Introduction
Colorectal cancer (CRC) is the third most commonly
diagnosed cancer worldwide. Despite advances in diagnosis and
treatment, CRC mortality has remained unchanged over the last 50
years and prognosis is closely associated with the disease stage at
the time of diagnosis (1), with a
5-year survival rate of only 8% in patients with stage IV CRC
(2).
Several patients develop bowel obstruction, which is
a well-recognized complication of advanced-stage CRC, with an
incidence of 7–47% (3,4). Compared to those with non-obstructive
CRC, the 5-year survival rate of patients with obstructive CRC was
reported to be ~20% (5–7). In addition, certain factors are
significantly different between the two groups, including
peritoneal metastasis, histological grade and recurrence. As
regards the treatment of patients with stage IV CRC, opinions vary
widely. For patients with complications, surgical treatment is
required. The development of modern technology enables the
effective treatment of a number of asymptomatic or minimally
symptomatic patients with stage IV CRC. The major aims of therapy
are to prolong survival and maintain the quality of life.
Asymptomatic patients may be treated without resection in order to
avoid complications and the risk of perioperative morbidity
(8,9). When compared to asymptomatic patients
who underwent surgical resection, asymptomatic patients with
distant metastasis who underwent resection exhibited no survival
benefits (10). Kaufman et
al (11) reported that
patients receiving surgical resection, chemotherapy, or a
combination of the two, had median survival times of 22, 15 and 30
months, respectively. In order to avoid local tumor complications
and improve the chances of further treatment, some studies
recommend palliative resection of the primary tumor in asymptomatic
patients (12–14).
Although the effects of obstruction and surgery on
survival were previously reported, the number of available studies
investigating the factors of obstruction in patients with stage IV
CRC in China is currently limited. Therefore, in the present study,
we aimed to investigate bowel obstruction in patients with stage IV
CRC and retrospectively analyze the clinicopathological
characteristics and long-term outcomes for such patients.
Patients and methods
Study population
Between August, 1994 and December, 2005 a total of
2,950 patients were diagnosed with CRC and treated at the Sixth
Affiliated Hospital of Sun Yat-sen University (Guangzhou, China). A
total of 381 patients were diagnosed with stage IV CRC and were
divided into two groups according to the presence (n=295) or
absence (n=86) of obstruction. We retrospectively analyzed the
clinicopathological characteristics of the CRC patients from a
computerized database and the patients were divided into subgroups
according to the recorded variables as follows: i) gender, age
(<60 and ≥60 years) and family history; ii) tumor location
(colon and rectum), tumor differentiation (well-, moderately and
poorly differentiated adenocarcinoma) and tumor size (≤5 and >5
cm); iii) blood transfusion, resection of the primary tumor,
ascites, peritoneal metastasis and hepatic metastasis.
Statistical analysis
Patient survival was analyzed with the Kaplan-Meier
method and the variables were compared using the log-rank test. A
multivariate analysis of the patients was performed using the Cox
proportional hazards model, which is mainly used in the analysis of
survival data for investigating the association between patient
survival and covariates (independent variables or predictors).
Results
Patients and tumor characteristics
The demographic, patient and pathological
characteristics of CRC are summarized in Table I. The mean age of the patients was
58.18 years (range, 25–87 years) in the non-obstructive and 56.58
years (range, 19–87 years) in the obstructive CRC groups. The
number of blood transfusions was similar between the two groups and
there was no significant difference in survival rate between
patients who received a blood transfusion and those who did not
(P=0.373) (Table II). The overall
survival rate was also compared by gender, family history of CRC,
age, tumor size, tumor location, peritoneal metastasis,
histological grade and histological type, but the differences were
not found to be statistically significant (Table II).
 | Table IAnalysis of demographic, patient and
pathological characteristics in patients with colorectal cancer,
with or without bowel obstruction (n=381). |
Table I
Analysis of demographic, patient and
pathological characteristics in patients with colorectal cancer,
with or without bowel obstruction (n=381).
| | Obstruction | |
|---|
| |
| |
|---|
| Characteristics | Cases | No | Yes | P-value |
|---|
| Gender | | | | 0.003 |
| Female | 227 | 164 | 63 | |
| Male | 154 | 131 | 23 | |
| Radical
resection | | | | 0.005 |
| No | 180 | 128 | 52 | |
| Yes | 201 | 167 | 34 | |
| Age (years) | | | | 0.165 |
| <60 | 189 | 152 | 37 | |
| ≥60 | 192 | 143 | 49 | |
| Family history | | | | 0.159 |
| No | 367 | 282 | 85 | |
| Yes | 14 | 13 | 1 | |
| Blood
transfusion | | | | 0.087 |
| No | 186 | 151 | 35 | |
| Yes | 195 | 144 | 51 | |
| Histological
type | | | | <0.001 |
| Villous
adenocarcinoma | 57 | 47 | 10 | |
| Tubular
adenocarcinoma | 262 | 210 | 52 | |
| Mucinous
adenocarcinoma | 39 | 30 | 9 | |
| Signet ring cell
tumor | 23 | 8 | 15 | |
| Ascites | | | | <0.001 |
| No | 295 | 222 | 73 | |
| Yes | 86 | 41 | 45 | |
| Tumor size (cm) | | | | 0.041 |
| ≤5 | 221 | 180 | 41 | |
| >5 | 160 | 116 | 44 | |
| Tumor location | | | | <0.001 |
| Colon | 147 | 115 | 32 | |
| Rectum | 234 | 180 | 54 | |
| Peritoneal
metastasis | | | | <0.001 |
| No | 331 | 279 | 52 | |
| Yes | 50 | 16 | 34 | |
| Hepatic
metastasis | | | | <0.001 |
| No | 285 | 240 | 45 | |
| Yes | 96 | 55 | 41 | |
| Histological
differentiation | | | | 0.520 |
| High | 40 | 33 | 7 | |
| Moderate | 241 | 188 | 53 | |
| Poor | 100 | 74 | 26 | |
| Table IIUnivariate analysis of patients with
stage IV colorectal cancer (n=381). |
Table II
Univariate analysis of patients with
stage IV colorectal cancer (n=381).
| Overall survival
rate (%) | |
|---|
|
| |
|---|
| Variables | 1-year | 3-year | 5-year | P-value |
|---|
| Gender | | | | 0.194 |
| Female | 95.6 | 87.8 | 78.9 | |
| Male | 93.5 | 81.3 | 68.6 | |
| Age (years) | | | | 0.235 |
| <60 | 96.7 | 88.8 | 75.4 | |
| ≥60 | 98.3 | 83.8 | 71.5 | |
| Family history | | | | 0.850 |
| No | 97.5 | 92.4 | 87.3 | |
| Yes | 48.6 | 20.8 | 20.8 | |
| Histological
type | | | | 0.796 |
| Villous
adenocarcinoma | 81.3 | 43.8 | 13.5 | |
| Tubular
adenocarcinoma | 96.5 | 90.8 | 82.9 | |
| Mucinous
adenocarcinoma | 71.5 | 22.0 | 22.0 | |
| Signet ring cell
tumor | 52.9 | 21.2 | 21.2 | |
| Blood
transfusion | | | | 0.373 |
| No | 96.2 | 86.8 | 75.1 | |
| Yes | 94.8 | 84.7 | 72.2 | |
| Tumor size
(cm) | | | | 0.362 |
| ≤5 | 95.4 | 87.8 | 76.8 | |
| >5 | 94.4 | 82.2 | 69.5 | |
| Tumor location | | | | 0.308 |
| Colon | 94.6 | 85.7 | 73.1 | |
| Rectum | 95.3 | 85.2 | 73.2 | |
| Ascites | | | | <0.001 |
| No | 96.6 | 91.1 | 82.2 | |
| Yes | 92.2 | 73.5 | 83.3 | |
| Peritoneal
metastasis | | | | 0.290 |
| No | 96.8 | 91.1 | 84.4 | |
| Yes | 90.5 | 65.5 | 41.7 | |
| Hepatic
metastasis | | | | 0.010 |
| No | 95.2 | 84.5 | 73.0 | |
| Yes | 95.2 | 82.9 | 64.5 | |
| Radical
resection | | | | <0.001 |
| No | 93.9 | 84.2 | 72.3 | |
| Yes | 96.5 | 87.1 | 78.5 | |
| Histological
differentiation | | | | 0.630 |
| High | 67.6 | 16.5 | 16.5 | |
| Moderate | 94.6 | 84.6 | 73.4 | |
| Poor | 94.9 | 83.3 | 67.8 | |
| Obstruction | | | | 0.044 |
| No | 96.9 | 90.7 | 84.3 | |
| Yes | 89.2 | 64.1 | 34.4 | |
Univariate and multivariate analysis of
patients with stage IV CRC
The univariate prognostic factors in patients with
stage IV CRC are summarized in Table
II. Ascites (P<0.001), hepatic metastasis (P=0.010) and
radical resection (P<0.001) were found to be associated with
outcome in stage IV CRC. However, certain factors, including
gender, age, family history, blood transfusion, histological grade
and tumor location, were not found to affect survival. In the
analysis of obstruction, the multivariate analysis demonstrated
that obstruction, ascites, hepatic metastasis and radical resection
were independent factors for the survival of patients with stage IV
CRC (Table III).
| Table IIIMultivariate analysis of factors
associated with survival in patients with stage IV colorectal
cancer. |
Table III
Multivariate analysis of factors
associated with survival in patients with stage IV colorectal
cancer.
| | | | | | | 95% CI for
Exp(B) |
|---|
| | | | | | |
|
|---|
| Factors | B | SE | Wald | df | Sig. | Exp(B) | Lower | Upper |
|---|
| Obstruction | 0.262 | 0.152 | 2.953 | 1 | 0.086 | 1.299 | 0.964 | 1.752 |
| Ascites | 0.152 | 0.144 | 1.105 | 1 | 0.293 | 1.164 | 0.877 | 1.545 |
| Hepatic
metastasis | 0.195 | 0.055 | 12.522 | 1 | <0.001 | 1.215 | 1.091 | 1.354 |
| Radical
resection | 0.693 | 0.110 | 39.976 | 1 | <0.001 | 2.000 | 1.613 | 2.480 |
Long-term outcomes
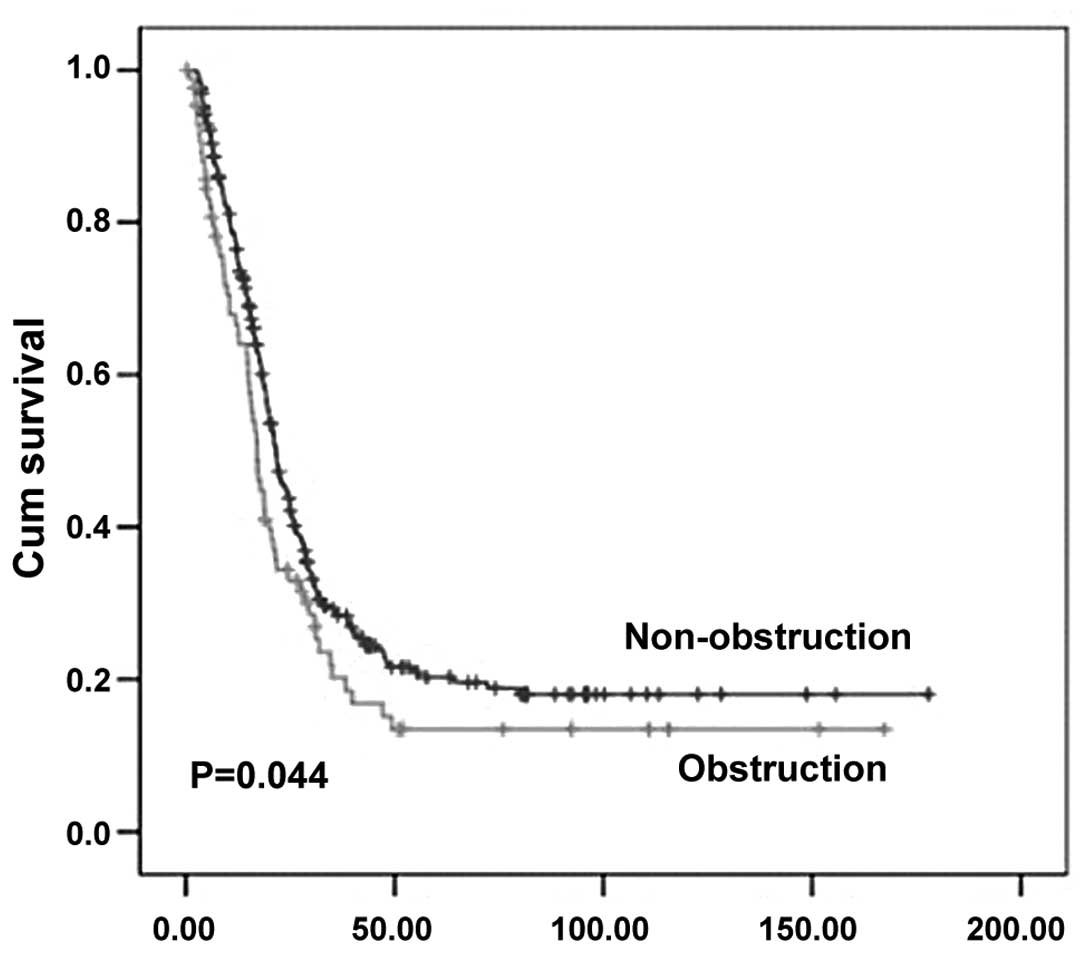
A comparison of the survival curves between the
non-obstruction and obstruction groups is shown in Fig. 1. The mean/median survival time was
49.4/21.6 and 37.2/17.1 months in the non-obstruction and
obstruction groups, respectively. In the colon, the mean/median
survival time was 54.4/21.4 and 48.0/17.8 months in the
non-obstruction and obstruction groups, respectively. The overall
3- and 5-year survival rates were 90.7 and 84.3% in the
non-obstruction group, respectively, and 64.1 and 34.4% in the
obstruction CRC group, respectively.
Discussion
It was recently reported that tumor size is
associated with the prognosis of CRC (15), which was inconsistent with our
results. The fact that the appropriate cut-off values and the
dynamic point of the optimal cut-off values were not taken into
consideration in this study, may explain the fact that we were
unable to verify the prognostic significance of tumor size.
In agreement with previous findings (16), in our study, the survival of
patients with radical resection was better compared to that of the
patients who had undergone non-radical resection, indicating that
complete tumor resection is associated with prognosis in patients
with stage IV CRC. The total number of patients with
non-obstructive CRC was 295 (~77.4%) and the survival of patients
with obstructive CRC was poor. A previous study reported that
patients aged <40 or >80 years were at an increased risk of
developing bowel obstruction (17). However, our study demonstrated that
the percentage of patients with obstructive CRC and advanced cancer
did not statistically differ between age groups. Similarly, the
differences in survival did not approach statistical significance
in the analysis by obstruction (Table III). However, obstructive CRC was
associated with a poor prognosis and shorter overall survival
according to the multivariate Cox regression model (Table III). This may due to the number
of patients enrolled in this study. Similar conclusions were also
reached by previous studies (18,19).
According to our results, the survival of CRC
patients with bowel obstruction is significantly associated with
radical resection, ascites and hepatic metastasis. The overall 1-,
3- and 5-year survival rates were lower in the obstructive compared
to those in the non-obstructive CRC group. However, bowel
obstruction was not found to be associated with a poorer prognosis
or shorter overall survival in the multivariate Cox regression
model, which was a finding inconsistent with previously reported
results (20). In addition,
intestinal obstruction may occur at any site along the colon and
rectum, while the risk of obstruction varies across the intestine.
In our study, 27 (31.3%) patients presented with bowel obstruction
at the level of the rectum and 59 (68.6%) patients had obstruction
of the colon. This result was similar to those of previous studies
(21,22). In our study, the histological
grade/type of CRC was not found to be an independent prognostic
factor (Table II), which was
different from previously reported findings (19). The difference observed in our study
may be a result of the inconsistent grading criteria and grouping
systems among different grades.
The presence of ascites was associated with
prognosis in the analysis of obstruction and surgical treatment.
Patients with ascites exhibited a significantly worse survival
compared to those without ascites, which is consistent with
previous findings (23). It is
recommended that patients with ascites receive non-surgical
treatment, such as hydration, corticosteroids and percutaneous
gastrostomy (24). Moreover, the
number of patients with hepatic metastases in our study was similar
or higher compared to that reported by previous studies. This
difference may be a result of the differences in tumor stage and
histological type; for example, ulcerated tumors were reported to
be associated with a higher metastatic risk (25).
There were some limitations to this study. The
number of patients in our study was relatively small and,
therefore, some factors associated with prognosis may have been
overlooked. In addition, several factors were not investigated in
this study, such as the levels of carcinoembryonic antigen and
CA19-9, chemotherapy and perineural invasion. Furthermore, data
regarding recurrence following surgery in patients with CRC were
not available.
In conclusion, we demonstrated that certain
prognostic factors may affect the outcome of patients with stage IV
CRC, although obstruction was not found to be an independent
indicator of survival. The patients with bowel obstruction had a
poorer prognosis compared to those with non-obstructive CRC,
whereas active radical surgery significantly improved the prognosis
of patients with stage IV CRC.
References
|
1
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
2
|
Jemal A, Siegel R, Ward E, et al: Cancer
statistics, 2006. CA Cancer J Clin. 56:106–130. 2006. View Article : Google Scholar
|
|
3
|
Chen HS and Sheen-Chen SM: Obstruction and
perforation in colorectal adenocarcinoma: an analysis of prognosis
and current trends. Surgery. 127:370–376. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lee YM, Law WL, Chu KW and Poon RT:
Emergency surgery for obstructing colorectal cancers: a comparison
between right-sided and left-sided lesions. J Am Coll Surg.
192:719–725. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Phillips RK, Hittinger R, Fry JS and
Fielding LP: Malignant large bowel obstruction. Br J Surg.
72:296–302. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ohman U: Prognosis in patients with
obstructing colorectal carcinoma. Am J Surg. 143:742–747. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
McArdle CS and Hole DJ: Emergency
presentation of colorectal cancer is associated with poor 5-year
survival. Br J Surg. 91:605–609. 2004.PubMed/NCBI
|
|
8
|
Michel P, Roque I, Di Fiore F, et al:
Colorectal cancer with non-resectable synchronous metastases:
should the primary tumor be resected? Gastroenterol Clin Biol.
28:434–437. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Clements D, Dhruva Rao P, Ramanathan D,
Adams R, Maughan TS and Davies MM: Management of the asymptomatic
primary in the palliative treatment of metastatic colorectal
cancer. Colorectal Dis. 11:845–848. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Scoggins CR, Meszoely IM, Blanke CD,
Beauchamp RD and Leach SD: Nonoperative management of primary
colorectal cancer in patients with stage IV disease. Ann Surg
Oncol. 6:651–657. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kaufman MS, Radhakrishnan N, Roy R, et al:
Influence of palliative surgical resection on overall survival in
patients with advanced colorectal cancer: a retrospective single
institutional study. Colorectal Dis. 10:498–502. 2008. View Article : Google Scholar
|
|
12
|
Stelzner S, Hellmich G, Koch R and Ludwig
K: Factors predicting survival in stage IV colorectal carcinoma
patients after palliative treatment: a multivariate analysis. J
Surg Oncol. 89:211–217. 2005. View Article : Google Scholar
|
|
13
|
Ruo L, Gougoutas C, Paty PB, Guillem JG,
Cohen AM and Wong WD: Elective bowel resection for incurable stage
IV colorectal cancer: prognostic variables for asymptomatic
patients. J Am Coll Surg. 196:722–728. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rosen SA, Buell JF, Yoshida A, et al:
Initial presentation with stage IV colorectal cancer: how
aggressive should we be? Arch Surg. 135:530–535. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kornprat P, Pollheimer MJ, Lindtner RA,
Schlemmer A, Rehak P and Langner C: Value of tumor size as a
prognostic variable in colorectal cancer: a critical reappraisal.
Am J Clin Oncol. 34:43–49. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Abdalla EK: Resection of colorectal liver
metastases. J Gastrointest Surg. 15:416–419. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wong SK, Kneebone A, Morgan M, Henderson
CJ, Morgan A and Jalaludin B: Surgical management of colorectal
cancer in south-western Sydney 1997–2001: a prospective series of
1293 unselected cases from six public hospitals. ANZ J Surg.
75:776–782. 2005.PubMed/NCBI
|
|
18
|
Liang H, Wang XN, Wang BG, et al:
Prognostic factors of young patients with colon cancer after
surgery. World J Gastroenterol. 12:1458–1462. 2006.PubMed/NCBI
|
|
19
|
Hotokezaka M, Jimi S, Hidaka H, et al:
Factors influencing outcome after surgery for stage IV colorectal
cancer. Surg Today. 38:784–789. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yang Z, Wang L, Kang L, et al:
Clinicopathologic characteristics and outcomes of patients with
obstructive colorectal cancer. J Gastrointest Surg. 15:1213–1222.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sarela AI, Guthrie JA, Seymour MT, Ride E,
Guillou PJ and O’Riordain DS: Non-operative management of the
primary tumour in patients with incurable stage IV colorectal
cancer. Br J Surg. 88:1352–1356. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Nash GM, Saltz LB, Kemeny NE, et al:
Radical resection of rectal cancer primary tumor provides effective
local therapy in patients with stage IV disease. Ann Surg Oncol.
9:954–960. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jayne DG, Fook S, Loi C and Seow-Choen F:
Peritoneal carcinomatosis from colorectal cancer. Br J Surg.
89:1545–1550. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Higashi H, Shida H, Ban K, et al: Factors
affecting successful palliative surgery for malignant bowel
obstruction due to peritoneal dissemination from colorectal cancer.
Jpn J Clin Oncol. 33:357–359. 2003. View Article : Google Scholar
|
|
25
|
Manfredi S, Lepage C, Hatem C, Coatmeur O,
Faivre J and Bouvier AM: Epidemiology and management of liver
metastases from colorectal cancer. Ann Surg. 244:254–259. 2006.
View Article : Google Scholar : PubMed/NCBI
|