterization of KIF20A as a prognostic biomarker and
therapeutic target for different subtypes of breast cancer. Int J
Oncol. 57:277–288. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Williams JM, Chen GC, Zhu L and Rest RF:
Using the yeast two-hybrid system to identify human epithelial cell
proteins that bind gonococcal Opa proteins: Intracellular gonococci
bind pyruvate kinase via their Opa proteins and require host
pyruvate for growth. Mol Microbiol. 27:171–186. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Stellfox ME, Nardi IK, Knippler CM and
Foltz DR: Differential binding partners of the Mis18α/β YIPPEE
domains regulate mis18 complex recruitment to centromeres. Cell
Rep. 15:2127–2135. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Nardi IK, Zasadzińska E, Stellfox ME,
Knippler CM and Foltz DR: Licensing of centromeric chromatin
assembly through the mis18α-mis18β heterotetramer. Mol Cell.
61:774–787. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Fujita Y, Hayashi T, Kiyomitsu T, Toyoda
Y, Kokubu A, Obuse C and Yanagida M: Priming of centromere for
CENP-A recruitment by human hMis18alpha, hMis18beta, and M18BP1.
Dev Cell. 12:17–30. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Wang J, Liu X, Dou Z, Chen L, Jiang H, Fu
C, Fu G, Liu D, Zhang J, Zhu T, et al: Mitotic regulator Mis18β
interacts with and specifies the centromeric assembly of molecular
chaperone holliday junction recognition protein (HJURP). J Biol
Chem. 289:8326–8336. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
He X, Hou J, Ping J, Wen D and He J: Opa
interacting protein 5 acts as an oncogene in bladder cancer. J
Cancer Res Clin Oncol. 143:2221–2233. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Nakamura Y, Tanaka F, Nagahara H, Ieta K,
Haraguchi N, Mimori K, Sasaki A, Inoue H, Yanaga K and Mori M: Opa
interacting protein 5 (OIP5) is a novel cancer-testis specific gene
in gastric cancer. Ann Surg Oncol. 14:885–892. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
He J, Zhao Y, Zhao E, Wang X, Dong Z, Chen
Y, Yang L and Cui H: Cancer-testis specific gene OIP5: A downstream
gene of E2F1 that promotes tumorigenesis and metastasis in
glioblastoma by stabilizing E2F1 signaling. Neuro Oncol.
20:1173–1184. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2-ΔΔCq method. Methods. 25:402–408. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Chinn SB and Myers JN: Oral cavity
carcinoma: Current management, controversies, and future
directions. J Clin Oncol. 33:3269–3276. 2015. View Article : Google Scholar : PubMed/NCBI
|