Introduction
Kidney cancer is the 13th most common malignancy,
with ~271,000 new cases diagnosed worldwide in 2008 (1). The incidence rates of kidney cancer
are the highest in Europe, North America and Australia, whereas
they are low in India, Japan, Africa and China. Over the past
several decades, the incidence rates of kidney cancer have been
steadily increasing by ~1.7% in males and 2.2% in females each year
in the United States (2,3). In 2010, 58,240 new cases of kidney
cancer and 13,040 deaths were reported in the United States
(4), accounting for ~4% of all new
primary cancer cases. In Taiwan, the estimated annual incidence
rate of kidney cancer was 5.22 and 2.45 per 100,000 males and
females, respectively, with estimated mortality rates of 2.56 and
2.02 per 100,000 males and females, respectively, in 2008 (5).
Approximately 25–30% of patients with kidney cancer
present with metastases at the time of diagnosis, since the
majority of kidney cancer cases initially present with an
asymptomatic clinical course. Patients with localized renal cell
carcinoma (RCC) may exhibit longer times to relapse following
nephrectomy, with a median duration of ~15–18 months. The majority
of relapses occur within the first 3 years after nephrectomy
(6,7). Metastatic RCC (mRCC) is a major
clinical problem for oncologic health care worldwide, due to its
extremely poor prognosis (6).
The economic impact of RCC on healthcare resources
has increasing significantly with its increasing incidence in the
United States and Asian countries. The annual economic burden of
RCC was estimated to be 0.60–5.19 billion USD (16,488–43,805 USD
per patient) in the United States (8). Furthermore, the economic burden of
RCC is expected to grow with the increasing use of targeted
therapies (9).
New targeted agents for the treatment of RCC are
continuously developed since 2005. There are currently two groups
of such agents, vascular endothelial growth factor-targeted
therapies and mammalian target of rapamycin inhibitors. Seven newer
targeted agents (sorafenib, sunitinib, pazopanib, everolimus,
temsirolimus, axitinib and cediranib) have been approved by the
Food and Drug Administration of the United States and Taiwan for
the treatment of RCC. However, these agents are significantly more
costly compared to traditional chemotherapy. In particular, due to
the lack of head-to-head comparisons, the information regarding
their comparative effectiveness is limited and their toxicities are
a major concern. Hence, with the aid of network meta-analysis, this
study aimed to compare the efficacy and safety among these 7 newer
targeted agents for patients with mRCC.
Materials and methods
Literature search
A systematic literature search of the Medline,
Embase, Cochrane Library and ClinicalTrials.gov databases was
performed to identify all clinical studies on those 7 newer
targeted agents for the treatment of mRCC between January 1, 1999
and August 31, 2013. The databases were searched using the
following medical subject headings or text keywords: metastatic or
advanced renal cell cancer or carcinoma and targeted agents. In
addition, we searched the references of the selected studies
manually to identify any overlooked literature. Only randomised
clinical trials (RCTs) of the 7 targeted agents for mRCC published
in English were considered in this study.
Data extraction
Two reviewers screened the titles and abstracts of
all identified studies to exclude ineligible studies and then read
the full texts of the remaining studies independently. We collected
data on patient demographic and clinical characteristics, study
design, interventions, direct outcomes and sample sizes from each
of the selected studies using a standardised data-recording
form.
Quality assessment
We used the Cochrane Collaboration Recommendations
for Assessment to evaluate the risk of bias in each included study
(10). The criteria for measuring
the risk of bias included i) allocation concealment, ii) random
sequence generation, iii) presence of blinding in the studies
(patients, assessors and physicians), iv) incomplete outcome data,
v) selective outcome reporting and vi) other sources of bias. Each
study was evaluated explicitly based on these 6 criteria using the
following scoring system: low risk of bias, high risk of bias or
unclear (either lack of information or uncertainty regarding the
potential for bias). We also assessed the quality of evidence in
these studies using the Grading of Recommendations, Assessment,
Development and Evaluations (GRADE) profiler (GRADEpro) software,
version 3.2 (The Cochrane Information Management System) (11). This software was used to perform
several of the required calculations, guide us through the process
of grading the quality of the evidence and create a Summary of
Findings table (10).
Data synthesis
We conducted a network meta-analysis, referred to as
mixed or multiple treatment comparisons (MTC) meta-analysis, to
compare the outcomes among the 7 newer targeted agents for mRCC,
which included direct (i.e., head-to-head) and indirect treatment
comparisons (12,13). The two major studied outcomes for
comparison were i) efficacy, in terms of longer progression-free
survival (PFS) as measured by the hazard ratio (HR) and ii) safety,
defined by the withdrawals due to adverse events, as measured by
the odds ratio. Indirect treatment comparisons were usually
performed based on the available direct treatment comparisons with
common comparators, such as placebo or a standard treatment.
Direct (head-to-head) comparisons of
treatment effects
We summarized the results of the available direct
(head-to-head) treatment comparisons from the included 7 RCTs using
the Review Manager (RevMan) software, version 5.2.3 (The Cochrane
Collaboration, Copenhagen, Denmark) (14).
Indirect comparisons of treatment
effects
Two methods of indirect meta-analysis were used: the
most frequently used method was the adjusted indirect comparisons
using the random effects model as described by Bucher et al
(15) and Caldwell et al
(16) and the Bayesian method
outlined by Lu and Ades (13).
According to the Bucher method, we calculated the
logarithm of the HR and its standard error and used each in
indirect comparisons for each included RCT. These comparisons
included direct within-trial comparisons between two treatment
strategies, as well as indirect comparisons constructed from trials
that had one treatment in common. We performed the indirect
comparisons using the Canadian Agency for Drugs and Technologies in
Health (CADTH) Indirect Treatment Comparisons software, version 1.0
(CADTH, Ottawa, ON, Canada) (17).
For safety, we also used the Bayesian method under
the logit random effects consistency model with the assumption of a
homogeneous variance for the specified random effect fitted to
perform the MTC on the log-odds scale. The default values of
various options in the GPU-Enabled Many-Task Computing (GeMTC)
package were applied for the required Bayesian computations in R.
The potential inconsistency between direct and indirect comparisons
could not be detected, as the inconsistency degree of freedom was 0
in our study. We used the GeMTC R package, version 0.2 (February
19, 2013) software, version 2.15.2 (R Foundation for Statistical
Computing, Vienna, Austria) (18).
Results
Results of literature search
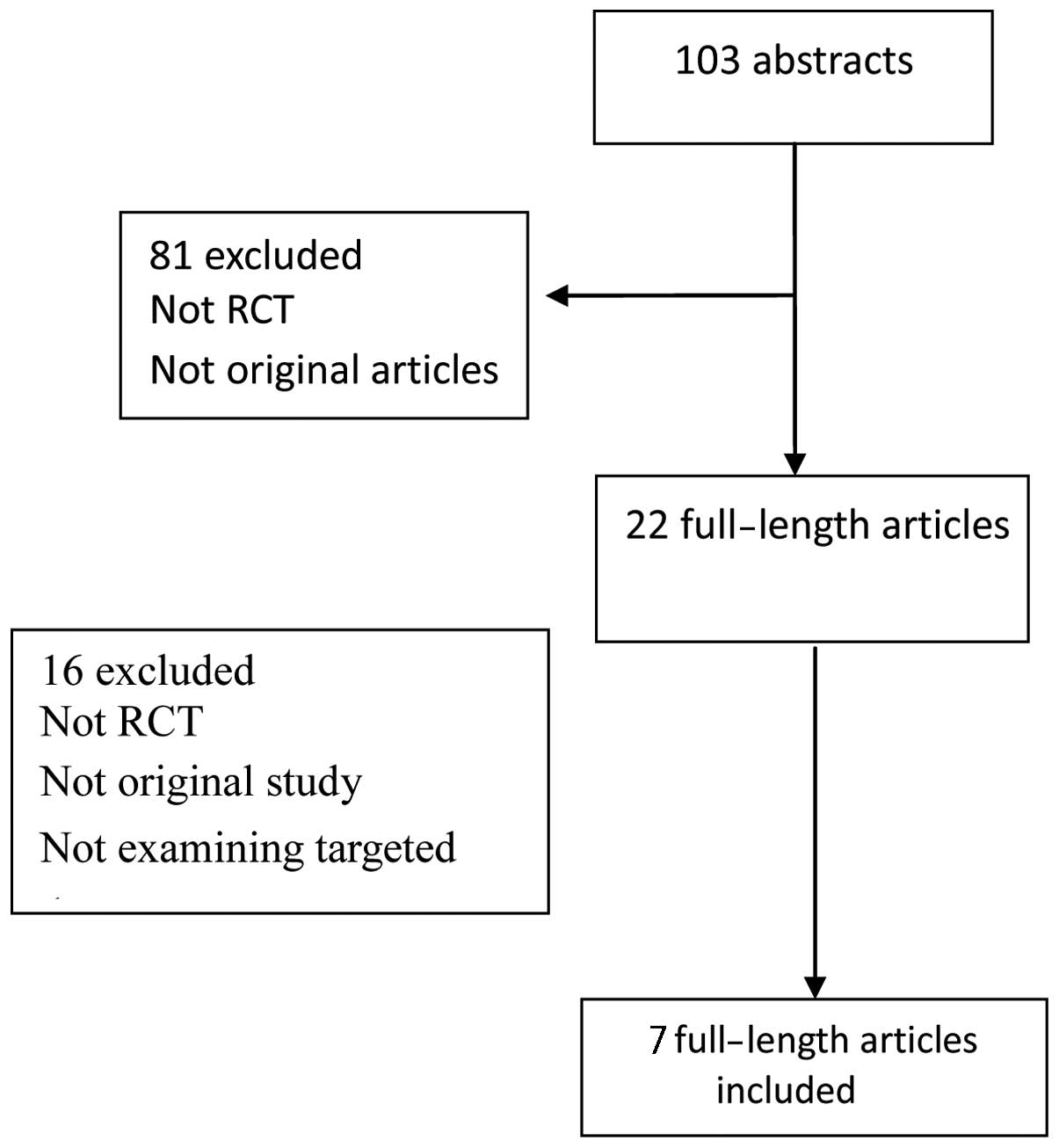
Fig. 1 depicts the
flow diagram of the systematic literature search and selection of
RCTs. The systematic literature search identified 103 abstracts. A
total of 81 articles were excluded, as they were not RCTs or did
not investigate at least one of our targeted drugs. After reviewing
22 full-length articles, only 7 RCTs matched the inclusion criteria
of this study (19–24). Two studies were head-to-head
comparisons of two newer targeted agents.
Characteristics of the selected RCTs
The demographic and clinical characteristics of the
7 selected RCTs are summarized in Table I. Each targeted agent was compared
to a placebo in RCTs. All the patients enrolled in the included
studies were aged >18 years, were diagnosed with metastatic
clear cell RCC, had a life expectancy of 12 weeks and had an
Eastern Cooperation Oncology Group performance status of 0 or 1.
All the patients had previously undergone nephrectomy or received a
systematic cytokine-based treatment. The prognostic risks were
classified according to the Memorial Sloan-Kettering Cancer Center
prognostic score (22).
 | Table IDemographic and clinical
characteristics of the selected randomized clinical trials. |
Table I
Demographic and clinical
characteristics of the selected randomized clinical trials.
| Study, year therapy
(refs.) | Intervention and
comparator | No. of males,
(%) | Median patient age,
years | ECOG PS, n (%) | MSKCC prognostic
risk, n (%)
Low/intermediate/high | No. of metastatic
sites (%) | Metastatic sites in
lung/liver
n (%) | Previous
nephrectomy
n (%) | Previous
cytokine-based systemic
n (%) |
|---|
|
|
|---|
| 0 | 1 | 2 | 1 | 2 | >2 | DM |
|---|
| TARGET, Escudier
et al, 2007 (19) | Sorafenib
(n=451) | 315 (70) | 58 | 219 (49) | 223 (49) | 7 (2) | 233 (52)/218
(48)/NA | 62 (14) | 131 (29) | 256 (57) | 2 (<1) | 348/116
(77)/(26) | 422 (94) | 374 (83) |
| Placebo (n=452) | 340 (75) | 59 | 210 (46) | 236 (52) | 4 (1) | 228 (50)/223
(49)/NA | 63 (14) | 129 (29) | 258 (57) | 2 (<1) | 348/117
(77)/(26) | 421 (93) | 368 (81) |
| VEG105192, Sternberg
et al, 2010 (21) | Pazopanib
(n=290) | 198 (68) | 59 | 123 (42) | 167 (58) | | 113 (39)/159 (55)/9
(3) | 53 (16) | 78 (27) | 159 (55) | | 214/106
(74)/(73) | 258 (89) | 135 (47) |
| Placebo (n=145) | 109 (75) | 60 | 60 (41) | 85 (59) | | 57 (39)/77 (53)/9
(3) | 20 (14) | 50 (34) | 75 (52) | | 75/32 (26)/(22) | 127 (88) | 67 (46) |
| Motzer et al,
2010 (20) | Everolimus
(n=277) | 216 (78) | 61 | | NA | | 81 (29)/156 (56)/40
(14) | 24 (9) | 68 (25) | 182 (66) | | 203/92 (73)/(33) | 269 (97) | 179 (65) |
| Placebo
(n=139) | 106 (76) | 60 | | | | 39 (28)/79 (57)/21
(15) | 21 (15) | 79 (57) | 39 (28) | | 112/53
(81)/(38) | 133 (96) | 93 (67) |
| AZD2171, Mulders
et al, 2012 (22) | Cediranib
(n=53) | 40 (75) | 60 | | NA | | 26 (49)/26 (49)/1
(2) | 7 (13) | 19 (36) | 26 (47) | | NA | 46 (87) | 27 (51) |
| Placebo (n=18) | 15 (83) | 61 | | | | 6 (33)/10 (56)/2
(11) | | | | | | 15 (83) | 9 (50) |
| AXIS, Rini et
al, 2011 (23) | Axitinib
(n=361) | 265 (73) | 61 | 195 (54) | 162 (45) | 1 (<1) | 100 (28)/134
(37)/118 (33) | | NA | | | NA | NA | 126 (35) |
| Sorafenib
(n=362) | 258 (71) | 61 | 200 (55) | 160 (44) | 0 | 79 (22)/225 (62)/34
(9) | | | | | | | 125 (35) |
| INTORSECT Hutson
et al, 2014 (24) | Temsirolimus
(n=259) | 259 (194) | 60 | 103 (40) | 150 (58) | 6 (2) | 50 (19)/178 (69)/
31(12) | | NA | | | NA | 223 (86) | 259 (100) |
| Sorafenib
(n=253) | 253 (114) | 60 | 113 (45) | 139 (55) | 1 (<1) | 44 (17)/177 (70)/
32 (13) | | | | | | 219 (87) | 253 (100) |
| Motzer et
al, 2013 (25) | Pazopanib
(n=557) | NA | NA | | NA | | NA | | NA | | | NA | NA | NA |
| Sunitinib
(n=553) | | | | | | | | | | | | | |
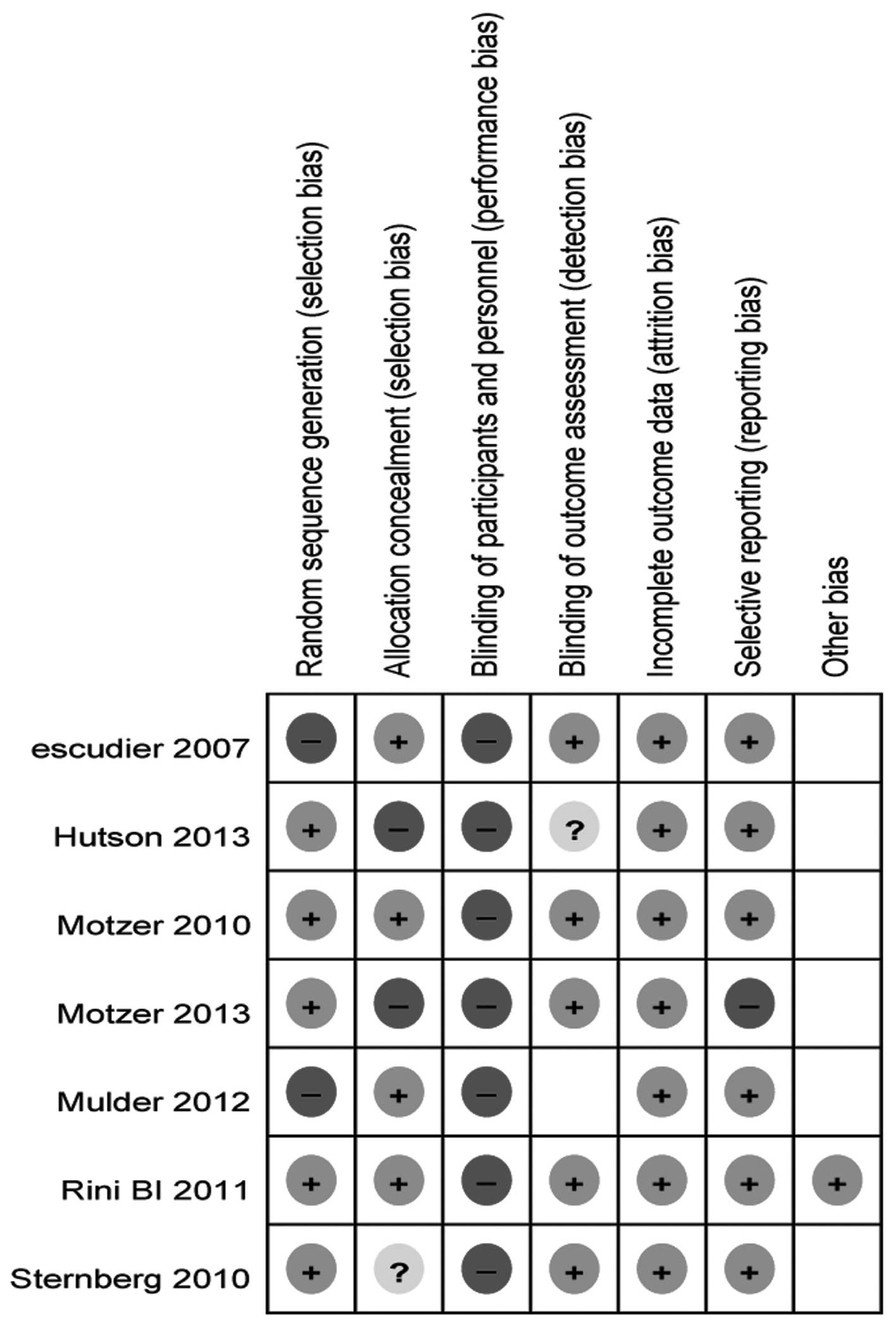
Quality assessment
The evaluation of the risk of each bias for the 7
selected RCTs is summarized in Fig.
2.
A total of 28.6% (2/7) of the trials described the
method used to generate the allocation sequence in sufficient
detail to allow an assessment of this item. A total of 57.1% (4/7)
of the trials had allocation concealment. No studies were
completely blinded and the participants were allowed to be
open-label when they exhibited progression during treatment. A
total of 57.1% (4/7) of the trials reported blinded outcome
assessors. Withdrawal or dropouts were reported in 85.7% (6/7) of
the trials (19–25). All the studies were found to have a
low risk of bias for selective outcome reporting. In these studies,
all expected outcomes were reported, including important side
effects and those outcomes that were pre-specified in Materials and
methods. All the included studies reported that adverse events were
actively monitored; therefore, the risk of bias was considered to
be low.
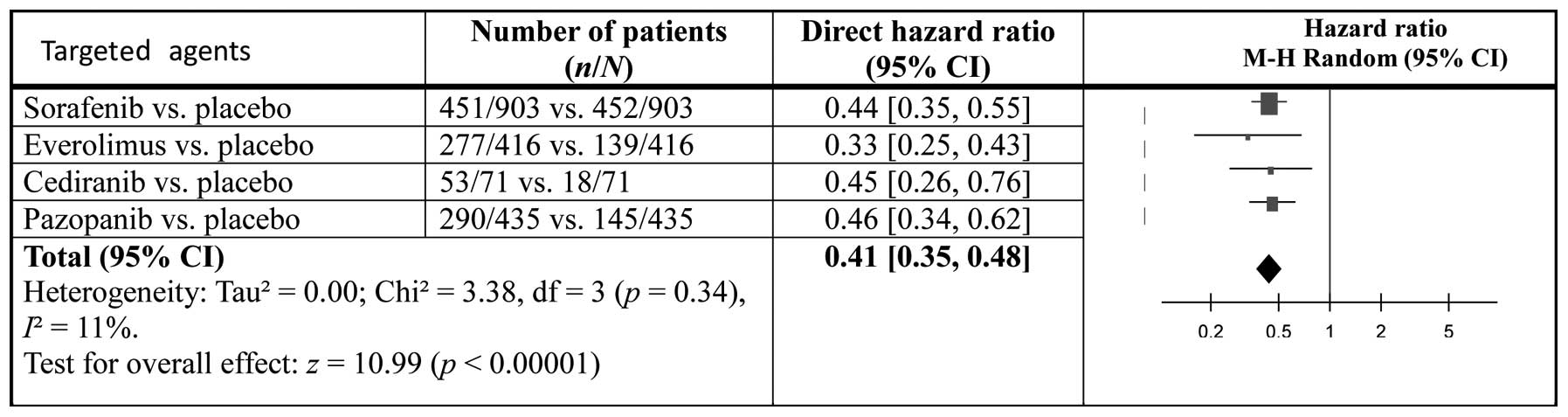
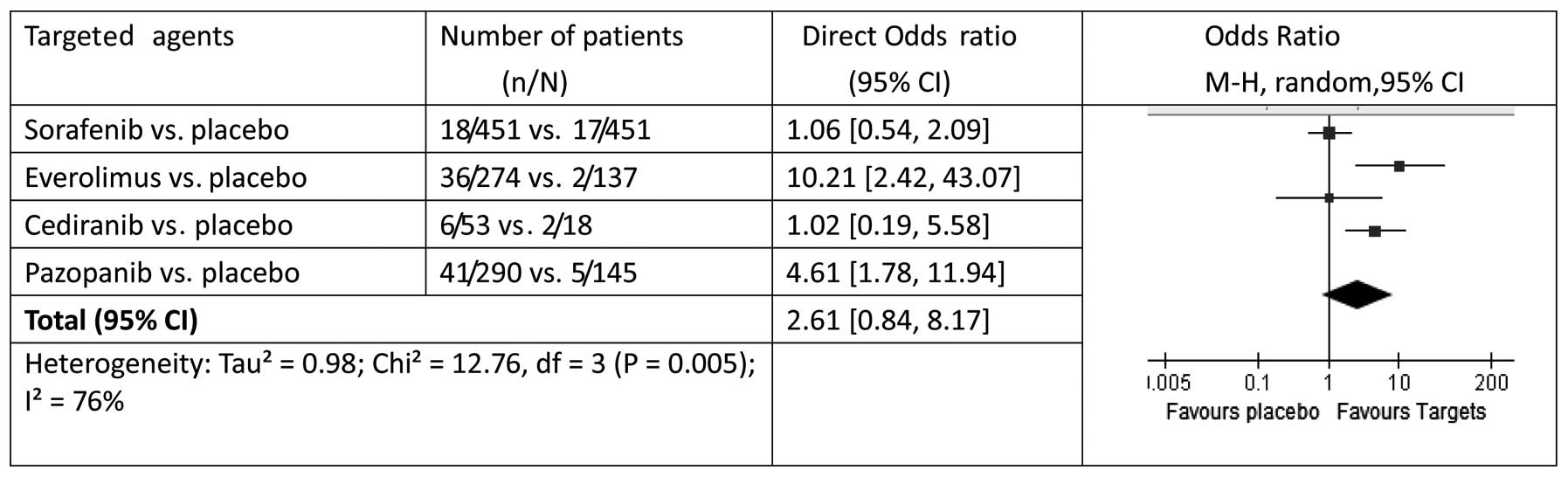
Direct comparison of treatment effects
(targeted agents vs. placebo)
The network graph and forest plot were drawn to
graphically display the results of the available direct comparisons
between treatments (Figs. 3 and
4). The outcome data were
extracted from the 7 selected RCTs including a total of 3,390
patients (Table I). The 7 newer
targeted agents achieved a statistically significant improvement in
PFS compared to placebo, with a non-significant higher risk of
adverse events (Fig. 4).
Indirect comparisons of treatment
effects
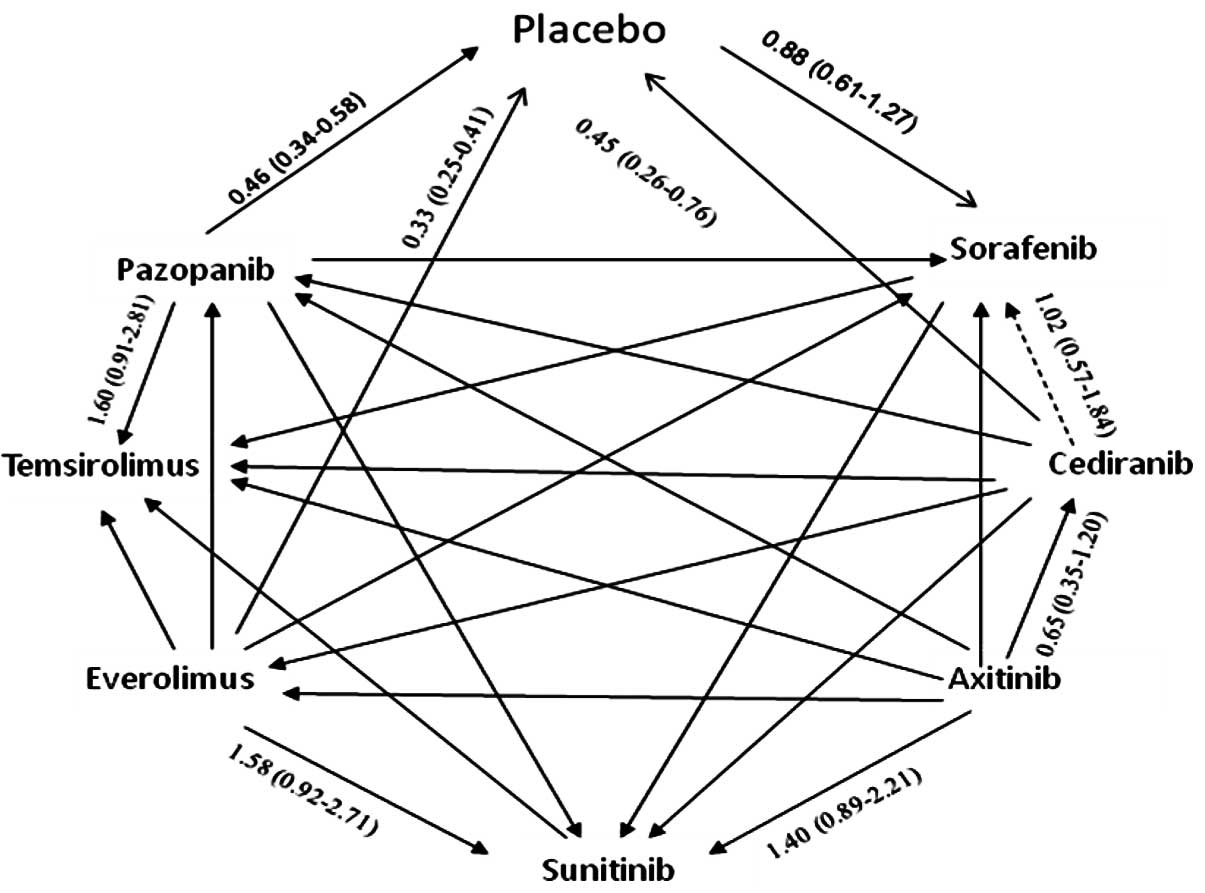
The network graph in Fig. 5 shows the results of our network
meta-analysis for comparisons of efficacy among the 7 newer
targeted agents for the treatment of mRCC. Specifically, as listed
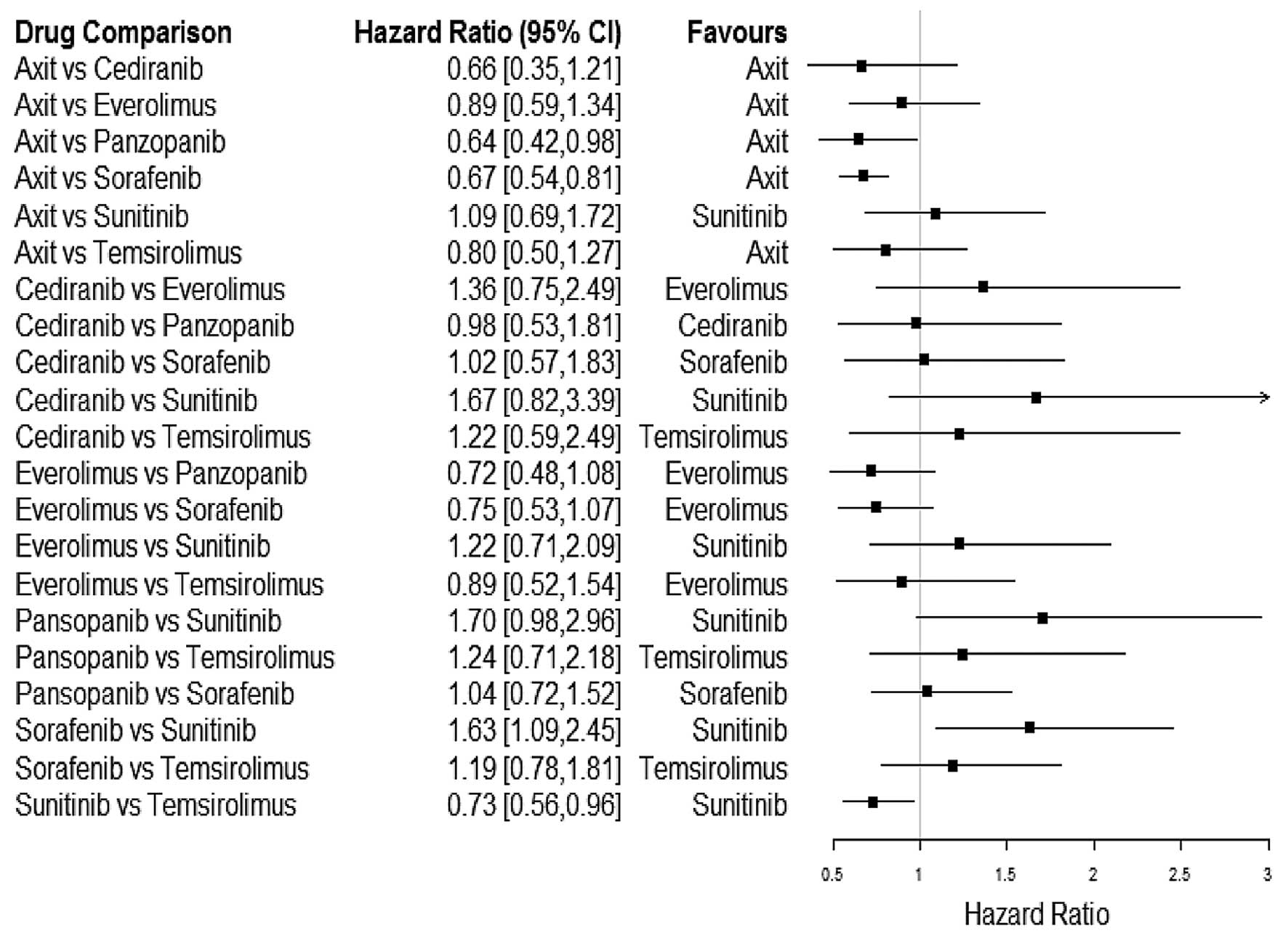
in the forest plots in Fig. 6,
axitinib exhibited significantly improved efficacy compared to
panzopanib [HR=0.64, 95% confidence interval (CI): 0.42–0.98] and
sorafenib (HR=0.67, 95% CI: 0.54–0.81); sunitinib was superior to
sorafenib (HR=1/1.63=0.61, 95% CI: 1/2.45–1/1.09) and temsirolimus
(HR=0.73, 95% CI: 0.56–0.96) regarding the efficacy outcome.
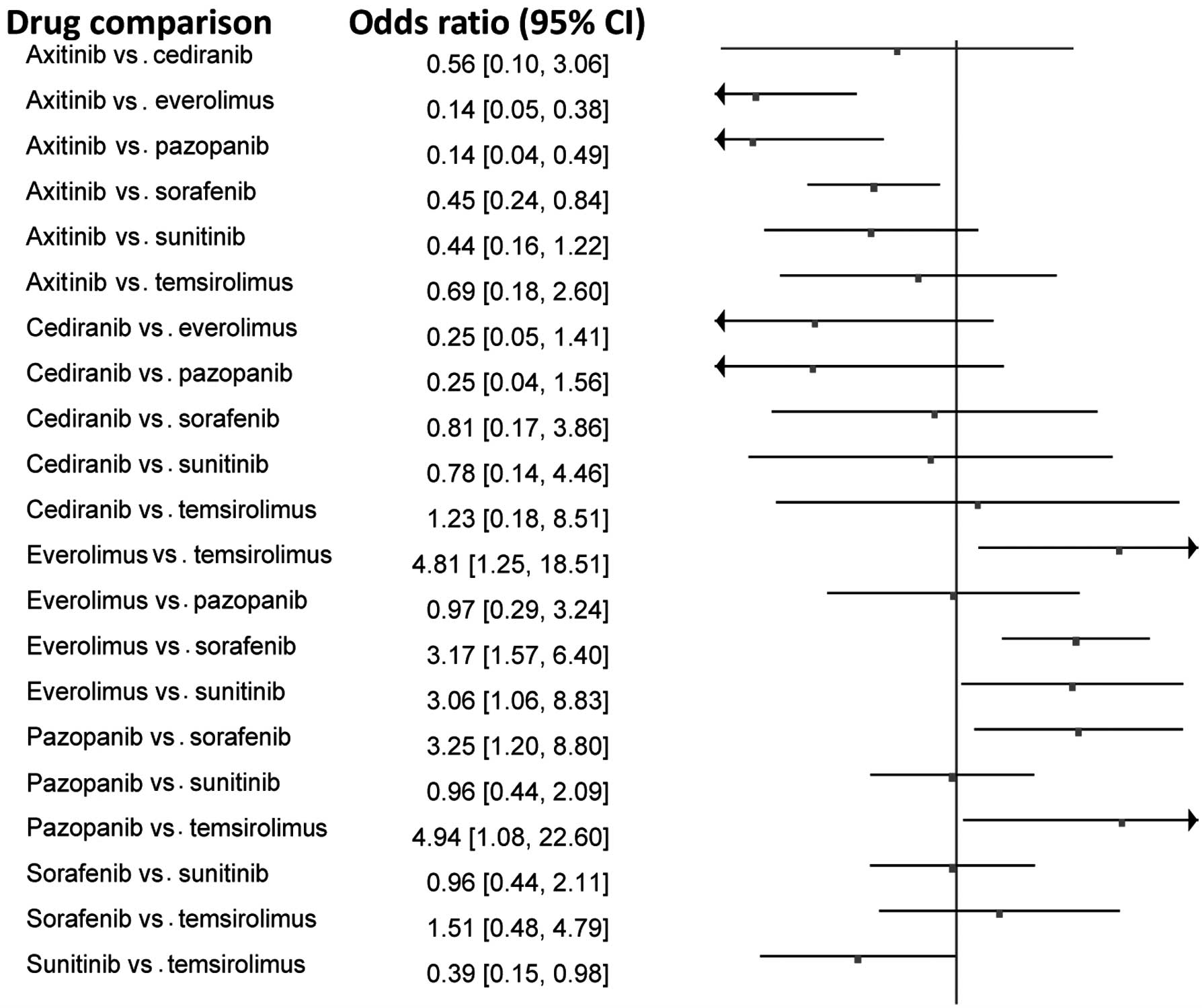
We also conducted a network meta-analysis for
comparisons of safety among the 7 newer targeted agents, which did
not reveal any statistically significant differences in the number
of withdrawals of adverse events (Fig.
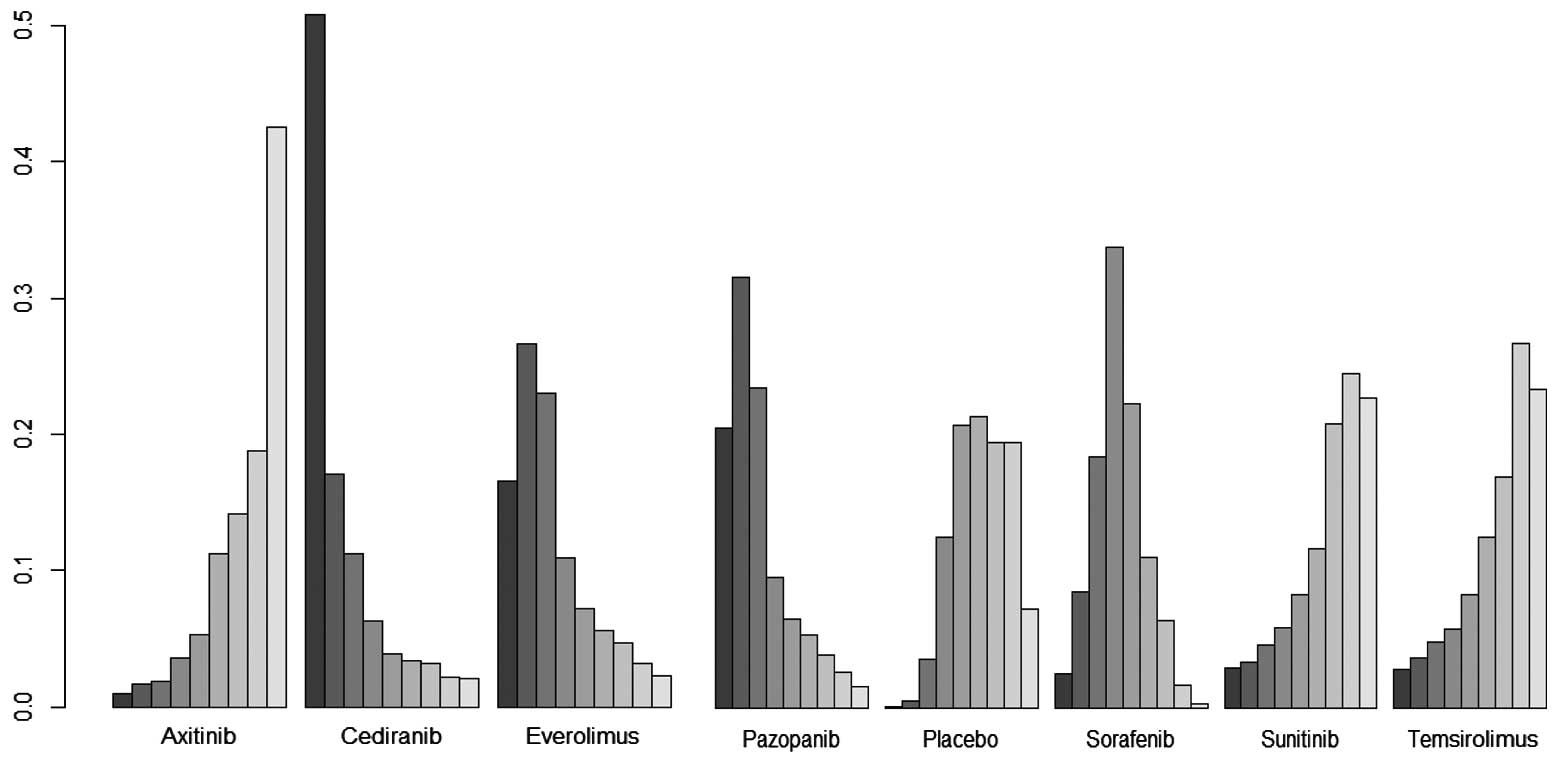
7). As shown in Fig. 8, the
ranking probabilities of the competing treatments and placebo from
the network meta-analysis of safety indicated that, of the 7 newer
targeted agents, axitinib was likely to be associated with the
lowest risk of withdrawals due to adverse events; conversely,
cediranib was associated with the highest risk of withdrawals due
to adverse events.
Discussion
The future trend in the treatment of RCC is the
introduction of novel agents that may prove more efficacious in the
prolongation of PFS and cause fewer adverse events compared to the
conventional systematic cytokine therapy. The 7 investigated
targeted agents (sorafenib, sunitinib, temsirolimus, everolimus,
pazopanib, axitinib and cediranib) have been approved by the Food
and Drug Administration in the United States and Europe. The lack
of head-to-head studies comparing these targeted agents in either
the first- or second-line treatment is the major weak point in
evidence-based medicine. Three head-to-head trials comparing two
targeted agents were recently completed; however, only the AXIS
study has published its results (23). More direct head-to-head studies
comparing two targeted agents are likely to be developed in the
future based on the current trial’s results. Therefore, we
performed this network meta-analysis on efficacy and safety by
using the available data from clinical trials in order to provide
patients and clinical practitioners with currently available
information and enable the selection of an effective and safe
treatment.
The results of this network indirect analysis
suggest that axitinib is a more suitable targeted therapy option to
prolong PFS after failure of the first-line treatment of mRCC.
Additionally, the findings of this analysis also suggested that
sunitinib is superior to sorafenib. This finding is consistent with
those from two recently published indirect comparison studies,
which indicated that sunitinib was superior to sorafenib (HR=0.58,
95% CI: 0.38–0.86, P<0.001; and HR=0.47, 95% CI: 0.316–0.713,
P<0.001) in the treatment of mRCC (26,27).
The results of our meta-analysis also indicated that axitinib
exhibits a higher efficacy and safety compared to sorafenib and
pazopanib in patients who previously received systematic treatment.
This finding is also in line with a recent systematic review and
meta-analysis for second-line treatments in the management of
advanced RCC (28). The authors of
that study reported that axitinib was superior to placebo (HR=0.25,
95% CI: 0.17–0.38) or sorafenib (HR=0.46, 95% CI: 0.32–0.68) and
pazapanib (HR=0.47, 95% CI: 0.26–0.85) in prolonging PFS.
Targeted agents are associated with a distinct
pattern of adverse events in mRCC, with the specific profiles and
relative severities varying by agent. The development of practical
adverse event management techniques to enable patients to achieve
the greatest benefit from treatment is an increasing concern. In
this study, we demonstrated that axitinib is the least likely to be
associated with adverse events among the 7 newer targeted agents, a
finding supported by the recent published AXIS study. That study
reported that axitinib was better tolerated compared to other
targeted agents, with a lower incidence of the adverse events often
seen with the currently approved targeted agents, such as
erythrodysaesthesia, cutaneous toxicities and myelosuppression
(23).
The cost of targeted therapy regimens is on the
increase as targeted agents are constantly developed. The
incremental cost for a life-year gained is 70,000 pounds for
sorafenib (29) 67,000 USD for
sunitinib and 90,000 pounds for temsirolimus (30). The cost of newer targeted agents is
also increasing in our country. Therefore, we must select the most
cost-effective and best tolerated drugs to treat patients in order
to conserve the limited medical resources.
There are some strengths and limitations to consider
when interpreting our analysis. The strengths of our analysis
include synthesizing data and comparing the efficacy and safety of
all 7 newer targeted agents using the relatively new approach of
network meta-analysis. We systematically extracted data from the
published RCTs and investigated the risk of bias of the included
studies in accordance with the Cochrane Handbook published in 2011
(31). In addition, patients with
mRCC did not undergo previous interventions other than systematic
therapy and no study assessed the relative effectiveness of each
new targeted agent. Our study aimed to provide preliminary
comparative results of these newer targeted agents to patients and
clinical practitioners to enable selection of the optimal targeted
agents.
There were some limitations to our meta-analysis.
First, those 7 targeted agents have been available over a
relatively short period of time; thus, the duration of the trials
was not sufficient to assess the long-term benefits and risks.
Moreover, some heterogeneity and reporting bias existed in the
identified RCTs, which is likely to affect the results of this
study. Second, unpublished data were excluded in the search
strategy; therefore, publication bias may exist in this analysis.
Third, we used the GRADE method to assess and grade the quality of
the evidence; however, the grading process entirely depends on the
reviewer’s personal judgment and, therefore, the quality may be
underestimated.
In conclusion, the results of this network analysis
indicated that sunitinib and axitinib may offer some clinical
benefit superior to that of sorafenib, pazopanib and temsirolimus.
Axitinib was associated with the lowest risk of withdrawals due to
adverse events. This summary of evidence may provide preliminary
data regarding the efficacy and safety of targeted agents to
physicians and patients enabling the design of evidence-based
treatment strategies for mRCC.
References
|
1
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Thun MJ, Ries LA, et al: Annual
report to the nation on the status of cancer, 1975–2005, featuring
trends in lung cancer, tobacco use, and tobacco control. J Natl
Cancer Inst. 100:1672–1694. 2008.
|
|
3
|
Mathew A, Devesa SS, Fraumeni JF Jr and
Chow WH: Global increases in kidney cancer incidence, 1973–1992.
Eur J Cancer Prev. 11:171–178. 2002.PubMed/NCBI
|
|
4
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar
|
|
5
|
Taiwan Cancer Registry. http://tcr.cph.ntu.edu.tw/main.php?Page=N1.
Accessed June 21, 2012
|
|
6
|
Gupta K, Miller JD, Li JZ, Russell MW and
Charbonneau C: Epidemiologic and socioeconomic burden of metastatic
renal cell carcinoma (mRCC): a literature review. Cancer Treat Rev.
34:193–205. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Athar U and Gentile TC: Treatment options
for metastatic renal cell carcinoma: a review. Can J Urol.
15:3954–3966. 2008.PubMed/NCBI
|
|
8
|
Shih YC, Chien CR, Xu Y, Pan IW, Smith GL
and Buchholz TA: Economic burden of renal cell carcinoma: Part I -
an updated review. Pharmacoeconomics. 29:315–329. 2011.PubMed/NCBI
|
|
9
|
Finley DS, Pantuck AJ and Belldegrun AS:
Tumor biology and prognostic factors in renal cell carcinoma.
Oncologist. 16(Suppl 2): 4–13. 2011. View Article : Google Scholar
|
|
10
|
Schünemann H, Brozek J and Oxman A: GRADE
handbook for grading quality of evidence and strength of
recommendation, version 3.2 (updated March 2009). The GRADE Working
Group. http://ims.cochrane.org/revman/gradepro.
Accessed June 21, 2012
|
|
11
|
Higgins JPT and Green S: Cochrane Handbook
for Systematic Reviews of Interventions, version 5.0.0. The
Cochrane Collaboration; 2008, View Article : Google Scholar
|
|
12
|
Lumley T: Network meta-analysis for
indirect treatment comparisons. Stat Med. 21:2313–2324. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lu G and Ades AE: Combination of direct
and indirect evidence in mixed treatment comparisons. Stat Med.
23:3105–3124. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Review Manager (RevMan) computer program,
version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane
Collaboration; 2013
|
|
15
|
Bucher HC, Guyatt GH, Griffith LE and
Walter SD: The results of direct and indirect treatment comparisons
in meta-analysis of randomized controlled trials. J Clin Epidemiol.
50:683–691. 1997. View Article : Google Scholar
|
|
16
|
Caldwell DM, Ades AE and Higgins JP:
Simultaneous comparison of multiple treatments: combining direct
and indirect evidence. BMJ. 331:897–900. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wells GA, Sultan SA, Chen L, Khan M and
Coyle D: Indirect Treatment Comparisons (ITC) computer program,
version 1.0. Ottawa: Canadian Agency for Drugs and Technologies in
Health; 2009
|
|
18
|
R Development Core Team. R: A Language and
Environment for Statistical Computing. R Foundation for Statistical
Computing; Vienna, Austria: http://www.R-project.org/.
Accessed August 14, 2013
|
|
19
|
Escudier B, Eisen T, Stadler WM, et al:
TARGET Study Group: Sorafenib in advanced clear-cell renal-cell
carcinoma. N Engl J Med. 356:125–134. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Motzer RJ, Escudier B, Oudard S, et al:
RECORD-1 Study Group: Phase 3 trial of everolimus for metastatic
renal cell carcinoma: final results and analysis of prognostic
factors. Cancer. 116:4256–4265. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sternberg CN, Davis ID, Mardiak J, et al:
Pazopanib in locally advanced or metastatic renal cell carcinoma:
results of a randomized phase III trial. J Clin Oncol.
28:1061–1068. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mulders P, Hawkins R, Nathan P, et al:
Cediranib monotherapy in patients with advanced renal cell
carcinoma: results of a randomised phase II study. Eur J Cancer.
48:527–537. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rini BI, Escudier B, Tomczak P, Kaprin A,
Szczylik C, Hutson TE, et al: Comparative effectiveness of axitinib
versus sorafenib in advanced renal cell carcinoma (AXIS): a
randomised phase 3 trial. Lancet. 378:1931–1939. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hutson TE, Escudier B, Esteban E, et al:
Randomized phase III trial of temsirolimus versus sorafenib as
second-line therapy after sunitinib in patients with metastatic
renal cell carcinoma. J Clin Oncol. 32:760–767. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Motzer RJ, Hutson TE, Cella D, et al:
Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N
Engl J Med. 369:722–731. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mills EJ, Rachlis B, O’Regan C, et al:
Metastatic renal cell cancer treatments: an indirect comparison
meta-analysis. BMC Cancer. 9:342009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Leung HW and Chan AL: Multikinase
inhibitors in metastatic renal cell carcinoma: indirect comparison
meta-analysis. Clin Ther. 33:708–716. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Larkin J, Paine A, Tumur I, Cappelleri JC,
Healey PJ Sr, Foley G, Mitchell S, Kroes M and Chen C: Second-line
treatments for the management of advanced renal cell carcinoma:
systematic review and meta-analysis. Expert Opin Pharmacother.
14:27–39. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hoyle M, Green C, Thompson-Coon J, Liu Z,
Welch K, Moxham T and Stein K: Cost-effectiveness of sorafenib for
second-line treatment of advanced renal cell carcinoma. Value
Health. 13:55–60. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Hoyle M, Green C, Thompson-Coon J, Liu Z,
Welch K, Moxham T and Stein K: Cost-effectiveness of temsirolimus
for first-line treatment of advanced renal cell carcinoma. Value
Health. 13:61–68. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Higgins JPT and Green S: Cochrane Handbook
for Systematic Reviews of Interventions, version 5.1.0. The
Cochrane Collaboration; 2011
|