Introduction
The treatment of patients with advanced
non-small-cell lung cancer (NSCLC) harboring echinoderm
microtubule-associated protein-like 4 anaplastic lymphoma kinase
(EML4-ALK) rearrangement has been revolutionized by the development
of crizotinib, a small-molecule inhibitor of the receptor tyrosine
kinases ALK, ROS1 and MET (1,2). Crizotinib has been reported to be well
tolerated; however, a proportion of the patients are unable to
continue treatment due to the adverse events (2). Several more potent and highly selective
second-generation ALK inhibitors have recently emerged for the
treatment of ALK-positive NSCLC, such as alectinib (3). Alectinib appears to exhibit a more
favorable toxicity profile compared to crizotinib (4).
This is the case report of a NSCLC patient
successfully treated with alectinib, following discontinuation of
crizotinib therapy for one year due to adverse events. This case
indicates that selected patients may continue to benefit from
alectinib following long-term discontinuation of crizotinib
therapy.
Case report
A 41-year-old male patient presented with bilateral
cervical and axillar lymph node enlargement. The patient underwent
a chest computed tomography (CT) scan, which revealed a nodule in
the right upper pulmonary lobe and ipsilateral mediastinal lymph
node enlargement. A cervical node biopsy was performed and the
histological examination confirmed the diagnosis of adenocarcinoma.
Immunohistochemical staining was positive for thyroid transcription
factor-1 and surfactant protein A. The patient had an Eastern
Cooperative Oncology Group performance status of 1 and received 4
cycles of carboplatin, pemetrexed and bevacizumab. As the tumor
response according to the Response Evaluation Criteria In Solid
Tumors (RECIST) guidelines was classified as partial response (PR),
the patient subsequently received maintenance chemotherapy with
pemetrexed and bevacizumab for 6 cycles. However, the treatment was
discontinued due to disease progression.
Written informed consent for the publication of the
medical documents was obtained from the patient.
As fluorescence in situ hybridization
revealed a translocation of ALK, the patient received crizotinib
therapy. After one month, the physical examination and chest CT
revealed a significant decrease in the maximum aggregate tumor
measurement. The tumor response was classified as PR, but the
treatment was discontinued due to crizotinib-related grade 3
general fatigue, according to the National Cancer Institute-Common
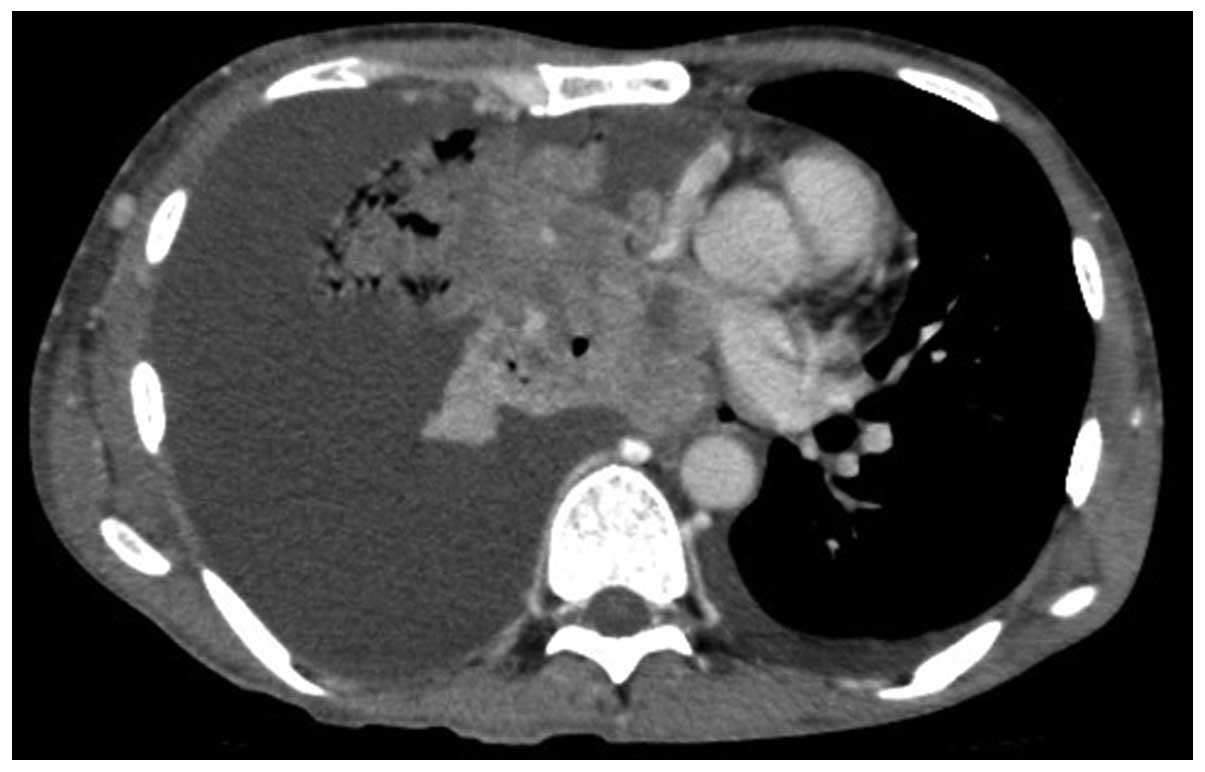
Toxicity Criteria, version 2.0. The patient declined additional
treatment and all the lesions, including the primary site and
cervical, axillar, mediastinal and abdominal lymph node metastases,
increased in size. A chest CT scan revealed a large mass with a
massive pleural effusion (Fig. 1).
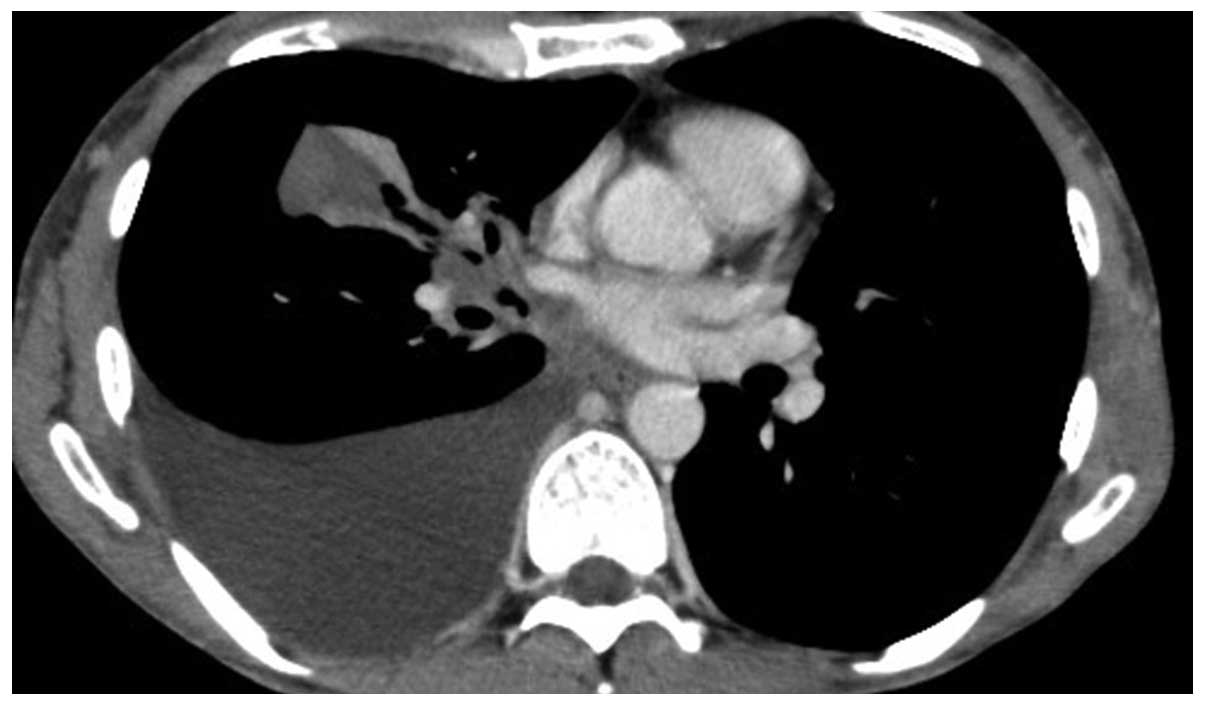
One year after the discontinuation of crizotinib, the patient
consented to receiving alectinib. After 2 weeks of alectinib
treatment, a chest CT revealed a significant decrease in the
maximum aggregate tumor measurement (Fig.
2). The tumor response according to the RECIST guidelines was
classified as PR. Adverse events, including general fatigue, were
not observed. At 4 weeks after the initiation of alectinib, the
patient remained alive and adverse event-free.
Discussion
Gaining genetic insight into the pathogenesis of
NSCLC has paved the way for significant advances in its treatment
(5). ALK was recently found to exert
a potent transforming effect through genetic rearrangement in
approximately 5% of patients with NSCLC (5). Tumor cells with EML4-ALK rearrangement
are dependent on its function, similar to tumor cells harboring
epithelial growth factor receptor mutations (5). Crizotinib is a first-generation ALK
inhibitor, which was previously reported to prolong
progression-free survival, increase response rates and improve the
quality of life in patients with advanced ALK-positive NSCLC
(6,7).
However, despite its marked efficacy in patients with ALK-positive
NSCLC, crizotinib has been associated with certain adverse events,
such as visual disorders, gastrointestinal side effects and
elevated liver aminotransferase levels (7). Two recent large-scale phase III studies
in patients with advanced AKL-positive NSCLC, with or without
previous systemic treatment for advanced disease, demonstrated that
the most common adverse events were visual disorders, diarrhea,
nausea and edema (8,9). As visual disorders have been
specifically associated with crizotinib therapy, attention has been
focused on these adverse events, although they are not severe or
life-threatening. In a previous study conducted by Blackhall et
al (9), comparing crizotinib and
chemotherapy in previously treated patients, crizotinib improved
symptoms including fatigue, cough, pain and dyspnea, whether the
comparator was pemetrexed or docetaxel. General fatigue is not a
common toxicity associated with crizotinib therapy (7); however, our patient exhibited grade 3
general fatigue and declined additional therapy. Even if the
incidence is not high, clinicians should not overlook the most
commonly observed adverse events experienced by the patients.
Alectinib, one of the highly selective
second-generation ALK inhibitors, was recently shown to be
effective in crizotinib-naive patients, as well as in those
resistant to crizotinib (10,11). Common adverse events also associated
with alectinib are visual disorders, gastrointestinal side effects
and pulmonary toxicity (12).
However, the toxicity profile of alectinib has been reported to be
milder compared to that of crizotinib (4). To date, our patient has developed no
severe adverse event, including general fatigue, which was observed
during treatment with crizotinib.
In this study, we presented a case of successful
treatment with alectinib in an ALK-positive NSCLC patient,
following discontinuation of crizotinib therapy for one year. It is
recommended that the patient's disease status and adverse events
are closely followed in ALK-positive NSCLC patients who are treated
with ALK inhibitors.
References
|
1
|
Landi L and Cappuzzo F: Management of
NSCLC: Focus on crizotinib. Expert Opin Pharmacother. 15:2587–2597.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Frampton JE: Crizotinib: A review of its
use in the treatment of anaplastic lymphoma kinase-positive,
advanced non-small cell lung cancer. Drugs. 73:2031–2051. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rossi A, Maione P, Sacco PC, Sgambato A,
Casaluce F, Ferrara ML, Palazzolo G, Ciardiello F and Gridelli C:
ALK inhibitors and advanced non-small cell lung cancer (review).
Int J Oncol. 45:499–508. 2014.PubMed/NCBI
|
|
4
|
Gadgeel SM, Gandhi L, Riely GJ, et al:
Safety and activity of alectinib against systemic disease and brain
metastases in patients with crizotinib-resistant ALK-rearranged
non-small-cell lung cancer (AF-002JG): Results from the
dose-finding portion of a phase 1/2 study. Lancet Oncol.
15:1119–1128. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pikor LA, Ramnarine VR, Lam S and Lam WL:
Genetic alterations defining NSCLC subtypes and their therapeutic
implications. Lung Cancer. 82:179–189. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kijima T, Takeuchi K, Tetsumoto S, et al:
Favorable response to crizotinib in three patients with echinoderm
microtubule-associated protein-like 4-anaplastic lymphoma kinase
fusion-type oncogene-positive non-small cell lung cancer. Cancer
Sci. 102:1602–1604. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shaw AT, Kim DW, Nakagawa K, et al:
Crizotinib versus chemotherapy in advanced ALK-positive lung
cancer. N Engl J Med. 368:2385–2394. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Solomon BJ, Mok T, Kim DW, et al: PROFILE
1014 Investigators: First-line crizotinib versus chemotherapy in
ALK-positive lung cancer. N Engl J Med. 371:2167–2177. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Blackhall F, Kim DW, Besse B, et al:
Patient-reported outcomes and quality of life in PROFILE 1007: A
randomized trial of crizotinib compared with chemotherapy in
previously treated patients with ALK-positive advanced
non-small-cell lung cancer. J Thorac Oncol. 9:1625–1633. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wu YL, Zhou C, Hu CP, et al: Afatinib
versus cisplatin plus gemcitabine for first-line treatment of Asian
patients with advanced non-small-cell lung cancer harbouring EGFR
mutations (LUX-Lung 6): An open-label, randomised phase 3 trial.
Lancet Oncol. 15:213–222. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Majem M and Pallarès C: An update on
molecularly targeted therapies in second- and third-line treatment
in non-small cell lung cancer: Focus on EGFR inhibitors and
anti-angiogenic agents. Clin Transl Oncol. 15:343–357. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Köhler J and Schuler M: LUX-Lung 3:
Redundancy, toxicity or a major step forward? Afatinib as
front-line therapy for patients with metastatic EGFR-mutated lung
cancer. Future Oncol. 10:533–540. 2014. View Article : Google Scholar : PubMed/NCBI
|