Introduction
Trimodality therapy consisting of induction
chemoradiotherapy (CRT) followed by surgery is a potential
treatment option for locally advanced non-small-cell lung cancer
(NSCLC). Two randomized phase III trials investigated the
prognostic effect of surgery following induction CRT in patients
with mediastinal lymph nodal metastasis (1,2). Although
these studies failed to demonstrate a benefit from the addition of
surgery in the overall patient population, the subset analysis of
the intergroup trial 0139 indicated that surgical resection
following induction CRT was beneficial for those who did not
undergo pneumonectomy, strongly suggesting the significance of
appropriate patient selection (2).
Thus, identifying factors for selecting patients likely to benefit
from trimodality therapy is crucial for determining the optimal
therapeutic strategy.
Clinical factors estimated prior to therapy
initiation are potential predictors of poor patient outcome. Among
these factors, lower lobe tumor origin was reported by several
investigators to be associated with an unfavorable prognosis in
surgically treated patients (3–5). However,
controversial results, obtained from patients with early-stage
NSCLC, suggested that there is no prognostic difference according
to tumor location (6).
In this study, we retrospectively investigated the
prognostic significance of tumor location in NSCLC patients with
clinical (c) N2/3 disease receiving trimodality therapy.
Patients and methods
Patients
Induction CRT has been used for locally advanced
NSCLC in Okayama University Hospital since 1998 (7,8). Among the
102 NSCLC patients who underwent induction CRT followed by surgery
between January, 1999 and November, 2011 at our institution, 76
patients with cN2/3 stage III disease were enrolled in this
retrospective study. The medical records of the NSCLC patients who
had undergone induction CRT followed by surgery were reviewed.
Staging was performed according to the International Association of
the Study of Lung Cancer TNM staging system for NSCLC, 7th edition
(9). Disease stage was determined
using chest radiography, enhanced chest and abdominal computed
tomography (CT) scans, enhanced brain magnetic resonance imaging
(MRI), radionuclide bone scan or 18-fluoro-2-deoxyglucose positron
emission tomography-CT scan and bronchoscopy. The regional
mediastinal lymph nodes for each lobe were defined as follows:
Right upper lobe (RUL) for superior mediastinal nodes, right middle
lobe (RML) for superior mediastinal and subcarinal nodes, right
lower lobe (RLL) for subcarinal and inferior mediastinal nodes,
left upper lobe (LUL) for superior mediastinal nodes and left lower
lobe (LLL) for subcarinal and inferior mediastinal nodes.
Metastatic lymph nodes extending over regional nodes were defined
as beyond regional. Staging cervical mediastinoscopy was undertaken
in a proportion of patients to evaluate bilateral node stations. 2
and 4 and subcarinal station 7.
This study was approved by the Institutional Review
Board/Ethics Committee of Okayama University, Okayama, Japan.
Induction therapy, surgery and
adjuvant treatment
Induction CRT was performed as previously described
(7). Briefly, docetaxel (40
mg/m2) was administered intravenously followed by
cisplatin (40 mg/m2) prior to radiotherapy on days 1 and
8. Chemotherapy was repeated with a 3- or 4-week interval.
Radiotherapy was initiated on the first day of chemotherapy using a
6–10 MV linear accelerator. A total radiation dose of 40–60 Gy was
planned using a conventional fractionation protocol (2 Gy/day). The
original volume included the primary tumor site, with a margin of 2
cm around the mass, the ipsilateral hilum and the entire width of
the mediastinum, with a margin of 1 cm around the radiographically
visible region of involvement, extending inferiorly to 2 cm below
the carina or 2 cm below the radiographically identified tumor
mass. Following induction CRT, the patients were evaluated for
response to treatment. Patients without progressive disease (PD)
and/or in good general condition proceeded to undergo surgery.
The surgical procedure was determined based on the
extent of the disease prior to induction therapy. Resection with
reconstruction of the chest wall or major vessels was performed
when necessary. The bronchial stump was covered with pericardial
fat tissue or an intercostal muscle pedicle. When a sleeve
resection was performed, the greater omentum was used to wrap the
anastomosis. Although posterolateral thoracotomy was the basic
approach, a median sternotomy or a trap-door approach was employed
for patients with supraclavicular or contralateral mediastinal
lymph node metastasis, or when securing great vessels, such as the
main pulmonary artery, was required to ensure safe resection.
Complete ipsilateral superior mediastinal and subcarinal lymph node
dissection was routinely undertaken. For patients with primary
lower lobe lesions, the lymph nodes of stations 8 and 9 were also
resected. Postoperative treatment was left to the primary
physician′s discretion.
Estimation
Radiological response was assessed using the Eastern
Cooperative Oncology Group (ECOG) criteria with certain
modifications, as previously reported, and was classified as
complete response (CR), partial response (PR), stable disease (SD)
and PD (7,10). The anastomotic complications included
bronchopleural or bronchovascular fistula, bleeding, bronchial
stenosis and malacia. As part of the routine follow-up care, chest
and abdominal CT and enhanced brain MRI examination were repeated
every 3 months for at least the first 2 years and every 6 months
during the 3–5 years following completion of the trimodality
therapy.
Statistical analysis
The overall survival (OS) and disease-free survival
(DFS) were calculated from the date of the initiation of induction
CRT until the date of death or the last follow-up for OS and until
confirmed death from any cause or disease recurrence at a local or
distant site for DFS. Locoregional recurrence was defined as that
developing in the ipsilateral chest or mediastinum and distant
recurrence as that developing in any other location.
The Wilcoxon rank-sum test and the Fisher′s exact
test were used to compare the differences between two groups, as
appropriate. A univariate analysis of OS and DFS was performed
using the Kaplan-Meier method with the log-rank test. All the data
were analyzed using JMP software, version 9.0.0 (SAS Institute
Inc., Cary, NC, USA). The statistical tests were two-sided and
P<0.05 was defined as indicating statistically significant
differences.
Results
Patient characteristics
Between January, 1999 and November, 2011, a total of
102 NSCLC patients underwent surgery following CRT at the Okayama
University Hospital. Patients with Pancoast tumors or cN0/1 disease
were excluded. As a result, 76 patients with cN2/3 disease were
enrolled in this retrospective study. The patient characteristics
are summarized in Table I. The median
patient age was 60 years (range, 31–76 years). The 76 patients
included 53 men and 23 women, 43 with adenocarcinomas and 33 with
non-adenocarcinomas. Of the 76 patients, 44 had stage IIIA and 32
had stage IIIB disease. The primary tumors were located in the RUL
(N=33), RML (N=5), RLL (N=11), LUL (N=20) and LLL (7 patients).
Mediastinal lymph node metastasis was pathologically confirmed in
36 patients by mediastinoscopy or endobronchial ultrasound-guided
transbronchial biopsy prior to induction CRT.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Variables | Patient no.
(n=76) | Non-lower lobe
(n=58) | Lower lobe
(n=18) | P-value |
|---|
| Median age (years),
range | 60, 31–76 | 60, 31–76 | 60, 43–74 | 0.47 |
| Gender |
|
|
|
|
|
Male/female | 53/23 | 41/17 | 12/6 | 0.77 |
| Smoking history |
|
|
| 0.10 |
|
Non-smoker/smoker | 17/59 | 10/48 | 7/11 |
|
| Histology |
|
|
|
|
|
Ad/Sq/AdSq/LC | 43/30/1/2 | 33/22/1/2 | 10/8/0/0 | 0.78 |
| Tumor location |
|
|
|
|
|
RUL/RML/RLL/LUL/LLL | 33/5/11/20/7 | – | – | – |
| cN |
|
|
|
|
|
N2/N3 | 66/10 | 49/9 | 17/1 | 0.44 |
| cN2/3 |
|
|
|
|
|
Single/multiple stations | 43/33 | 33/25 | 10/8 | 1.00 |
| cN2/3 |
|
|
|
|
|
Regional/beyond regional
nodes | 53/23 | 46/12 | 7/11 | 0.0016a |
| cStage |
|
|
|
|
|
IIIA/IIIB | 44/32 | 30/28 | 14/4 | 0.060 |
| Median radiation dose
(Gy), range | 46, 18.63 | 46, 30.63 | 46, 8.54 | 0.42 |
| Completion of
induction treatment |
|
|
|
|
|
Yes/no | 49/27 | 36/22 | 13/5 | 0.58 |
| Radiological
response |
|
|
|
|
|
CR/PR/SD/PD | 1/35/40/0 | 1/26/31/0 | 0/9/9/0 | 0.72 |
| Operation |
|
|
|
|
| Not
pneumonectomy/pneumonectomy | 71/5 | 54/4 | 17/1 | 1.00 |
| Severe postoperative
complicationsb |
|
|
|
|
|
Yes/no | 4/72 | 2/56 | 2/16 | 0.24 |
| Pathological response
(primary lesion)c |
|
|
|
|
|
0/1/2/3 | 1/14/30/31 | 1/8/25/24 | 0/6/5/7 | 0.22 |
| pN |
|
|
|
|
|
0/1/2/3 | 44/3/23/6 | 35/2/19/2 | 9/1/4/4 | 0.12 |
| pCR |
|
|
|
|
|
Yes/no | 22/54 | 18/40 | 4/14 | 0.56 |
| Adjuvant therapy |
|
|
|
|
|
Yes/no | 30/46 | 25/33 | 5/13 | 0.28 |
| Recurrence |
|
|
|
|
|
Yes/no | 32/44 | 19/39 | 13/5 | 0.0054a |
Trimodality therapy
Of the 76 patients, 49 had completed the planned
induction CRT without dose reduction of chemotherapy or
radiotherapy. The toxicities were similar to those previously
described (7). The median radiation
dose was 46 Gy. The radiological response was CR in 1 patient
(1.3%), PR in 35 (46.1%) and SD in 40 (52.6%), whereas there were
no reported cases of PD (Table I).
Lobectomy was performed in 54 patients, sleeve lobectomy in 10,
bilobectomy in 7 and pneumonectomy in 5 patients. All the patients
underwent complete resection, with a negative bronchial margin
confirmed by frozen section. The median postoperative hospital stay
was 23 days. Severe postoperative pulmonary complications,
including anastomotic complications and empyema, occurred in 4
patients. There was no reported trimodality treatment-related
mortality.
Lobe-specific treatment response and
survival
The patient characteristics and response to
treatment in patients with non-lower lobe and lower lobe tumors are
presented in Table I. There was a
significant difference in the incidence of beyond regional nodal
metastasis between non-lower lobe and lower lobe tumors. Lower lobe
tumors were associated with a higher incidence of beyond regional
nodal metastasis compare to non-lower lobe tumors (61.1 vs. 20.7%,
respectively; P=0.0016). Radiological responses (CR or PR) were
documented in 27 (46.6%) of the patients with non-lower lobe and 9
(50.0%) of those with lower lobe tumors (P=0.72). Severe
postoperative complications, including empyema and anastomotic
complications, occurred in 2 patients (3.4%) with non-lower lobe
and 2 (1.1%) with lower lobe tumors (P=0.24). Adjuvant treatment
was administered to 25 patients (43.1%) with non-lower lobe and 5
(27.8%) with lower lobe tumors (P=0.28).
At the time of data analysis in June, 2013, the
5-year OS and DFS were 69.4 and 53.5%, respectively. The median
follow-up period was 64 months. To clarify pre- and post-treatment
prognostic factors, we separately analyzed pretreatment and
treatment-related prognostic factors. The significant pretreatment
prognostic factor for OS were found to be tumor location and
presence of beyond regional nodal metastases. The significant
prognostic factors for DFS were tumor location, cN stage and
presence of beyond regional nodal metastases (Table II). Among the treatment-related
factors, there was no significant prognostic factor for OS, whereas
radiological response was the only significant prognostic factor
for DFS.
| Table II.Prognostic factors. |
Table II.
Prognostic factors.
| Variables | Patient no.
(n=76) | 5-year OS rate
(%) | P-value | 5-year DFS rate
(%) | P-value |
|---|
| Pretreatment
variables |
|
|
|
|
|
| Age
(years) |
|
|
|
|
|
|
≤60/60> |
41/35 |
68.2/71.6 | 0.92 |
50.2/57.8 | 0.81 |
|
Gender |
|
|
|
|
|
|
Male/female |
53/23 |
67.0/71.7 | 0.35 |
57.9/43.9 | 0.20 |
| Smoking
history |
|
|
|
|
|
|
Non-smoker/smoker |
17/59 |
70.6/69.3 | 0.62 |
36.8/58.3 | 0.15 |
|
Histology |
|
|
|
|
|
|
Ad/non-Ad |
43/33 |
67.8/69.2 | 0.55 |
41.0/67.7 | 0.19 |
| Tumor
location |
|
|
|
|
|
|
Non-lower/lower
lobe |
58/18 |
77.0/37.9 | 0.022a |
64.4/20.1 | 0.0007a |
| cN |
|
|
|
|
|
|
2/3 |
66/10 |
72.6/49.2 | 0.075 |
59.0/14.6 | 0.050a |
|
c-N2/3 |
|
|
|
|
|
|
Single/multiple
stations |
43/33 |
79.2/65.0 | 0.18 |
63.1/41.3 | 0.055 |
|
cN2/3 |
|
|
|
|
|
|
Regional/beyond
regional nodes |
53/23 |
77.7/48.9 | 0.037a |
68.0/18.6 | 0.0014a |
|
cStage |
|
|
|
|
|
|
IIIA/IIIB |
44/32 |
72.1/64.9 | 0.17 |
50.6/57.0 | 0.74 |
| Treatment-related
variables |
|
|
|
|
|
|
Completion of induction
CRT |
|
|
|
|
|
|
Yes/no |
49/27 |
71.3/66.5 | 0.38 |
53.2/54.6 | 0.92 |
|
Radiological response |
|
|
|
|
|
|
CR or PR/SD |
36/40 |
76.8/61.7 | 0.15 |
71.5/36.4 | 0.0015a |
|
Operation |
|
|
|
|
|
|
Not
pneumonectomy/pneumonectomy |
71/5 |
71.3/40.0 | 0.054 |
53.1/60.0 | 0.92 |
| Severe
postoperative complicationsb |
|
|
|
|
|
|
Yes/no |
4/72 |
NR/70.9 | 0.18 |
NR/54.7 | 0.50 |
|
Pathological response (primary
lesion)c |
|
|
|
|
|
|
3/0–2 |
31/45 |
73.0/66.0 | 0.98 |
65.0/45.2 | 0.29 |
| pN |
|
|
|
|
|
|
0.1
(downstaged)/2–3 (not downstaged) |
47/29 |
81.8/49.7 | 0.082 |
59.4/43.8 | 0.13 |
|
pCR |
|
|
|
|
|
|
Yes/no |
22/54 |
80.5/64.5 | 0.72 |
62.2/49.1 | 0.64 |
|
Adjuvant therapy |
|
|
|
|
|
|
Yes/no |
30/46 |
69.1/71.5 | 0.62 |
44.8/60.6 | 0.54 |
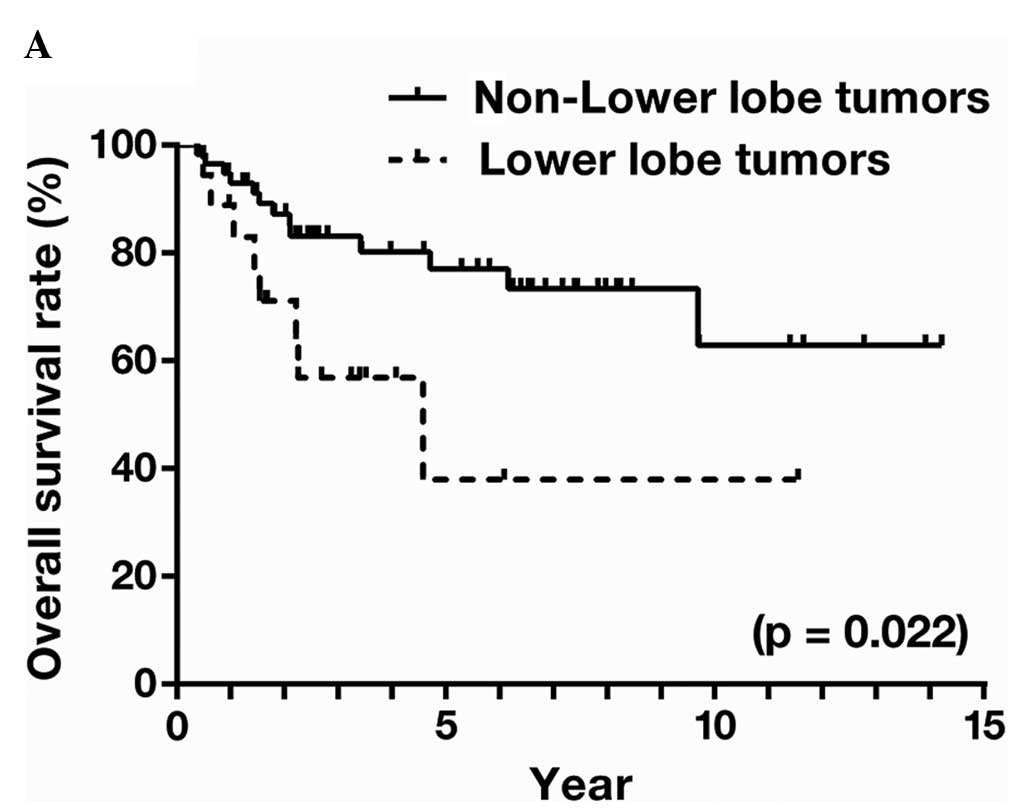
For the entire patient group, lower lobe tumors were
associated with significantly shorter OS and DFS compared to other
locations (OS, P=0.022; and DFS, P=0.0007; Fig. 1A and B). The respective 5-year OS and
DFS were 77.0 and 64.4% for non-lower lobe tumors and 37.9 and
20.1% for lower lobe tumors. The disease relapsed as distant
metastasis in 14 and locoregional recurrence in 5 patients with
non-lower lobe tumors and as distant metastasis in 11 and
locoregional recurrence in 2 patients with lower lobe tumors
(P=0.67).
When the analysis was limited to pathologically
proven N2/3 disease prior to induction CRT (n=36), patients with
lower lobe tumors tended to have an unfavorable OS (P=0.068) and
DFS (P=0.0075) compared to those with non-lower lobe tumors
(Table III). The respective 5-year
OS and DFS were 80.4 and 66.0% in patients with non-lower lobe
tumors and 38.1 and 14.3% in those with lower lobe tumors.
| Table III.Prognostic factors limited to
pathologically proven N2/3 disease. |
Table III.
Prognostic factors limited to
pathologically proven N2/3 disease.
| Variables | Patient no.
(n=36) | 5-year OS rate
(%) | P-value | 5-year DFS rate
(%) | P-value |
|---|
| Pretreatment
variables |
|
|
|
|
|
| Age
(years) |
|
|
|
|
|
|
≤60/>60 |
19/17 |
80.9/61.6 | 0.15 |
52.9/57.4 | 0.63 |
|
Gender |
|
|
|
|
|
|
Male/female |
24/12 |
66.1/80.0 | 0.18 |
55.7/58.3 | 0.95 |
| Smoking
history |
|
|
|
|
|
|
Non-smoker/smoker |
10/26 |
83.4/66.5 | 0.14 |
50.0/57.9 | 0.72 |
|
Histology |
|
|
|
|
|
|
Ad/non-Ad |
19/17 |
65.6/76.5 | 0.94 |
36.9/76.0 | 0.12 |
| Tumor
location |
|
|
|
|
|
|
Non-lower/lower
lobe |
29/7 |
80.4/38.1 | 0.068 |
66.0/14.3 | 0.0075a |
| cN |
|
|
|
|
|
|
2/3 |
33/3 |
69.7/100 | 0.38 |
55.8/50.0 | 0.64 |
|
cN2/3 |
|
|
|
|
|
|
Single/multiple
stations |
24/12 |
82.6/52.1 | 0.096 |
65.4/33.8 | 0.12 |
|
cN2/3 |
|
|
|
|
|
|
Regional/beyond
regional nodes |
29/7 |
77.1/47.6 | 0.37 |
64.1/NR | 0.097 |
|
cStage |
|
|
|
|
|
|
IIIA/IIIB |
27/9 |
67.0/85.7 | 0.76 |
53.0/64.8 | 0.75 |
| Treatment-related
variables |
|
|
|
|
|
|
Completion of induction
CRT |
|
|
|
|
|
|
Yes/no |
22/14 |
74.4/68.8 | 0.43 |
53.2/60.1 | 0.85 |
|
Radiological response |
|
|
|
|
|
|
CR/PR and SD |
12/24 |
81.8/65.1 | 0.19 |
73.3/44.5 | 0.075 |
|
Operation |
|
|
|
|
|
|
Not
pneumonectomy/pneumonectomy |
35/1 |
70.8/100 | 0.56 |
54.1/100 | 0.40 |
| Severe
postoperative complicationsb |
|
|
|
|
|
|
Yes/no |
0/36 |
−/71.8 | – |
−/55.7 | – |
|
Pathological response (primary
lesion)c |
|
|
|
|
|
|
3/0–2 |
12/24 |
83.3/65.4 | 0.62 |
40.4/83.3 | 0.10 |
| pN |
|
|
|
|
|
|
0.1
(downstaged)/2–3 (not downstaged) |
16/20 |
87.5/57.6 | 0.19 |
60.0/52.2 | 0.71 |
|
pCR |
|
|
|
|
|
|
Yes/no |
7/29 |
85.7/68.3 | 0.81 |
85.7/47.6 | 0.31 |
|
Adjuvant therapy |
|
|
|
|
|
|
Yes/no |
16/20 |
68.6/49.8 | 0.73 |
43.8/64.6 | 0.80 |
Discussion
In this study, we demonstrated that tumors arising
from the lower lobe were associated with a poor prognosis in
patients with locally advanced NSCLC treated with trimodality
therapy. The patient characteristics were similar between the two
groups and there were no significant differences in the effect of
induction CRT between patients with non-lower lobe tumors and those
with a lower lobe tumor origin.
One possible explanation for our results is that, at
the time of diagnosis, NSCLC patients with tumors arising from the
lower lobe had a more extensive disease than expected. Rocha et
al (11) demonstrated in their
prospective cohort study of 109 NSCLC patients that a lower lobe
location of the primary tumor was significantly associated with
upstaging following surgery for early-stage (cstage I/II) NSCLC.
Kudo et al (5) also reported
in their retrospective cohort study of 978 NSCLC patients that the
OS rates were similar between patients with LLL and those with
non-LLL tumors, regardless of stage, although the 5-year OS rates
were significantly poorer for LLL tumors compared to non-left lower
tumors among patients with lymph node metastasis. Indeed, our
results demonstrated that lower lobe tumors were associated with a
significantly higher incidence of beyond regional nodal metastases
compared to non-lower lobe tumors. In addition, it has been
reported that LLL tumors anatomically tend to metastasize to the
contralateral mediastinal nodes via subcarinal nodes more readily
compared to RLL tumors (12).
Considering these observations, the higher rate of lymph node
metastasis from lower lobe tumors possibly contributes to the
unfavorable prognosis in patients with such tumors among the
patient population with the same cstage, based on radiographic
evaluation. There was no significant difference in OS and DFS
between tumors originating in the right or left lower lobe. Our
findings, along with those of previous studies, also suggest that
tumor location may be a prognostic factor and it should be included
as a stratification factor in the design of randomized studies,
such as the intergroup trial 0139. Imbalanced distribution of tumor
location in each arm may significantly affect the outcome of
treatment in randomized studies.
There was no statistically significant difference in
the effects of induction CRT between non-lower lobe and lower lobe
tumors, although the latter were associated with a poorer
pathological CR rate (lower lobe vs. non-lower lobe tumors, 22.2
vs. 31.0%). Lower lobe tumors may generally be more affected by
respiratory movement during radiotherapy compared to non-lower lobe
tumors and the radiation fields may be wider in lower lobe compared
to those in non-lower lobe tumors (13). Although the exact reason is not known,
the difference in respiratory movement during radiation may be
responsible for the poor prognosis of patients with lower lobe
tumors.
The limitations of this study include its
retrospective nature and the small sample size, suggesting that a
significant selection bias may be present. In addition, N2/3 stage
was not confirmed pathologically prior to induction CRT and certain
cases were overestimated as advanced-stage. Therefore, we performed
an analysis limited to the 36 cases of pathologically proven N2/3
disease. There was a tendency of poor survival in patients with
lower lobe tumors compared to those with non-lower lobe tumors.
In conclusion, tumors arising from the lower lobes
of the lungs were found to be a poor prognostic factor in NSCLC
patients with N2/3 disease receiving trimodality therapy. Our
results suggest that, when designing randomized studies for locally
advanced NSCLC with mediastinal metastasis, particularly when
trimodality therapy is included in the protocol, the tumor location
should be considered as a stratification factor.
Acknowledgements
Katsuyuki Hotta has received honoraria from Chugai
Pharmaceutical, Eli Lilly Japan and Pfizer. Katsuyuki Kiura has
received honoraria from AstraZeneca, Chugai Pharmaceutical, Daiichi
Sankyo, Eli Lily, GlaxoSmithKline, Novartis, Sanofi-Aventis and
Taiho Pharmaceutical.
References
|
1
|
van Meerbeeck JP, Kramer GW, Van Schil PE,
et al: Randomized controlled trial of resection versus radiotherapy
after induction chemotherapy in stage IIIA-N2 non-small-cell lung
cancer. J Natl Cancer Inst. 99:442–450. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Albain KS, Swann RS, Rusch VW, et al:
Radiotherapy plus chemotherapy with or without surgical resection
for stage III non-small-cell lung cancer: a phase III randomised
controlled trial. Lancet. 374:379–386. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ichinose Y, Kato H, Koike T, et al:
Completely resected stage IIIA non-small cell lung cancer: the
significance of primary tumor location and N2 station. J Thorac
Cardiovasc Surg. 122:803–808. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ou SH, Zell JA, Ziogas A and Anton-Culver
H: Prognostic factors for survival of stage I nonsmall cell lung
cancer patients: a population-based analysis of 19,702 stage I
patients in the California Cancer Registry from 1989 to 2003.
Cancer. 110:1532–1541. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kudo Y, Saji H, Shimada Y, et al: Do
tumours located in the left lower lobe have worse outcomes in lymph
node-positive non-small cell lung cancer than tumours in other
lobes? Eur J Cardiothorac Surg. 42:414–419. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Puri V, Garg N, Engelhardt EE, et al:
Tumor location is not an independent prognostic factor in early
stage non-small cell lung cancer. Ann Thorac Surg. 89:1053–1059.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Katayama H, Ueoka H, Kiura K, et al:
Preoperative concurrent chemoradiotherapy with cisplatin and
docetaxel in patients with locally advanced non-small-cell lung
cancer. Br J Cancer. 90:979–984. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Toyooka S, Kiura K, Shien K, et al:
Induction chemoradiotherapy is superior to induction chemotherapy
for the survival of non-small-cell lung cancer patients with
pathological mediastinal lymph node metastasis. Interact Cardiovasc
Thorac Surg. 15:954–960. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Goldstraw P, Crowley J, Chansky K, et al:
International Association for the Study of Lung Cancer
International Staging Committee; Participating Institutions: The
IASLC Lung Cancer Staging Project: proposals for the revision of
the TNM stage groupings in the forthcoming (seventh) edition of the
TNM Classification of malignant tumours. J Thorac Oncol. 2:706–714.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Oken MM, Creech RH, Tormey DC, et al:
Toxicity and response criteria of the Eastern Cooperative Oncology
Group. Am J Clin Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rocha AT, McCormack M, Montana G and
Schreiber G: Association between lower lobe location and upstaging
for early-stage non-small cell lung cancer. Chest. 125:1424–1430.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nohl-Oser HC: An investigation of the
anatomy of the lymphatic drainage of the lungs as shown by the
lymphatic spread of bronchial carcinoma. Ann R Coll Surg Engl.
51:157–176. 1972.PubMed/NCBI
|
|
13
|
Hayakawa K, Mitsuhashi N, Saito Y, et al:
Impact of tumor extent and location on treatment outcome in
patients with stage III non-small cell lung cancer treated with
radiation therapy. Jpn J Clin Oncol. 26:221–228. 1996. View Article : Google Scholar : PubMed/NCBI
|