Introduction
Bacillus Calmette-Guérin (BCG) instillation as an
adjuvant to transurethral resection of the bladder tumour (TURBT)
is the most effective and widely used therapy for
non-muscle-invasive bladder cancer (NMIBC). Although BCG therapy
may improve the prognosis of NMIBC patients, 20–40% patients fail
to respond (1,2). BCG treatment commonly induces
granulomatous inflammatory changes in the bladder, which produce
irritative symptoms. The systemic side effects may vary from mild
malaise and fever to life-threatening or fatal sepsis (3). Therefore, it is important to identify a
reliable predictive biomarker. Several studies have attempted to
identify risk factors for disease recurrence and it was recently
demonstrated that certain factors may predict the recurrence of
NMIBC (4). Although these results are
useful for predicting the effectiveness of BCG therapy in various
settings, a number of emerging factors have not been
considered.
Recently, the association between inflammation and a
variety of cancers has been reported (5,6). In our
previous study, we demonstrated that pyuria was a prognostic marker
of recurrence and progression of newly diagnosed NMIBC (7). The aim of this study was to evaluate the
utility of pyuria as a predictive marker of BCG treatment for
NMIBC.
Patients and methods
Study group
Between 1994 and 2007, 243 patients were diagnosed
with NMIBC based on histopathological evaluation and were treated
with intravesical instillation of BCG following TURBT at the Tokyo
Metropolitan Tama Medical Center (Tokyo, Japan).
Urine analysis
Urine analysis for pyuria was performed prior to
TURBT and a sample for urine culture was collected at the same
time. The cases with NMIBC confirmed by pathological examination
underwent BCG instillation. Pyuria was defined as ≥10 white blood
cells per high power field of urine (8).
Individual patient data, including number of tumors,
tumor size, tumor grade [1973 WHO classification (9)], pathological T stage, presence of
concomitant carcinoma in situ and intravesical therapy, were
obtained from patient medical records.
Treatment
Instillation with 40, 80 or 81 mg BCG (Tokyo or
Connaught strain were obtained from Japan BCG or Nippon Kayaku,
Tokyo, Japan, respectively) diluted in 40 ml saline was performed
between 14 and 28 days after TURBT. The instillation was repeated
once weekly for 6–8 consecutive weeks. None of the patients
received maintenance instillation. During follow-up, all the
patients underwent cystoscopy, urine analysis and cytology every 3
months following BCG treatment.
Statistical analysis
The time-to-recurrence following BCG treatment was
defined as the time from the date of the first instillation of BCG
to the date of bladder cancer recurrence. Patients who remained
alive without recurrence, or those who succumbed prior to
recurrence, were censored at the date of the last available
follow-up cystoscopy.
The distribution of recurrence-free survival (RFS)
was constructed using the Kaplan-Meier method. The association
between survival and each parameter was analyzed with the log-rank
test. Univariate and multivariate Cox proportional hazards
regression models were summarized with risk ratios and 95%
confidence intervals. The statistical analyses were performed using
the JMP® software package. A P-value <0.05 was considered
statistically significant.
Results
Patient characteristics
The characteristics of the patients and their tumors
are summarized in Table I. Of the 243
patients treated with BCG instillation, 117 (48%) developed
subsequent recurrence. In this analysis, we assessed the presence
of pyuria at the time of recurrent tumor resection, prior to BCG
treatment. Pyuria was detected in 37 of the 243 patients (15%)
treated with BCG. Recurrence survivors were followed up for a
median period of 10 months. The RFS rates at 1 and 3 years were 72
and 56%, respectively. The median time of RFS was 45 months.
 | Table I.Characteristics of patients receiving
intravesical BCG treatment (n=243). |
Table I.
Characteristics of patients receiving
intravesical BCG treatment (n=243).
| Characteristics | No. of patients
(%) |
|---|
| Age (years) |
|
|
<80 | 192 (79) |
| ≥80 | 51 (21) |
| Gender |
|
| Male | 196 (81) |
|
Female | 47 (19) |
| Pyuria (no. of
WBC/hpf) |
|
| ≤9 | 206 (85) |
| ≥10 | 37 (15) |
| No. of tumors |
|
| 1 | 107 (44) |
| 2–7 | 121 (50) |
| ≥8 | 15 (6) |
| Tumor size (cm) |
|
|
<3 | 239 (98) |
| ≥3 | 4 (2) |
| T stage |
|
| Ta | 200 (82) |
| T1 | 43 (18) |
| Carcinoma in
situ |
|
| No | 215 (88) |
| Yes | 28 (12) |
| Grade |
|
| G1 | 74 (30) |
| G2 | 124 (51) |
| G3 | 45 (19) |
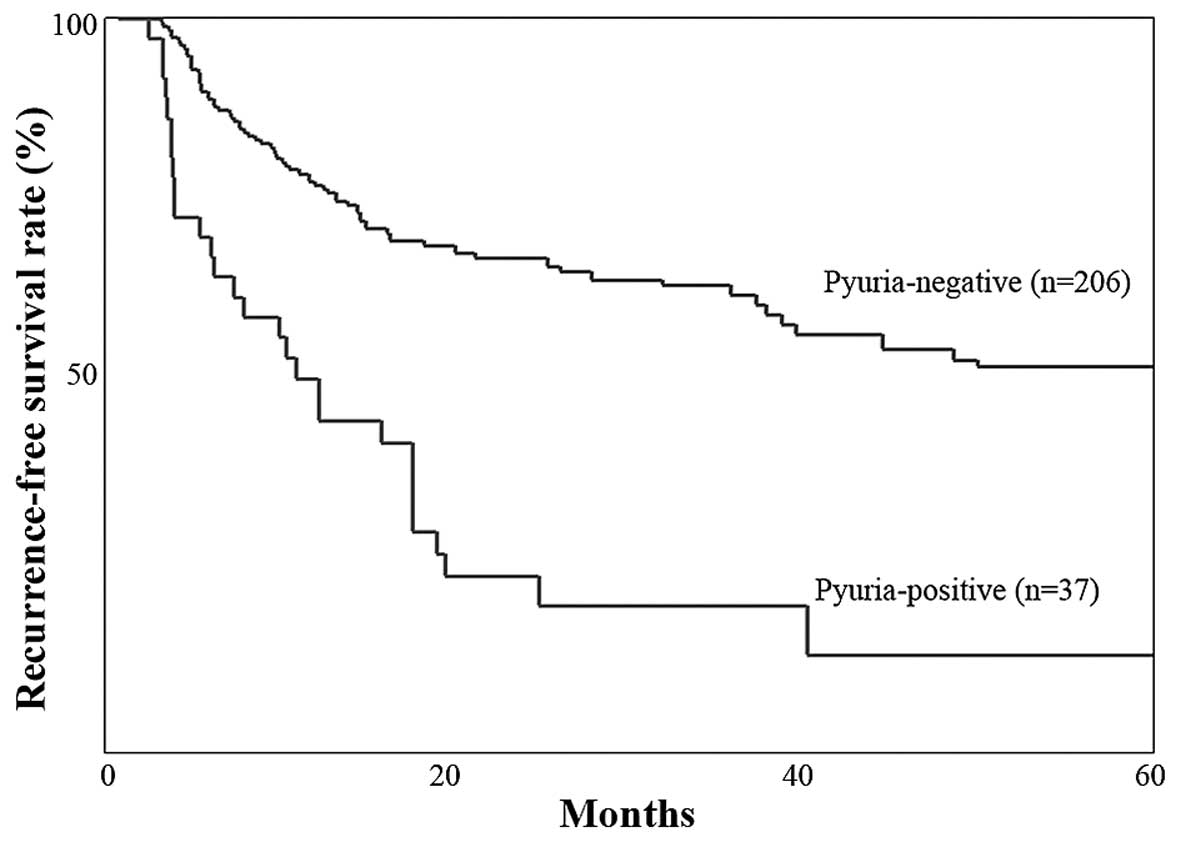
Tumor recurrence
Tumor recurrence was diagnosed in 30 (81%) of the 37
patients with pyuria and 87 (42%) of the 206 patients without
pyuria following BCG treatment. The RFS rates at 3 years were
significantly lower among patients with pyuria vs. those without
(20 vs. 62%, respectively; P<0.0001) (Fig. 1). The univariate regression analysis
revealed that pyuria was associated with RFS following BCG therapy.
Specifically, patients with pyuria appeared to be resistant to BCG
treatment. The previously reported factors (age, gender, tumor
number, tumor size, T stage and grade) were also associated with
RFS following BCG treatment (Table
II). Prior recurrence rates were not considered, since only
newly diagnosed patients were included in this study. The
multivariate regression analysis revealed that pyuria was an
independent predictor of tumor recurrence following BCG treatment
(Table II). In this model, age,
tumor number and size were also identified as independent
predictors of tumor recurrence following BCG treatment (Table II).
| Table II.Univariate and multivariate analysis
of recurrence following intravesical BCG treatment. |
Table II.
Univariate and multivariate analysis
of recurrence following intravesical BCG treatment.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (years) |
|
|
|
| <80
vs. ≥80 | 2.26 (1.50–3.35) | 0.0002 | 1.89 (1.22–2.87) | 0.005 |
| Gender | 1.56 (1.01–2.38) | 0.0493 |
| 0.309 |
| Male vs.
female |
|
|
|
|
| Pyuria
(cells/hpf) | 3.36 (2.17–5.08) | <0.0001 | 3.05 (2.06–4.84) | <0.0001 |
| ≤9 vs.
>9 |
|
|
|
|
| No. of tumors |
|
|
|
|
| Single
vs. 2–7 | 1.51 (1.03–2.25) | 0.0038 | 1.25 (1.02–1.76) | 0.0153 |
| 2–7 vs.
>7 | 2.23 (1.08–4.15) |
| 2.80 (1.32–5.38) |
|
| Tumor size |
|
|
|
|
| ≤3 vs. >3 cm | 3.75 (1.93–6.50) | 0.0004 |
| 0.124 |
| T stage |
|
|
|
|
| Ta vs.
T1 | 2.47 (1.61–6.55) | 0.0351 |
| 0.854 |
| Carcinoma in
situ |
|
|
|
|
| No vs.
yes |
| 0.254 |
| 0.800 |
| Grade |
|
|
|
|
| G1 vs.
G2 | 1.66 (1.08–2.62) | 0.0492 |
| 0.247 |
| G2 vs.
G3 | 1.29 (1.03–1.54) |
|
|
|
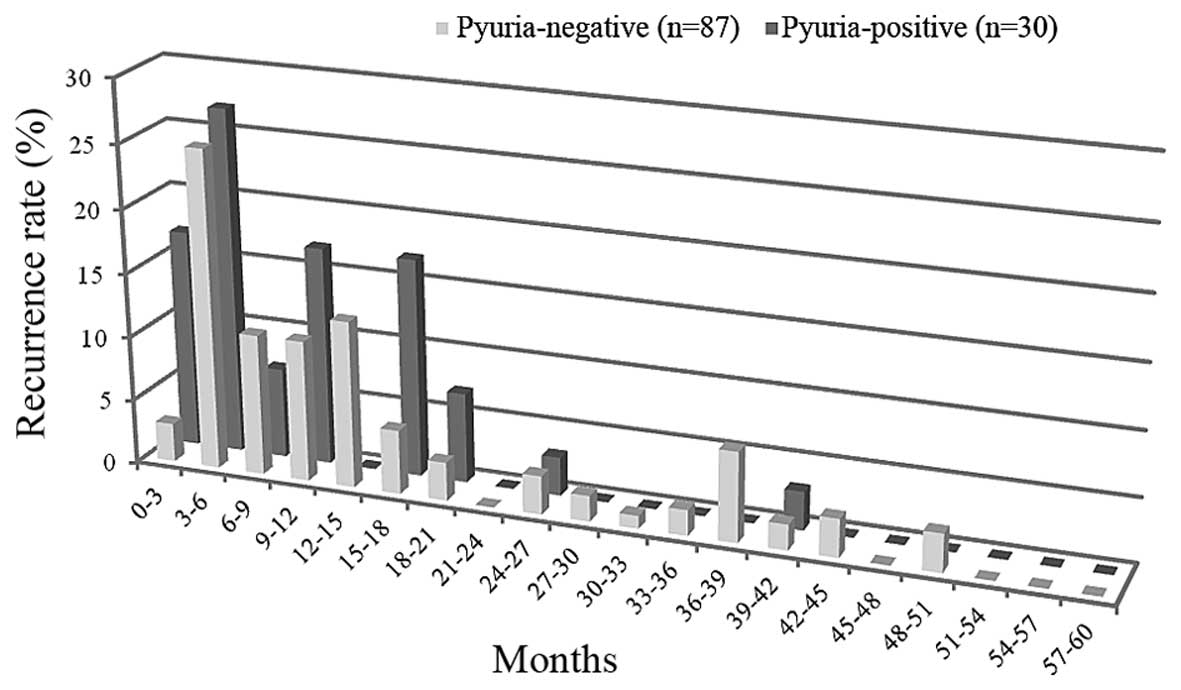
BCG relapsing was further defined by time of
recurrence as early (within 12 months), intermediate (12–24 months)
or late (>24 months) (10).
Recurrence within 12 months was observed in 21 (68%) of the 30
recurrent cases with pyuria and in only 43 (50%) of the 87
recurrent cases without pyuria. Recurrence after 24 months was
observed in 1 (3%) of the 30 recurrent cases with pyuria and in
only 20 (23%) of the 87 recurrent cases without pyuria (Fig. 2). These data suggested that pyuria was
associated with early recurrence following BCG treatment.
Discussion
Recent studies reported that inflammation within the
tumor microenvironment may promote the growth and invasion of
cancer cells through an increase in cell proliferation, survival,
migration and angiogenesis (11). In
our previous study, we demonstrated that NMIBC with pyuria was
associated with poor clinical prognosis and that the presence of
the pyuria could be used as an indicator of recurrence and
progression (7).
Intravesical BCG treatment is effective for NMIBC,
particularly for high- and intermediate-risk tumors (12). Although the precise mechanism of BCG
immunotherapy is not known, previous studies have suggested that
the response to BCG is dependent upon immunological reaction
(13). A high degree of leukocyte
infiltration is commonly observed in cancer-related inflammation.
Recent studies have reported that inflammation within the tumor
microenvironment may be associated with poor prognosis (14,15).
Therefore, we hypothesized that tumor-associated inflammation may
exert a detrimental effect on BCG treatment and lead to eventual
tumor recurrence. Pyuria is a established marker of inflammation.
In this study, we assessed the presence of pyuria at the time of
tumor recurrence and observed that pyuria independently predicted
response to BCG.
The present study demonstrated that NMIBC with
pyuria exhibited a higher overall recurrence rate compared with
NMIBC without pyuria. It was previously demonstraded that BCG
treatment may decrease early recurrence and maintain a low
recurrence rate up to 800 days (16).
In the pyuria-positive group, early recurrence (within 6 months)
was observed more frequently, whereas late recurrence (after 24
months) was observed in only 1 case (Fig.
2). These findings suggest that bladder cancers with pyuria are
resistant to BCG therapy.
There are a number of possible explanations for this
association between BCG resistance and pyuria. First, since bladder
tumors may grow in an inflammatory environment, cancer cells are
already resistant to immune cells. Additionally, the inflammation
induced by the bladder tumor may inhibit the antitumor immune
reaction produced by BCG treatment. In this immune escape, the
neutrophils or other immune cells, including macrophages,
regulatory T cells, or MDSCs, recruited through the inflammatory
process, may be the key players (6).
However, further investigation is warranted.
The limitations of the present study included the
small number of patients, the retrospective nature of the analysis,
conducted via medical chart review, and that the regimen of BCG was
not the currently standard regimen. Recently, the efficacy of
maintenance treatment with BCG has been reported (17). In the present study, all the cases
only received 8 cycles of weekly intravesical instillations and no
maintenance administration of BCG.
We compared the efficacy of intravesical
instillation therapy with BCG following TURBT between NMIBC
patients with pyuria and those without pyuria. BCG treatment
suppressed recurrence in pyuria-negative patients. Therefore, the
presence of pyuria may be an independent predictor for BCG therapy
according to the multivariate analysis. The prophylactic effect of
BCG during the early phase (within 8 months) was weak in the
pyuria-positive group.
References
|
1
|
Brake M, Loertzer H, Horsch R and Keller
H: Recurrence and progression of stage T1, grade 3 transitional
cell carcinoma of the bladder following intravesical immunotherapy
with bacillus Calmette-Guérin. J Urol. 163:1697–1701. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brake M, Loertzer H, Horsch R and Keller
H: Long-term results of intravesical bacillus Calmette-Guérin
therapy for stage T1 superficial bladder cancer. Urology.
55:673–678. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lamm DL, van der Meijden PM, Morales A,
Brosman SA, Catalona WJ, Herr HW, Soloway MS, Steg A and Debruyne
FM: Incidence and treatment of complications of bacillus
Calmette-Guérin intravesical therapy in superficial bladder cancer.
J Urol. 147:596–600. 1992.PubMed/NCBI
|
|
4
|
Lima L, Dinis-Ribeiro M, Longatto-Filho A
and Santos L: Predictive biomarkers of bacillus Calmette-Guérin
immunotherapy response in bladder cancer: Where are we now? Adv
Urol. 2012:2326092012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Coussens LM and Werb Z: Inflammation and
cancer. Nature. 420:860–867. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Whiteside TL: The tumor microenvironment
and its role in promoting tumor growth. Oncogene. 27:5904–5912.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Azuma T, Nagase Y and Oshi M: Pyuria
predicts poor prognosis in patients with non-muscle-invasive
bladder cancer. Clin Genitourin Cancer. 11:331–336. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Echols RM, Tosiello RL, Haverstock DC and
Tice AD: Demographic, clinical, and treatment parameters
influencing the outcome of acute cystitis. Clin Infect Dis.
29:113–119. 1999. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mostofi FK, Sobin LH and Tosoni I:
Histological Typing of Urinary Bladder TumoursInternational
Histological Classification of Tumours, No 19. World Health
Organisation; Geneva: 1973
|
|
10
|
Nieder AM, Brausi M, Lamm D, O'Donnell M,
Tomita K, Woo H and Jewett MA: Management of stage T1 tumors of the
bladder: International Consensus Panel. Urology. 66:(Suppl 1).
108–125. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hagemann T, Balkwill F and Lawrence T:
Inflammation and cancer: A double-edged sword. Cancer Cell.
12:300–301. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Millán-Rodríguez F, Chéchile-Toniolo G,
Salvador-Bayarri J, Palou J, Algaba F and Vicente-Rodríguez J:
Primary superficial bladder cancer risk groups according to
progression, mortality and recurrence. J Urol. 164:680–684. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zuiverloon TC, Nieuweboer AJ, Vékony H,
Kirkels WJ, Bangma CH and Zwarthoff EC: Markers predicting response
to bacillus Calmette-Guérin immunotherapy in high-risk bladder
cancer patients: A systematic review. Eur Urol. 61:128–145. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Donskov F and von der Maase H: Impact of
immune parameters on long-term survival in metastatic renal cell
carcinoma. J Clin Oncol. 24:1997–2005. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ilie M, Hofman V, Ortholan C, Bonnetaud C,
Coëlle C, Mouroux J and Hofman P: Predictive clinical outcome of
the intratumoral CD66b-positive neutrophil-to-CD8-positive T-cell
ratio in patients with resectable nonsmall cell lung cancer.
Cancer. 118:1726–1737. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hinotsu S, Akaza H, Isaka S, et al: BCG
Tokyo 172 Strain Study Group: Sustained prophylactic effect of
intravesical bacille Calmette-Guérin for superficial bladder
cancer: A smoothed hazard analysis in a randomized prospective
study. Urology. 67:545–549. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lamm DL, Blumenstein BA, Crissman JD, et
al: Maintenance bacillus Calmette-Guérin immunotherapy for
recurrent TA, T1 and carcinoma in situ transitional cell carcinoma
of the bladder: A randomized Southwest Oncology Group Study. J
Urol. 163:1124–1129. 2000. View Article : Google Scholar : PubMed/NCBI
|