Introduction
Rectal cancer is one of the most common types of
cancer in Japan and other developed nations. The introduction of
preoperative chemoradiotherapy (CRT) and total mesorectal excision
(TME) for the management of locally advanced rectal cancer has
decreased local recurrence rates and increased patient survival
(1–3). However, disease recurrence remains
the major cause of mortality in rectal cancer patients.
Identification of predictors for disease recurrence and poor
prognosis would aid in the successful treatment of these patients.
Predictive pathological and molecular biomarkers for revelaing the
prognosis for patients with rectal cancer following preoperative
CRT have been reported (4,5). Several studies have shown that the
tumor regression grade (TRG) or a pathological response following
preoperative CRT are predictors of clinical outcomes (6–9).
Moreover, the apoptotic and proliferative status has been reported
to be associated with tumor recurrence and poor prognosis (10,11).
Radiotherapy is an effective tool for local control that functions
by inducing cancer cell apoptosis and death and inhibiting cell
growth in various malignancies.
The anti-M30 monoclonal antibody reacts with a
caspase-cleaved product of keratin 18, a type I intermediate
filament protein and major component of single-layer and glandular
epithelial cells, which only detects apoptotic events in tumor or
normal epithelial cells (12).
Although terminal deoxyribonucleotidyl transferase dUTP nick
end-labeling (TUNEL) is a common method used for the detection of
DNA fragmentation resulting from the apoptotic signaling cascade it
has also been used to evaluate apoptotic cell death, the anti-M30
antibody is considered to be a promising alternative to the TUNEL
assay for the detection of apoptotic cells (13). Previous studies have shown that the
apoptotic status of cancer cells following CRT using M30
immunohistochemistry was not associated with local recurrence and
prognosis, although the level of apoptosis in primary tumors
without pretreatment predicted a high risk of local recurrence and
a poor prognosis for rectal cancer patients (10,14–16).
The studies mentioned previously have suggested that the
predisposition to intrinsic apoptosis prior to CRT was more
important than therapy-induced apoptosis for local recurrence and
prognosis. However, we hypothesized that therapy-induced apoptosis
is not present at the time of evaluation due to the interval
between CRT and surgery, and that the residual cancer cells possess
intrinsic or spontaneous apoptotic potential.
The aim of this retrospective study was to evaluate
residual rectal cancer cells following preoperative CRT by M30
immuno staining, in addition to investigating the correlation of
M30 expression with clinical outcomes and the expression of
apoptotic and proliferative markers.
Materials and methods
Patients and specimens
From 2001 to 2011, 77 patients with rectal cancer
received preoperative CRT followed by surgery at Mie University
Hospital (Mie, Japan). The criteria used for the induction of
preoperative CRT were that patients were required to i) be ≤80
years of age; ii) be diagnosed as clinical stage II/III based on
the International Union Against Cancer TNM classification, with no
evidence of distant metastases; iii) exhibit no invasion of the
external sphincter muscle or elevator muscle of the anus; and iv)
show no evidence of deep venous thrombosis. In total five patients
exhibited a complete pathological response and were excluded from
participation in this study. The study design was approved by Mie
University Hospital’s Ethics review board. All patients signed
informed consent forms to allow for the use of their tissues in
this study.
5-Fluorouracil (5-FU)-based CRT
regimen
Patients with rectal cancer were treated with
short-course (a dose of 20 Gy in 4 fractions) or long-course (a
dose of 45 Gy in 25 fractions) of radiotherapy using the 4-field
box technique with concurrent chemotherapy to take advantage of
5-FU radiosensitization. Patients underwent concurrent
pharmacokinetic modulation chemotherapy [5-FU administered by
intravenous infusion: 600 mg/m2 for 24 h, and
tegafur-uracil (UFT) administered orally: 400 mg/m2 for
5 days] (17). Short-course
radiotherapy at the Mie University Hospital is different from
standard short-course radiotherapy, which consists of a dose of 25
Gy in 5 fractions. The present regimen was designed as described
previously for several reasons: a biologically equivalent dose
(BED) of 20 Gy in 4 fractions was calculated using a linear
quadratic model, and its BED was 30 Gy (α/β ratio, 10 Gy), which
had sufficient efficacy in reducing the local failure of
radiotherapy (18). Furthermore,
the reduction of postoperative complications, such as ileitis
induced by preoperative radiotherapy, were considered. In total 50
patients received short-course radiotherapy with chemotherapy over
1 week. The remaining 22 patients received long-course radiotherapy
with chemotherapy for 4 weeks. The time interval between
preoperative CRT and surgery was 2–3 weeks for short-course and 4–6
weeks for long-course irradiation patients. The patients underwent
standard surgery, including TME, and received 5-FU-based adjuvant
chemotherapy following surgery for between 6 months to 1 year.
Clinical and pathological response to
CRT
The clinical response following preoperative CRT was
evaluated by a barium enema, endoscopy, computed tomography and
magnetic resonance imaging. The clinical response was subsequently
graded as a complete response, a partial response, no change or
progressive disease. The TRG was evaluated using the 3-point Ryan
TRG system (19). The 3-point Ryan
system combines TRG1 (no viable cancer cells) and TRG2 (single
cells or small groups of cancer cells) to form one category:
3-point TRG1. TRG3 (residual cancer outgrown by fibrosis) forms the
3-point TRG2, and TRG4 (significant fibrosis outgrown by cancer)
and TRG5 (no fibrosis with extensive residual cancer) are combined
in order to form the 3-point TRG3.
Immunohistochemistry for M30, Bax, Bcl-2,
Ki67 and PCNA
Immunohistochemistry was performed as described
previously (20). Anti-M30
CytoDeath (mouse monoclonal antibody, clone M30; dilution 1:100;
Peviva AB, Bromma, Sweden), polyclonal rabbit anti-human Bax (code
A3533; dilution 1:2000; DakoCytomation, Carpinteria, CA, USA),
monoclonal mouse anti-human Bcl-2 oncoprotein (clone 124; dilution
1:100; DakoCytomation), monoclonal mouse anti-human Ki-67 antigen
(clone MIB-1; used as supplied; DakoCytomation), monoclonal mouse
anti-proliferating cell nuclear antigen (PCNA; clone PC10; dilution
1:200; DakoCytomation) antibodies were used as primary antibodies.
Negative controls were run simultaneously. M30 positivity was
identified as brown cytoplasmic staining.
Immunohistochemical evaluation of
M30
The number of cytoplasmic M30 positive cells in
residual cancer cells per five fields at a magnification of ×100
was counted under a light microscope (BX50, Olympus, Tokyo, Japan).
Each sample was evaluated in a blinded manner by two investigators
who had no clinical or pathological information regarding the
origin of the samples.
Quantitative polymerase chain reaction
(qPCR)
Microdissection of FFPE, cDNA synthesis, and qPCR
were performed as described previously (20). Primers for BAX, BCL2,
MKI67, PCNA, GAPDH and ACTB (β-actin)
were designed with Primer3 software (Biology Workbench Version 3.2;
San Diego Super Computer Center, University of California, San
Diego, CA, USA). The sequences used were as follows:
BAX-specific primers, sense: CTTTGCCAGCAAAC TGGTG,
antisense: CAGCCCATGATGGTTCTGA; BCL2-specific primers,
sense: TCGCCCTGTGGATGACTGA, antisense: CAGAGACAG C CAG GAGA A AT CA
A; MKI67-specific primers, sense: TGAGCCTGTACGGCTAAA ACA,
antisense: TTGACTTCCTTCCATTCTGAAG; PCNA-specific primers,
sense: GAAGCACCAAACCAGGA GAA, antisense: TATCGGCATATACGTGCAAA;
GAPDH, sense: GGAAGGTGAAGGTCGGAGTC, antisense:
AATGAAGGGGTCATTCATGG; and ACTB, sense: ACAGAGCCTCGCCTTTGC,
antisense: GCGGCGATAT CATCATCC. Relative mRNA levels were
determined by the standard curve method. Standard curves and line
equations were generated using 5-fold serially diluted solutions of
cDNA from the colon cancer cell line, Lovo or Human Reference Total
RNA (Clontech Laboratories, Inc., Mountain View, CA, USA). Target
gene expression was calculated using the standard curve and
quantitative normalization of cDNA in each sample was performed
using the expression of the ACTB gene as an internal
control.
Statistical analyses
Statistical analyses were performed using Stat View
5.0 for Windows (SAS Institute Inc., Cary, NC, USA). The values of
each target gene are expressed as the median values in tables.
Significant differences were analyzed using the Chi-square test.
The associations between continuous and categorical variables were
evaluated using the Mann-Whitney U test for the two groups.
Recurrence-free survival (RFS) and overall survival (OS) times were
calculated from the date of surgery to the date of disease
recurrence or patient death, respectively. RFS and OS probabilities
were calculated using the Kaplan-Meier product limit method, and
intergroup differences were determined using a log-rank test.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Patient and tumor characteristics
The median age of the study subjects was 64 years
(range, 35–77 years) and the male:female ratio was 5:2 (Table I). Post-CRT pathological T stages
were ypT0 (n=1), pT1 (n=7), ypT2 (n=19), ypT3 (n=43) and ypT4 (n=2)
(Table I). In total, 25 patients
(35%) presented with lymph node metastases. Sixty-three tumors
(88%) had well- or moderately differentiated adenocarcinoma
histology. Local recurrence alone was exhibited in 4 patients
(5.5%), while 15 patients (20.8%) had distant recurrence. Patterns
of distant recurrence were observed as both liver and lung
metastases in 2 patients, lung metastasis alone in 9 patients,
liver metastasis alone in 1 patient and peritoneal metastasis in 2
patients. The median follow-up period was 62 months (range, 9–147
months).
 | Table I.Patient characteristics and the
correlation of M30 staining with clinicopathological variables. |
Table I.
Patient characteristics and the
correlation of M30 staining with clinicopathological variables.
| Variables | No. (%) | M30-negative
(n=38) | M30-positive
(n=34) | P-value |
|---|
| Gender | | | | |
| Male | 54 (75) | 29 | 25 | 0.785 |
| Female | 18 (25) | 9 | 9 | |
| Age (median; 64) | | | | |
| <64 | 36 (50) | 21 | 15 | 0.345 |
| ≥64 | 36 (50) | 17 | 19 | |
| ypT
classification | | | | |
| 1/2 | 27 (38) | 10 | 17 | 0.038 |
| 3/4 | 45 (62) | 28 | 17 | |
| ypN
classification | | | | |
| Absent | 47 (65) | 21 | 26 | 0.059 |
| Present | 25 (35) | 17 | 8 | |
| Postoperative
stage | | | | |
| I/II | 44 (61) | 18 | 26 | 0.011 |
| III/IV | 28 (39) | 20 | 8 | |
| Lymphatic
invasion | | | | |
| Absent | 18 (25) | 9 | 9 | 0.785 |
| Present | 54 (75) | 29 | 25 | |
| Vascular
invasion | | | | |
| Absent | 36 (50) | 15 | 21 | 0.059 |
| Present | 36 (50) | 23 | 13 | |
| Histology | | | | |
| Well/moderate | 63 (88) | 32 | 31 | 0.372 |
|
Poor/signet/mucinous | 9 (12) | 6 | 3 | |
| TRG | | | | |
| Grade 1 | 16 (23) | 7 | 9 | 0.684 |
| Grade 2 | 37 (51) | 21 | 16 | |
| Grade 3 | 19 (26) | 10 | 9 | |
| Radiotherapy | | | | |
| Short (20 Gy/4
fractions) | 50 (69) | 25 | 25 | 0.477 |
| Long (45 Gy/25
fractions) | 22 (31) | 13 | 9 | |
| Recurrence | | | | |
| Absent | 53 (74) | 24 | 29 | 0.030 |
| Present | 19 (26) | 14 | 5 | |
Correlation between M30 staining and
clinicopathological variables
There were 34 patients (47%) with M30 staining
(range of percentage of M30-positive cancer cells, 0–32%). The mean
percentage of cancer cells with M30 staining was particularly low,
2.93%. Therefore, patients were divided into two groups according
to M30 positivity. Table I shows
the correlation of M30 staining with clinicopathological variables.
Patients without M30 staining of residual rectal cancer following
CRT more frequently had advanced ypT classification, advanced
postoperative stage, and tumor recurrence (P=0.038, 0.011 and
0.030, respectively). M30 positivity was correlated with lymph node
metastasis and vascular invasion, despite the lack of significant
differences (P=0.059 and 0.059, respectively). We observed no
correlation between M30 staining and other clinicopathological
findings, including TRG.
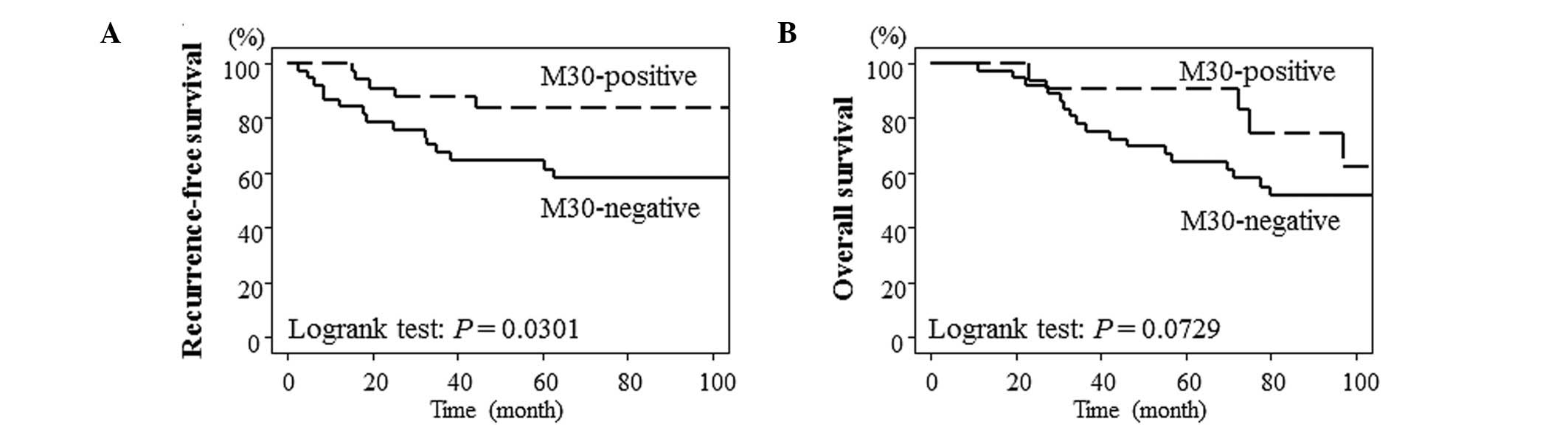
Lack of M30 staining was associated with
poor RFS
Fig. 1 shows the
survival curve for RFS and OS according to M30 positivity using the
Kaplan-Meier method. Lack of M30 staining was significantly
associated with poorer RFS (P=0.0301). Furthermore, there was a
tendency to have an improved prognosis in patients with positive
positive M30 staining compared with patients lacking M30 staining
(P=0.0729).
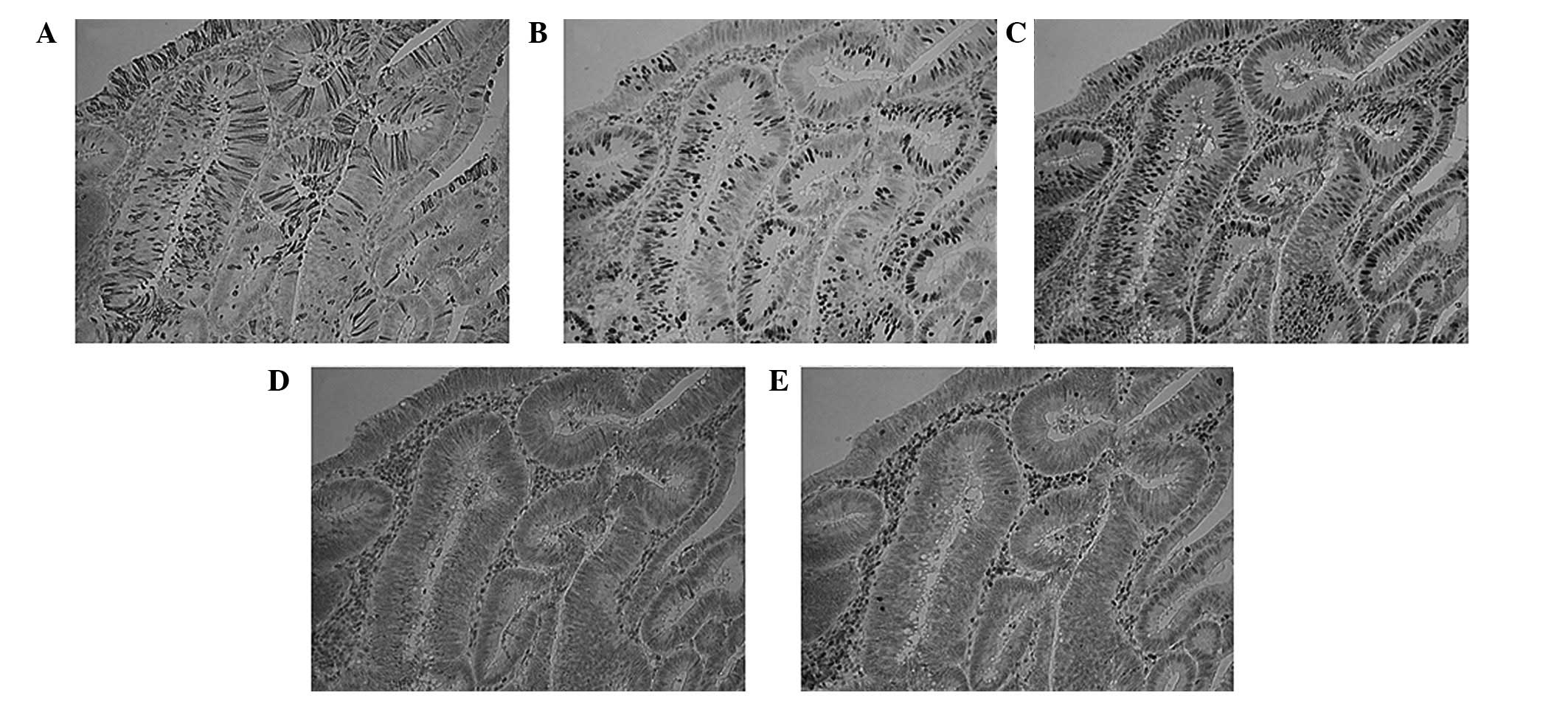
Immunohistochemical findings for M30,
Bax, Bcl-2, Ki67 and PCNA
The expression of apoptotic markers, Bax and Bcl-2,
and proliferative markers, Ki67 and PCNA were examined, in cases
with high M30 expression. Residual cancer cells with M30 staining
lacked Ki67 and PCNA expression. However, there was no correlation
between M30 staining and apoptotic markers (Fig. 2).
Correlation of M30 staining with BAX,
BCL2, MKI67 and PCNA expression
In the transcriptional analysis, there was no
correlation between M30 staining and the expression of BAX,
BCL2, MKI67 or PCNA (Table II).
| Table II.Expression of M30 and proliferative
and apoptotic markers. |
Table II.
Expression of M30 and proliferative
and apoptotic markers.
| Gene | M30-positive
(n=21) | M30-negative
(n=29) | P-value |
|---|
| BAX | 0.807 | 0.743 | 0.7161 |
| BCL2 |
1.13×10−4 | 0.000 | 0.3247 |
| PCNA | 0.018 | 0.022 | 0.7854 |
| MKI67 |
14.4×10−6 |
3.8×10−6 | 0.8483 |
Discussion
In this study, the immunohistochemical evaluation of
M30 for apoptotic status correlated with low T stage and tumor
recurrence in patients with locally advanced rectal cancer
subsequent to preoperative CRT. Furthermore, we observed that
patients with M30 staining demonstrated improved RFS. The results
of this study are different to those of other studies in that the
apoptotic status following preoperative CRT was not associated with
tumor recurrence or a poor prognosis (10,14–16).
One reason for this discrepancy is that the analyses performed in
the present study utilized M30 positivity compared with previous
studies which divided groups by the mean of median values of
M30-positive cells. Adell et al (21) demonstrated that the mean percentage
of apoptotic cells was 1.1% (0–14.5%) in rectal cancer following
preoperative radiotherapy using the TUNEL method. Koornstra et
al (22) reported that the
mean percentage of cancer cells with M30 staining was ∼2% in
primary colorectal cancer. The results of those studies suggested
that there were a small number of apoptotic cancer cells in primary
and pretreated rectal cancer. In this study, the mean percentage of
cancer cells with M30 staining was 2.93%. Therefore, we divided the
patients into two groups according to M30 positivity. Results
obtained from the pathological response demonstrated no significant
correlation between M30 staining and TRG. This may have been due to
the fact that TRG is determined by quantifying the proportion of
residual cancer cells relative to the stroma with fibrosis and
vasculopathy of the entire tumor bed, and does not reflect
therapy-induced apoptosis of residual cancer cells. Furthermore,
M30 is expressed during early apoptosis except for
caspase-independent apoptosis and mitotic catastrophe (12). In this study, M30 expression likely
represents spontaneous apoptosis rather than therapy-induced
apoptosis due to the time intervals between preoperative CRT and
surgery, and cancer cells induced by apoptosis are replaced by
fibrosis. However, de Bruin et al (14) reported that M30-positive cells were
increased by radiotherapy, suggesting that radiotherapy induced
apoptosis.
We also investigated whether there was any
correlation between the apoptotic status evaluated by M30 and the
expression of apoptotic and proliferative markers. In the
transcriptional analysis, we observed no significant correlation
between M30 staining and the gene expression of BAX, BCL2
MKI67 and PCNA. However, the gene expression of
MKI67, PCNA and BCL2 correlated with the
pathological response following CRT (data not shown). This suggests
that TRG reflects the proliferative activity of residual cancer
cells following CRT. Results of the immuno histochemical evaluation
of M30, Bax, Bcl-2, Ki67 and PCNA revealed that M30-positive cells
lacked Ki67 expression. The Ki67 protein is present during all
active phases of the cell cycle, with the exception of the G0
phase. This finding confirmed that M30 staining detected cell
death. By contrast, the expression of Bax, Bcl-2, and PCNA did not
correlate with M30 staining. Bcl-2 and Bax regulate caspase
activation. Bcl-2 is an important inhibitor of apoptosis, while the
overexpression of Bax induces apoptosis (23). The M30 cytodeath antibody
recognizes a neo-epitope formed following the caspase cleavage of
keratin 18 and detects apoptosis of an epithelial origin.
Therefore, the difference in apoptotic status determined between
M30 and these apoptotic markers may result in no significant
correlation between M30 and the apoptotic markers.
In conclusion, the evaluation of M30 expression is
useful in the prediction of tumor recurrence in rectal cancer
patients treated with preoperative CRT, although it is unknown as
to whether the apoptosis detected by M30 staining was intrinsic or
induced by therapy. However, the data in this study should be
interpreted with caution. A significant limitation of this study
was the small number of patients studied (n=72), particularly those
with recurrence (n=19), and the retrospective nature of the study.
This study also included two neoadjuvant radiation regimens with
different time intervals between pretreatment and surgery.
Furthermore, our short-course regimen deviated from the standard
method. Therefore, a larger study population, long-term follow-up
and unification of pretreatments are required in order to validate
the results.
Acknowledgements
The authors would like to thank Motoko
Ueeda, Yuka Kato and Chihiro Hibi for providing excellent technical
assistance.
References
|
1.
|
Sauer R, Becker H, Hohenberger W, et al:
Preoperative versus postoperative chemoradiotherapy for rectal
cancer. N Engl J Med. 351:1731–1740. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
van den Brink M, Stiggelbout AM, van den
Hout WB, et al: Clinical nature and prognosis of locally recurrent
rectal cancer after total mesorectal excision with or without
preoperative radiotherapy. J Clin Oncol. 22:3958–3964.
2004.PubMed/NCBI
|
|
3.
|
Guillem JG, Chessin DB, Cohen AM, et al:
Long-term oncologic outcome following preoperative combined
modality therapy and total mesorectal excision of locally advanced
rectal cancer. Ann Surg. 241:829–838. 2005. View Article : Google Scholar
|
|
4.
|
Smith FM, Reynolds JV, Miller N, et al:
Pathological and molecular predictors of the response of rectal
cancer to neoadjuvant radiochemotherapy. Eur J Surg Oncol.
32:55–64. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Bertolini F, Bengala C, Losi L, et al:
Prognostic and predictive value of baseline and posttreatment
molecular marker expression in locally advanced rectal cancer
treated with neoadjuvant chemoradiotherapy. Int J Radiat Oncol Biol
Phys. 68:1455–1461. 2007. View Article : Google Scholar
|
|
6.
|
Rodel C, Martus P, Papadoupolos T, et al:
Prognostic significance of tumor regression after preoperative
chemoradiotherapy for rectal cancer. J Clin Oncol. 23:8688–8696.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Bujko K, Michalski W, Kepka L, et al:
Association between pathologic response in metastatic lymph nodes
after preoperative chemoradiotherapy and risk of distant metastases
in rectal cancer: an analysis of outcomes in a randomized trial.
Int J Radiat Oncol Biol Phys. 67:369–377. 2007. View Article : Google Scholar
|
|
8.
|
Dhadda AS, Dickinson P, Zaitoun AM, et al:
Prognostic importance of Mandard tumour regression grade following
pre-operative chemo/radiotherapy for locally advanced rectal
cancer. Eur J Cancer. 47:1138–1145. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Topova L, Hellmich G, Puffer E, et al:
Prognostic value of tumor response to neoadjuvant therapy in rectal
carcinoma. Dis Colon Rectum. 54:401–411. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Tannapfel A, Nusslein S, Fietkau R, et al:
Apoptosis, proliferation, bax, bcl-2 and p53 status prior to and
after preoperative radiochemotherapy for locally advanced rectal
cancer. Int J Radiat Oncol Biol Phys. 41:585–591. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Rupa JD, de Bruine AP, Gerbers AJ, et al:
Simultaneous detection of apoptosis and proliferation in colorectal
carcinoma by multiparameter flow cytometry allows separation of
high and low-turnover tumors with distinct clinical outcome.
Cancer. 97:2404–2411. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Leers MP, Kolgen W, Bjorklund V, et al:
Immunocytochemical detection and mapping of a cytokeratin 18
neo-epitope exposed during early apoptosis. J Pathol. 187:567–572.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Caulin C, Salvesen GS and Oshima RG:
Caspase cleavage of keratin 18 and reorganization of intermediate
filaments during epithelial cell apoptosis. J Cell Biol.
138:1379–1394. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
de Bruin EC, van de Velde CJ, van de Pas
S, et al: Prognostic value of apoptosis in rectal cancer patients
of the Dutch total mesorectal excision trial: radiotherapy is
redundant in intrinsically high-apoptotic tumors. Clin Cancer Res.
12:6432–6436. 2006.PubMed/NCBI
|
|
15.
|
de Heer P, Gosens MJ, de Bruin EC, et al:
Cyclooxygenase 2 expression in rectal cancer is of prognostic
significance in patients receiving preoperative radiotherapy. Clin
Cancer Res. 13:2955–2960. 2007.PubMed/NCBI
|
|
16.
|
Gosens MJ, Dresen RC, Rutten HJ, et al:
Preoperative radiochemotherapy is successful also in patients with
locally advanced rectal cancer who have intrinsically high
apoptotic tumours. Ann Oncol. 19:2026–2032. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Yoshikawa R, Kusunoki M, Yanagi H, et al:
Dual antitumor effects of 5-fluorouracil on the cell cycle in
colorectal carcinoma cells: a novel target mechanism concept for
pharmacokinetic modulating chemotherapy. Cancer Res. 61:1029–1037.
2001.
|
|
18.
|
Colorectal Cancer Collaborative Group:
Adjuvant radiotherapy for rectal cancer: a systematic overview of
8,507 patients from 22 randomised trials. Lancet. 358:1291–1304.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Ryan R, Gibbons D, Hyland JM, et al:
Pathological response following long-course neoadjuvant
chemoradiotherapy for locally advanced rectal cancer.
Histopathology. 47:141–146. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Saigusa S, Tanaka K, Toiyama Y, et al:
Correlation of CD133, OCT4, and SOX2 in rectal cancer and their
association with distant recurrence after chemoradiotherapy. Ann
Surg Oncol. 16:3488–3498. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Adell GC, Zhang H, Evertsson S, et al:
Apoptosis in rectal carcinoma: prognosis and recurrence after
preoperative radiotherapy. Cancer. 91:1870–1875. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Koornstra JJ, Rijcken FE, De Jong S, et
al: Assessment of apoptosis by M30 immunoreactivity and the
correlation with morphological criteria in normal colorectal
mucosa, adenomas and carcinomas. Histopathology. 44:9–17. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Reed JC: Double identity for proteins of
the Bcl-2 family. Nature. 387:773–776. 1997. View Article : Google Scholar : PubMed/NCBI
|