Introduction
The incidence and mortality of thyroid cancer are
increasing worldwide. Differentiated thyroid cancer (DTC), namely
papillary thyroid carcinoma (PTC) and follicular thyroid carcinoma
(FTC), comprise ∼94% of these cases (1). Despite the majority of the DTC
patients having indolent disease, ∼5–10% of these patients will
eventually develop metastatic disease, no longer responding to
radioiodine (RAI) therapy or thyroid-stimulating hormone (TSH)
suppression and exhibiting a more aggressive course and short
survival (2–4). Doxorubicin is the only currently
available treatment option that has been approved by the Food and
Drug Administration (FDA) for such patients, with a
progression-free survival (PFS) of only 2 months and a median
overall survival (OS) of 8 months; however, it is accompanied by
severe myelosuppression and cumulative cardiotoxicity (5). Therefore, RAI-refractory DTC is a
disease requiring novel therapeutic options exhibiting better
efficacy and less toxicity.
Activating mutations in certain genes were
previously reported to play a critical role in the development of
DTC and the majority of DTCs may be due to single activating
somatic mutations in one of three genes: BRAF mutations, RET/PTC
rearrangements and Ras mutations (6–9).
Sorafenib is a small-molecule multikinase inhibitor that targets
several molecular signals which have been proven as potential
therapeutic targets in DTC. Four phase II trials using sorafenib
for metastatic thyroid cancer were recently published (10–13)
and the promising preliminary results of those studies prompted the
off-label use of commercially available sorafenib in patients with
metastatic DTC refractory to RAI and TSH suppression. This study
aimed to assess the clinical efficacy and safety of sorafenib
treatment in Chinese patients with thyroid cancer.
Patients and methods
Patient details
The patients with metastatic DTC treated with
sorafenib between January, 2011 and June, 2012 were entered into a
retrospective database. Adult patients had histologically proven
PTC or FTC and RAI-refractory disease, defined as a cumulative RAI
dose of ≥600 mCi or no-iodine uptake on a post-radioactive iodine
scan. All patients had evidence of progressive disease (PD) within
3 months prior to the initiation of sorafenib under adequate TSH
suppression (<0.5 mU/l). Patients who were treated with
single-agent sorafenib and at least one follow-up imaging study to
assess response after 2 months of therapy were included in this
series.
Sorafenib treatment
Patients were treated with 400 mg sorafenib (BAY
43–9006; Bayer HealthCare Pharmaceuticals, Montville, NJ, USA),
administered orally twice a day. Dose reductions and treatment
interruptions were allowed due to toxicity. All patients but one
were administered sorafenib until PD or intolerable toxicity.
Study endpoints and evaluation of
efficacy
The primary endpoints were the determination of
response and PFS. The secondary study endpoints included adverse
events (AEs), OS and the correlation between radiographical
response and tumor marker response.
Computed tomography scans were performed prior to
and every 2–3 months following treatment. The evaluation of
efficacy used Response Evaluation Criteria In Solid Tumors, version
1.0. The target lesions (TLs) were defined as those that could be
accurately measured in at least one dimension, with a longest
diameter of ≥1 cm. A durable response was defined as partial
response (PR) and stable disease (SD) lasting >6 months. The PFS
was defined as the time from the initiation of sorafenib
administration to disease progression or death. The OS was defined
as the time from the initiation of sorafenib to the time of death
from any cause or the last follow-up.
Tumor marker evaluation
Serum thyroglobulin (TG) levels were measured at the
baseline and at the same time, corresponding to each radiographic
assessment, in all patients. A tumor marker complete response (CR)
was defined as a decline to the normal range (including the normal
range at baseline). A tumor marker PR was defined as a >25%
decline from baseline, but to levels higher than the upper limit of
the normal range. PD was defined as a >25% increase from
baseline. SD was defined as any response between PR and PD.
Safety profile
Hematological and non-hematological toxicities
associated with sorafenib were classified according to the revised
National Cancer Institute Common Toxicity Criteria for Adverse
Events, version 4.0.
Statistical methods
SPSS software, version 11.5 (SPSS Inc., Chicago, IL,
USA) was used for statistical analysis. The Kaplan-Meier method was
used to estimate the median PFS, the median OS and the 1- and
2-year survival rates. The comparisons between groups with
different tumor marker responses were performed with the log-rank
test. The χ2 test was used to assess the correlation
between tumor marker response and radiographic efficacy. The
response in different organs was compared using the
two-independent-samples test.
Results
Clinical characteristics
A total of 8 patients were included in this series.
The median patient age was 55 years (range, 43–67 years) and 62.5%
of the patients were female. Seven of the patients (87.5%) had a
diagnosis of PTC and 1 patient (12.5%) presented with FTC. The lung
parenchyma was the most common metastatic location (87.5%),
followed by the lymph nodes (neck, mediastinal, hilar and inguinal
nodes) (62.5%), bone (37.5%), soft tissue (37.5%), renal parenchyma
(12.5%) and trachea (12.5%). All patients presented with >1
location of metastatic disease. Seven patients received >600 mCi
of RAI (range, 620–1,820 mCi) and 1 patient had TLs with no
iodine-uptake on a post-RAI scan performed under conditions of a
low iodine diet and adequate TSH elevation; thus, all patients were
considered to have refractory disease. There was a significant
difference in the TG baseline levels among the patients (range,
0.9->29,997.0 ng/ml).
Response and survival
PR was achieved in 4 of the 8 patients (50.0%)
within the first 6 months of treatment; SD was observed in 3
(37.5%) and PD in 1 patient (12.5%), which consisted of the
development of new lymph node lesions. No patients achieved a CR. A
durable response was observed in 5 of the 8 patients (62.5%). At
the time of data analysis, the cumulative number of patients with
PD was 4 (50.0%) and they all succumbed to the disease. Of note, 1
patient with PTC had a visible nodule on their neck that had
decreased in size by 32.6% at 4 weeks and had a PR verified by CT
at 8 weeks; however, the patient underwent a dose reduction to 400
mg/day due to palmar-plantar erythrodysesthesia at 12 weeks,
developed PD 4 months later and eventually succumbed to the disease
(Fig. 1). Another female patient
had achieved a PR at 6 months; however, the sorafenib dose was
decreased to 200 mg/day due to grade 4 hypocalcemia, the patient
experienced disease progression 3 months later and succumbed to the
disease shortly thereafter.
The median PFS was 40.1 weeks, with 1- and 2-year
PFS rates of 49.6%. The median OS was 55.0 weeks. The 1- and 2-year
survival rates were 85.7 and 42.9%, respectively.
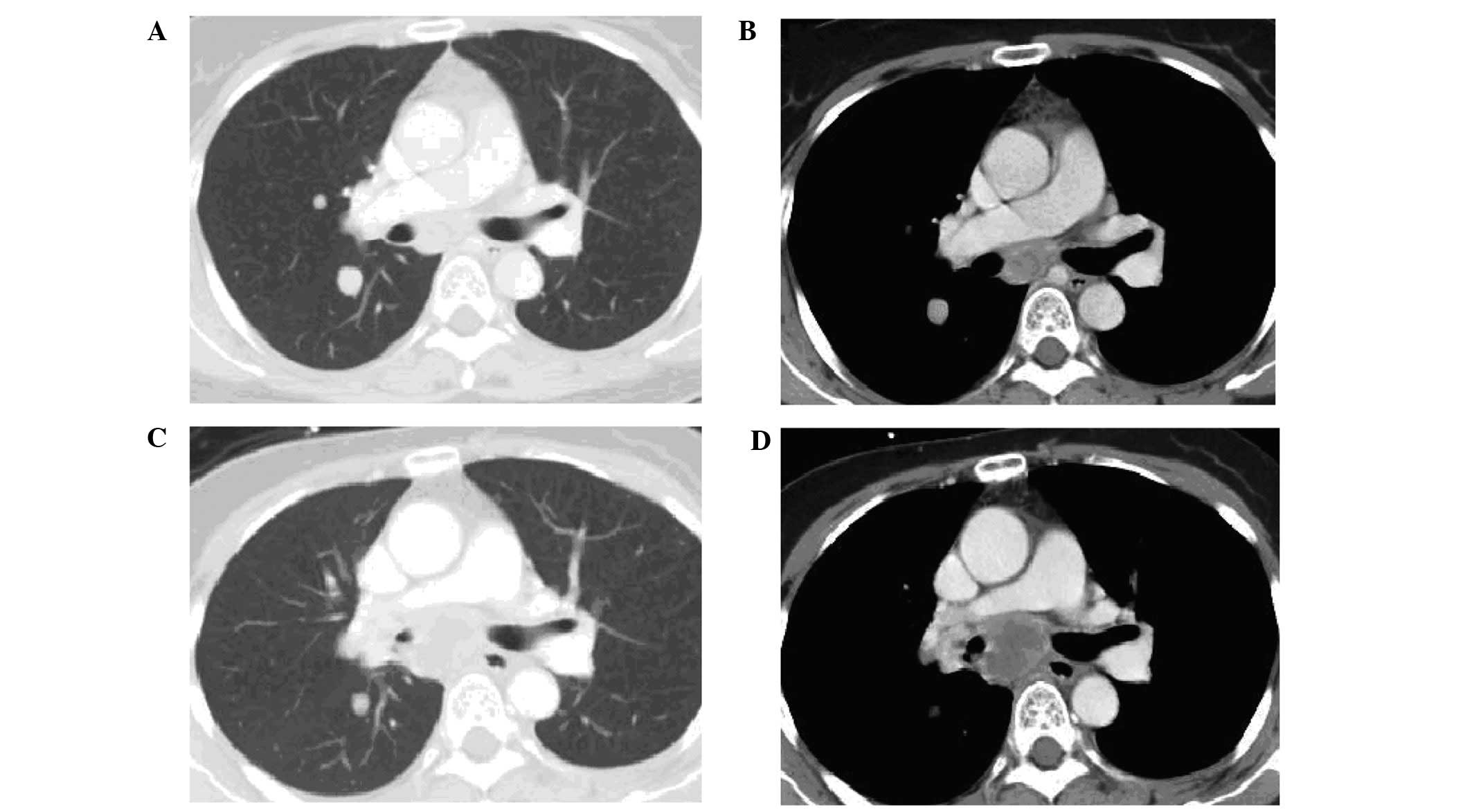
Response by organ site
The response of TLs by organ site was assessed and
the TLs of the lungs (median change, −30.7%; range, −67 to 0%) were
shown to be more sensitive compared to those of the lymph nodes
(median change, 6.3%; range, −42 to 44%) (Wilcoxon rank-sum test
P=0.009). Tumor regression in response to sorafenib may be observed
in the lungs with simultaneous progression in the lymph nodes in
the same patient (Fig. 2).
Tumor marker response
The tumor marker response was assessed in all
patients. CR was oserved in 4 of the 8 patients (50.0%), including
2 patients with TG levels within the normal range at baseline; PR
was observed in 2 patients (25.0%) and SD in the remaining 2
patients (25.0%). The overall median PFS was not reached in the
patients with tumor marker CR, although their PFS was significantly
longer compared to that of the patients with tumor marker PR or SD
(26.1 weeks, χ2=6.834, P=0.009). There was no
significant correlation between tumor marker response with
radiological response using the Pearson’s coefficient test
(χ2=0.000, P=1.000).
Treatment tolerability and AEs
The median duration of the treatment was 3–25
months. The treatment was discontinued in 4 patients (2 patients
had PD, 1 patient was administered radiotherapy due to severe pain
attributed to iliac bone metastasis and soft tissue invasion and 1
patient could no longer afford the cost of the treatment after 3
months). Five patients (62.5%) underwent a reduction in the dose of
sorafenib due to AEs (2 patients required a dose reduction by one
dose level to 600 mg/day, 1 patient underwent a further reduction
to 400 mg/day and another 2 patients to the lowest dose level of
200 mg/day). The median time to dose reduction for all toxicities
was 56 days (range, 20–82 days). The toxicities are summarized in
Table I. Hematological toxicities
were uncommon and of low degree. In terms of non-hematological
toxicities, palmar-plantar erythrodysesthesia was the most common
AE and over half of the patients complained of alopecia,
hypertension, diarrhea, fatigue and weight loss. Electrolyte
abnormalities were uncommon, although 1 patient experienced grade 4
hypocalcemia despite daily calcium injections. The only grade 4
gastrointestinal toxicity observed was an elevation in amylase
levels, which subsided following a dose reduction.
 | Table I.Treatment-related adverse events
according to the Common Toxicity Criteria for Adverse Events
(version 4.0). |
Table I.
Treatment-related adverse events
according to the Common Toxicity Criteria for Adverse Events
(version 4.0).
| Event | Grade 1
| Grade 2
| Grade 3
| Grade 4
|
|---|
| Patient no. | % | Patient no. | % | Patient no. | % | Patient no. | % |
|---|
| Blood and lymphatic
system disorders | | | | | | | | |
| Anemia | 2 | 25.0 | - | - | - | - | - | - |
| Cardiovascular
acute coronary syndrome | - | - | 1 | 12.5 | - | - | - | - |
| Eye disorders | | | | | | | | |
| Blurred vision | 1 | 12.5 | - | - | - | - | - | - |
| Gastrointestinal
disorders | | | | | | | | |
| Diarrhea | 3 | 37.5 | 1 | 12.5 | - | - | - | - |
| Nausea | 3 | 37.5 | - | - | - | - | - | - |
| Oral mucositis | - | - | 1 | 12.5 | - | - | - | - |
| General disorders and
administration site conditions | | | | | | | | |
| Fatigue | 3 | 37.5 | 1 | 12.5 | - | - | - | - |
| Investigations | | | | | | | | |
| ALT/AST
increased | 3 | 37.5 | 1 | 12.5 | - | - | - | - |
|
Lymphocytopenia | 1 | 12.5 | 3 | 37.5 | | | | |
| Serum amylase
increased | 1 | 12.5 | - | - | - | - | 1 | 12.5 |
| Weight loss | 2 | 25.0 | 3 | 37.5 | - | - | - | - |
| Metabolism and
nutrition disorders | | | | | | | | |
| Anorexia | 1 | 12.5 | - | - | - | - | - | - |
| Hypocalcemia | 3 | 37.5 | - | - | - | - | 1 | 12.5 |
| Hypokalemia | 1 | 12.5 | - | - | - | - | - | - |
| Nervous system
disorders | | | | | | | | |
| Headache | 1 | 12.5 | - | - | - | - | - | - |
| Respiratory,
thoracic and mediastinal disorders | | | | | | | | |
| Bronchopulmonary
hemorrhage | 1 | 12.5 | - | - | - | - | - | - |
| Epistaxis | 2 | 25.0 | - | - | - | - | - | - |
| Skin and
subcutaneous tissue disorders | | | | | | | | |
| Alopecia | 2 | 25.0 | 3 | 37.5 | 1 | 12.5 | - | - |
| Palmar-plantar
erythrodysesthesia | 1 | 12.5 | 3 | 37.5 | 3 | 37.5 | - | - |
| Rash | 1 | 12.5 | - | - | - | - | - | - |
| Vascular
disorders | | | | | | | | |
| Hypertension | 2 | 25.0 | 2 | 25.0 | 1 | 12.5 | - | - |
Discussion
Sorafenib has been approved by the FDA for the
treatment of unresectable hepatocellular carcinoma and advanced
renal cell carcinoma. Sorafenib inhibits the tyrosine kinase
activities of the vascular endothelial growth factor receptor
(VEGFR)-2 and -3, platelet-derived growth factor receptor, FMS-like
tyrosine kinase 3 and c-Kit, as well as certain intracellular
serine/threonine kinases (such as, C-Raf and B-Raf) (14). The most common BRAF mutation is the
V600E transversion, which may cause constitutive kinase activity
and has been found in PTC (6).
BRAF plays a critical role in cell signaling as an activator within
the mitogen-activated protein kinase pathway. Gain-of-function
mutations in the BRAF oncogene are the most frequent genetic
alterations found in PTC, occurring in ∼45% of cases (8), as do Ras mutations (10%) and
rearrangements in the RET gene (RET/PTC) in 5–30% of cases. These
mutations were also described in FTC, affecting >40% of cases
and leading to a more aggressive disease (15). In addition, the overexpression of
VEGF may contribute to the development and progression of DTC
(16,17). Those findings provided the
rationale for using sorafenib in patients with metastatic DTC.
The first trial of sorafenib in the treatment of
metastatic thyroid cancer was reported by Gupta-Abramson et
al (10). In that trial, 27 of
30 patients had DTC and of those patients, 68% had a diagnosis of
PTC. Seven patients (26%) had a PR lasting for 18–84 weeks, 16
patients (59%) had SD lasting for 14–89 weeks and the median PFS
was 79 weeks. Two phase II clinical trials of sorafenib reported an
efficacy of this drug in metastatic DTC. In a study by Schneider
et al (18), 31 patients
with progressive, metastatic or locally advanced RAI-refractory DTC
received sorafenib. After a median follow-up of 25 months, the
response rates were 31% PR and 42% SD, the median PFS was 18 months
and the median OS 34.5 months. In addition, Hoftijzer et al
(12) reported a PR rate of 25%,
an SD rate of 34%, a PD rate of 22% and a median PFS of 58 weeks in
31 patients with progressive DTC.
It was previously demonstrated that varying
responses to treatment in different organs is often encountered in
metastatic thyroid cancer patients treated with sorafenib. For
example, lung metastases respond more favorably to sorafenib
compared to lymph nodes (19).
Cabanillas et al (20)
reported the refractory nature of the bone metastases and pleural
lesions. The pathophysiological mechanism underlying this variable
response has not been fully elucidated. Whether these differences
in response are due to the different expression of various VEGFRs
or whether these are due to a non-VEGF-mediated mechanism, such as
differences in drug concentrations among tissues, remains to be
determined (19).
This pilot study presented our experience with
metastatic, progressive RAI-refractory DTC treated with sorafenib
at the Cancer Hospital of the Chinese Academy of Medical Sciences.
Our results were a PR rate of 50%, achieved within the first 6
months of treatment, with a durable response rate of 62.5%. The
median PFS and OS were 40.1 and 55.0 weeks, respectively. The PR
rate appeared to be superior compared to that in published phase II
trials evaluating sorafenib in DTC (10–12,18).
These differences in response may simply reflect the pre-study
characteristics of our patient group. The majority of the patients
(87.5%) had developed lung metastases, which responded better to
sorafenib compared to other organ lesions. However, inconsistent
with the response rate, the PFS and OS were shorter compared to
those observed in other phase II trials (10,11,18).
This difference may be attributed to the dose reduction due to the
development of AEs, with 2 of the 3 patients who underwent a
reduction in the dose of sorafenib to <400 mg/day experiencing
disease progression and eventually succumbing to the disease. Our
study also demonstrated that the lung metastases tended to respond
better to sorafenib, with the lymph nodes being less sensitive.
Tumor regression in response to sorafenib may occur in the lungs,
with simultaneous lesion progression in the lymph nodes in the same
patient. This variability of response by tissue site observed in
these patients requires validation by larger studies.
Monitoring the disease with tumor markers may be of
value in thyroid cancer. It is well known that serum TG is a highly
sensitive and specific marker of DTC metastasis and recurrence and
also reflects tumor burden. The change in serum TG levels prior to
and following treatment was considered to be a prognostic
indicator, assessing the efficacy of RAI treatment for bone
metastases (21). However, our
data suggested that the TG response in DTC patients treated with
sorafenib did not correlate with radiological response
(χ2=0.000, P=1.000) and may not be relied upon as a
marker of response. This result was in accordance with those
reported in other phase II trials of tyrosine-kinase inhibitors
(TKIs) in DTC, although the PFS and OS were longer in patients with
tumor marker CR compared to those in patients without tumor marker
CR (11). These results may
reflect organ-specific tumor resistance, which is often encountered
in patients with metastatic thyroid cancer treated with TKIs. Since
DTC bone metastases may also produce and secrete TG, the serum TG
levels are commonly significantly elevated in DTC patients with
bone metastases. Sorafenib was shown to be less effective in
patients with bone metastases (12). Notably, TLs were generally lung
lesions which were more sensitive to sorafenib; therefore, the
tumor marker response was not in accordance with the radiological
response during TKI treatment for DTC, although patients with bone
metastases with high levels of TG exhibited a significantly worse
PFS and OS. This may suggest that, in patients with progressing
bone lesions, TKI may not be effective and external beam radiation
should be considered prior to TKI treatment.
The tolerability of sorafenib at the standard dose
level was poor and 62.5% of the patients underwent a dose reduction
due to AEs, with 2 patients having a dose reduction to the lowest
level of 200 mg/day. Palmar-plantar erythrodysesthesia was the most
common AE, occurring in 87.5% patients and reaching grade 3 in
37.5% of the patients, followed by alopecia, hypertension,
diarrhea, fatigue and weight loss. These results were similar to
those reported by other phase II clinical trials of sorafenib in
thyroid cancer (11,13,18).
Notably, 1 patient developed grade 4 hypocalcemia on sorafenib,
despite daily intravenous calcium supplementation, and another
patient experienced a grade 4 amylase level elevation and grade 3
weight loss and fatigue. All AEs ameliorated following a dose
reduction of sorafenib to 200 mg/day.
In conclusion, sorafenib appears to be of value in
the treatment of patients with progressive metastatic
RAI-refractory DTC, since it increases clinical response and
prolongs PFS, even in patients exhibiting SD as their best response
to treatment. However, the mechanism underlying the differential
response of various metastatic sites (lungs, lymph nodes) requires
further elucidation. Patients with bone metastases and high TG
levels may be resistant to sorafenib and other prior treatment,
such as radiotherapy, should be considered. However, more efficient
agents or agent combinations are required to decrease the tumor
burden and improve survival, without adversely affecting the
quality of life of the patient.
Acknowledgements
This study was supported by Bayer Co.,
Ltd. and was partly funded by the Chinese National Major Project
for New Drug Innovation (nos. 2008ZX09312 and 2012ZX09303012) and
the Beijing Municipal Science and Technology Commission Major
Project for New Drug Innovation (no. Z121107005112005), P.R.
China.
References
|
1.
|
Sherman SI: Thyroid carcinoma. Lancet.
361:501–511. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Mazzaferri EL: An overview of the
management of papillary and follicular thyroid carcinoma. Thyroid.
9:421–427. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Jonklaas J, Sarlis NJ, Litofsky D, et al:
Outcomes of patients with differentiated thyroid carcinoma
following initial therapy. Thyroid. 16:1229–1242. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Sampson E, Brierley JD, Le LW, et al:
Clinical management and outcome of papillary and follicular
(differentiated) thyroid cancer presenting with distant metastasis
at diagnosis. Cancer. 110:1451–1456. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Shimaoka K, Schoenfeld DA, DeWys WD, et
al: A randomized trial of doxorubicin versus doxorubicin plus
cisplatin in patients with advanced thyroid carcinoma. Cancer.
56:2155–2160. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Caronia LM, Phay JE and Shah MH: Role of
BRAF in thyroid oncogenesis. Clin Cancer Res. 17:7511–7517. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Cohen Y, Xing M, Mambo E, et al: BRAF
mutation in papillary thyroid carcinoma. J Natl Cancer Inst.
95:625–627. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Henderson YC, Shellenberger TD, Williams
MD, et al: High rate of BRAF and RET/PTC dual mutations associated
with recurrent papillary thyroid carcinoma. Clin Cancer Res.
15:485–491. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Antonelli A, Fallahi P, Ferrari SM, et al:
New targeted therapies for thyroid cancer. Curr Genomics.
12:626–631. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Gupta-Abramson V, Troxel AB, Nellore A, et
al: Phase II trial of sorafenib in advanced thyroid cancer. J Clin
Oncol. 26:4714–4719. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Kloos RT, Ringel MD, Knopp MV, et al:
Phase II trial of sorafenib in metastatic thyroid cancer. J Clin
Oncol. 27:1675–1684. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Hoftijzer H, Heemstra KA, Morreau H, et
al: Beneficial effects of sorafenib on tumor progression, but not
on radioiodine uptake, in patients with differentiated thyroid
carcinoma. Eur J Endocrinol. 161:923–931. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Ahmed M, Barbachano Y, Riddell A, et al:
Analysis of the efficacy and toxicity of sorafenib in thyroid
cancer: a phase II study in a UK based population. Eur J
Endocrinol. 165:315–322. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Wilhelm SM, Adnane L, Newell P, et al:
Preclinical overview of sorafenib, a multikinase inhibitor that
targets both Raf and VEGF and PDGF receptor tyrosine kinase
signaling. Mol Cancer Ther. 7:3129–3140. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Garcia-Rostan G, Zhao H, Camp RL, et al:
ras mutations are associated with aggressive tumor phenotypes and
poor prognosis in thyroid cancer. J Clin Oncol. 21:3226–3235. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Vieira JM, Santos SC, Espadinha C, et al:
Expression of vascular endothelial growth factor (VEGF) and its
receptors in thyroid carcinomas of follicular origin: a potential
autocrine loop. Eur J Endocrinol. 153:701–709. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Jo YS, Li S, Song JH, et al: Influence of
the BRAF V600E mutation on expression of vascular endothelial
growth factor in papillary thyroid cancer. J Clin Endocrinol Metab.
91:3667–3670. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Schneider TC, Abdulrahman RM, Corssmit EP,
et al: Long-term analysis of the efficacy and tolerability of
sorafenib in advanced radio-iodine refractory differentiated
thyroid carcinoma: final results of a phase II trial. Eur J
Endocrinol. 167:643–650. 2012. View Article : Google Scholar
|
|
19.
|
Cabanillas ME, Waguespack SG, Bronstein Y,
et al: Treatment with tyrosine kinase inhibitors for patients with
differentiated thyroid cancer: the M. D. Anderson experience. J
Clin Endocrinol Metab. 95:2588–2595. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Cabanillas ME, Hu MI, Durand JB, et al:
Challenges associated with tyrosine kinase inhibitor therapy for
metastatic thyroid cancer. J Thyroid Res. 2011:9857802011.
View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Qiu ZL, Song HJ, Xu YH, et al: Efficacy
and survival analysis of 131I therapy for bone
metastases from differentiated thyroid cancer. J Clin Endocrinol
Metab. 96:3078–3086. 2011.PubMed/NCBI
|