Introduction
Neurothekeomas, or nerve sheath myxomas, are benign
peripheral nerve sheath-derived neoplasms that are continuously
subjected to conceptual changes in classification. The origin of
these tumors has not been elucidated and their etiology has been
debated upon (1,2). Their reproducible clinical,
histopathological and immunohistochemical differences were
demonstrated in a large series of studies (2–4).
Clinically, neurothekeoma is a slowly growing, usually
asymptomatic, dermal or, less frequently, mucosal or submucosal
tumor, occurring 2–4 times more frequently in women compared to men
(5,6). Neurothekeoma commonly develops on the
head, neck and upper extremities of young females in the second and
third decades of life. Other studies have documented different
locations, including the tongue, eyelids and oral mucosa (4,7,8). To
the best of our knowledge, this is the first case report of
neurothekeoma developing simultaneously in the thoracic and lumbar
area in an adult male.
Case report
A 51-year-old Chinese male patient presented with a
5-year history of a right lumbar mass and 1-year history of a right
thoracic wall mass. The right lumbar mass enlarged slowly, unlike
the right thoracic wall mass, which enlarged quickly, particularly
over the last 6 months. There was no reported pain, fever,
palpitations, irritability, dysphagia, dyspnea, weight loss, or
other significant medical of familial history. The patient did not
have a history of smoking and did not report any history of trauma.
Examination of the lesions revealed a solid mass in the right
thoracic wall and an elastic mass in the right lumbar area, which
were painless, non-tender, elliptical, firm, without local erythema
or edema of the overlying skin. Physical examination did not reveal
signs of lymphadenopathy or hepatosplenomegaly. Neurological
examination was normal.
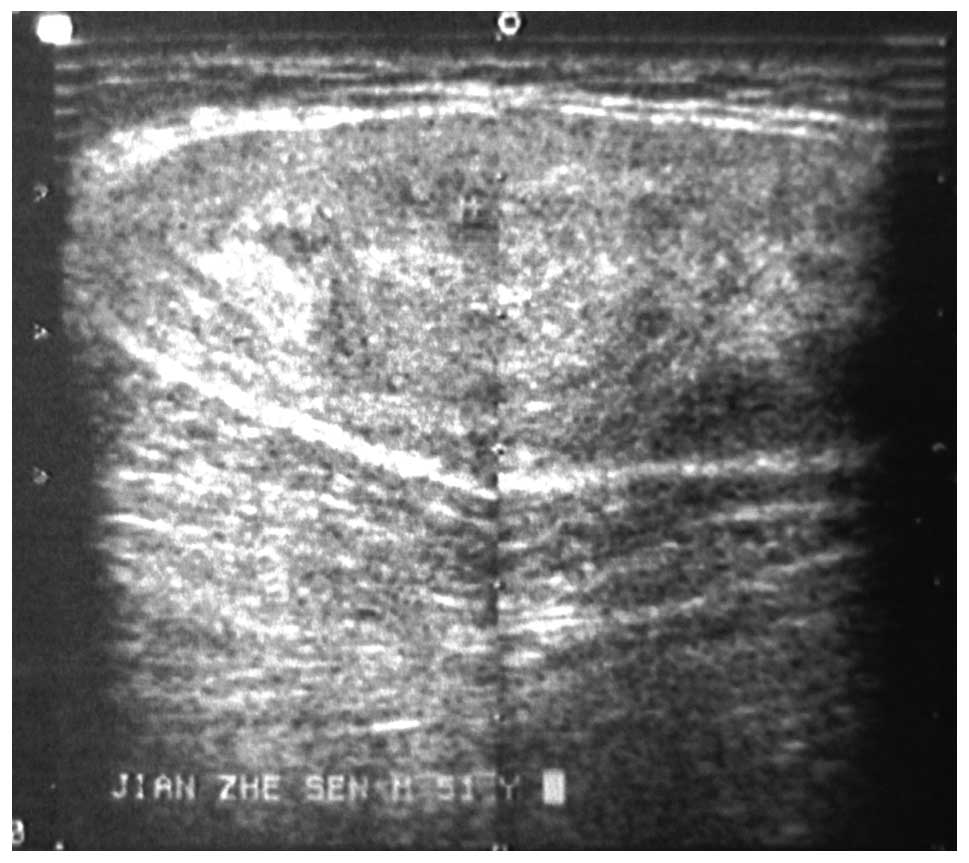
Ultrasonography of the thoracic and lumbar masses
showed a solid echo group, with clear boundaries and heterogeneous
internal echo (Fig. 1). Color
doppler flow imaging demonstrated a limited number of blood flow
signals in the mass. The thoracic X-rays, electrocardiogram and
serum electrolyte levels were normal.
The two masses were completely excised along the
capsule under local anaesthesia and the incisions were closed in
layers following adequate hemostasis. The surgical time was 2 h,
with an intraoperative blood loss of 30 ml. The dimensions of the
thoracic mass were ∼7.0×7.0×3.0 cm and those of the lumbar mass
∼4.0×7.0×3.0 cm. The tumors were encapsulated, with a solid and
gelatinous sectional plane.
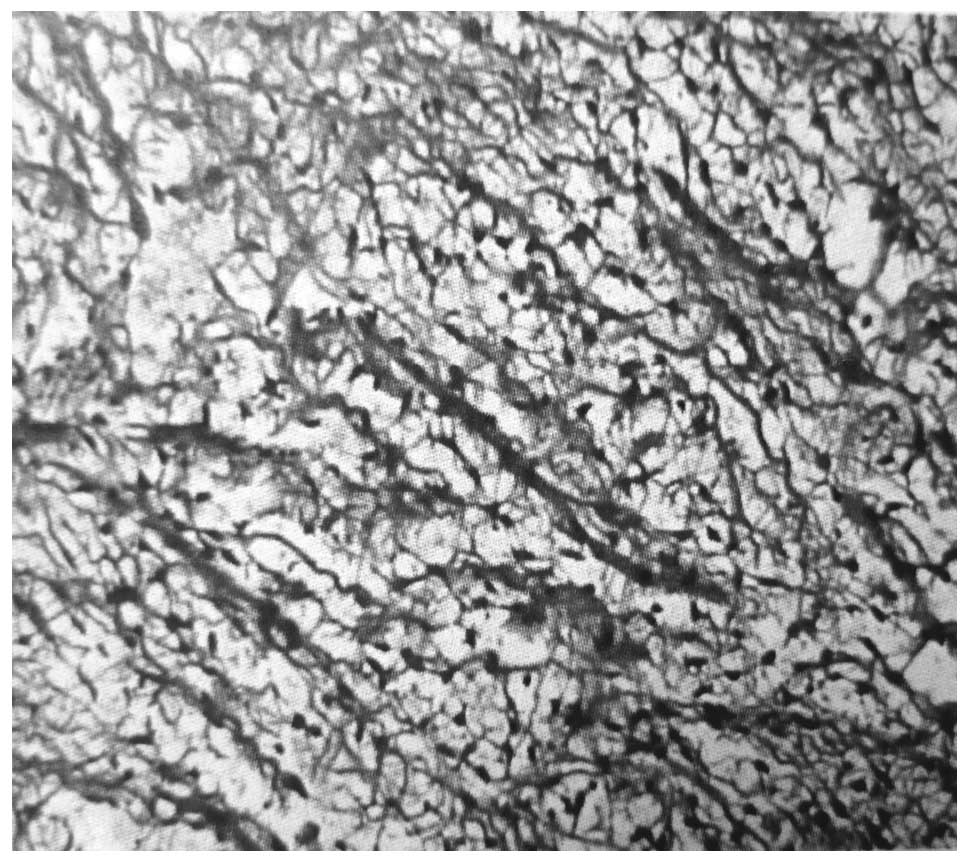
Histopathologically, the examination of the
microscopic slides of the two tumors revealed spindle and similar
epithelioid cells, arranged in fascicles, often in a geographical
pattern, in a background of myxoid stroma (Fig. 2). The immunohistochemical analysis
demonstrated that the tumor cells were positive for vimentin, CD57
and actin and negative for S-100 protein, HMB-45 and CD34. The
tumors were diagnosed as neurothekeomas. The patient remains alive
at the 7 year follow-up, without evidence of recurrence.
Discussion
Neurothekeoma was first described in 1969 under the
term ‘nerve sheath myxoma’; the name ‘neurothekeoma’ was adopted by
Gallager and Helwig (9) in 1980.
Neurothekeoma is an unusual benign soft tissue tumor of the
peripheral nervous system, which commonly occurs on the head, neck
and upper extremities of young females in the second and third
decades of life (10–12). To the best of our knowledge, this
is the first case report of neurothekeoma developing simultaneously
in the thoracic and lumbar area in an adult male.
Historically, neurothekeoma has been subclassified
as myxoid, cellular or mixed type, based on the amount of the
myxoid component; in our case, the neurothekeomas were of the
cellular subtype (13). Typically,
cellular neurothekeomas display a characteristic fascicular pattern
of spindle and epithelioid cells, with variable cytologic atypia
and mitotic activity (14).
Immunostaining demonstrated that the cells were negative for S-100
protein and HMB-45 and positive for vimentin, neuron-specific
enolase and NKI/C3 (14).
Neurothekeomas are difficult to diagnose prior to
performing a biopsy, due to the lack of specific clinical
manifestations or imaging characteristics. The diagnosis of the
thoracic mass was oriented towards lipoma prior to surgical
excision. Clinically, neurothekeoma is a commonly asymptomatic,
dermal, mucosal or submucosal tumor. On computed tomography scans,
it is identified as a hypoattenuated-to-isoattenuated mass, with
variable enhancement and vascularity patterns. On magnetic
resonance imaging scans, it exhibits well-defined margins,
intermediate signal on T1-weighted images, high signal on
T2-weighted images and heterogeneous mild-to-moderate gadolinium
contrast enhancement (15). The
differential diagnosis of neurothekeoma should include other neural
entities, such as schwannoma, true neuroma and myxoid neurofibroma.
The effective treatment of choice is complete surgical excision
with clear margins. No malignant transformation or metastasis have
been reported and local recurrence is extremely uncommon when there
are clear surgical margins.
In conclusion, neurothekeomas are uncommon, usually
small tumours, which are treated by simple excision. To the best of
our knowledge, this is the first case report of neurothekeomas
developing simultaneously in the thoracic and lumbar area in an
adult male. Neurothekeomas are difficult to diagnose prior to
biopsy. Although this is a rare type of tumor, the clinician should
consider this entity in differential diagnosis, as it is imperative
to distinguish it from malignant lesions, in order to avoid
unnecessary aggressive treatment.
Acknowledgements
This study was supported by the Anhui
Provincial Natural Science Foundation (1308085MH156).
References
|
1.
|
Barnhill RL and Mihm MC Jr: Cellular
neurothekeoma. A distinctive variant of neurothekeoma mimicking
nevomelanocytic tumors. Am J Surg Pathol. 14:113–120. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Hornick JL and Fletcher CD: Cellular
neurothekeoma: detailed characterization in a series of 133 cases.
Am J Surg Pathol. 31:329–340. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Fetsch JF, Laskin WB and Miettinen M:
Nerve sheath myxoma: a clinicopathologic and immunohistochemical
analysis of 57 morphologically distinctive, S-100 protein- and
GFAP-positive, myxoid peripheral nerve sheath tumors with a
predilection for the extremities and a high local recurrence rate.
Am J Surg Pathol. 29:1615–1624. 2005. View Article : Google Scholar
|
|
4.
|
Papalas JA, Proia AD, Hitchcock M, Gandhi
P and Cummings TJ: Neurothekeoma palpebrae: a report of 3 cases. Am
J Dermatopathol. 32:374–379. 2010.PubMed/NCBI
|
|
5.
|
Papadopoulos EJ, Cohen PR and Hebert AA:
Neurothekeoma: report of a case in an infant and review of the
literature. J Am Acad Dermatol. 50:129–134. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Marocchio LS, Oliveira DT and Consolaro A:
Myxoid neurothekeoma of the oral mucosa: an unusual benign tumor.
Oral Dis. 10:408–409. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Peñarrocha M, Bonet J, Minguez JM and Vera
F: Nerve sheath myxoma (neurothekeoma) in the tongue of a newborn.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 90:74–77.
2000.PubMed/NCBI
|
|
8.
|
Pepine M, Flowers F and Ramos-Caro FA:
Neurothekeoma in a 15-year-old boy: case report. Pediatr Dermatol.
9:272–274. 1992.PubMed/NCBI
|
|
9.
|
Gallager RL and Helwig EB: Neurothekeoma -
a benign cutaneous tumor of neural origin. Am J Clin Pathol.
74:759–764. 1980.PubMed/NCBI
|
|
10.
|
Roholt NS, Guitart J and Eramo LR: A
gradually enlarging asymptomatic nasal mass. Pediatr Dermatol.
12:191–194. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Busam KJ, Mentzel T, Colpaert C, Barnhill
RL and Fletcher CD: Atypical or worrisome features in cellular
neurothekeoma: a study of 10 cases. Am J Surg Pathol. 22:1067–1072.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Strumia R, Lombardi AR and Cavazzini L:
Cellular neurothekeoma. Acta Derm Venereol. 79:162–163. 1999.
View Article : Google Scholar
|
|
13.
|
Argenyi ZB, LeBoit PE, Santa Cruz D,
Swanson PE and Kutzner H: Nerve sheath myxoma (neurothekeoma) of
the skin: light microscopic and immunohistochemical reappraisal of
the cellular variant. J Cutan Pathol. 20:294–303. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Barnhill RL: Nerve sheath myxoma
(neurothekeoma). J Cutan Pathol. 21:91–93. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
O’Rourke H, Meyers SP and Katzman PJ:
Neurothekeoma in the upper extremity: magnetic resonance imaging
and computed tomography findings. J Comput Assist Tomogr.
29:847–850. 2005.PubMed/NCBI
|