Introduction
Pancreatic cancer is the fourth leading cause of
cancer-related fatalities in the USA with a 5-year survival rate of
4–6% (1,2). The only curative treatment for
pancreatic cancer is surgical resection (3). However, 25% of patients with pancreatic
cancer are candidates for curative pancreatectomy. In recent years,
chemoradiotherapy (CRT) has been considered as a reasonable
treatment for locally advanced pancreatic cancer (LAPC). The main
complications of pancreatic cancer include diabetes,
thrombophlebitis, weight loss and mental symptoms, while GI
hemorrhage with serious prognosis is so unusual that investigators
seldom have the research and systematic exposition, leading to a
long-term limit in the research in this field.
Gastrointestinal (GI) hemorrhage is caused by
numerous different lesions and varies greatly in severity, ranging
from clinically insignificant to life threatening (4). It is a frequent cause of
hospitalization, although a number of advances have been made in
diagnosis and treatments. Studies from the United States indicated
that hospitalizations for upper GI (UGI) hemorrhage in the early
1990s occurred at an annual incidence of ~100/100,000 population
and were ~5 times more common than hospitalizations for lower GI
hemorrhage (5–9). UGI hemorrhage usually causes fatalities
in 6–14% of those it affects (9,10). Patient
morbidity and mortality is typically proportional to the degree of
initial blood loss, the rate of rebleeding following endoscopy,
underlying illnesses, and of note, the age of the patient age
(10–13). A systematic study by Laine et
al (14) suggested that the most
common causes of UGI hemorrhage include peptic ulcer disease
[32.1/100,000, (with gastric ulcers more than duodenal)], gastritis
or duodenitis (10.0/100,000), angiodysplasia (5.02/100,000),
esophageal ulcer (2.71/100,000), esophageal varices (1.25/100,000),
Dieulafoy's lesion (1.26/100,000), gastrojejunal ulcer
(1.49/100,000) and unspecified peptic ulcer (0.83/100,000).
Abdominal arteriography may localize GI hemorrhage sources in
approximately one-third of cases. Selective embolization may
provide definitive hemostasis in the outcomes of the majority of
instances of GI hemorrhage (15).
However, there are few studies on the rate and the risk factors of
GI hemorrhage in patients with pancreatic cancer, which lead to an
ambiguous GI hemorrhage rate of pancreatic cancer and controversy
remains in the cause, treatment and outcome.
Therefore, the present study evaluated the incidence
and survival time of the GI hemorrhage patients in pancreatic
cancer in The First Affiliated Hospital of Liaoning Medical
University (Jinzhou, China) over the past 6 years, to assess the
clinical characteristics and to determine the risk factors for it.
The study aimed to overcome the incomplete estimates of GI
hemorrhage patients in pancreatic cancer in the previous
studies.
Materials and methods
Patients
A total of 246 pancreatic cancer patients
(male:female, 190:56; median age, 63.3 years) admitted at The First
Affiliated Hospital of Liaoning Medical University between August
2006 and 2012 were retrospectively evaluated. Pancreatic cancer was
defined according to the National Comprehensive Cancer Network
(NCCN; http://www.nccn.org/professionals/physician_gls/f_guidelines.asp)
for oncologists. Inclusion criteria included pathologically-proven
pancreatic adenocarcinoma, >18 years and the Eastern Cooperative
Oncology Group performance status of 0 to 2. Exclusion criteria
included patients who did not have pathologically-proven pancreatic
adenocarcinoma. Patients with psychosis, sepsis (the presence of ≥2
of the following features was considered evidence of sepsis: i)
Temperature 38°C or 36°C, ii) heart rate 90 beats/min, iii)
respiratory rate 20 breaths/min or iv) leukocyte cell count 12,000
or 4,000/mm3), 10% band forms (16) or coagulopathy (coagulopathy was
defined as a platelet count of 50,000/mm3, a prothrombin
time/international normalized ratio of 1.5 or an activated partial
thromboplastin time 2.03 the control value) were also excluded for
the protocol analysis. The study was approved by the Ethics
Committee of the First Affiliated Hospital of Liaoning Medical
University.
GI hemorrhage
GI hemorrhage was defined as any episode of fresh
blood or coffee ground materials in nasogastric aspirate,
hematemesis, melena or bloody stool. GI hemorrhage was considered
severe if accompanied by hypotension (systolic blood pressure, 100
mmHg), a decrease in the hemoglobin (Hb) level of 2 g/dl or
requiring blood transfusion (17). In
the study, to determine the risk factors for GI hemorrhage, the
history of peptic ulcer, alcohol, smoking or hemorrhage were
recorded. The treatment for GI hemorrhage includes endoscopic
hemostasis, angiography, embolization and conservative care. The
methods of endoscopic hemostasis were hypertonic saline-epinephrine
injection, human plasmin thrombin injection, argon plasma
coagulation or hemoclipping. Rebleeding was confined to episodes
within 7 days after successful hemostasis therapy.
Treatment for pancreatic cancer
For regression analysis, regimens of treatment
methods for pancreatic cancer mainly included surgery, chemotherapy
and CRT. The specific scheme is formulated in accordance with the
NCCN guidelines. All the chemotherapy regimens of CRT performed for
LAPC were classified into three groups: Gemcitabine, 5-fluorouracil
(5-FU) and 5-FU plus gemcitabine. The gemcitabine group was
administered 1,000 mg/m2 of gemcitabine on days 1, 8 and
15 of a 4-week regimen or gemcitabine (same as above) along with 70
mg/m2 of cisplatin on day 1 of the regimen. The 5-FU
group received either 5-FU (1,000 mg/m2 on days 1–3 of a
4-week regimen) or TS-1 (60–80 mg for 2 weeks), or a combination of
5-FU (1,000 mg/m2 on days 1–3), etoposide (100
mg/m2 on days 1–3) and cisplatin (70 mg/m2 on
day 1). For the 5-FU plus gemcitabine group, 1,000 mg/m2
of 5-FU was administered on days 1–3 and 1,000 mg/m2
gemcitabine on days 1, 8 and 15 of a 4-week regimen. All the
radiotherapy regimens of CRT performed for pancreatic cancer were
either three-dimensional conformal radiotherapy (total dose,
4,000–5,400 cGy; one dose, 180–250 cGy; fraction, 28) or
intensity-modulated radiotherapy (total dose, 4,200–6,000 cGy; one
dose, 200–293 cGy; fraction, 25).
Statistical analysis
To investigate the baseline characteristics, the
χ2 test and Student's t-test were used. Categorical
variables were analyzed by the χ2 test and continuous
variables were assessed by the Student's t-test. To evaluate the
survival effect of GI hemorrhage, Cox regression test was used. The
Kaplan-Meier method and the log-rank test were used to compare the
survival rate between patients with and without GI hemorrhage.
Univariate analysis and multivariate logistic regression were used
to detect independent risk factors associated with hemorrhage for
pancreatic cancer and prognosis. P<0.05 was considered to
indicate a statistically significant difference. Analyses were
performed using SPSS software, version 17.0 (SPSS Inc., Chicago,
IL, USA).
Results
Patient characteristics
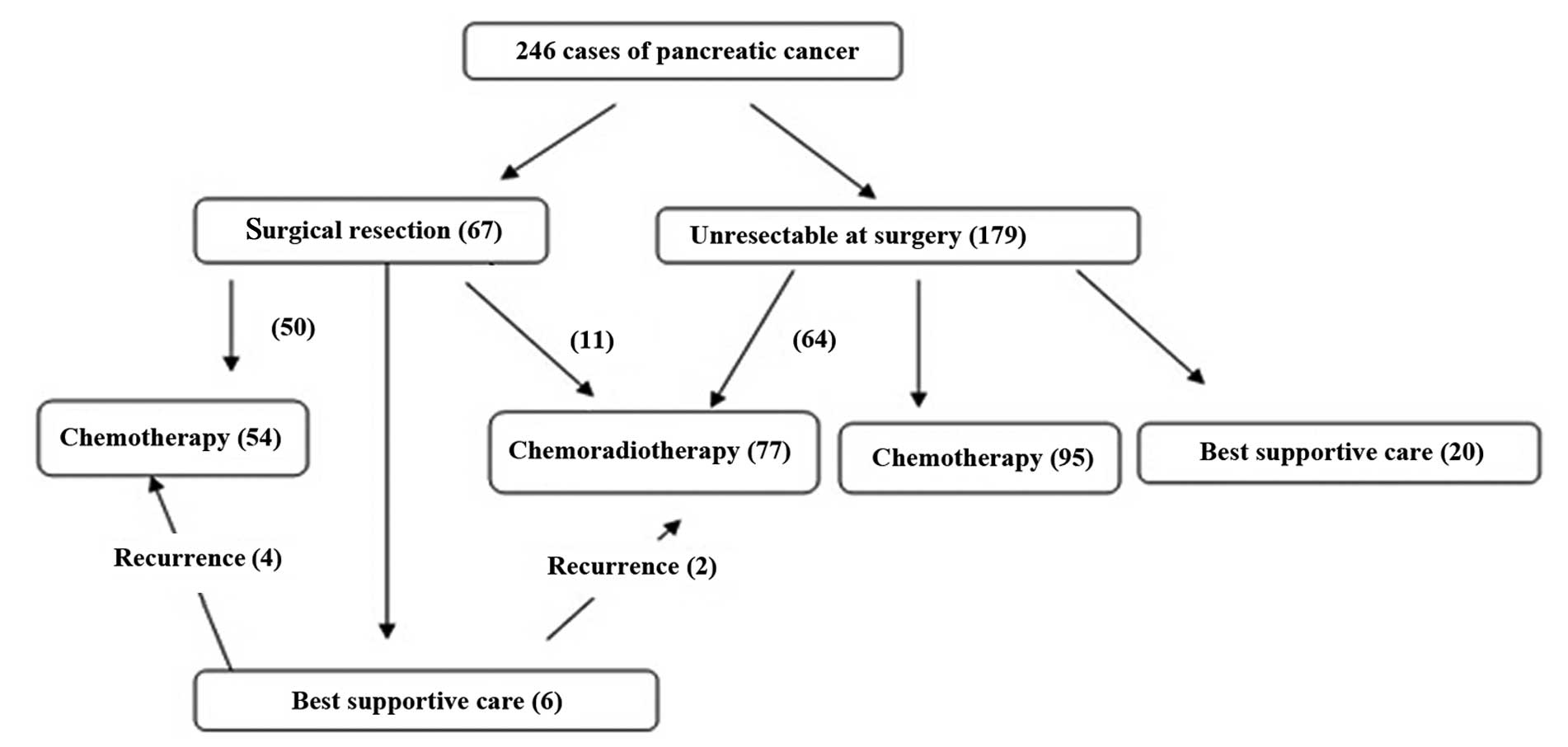
During the 6-year study period, 246 patients with
pancreatic cancer were eligible for analysis (Table I). The average age at the time of the
diagnosis of pancreatic cancer was 63.4±10.92 years. Male patients
accounted for 77.24% of the population, ~2 times more than females.
A total of 3 patients suffered from a history of hemorrhage prior
to the diagnosis of pancreatic cancer. The tumors were mostly
located at the pancreatic head (57.72%). The most common symptom
when diagnosed with pancreatic cancer is abdominal distension or
pain (53.66%). The level of carbohydrate antigen 19-9 (CA19-9) was
549.1±967.1 U/ml. Surgery was performed for 67 patients (27.25%)
and CRT was delivered to 77 patients (31.30%), with the specific
dose determined according to the NCCN guidelines for pancreatic
cancer (Fig. 1). The median follow-up
period was 14.6 months (range, 1.5–60.1 months).
 | Table I.Baseline clinical characteristics of
pancreatic cancer patients. |
Table I.
Baseline clinical characteristics of
pancreatic cancer patients.
| Variables | Number |
|---|
| Gender,
male/female | 190/56 |
| Age,
yearsa | 63.4±10.92 |
| Alcohol, yes/no | 167/79 |
| Smoking, yes/no | 140/106 |
| Past hemorrhage
history, yes/no | 3/243 |
| Past ulcer history,
yes/no | 22/224 |
| Past diabetes
history, yes/no | 25/221 |
| Past cirrhosis
history, yes/no | 30/216 |
| Initial stage,
I/II/III/IV | 67/6/29/144 |
| Recived treatment
prior to hemorrhage, chemotherapy/concurrent
chemoradiotherapy/others | 156/60/30 |
| Initial clinical
symptoms, stained yellow/abdominal distension or
pain/diabete/ileus/others | 64/132/13/13/24 |
| Tumor location, head
of pancreas/body of pancreas/tail of pancreas | 142/49/55 |
| CA19-9 at diagnosis,
U/ml | 549.1±967.1 |
| Initial blood
pressure |
|
| Systolic,
mmHga | 138.1±17.2 |
|
Diastolic, mmHga | 82.7±11.3 |
| Initial heart
ratesa | 92.0±20.1 |
| Hemoglobin,
g/dla | 138.3±24.7 |
| Platelet,
109/la | 239.0±67.2 |
| INR/PTT,
seca |
1.21±14.7/46.3±41.6 |
GI hemorrhage
There were 32 patients (13.0%) who suffered from GI
hemorrhage (Table II). The initial
Hb was 11.2±25.5 g/dl, which decreased to 8.4±17.1 g/dl when
bleeding and the median CA19-9 level increased from 456.7±547.1 to
1,408.5±789.4. Among the total 32 GI hemorrhage patients, there
were 7 patients belonging to the mild GI hemorrhage group with
grade 1, 15 patients in the moderate GI hemorrhage group with grade
2 or 3 and 10 patients in the severe GI hemorrhage group with grade
4 or 5. Due to a bad physical state, conservative care was
delivered to 11 cases and endoscopic hemostasis to 20 cases, while
only 1 case underwent angiography and embolization. Prior to GI
hemorrhage, surgical treatment was delivered to 5 patients (15.6%)
and CRT was delivered to 25 patients (78.13%). The most common
major initial clinical symptoms for GI hemorrhage were melena or
blood stool and haematemesis. Due to a bad physical state, only 20
patients underwent UGI endoscopy. The results showed the cause of
bleeding to be a gastric ulcer in 8 patients, duodenal ulcer in 5,
radiation gastritis in 3 and another reason in 4. UGI endoscopy was
not performed in 12 patients upon the rejection of their guardians
or a bad physical state. As the patients were in terminal stages,
the guardians did not want them to undergo any more examinations.
Hemorrhage was successfully stopped by endoscopic treatment in 12
patients (37.5%). The methods of endoscopic hemostasis included
hypertonic saline-epinephrine injection, argon plasma coagulation,
human plasmin thrombin injection or hemoclipping. Embolization was
performed in 1 patient and hemorrhage was finally stopped. However,
7 cases rebled and 18 patients in total succumbed to GI hemorrhage.
The average time from GI hemorrhage to mortality was 31.5±21.6 days
and the average overall survival rate was 10.0±6.2 months.
| Table II.Clinical characteristics of pancreatic
cancer patients with GI hemorrhage (n=32). |
Table II.
Clinical characteristics of pancreatic
cancer patients with GI hemorrhage (n=32).
| Variables | Number |
|---|
| Gender,
male/female | 24/8 |
| Age,
yearsa | 62.4±8.7 |
| Alcohol, yes/no | 29/3 |
| Smoking, yes/no | 25/7 |
| Past hemorrhage
history, yes/no | 2/30 |
| Hemoglobin, g/dl |
|
|
Initial | 11.2±25.5 |
| At
bleeding | 8.4±17.1 |
| CA19-9 level,
U/ml |
|
|
Initial | 456.7±547.1 |
| At
bleeding | 1,408.5±789.4 |
| Severity |
|
| Mild | 7 |
|
Moderate | 15 |
|
Severe | 10 |
| Treatment |
|
|
Endoscopic hemostasis | 20 |
|
Angiography and
embolization | 1 |
|
Conservative care | 11 |
| Initial clinical
symptoms at diagnosis of pancreatic cancer, stained
yellow/abdominal distension or pain/diabete/ileus/others | 12/18/0/1/1 |
| Time to mortality
from hemorrhage | 31.5±21.6 days |
| Survival time from
diagnosis | 10.0±6.2 months |
| H. pylori
infection, yes/no | 10/22 |
| Hemorrhage related
mortality, yes/no | 20/12 |
| Initial clinical
symptoms of GI hemorrhage |
|
| Melena or
blood stool | 18 |
|
Haematemesis | 9 |
| Abdominal
distention | 3 |
| Stomach
ache | 2 |
Risk factors for GI hemorrhage
The incidence of GI hemorrhage was 13.0 (n=32) and
10.2% (n=25) of patients succumbed due to bleeding. The present
study analyzed the association between clinical parameters and the
risk of GI hemorrhage. In the univariate analysis, there was no
statistically significant difference in gender, age, past ulcer
history, past diabetes history, past cirrhosis history, the type of
received treatment prior to hemorrhage, initial blood pressure,
initial heart rates, Hb, platelet and international normalized
ratio/partial thromboplastin time between the GI hemorrhage and the
no-GI hemorrhage groups (Table
III). Alcohol, smoking, past hemorrhage history, initial stage,
tumor location and CA19-9 level at diagnosis of pancreatic cancer
(P<0.05) were risk factors for GI hemorrhage. Alcohol
consumption was noted for 29/32 (90.6%) patients in the GI
hemorrhage group and 138/214 (64.5%) patients in the no-GI
hemorrhage group (P<0.05). Additionally, smoking was reported by
25/32 (78.1%) patients in the GI hemorrhage group and 115/214
(53.7%) patients in the no-GI hemorrhage group (P<0.05). The
factors of past hemorrhage history, initial stage at diagnosis of
pancreatic cancer, tumor location and ulcer sizes and CA19-9 level
at diagnosis of pancreatic cancer were significantly different
between the GI hemorrhage and the no-GI hemorrhage groups
(P<0.05).
| Table III.Baseline clinical characteristics of
pancreatic cancer patients. |
Table III.
Baseline clinical characteristics of
pancreatic cancer patients.
|
| GI hemorrhage |
|---|
|
|---|
| Variables | Presence, n (%) | P-value |
|---|
| Gender,
male/female | 24 (12.6)/8
(14.3) | NS |
| Age,
yearsa |
|
|
|
≤65 | 22 (12.4) | NS |
|
>65 | 10 (14.7) |
|
| Alcohol,
yes/no | 29 (17.4)/3
(3.8) | <0.01 |
| Smoking,
yes/no | 25 (17.9)/7
(6.6) | <0.01 |
| Past hemorrhage
history, yes/no | 2 (66.7)/30
(12.3) | <0.01 |
| Past ulcer history,
yes/no | 3 (13.6)/29
(12.9) | NS |
| Past diabetes
history, yes/no | 4 (16.0)/28
(12.7) | NS |
| Past cirrhosis
history, yes/no | 2 (6.7)/30
(13.9) | NS |
| Initial stage,
I/II/III/IV | 8 (11.9)/4 (66.7)/6
(20.7)/14 (9.7) | <0.01 |
| Recived treatment
prior to hemorrhage, chemotherapy/concurrent
chemoradiotherapy/others | 18 (11.5)/8
(13.3)/6 (20.0) | NS |
| Tumor location,
head of pancreas/body of pancreas/tail of panaceas | 13 (9.2)/13
(26.5)/6 (10.9) | <0.01 |
| Initial clinical
symptoms, stained yellow/abdominal distension or
pain/diabete/ileus/others | 12 (18.8)/18
(13.6)/0 (0)/1 (7.7)/1 (4.2) | NS |
| CA19-9 at
diagnosis, U/ml |
|
|
|
≤1,000 | 13 (7.6) | <0.01 |
|
>1,000 | 19 (25.3) |
|
| Initial blood
pressure |
|
|
|
Systolic, mmHga | 131.6±39.0 | NS |
|
Diastolic, mmHga | 76.0±17.5 | NS |
| Initial heart
ratesa | 93.0±26.5 | NS |
| Hemoglobin,
g/dla | 8.4±17.1 | NS |
| Platelet,
109/la | 208±147 | NS |
| INR/PTT,
seca |
1.13±0.36/45.1±54.7 | NS |
In multivariate analysis, only initial stage IV
tumors [odds ratio (OR), 21.94; 95% confidence interval (CI),
2.274–211.642] were a significant risk factor for GI hemorrhage
(Table IV). The hazard ratio was
1.246 (95% CI, 0.754–2.060) for the effects of GI hemorrhage on the
survival rate, but it was not significant (Table V).
| Table IV.Logistic multivariate regression
analysis of GI hemorrhage in all patients (n=246). |
Table IV.
Logistic multivariate regression
analysis of GI hemorrhage in all patients (n=246).
| Variables | B | SE | Wald | df | P-value | Exp (B) | 95% CI for Exp
(B) |
|---|
| Alcohol | −0.728 | 0.876 | 0.691 | 1 | 0.406 | 0.483 | 0.087–2.689 |
| Smoking | 0.192 | 0.673 | 0.081 | 1 | 0.776 | 1.211 | 0.324–4.525 |
| PHH | −22.598 | 3,991.455 | 0.000 | 1 | 0.995 | 0.000 | 0.000 |
| Stage |
|
| 7.165 | 3 | 0.067 |
|
|
| Stage (1) | 0.144 | 0.498 | 0.084 | 1 | 0.772 | 1.155 | 0.435–3.066 |
| Stage (2) | −19.245 | 16,326.303 | 0.000 | 1 | 0.999 | 0.000 | 0.000 |
| Stage (3) | 3.088 | 1.156 | 7.132 | 1 | 0.008 | 21.940 | 2.274–211.642 |
| Tl |
|
| 8.250 | 2 | 0.016 |
|
|
| Tl (1) | 36.977 | 5,793.616 | 0.000 | 1 | 0.995 | 1.146E16 | 0.000 |
| Tl (2) | 32.788 | 5,793.616 | 0.000 | 1 | 0.995 | 1.737E14 | 0.000 |
| CA19-9 | −0.772 | 0.503 | 2.353 | 1 | 0.125 | 0.462 | 0.172–1.239 |
| Constant | −15.521 | 4,199.319 | 0.000 | 1 | 0.997 | 0.000 |
|
| Table V.Cox regression analysis of the effect
of GI hemorrhage on the survival rate. |
Table V.
Cox regression analysis of the effect
of GI hemorrhage on the survival rate.
| Variable | P-value | HR | 95.0% CI for
HR |
|---|
| Age >65
years | 0.968 | 1.000 | 0.985–1.016 |
| Gender, male | 0.125 | 1.352 | 0.919–1.989 |
| Alcohol,
yes/no | 0.929 | 1.021 | 0.641–1.626 |
| Smoking,
yes/no | 0.271 | 0.801 | 0.540–1.189 |
| Past hemorrhage
history, yes/no | 0.819 | 1.095 | 0.503–2.384 |
| Past ulcer history,
yes/no | 0.142 | 0.458 | 0.162–1.298 |
| Past diabetes
history, yes/no | 0.440 | 0.808 | 0.470–1.388 |
| Past cirrhosis
history, yes/no | 0.487 | 0.350 | 0.540–1.650 |
| Initial stage
(I) | 0.056 |
|
|
| Initial stage
(II) | 0.017 | 0.540 | 0.326–0.895 |
| Initial stage
(III) | 0.811 | 1.135 | 0.400–3.220 |
| Initial stage
(IV) | 0.390 | 1.246 | 0.754–2.060 |
| Initial clinical
symptoms (stained yellow) | 0.019 |
|
|
| Initial clinical
symptoms (abdominal distension or pain) | 0.050 | 2.117 | 0.999–4.490 |
| Initial clinical
symptoms (diabete) | 0.017 | 2.299 | 1.162–4.550 |
| Initial clinical
symptoms (ileus) | 0.001 | 4.552 | 1.874–11.060 |
| Initial clinical
symptoms (others) | 0.095 | 2.173 | 0.873–5.408 |
| Tumor location
(head of pancreas) | 0.225 |
|
|
| Tumor location
(body of pancreas) | 0.093 | 0.674 | 0.425–1.068 |
| Tumor location
(tail of panceas) | 0.697 | 0.906 | 0.549–1.493 |
| CA19-9 | 0.668 | 0.924 | 0.646–1.324 |
Survival
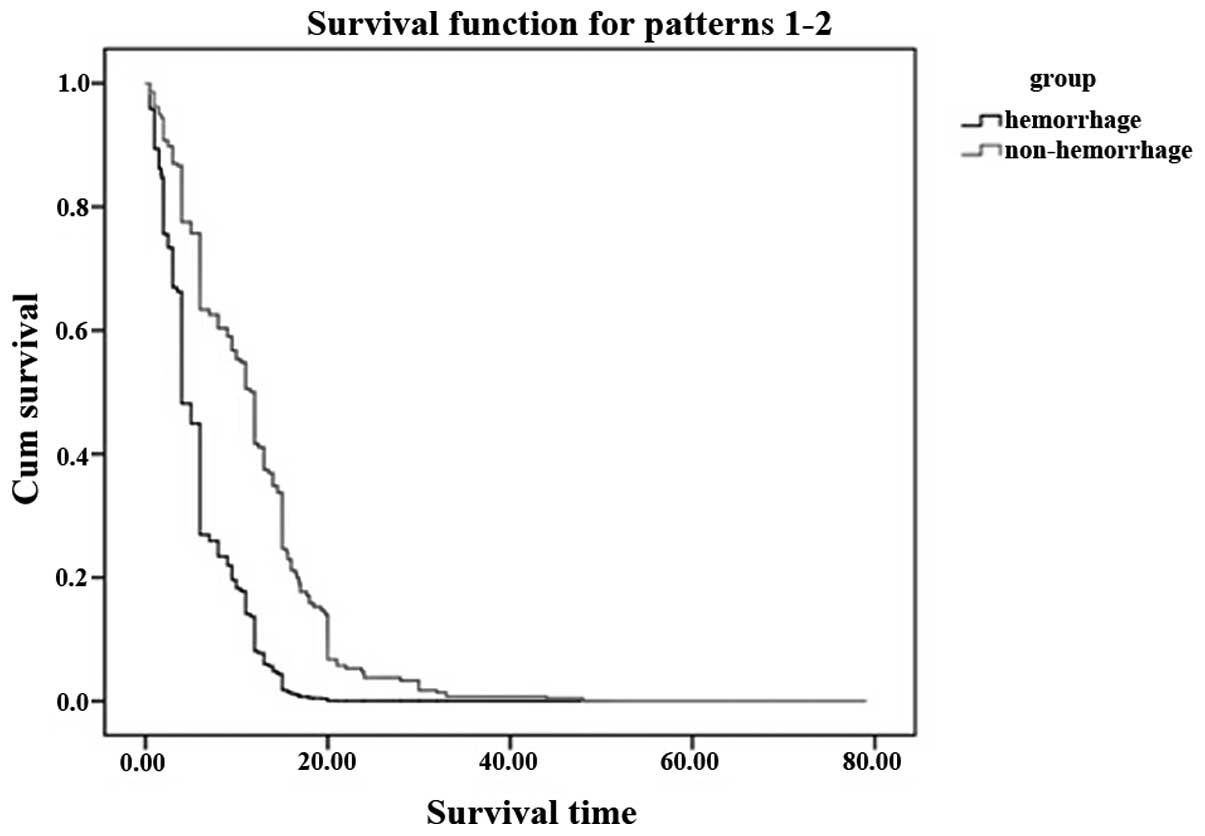
A total of 212 patients (86.2%) had succumbed at the
time of final analysis. The median overall survival time was 9.0
months (range, 2.0–6.0 months) in patients without GI hemorrhage
and 14.5 months (range, 0.5–48.0 months) in patients with GI
hemorrhage (Fig. 2), although the
difference of the overall survival time was significant with
P<0.05. The median period from clinically diagnosed GI
hemorrhage to fatality was extremely short (30 days range from 1 h
to 65 days).
Discussion
In certain cases, GI hemorrhage may be a symptom of
a serious or life-threatening condition that should be immediately
evaluated in an emergency setting. The present analysis showed that
the median period from GI hemorrhage to mortality is extremely
short for the patients with pancreatic cancer, and the median
overall survival time of the patients with GI hemorrhage was
significantly shorter than that of patients without GI hemorrhage,
which was similar with other studies (18–20), and
is critical if not treated properly. The main treatment for GI
hemorrhage in patients include fasting, proton pump inhibitor and
endoscopic therapy, which may be effective to a certain degree,
however, the effect to patients of GI hemorrhage with pancreatic
cancer was not so clear, with an even shorten survival rate. The
patients of pancreatic cancer are common in a significant tumor
load state and their body condition is extremely poor, therefore,
clinical doctors are usually unable to do anything. From this
perspective, it is critical to early diagnose GI hemorrhage and to
prevent it as soon as possible.
There are certain studies that are committed to the
cause prevention and the treatment of GI hemorrhage, while there
are few studies that focus on the early prevention, early diagnosis
and the reasonable treatment of GI hemorrhage associated with
pancreatic cancer. Regarding the risk factors for GI hemorrhage of
pancreatic cancer, a study reported that the independent risk
factor for GI hemorrhage was tumor location in the pancreatic body
(21). The patients enrolled in the
present study received CRT for pathologically proven LAPC. However,
there are few studies that reported the risk factors of all the
stages of pancreatic cancer patients. In the present study, the
initial clinical tumor stage of IV was one of the main factors (OR,
21.94, P=0.008). To a certain degree, the late stage of pancreatic
cancer as the independent risk factor is understandable and it is
likely associated with numerous factors, such as heavy tumor
burden, complex treatment, poor physical fitness of patients and
the larger mass may even increase the probability of violations of
the digestive tract. Thus, more studies are required to investigate
whether there is any difference between the different tumor stages
or the different treatment.
The present study has several limitations. First, it
was a retrospective study and a small number of patients were
evaluated. Second, regarding the therapy of pancreatic cancer, the
chemotherapy and pain management-induced adverse effects could not
be excluded. In addition, the regimens were different between each
other and the numbers of patients receiving gemcitabine differed
from those receiving 5-FU, and several studies have reported that
gemcitabine is more toxic than 5-FU (22,23). Third
is hospital stay and blood transfusion, which were evaluated in
other studies (24,25). Therefore, further studies are required
to improve the outcomes in GI hemorrhage patients with pancreatic
cancer.
In conclusion, the present results show that GI
hemorrhage is critical in pancreatic cancer patients. Not only was
the median overall survival rate of the patients with GI hemorrhage
significantly shorter than that of patients without GI hemorrhage,
but the time from GI hemorrhage to mortality was also extremely
short. Clinical oncologists should pay more attention to those who
had a late stage of pancreatic cancer. The clinicians should
consider GI hemorrhage in pancreatic cancer patients. Extensive
studies are required to explore more effective treatment
measures.
References
|
1
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J and
Thun MJ: Cancer statistics, 2009. CA Cancer J Clin. 59:225–249.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Olowokure O and Qi X: Pancreatic cancer:
Current standards, working towards a new therapeutic approach.
Expert Rev Anticancer Ther. 14:495–497. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Winek T, Hamre D, Mozell E and Vetto RM:
Prognostic factors for survival after pancreaticoduodenectomy for
malignant disease. Am J Surg. 159:454–456. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rockey DC: To transfuse or not to
transfuse in upper gastrointestinal hemorrhage? That is the
question. Hepatology. 60:422–424. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Longstreth GF: Epidemiology and outcome of
patients hospitalized with acute lower gastrointestinal hemorrhage:
A population-based study. Am J Gastroenterol. 92:419–424.
1997.PubMed/NCBI
|
|
6
|
Longstreth GF: Epidemiology of
hospitalization for acute upper gastrointestinal hemorrhage: A
population-based study. Am J Gastroenterol. 90:206–210.
1995.PubMed/NCBI
|
|
7
|
Wollenman CS, Chason R, Reisch JS and
Rockey DC: Impact of ethnicity in upper gastrointestinal
hemorrhage. J Clin Gastroenterol. 48:343–350. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fallah MA, Prakash C and Edmundowicz S:
Acute gastrointestinal bleeding. Med Clin North Am. 84:1183–1208.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Greenspoon J, Barkun A, Bardou M, Chiba N,
Leontiadis GI, Marshall JK, Metz DC, Romagnuolo J and Sung J:
International Consensus Upper Gastrointestinal Bleeding Conference
Group: Management of patients with nonvariceal upper
gastrointestinal bleeding. Clin Gastroenterol Hepatol. 10:234–239.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cooper GS, Chak A, Way LE, Hammar PJ,
Harper DL and Rosenthal GE: Early endoscopy in upper
gastrointestinal hemorrhage: Associations with recurrent bleeding,
surgery and length of hospital stay. Gastrointest Endosc.
49:145–152. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Simoens M, Gevers AM and Rutgeerts P:
Endoscopic therapy for upper gastrointestinal hemorrhage: A state
of the art. Hepatogastroenterology. 46:737–745. 1999.PubMed/NCBI
|
|
12
|
Longstreth GF and Feitelberg SP:
Outpatient care of selected patients with acute non-variceal upper
gastrointestinal haemorrhage. Lancet. 345:108–111. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Silverstein FE, Gilbert DA, Tedesco FJ,
Buenger NK and Persing J: The national ASGE survey on upper
gastrointestinal bleeding. II. Clinical prognostic factors.
Gastrointest Endosc. 27:80–93. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Laine L, Yang H, Chang SC and Datto C:
Trends for incidence of hospitalization and death due to GI
complications in the United States from 2001 to 2009. Am J
Gastroenterol. 107:1190–1195; quiz 1196. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Charbonnet P, Toman J, Bühler L, Vermeulen
B, Morel P, Becker CD and Terrier F: Treatment of gastrointestinal
hemorrhage. Abdom Imaging. 30:719–726. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bone RC, Balk RA, Cerra FB, Dellinger RP,
Fein AM, Knaus WA, Schein RM and Sibbald WJ: The ACCP/SCCM
Consensus Conference Committee. American College of Chest
Physicians/Society of Critical Care Medicine: Definitions for
sepsis and organ failure and guidelines for the use of innovative
therapies in sepsis. Chest. 101:1644–1655. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Davenport RJ, Dennis MS and Warlow CP:
Gastrointestinal hemorrhage after acute stroke. Stroke. 27:421–424.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shinchi H, Takao S, Noma H, Matsuo Y,
Mataki Y, Mori S and Aikou T: Length and quality of survival after
external-beam radiotherapy with concurrent continuous
5-fluorouracil infusion for locally unresectable pancreatic cancer.
Int J Radiat Oncol Biol Phys. 53:146–150. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Li CP, Chao Y, Chi KH, Chan WK, Teng HC,
Lee RC, Chang FY, Lee SD and Yen SH: Concurrent chemoradiotherapy
treatment of locally advanced pancreatic cancer: Gemcitabine versus
5-fluorouracil, a randomized controlled study. Int J Radiat Oncol
Biol Phys. 57:98–104. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chauffert B, Mornex F, Bonnetain F,
Rougier P, Mariette C, Bouché O, Bosset JF, Aparicio T, Mineur L,
Azzedine A, et al: Phase III trial comparing intensive induction
chemoradiotherapy (60 Gy, infusional 5-FU and intermittent
cisplatin) followed by maintenance gemcitabine with gemcitabine
alone for locally advanced unresectable pancreatic cancer.
Definitive results of the 2000–01 FFCD/SFRO study. Ann Oncol.
19:1592–1599. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee KJ, Kim HM, Jung JW, Chung MJ, Park
JY, Bang S, Park SW, Lee WJ, Seong JS and Song SY: Gastrointestinal
hemorrhage after concurrent chemoradiotherapy in locally advanced
pancreatic cancer. Gut Liver. 7:106–111. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Crane CH, Abbruzzese JL, Evans DB, Wolff
RA, Ballo MT, Delclos M, Milas L, Mason K, Charnsangavej C, Pisters
PW, et al: Is the therapeutic index better with gemcitabine-based
chemoradiation than with 5-fluorouracil-based chemoradiation in
locally advanced pancreatic cancer? Int J Radiat Oncol Biol Phys.
52:1293–1302. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Huguet F, Girard N, Guerche CS, Hennequin
C, Mornex F and Azria D: Chemoradiotherapy in the management of
locally advanced pancreatic carcinoma: A qualitative systematic
review. J Clin Oncol. 27:2269–2277. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cheung J, Yu A, LaBossiere J, Zhu Q and
Fedorak RN: Peptic ulcer bleeding outcomes adversely affected by
end-stage renal disease. Gastrointest Endosc. 71:44–49. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Toke AB: GI bleeding risk in patients
undergoing dialysis. Gastrointest Endosc. 71:50–52. 2010.
View Article : Google Scholar : PubMed/NCBI
|