Introduction
Colorectal cancer (CRC) is a major cause of
cancer-related fatalities worldwide (1). In 2012, the American Cancer Society
estimated that 143,460 new cases of CRC would be diagnosed, and
51,690 would succumb to this disease (2). The majority of CRC-related fatalities
can be prevented through early diagnosis and surgical removal of
early-stage cancer. The five-year survival rates of CRC patients
range from <8% at stage IV to >93% at stage I (3). However, the majority of early-stage CRC
patients exhibit no symptoms. In addition, the available
methodologies for early detection are based on traditional
screening methods, such as the fecal occult blood test (FOBT) as
the primary screening tool, followed by colonoscopy for
FOBT-positive patients. However, these techniques have inherent
limitations. Although widely used, FOBT has poor sensitivity for
detecting early-stage CRC. Colonoscopy, despite its specificity and
sensitivity, is not suitable for the general population due to its
high cost, invasiveness, requirement for bowel preparation and
sedation, and association with medical complications. A stool DNA
test may be a promising alternative in the future, but the
widespread application of this technique is limited by
labor-intensive handling and high costs (4). Thus far, indicators that precisely
predict the presence of early-stage tumors are lacking. Therefore,
the development of new markers is urgently required for the rapid,
noninvasive, and highly sensitive screening of CRC patients.
MicroRNAs (miRNAs) are small (18–25 nucleotides)
noncoding RNAs that regulate the translation of specific genes
through sequence-specific binding to the 3′ untranslated region of
target mRNAs. MiRNAs reportedly have important roles in various
cellular processes that are commonly involved in cancer; these
processes include cell growth, differentiation, invasion,
angiogenesis and epithelial-mesenchymal transition (5,6). Due to
their oncogenic or tumor-suppressive properties, certain miRNAs
participate in carcinogenesis (7,8). A
previous study revealed the presence of large quantities of miRNAs
in serums. Circulating miRNAs can withstand unfavorable
physiological conditions, such as extreme variations in pH,
temperature, and multiple freeze/thaw cycles (9). Furthermore, the profiles of circulating
miRNAs show consistent expression levels across physiologically
healthy individuals (10). The
diagnostic value of circulating miRNAs for the early detection of
cancer has been successfully investigated in numerous malignancies,
including CRC. Therefore, miRNAs are potentially useful biomarkers
that may be sensitive and specific for the early detection of
CRC.
MicroRNA-21 (miR-21) is an oncomiRNA that modulates
the expression of multiple cancer-related target genes, such as
PTEN, TPM1 and PDCD. miR-21 is overexpressed
in various human tumors, particularly in the serum and tissue of
CRC patients (11). This finding
indicates that miR-21 can serve as a diagnostic marker for CRC.
Recent studies have investigated the diagnostic
value of miR-21 in CRC and have raised concerns regarding the
biomarker potential of miR-21. However, the findings of these
studies are inconsistent. Therefore, a meta-analysis of these
studies was conducted to assess the diagnostic value of miR-21 in
CRC.
Materials and methods
Search strategy
Several relevant literature databases (PubMed,
Embase, OvidSP, The Cochrane Library and Web of Science) and three
Chinese databases (Chinese National Knowledge Infrastructure, Wei
Pu DATA and Wan Fang DATA) were searched for studies that estimated
the diagnostic value of miR-21 in CRC. The key words for the
literature retrieval were ‘microRNA-21,’ ‘miR-21,’ ‘miRNA-21’ or
‘hsa-miR-21;’ ‘colorectal,’ ‘large intestine,’ ‘large bowel,’
‘colon,’ ‘colonic,’ ‘rectal’ or ‘rectum;’ and ‘cancer,’ ‘cancers,’
‘carcinoma,’ ‘carcinomas,’ ‘tumor,’ ‘tumors,’ ‘neoplasm’ or
‘neoplasms;’ and ‘serum,’ ‘sera,’ ‘serums,’ ‘blood,’ ‘plasma,’
‘plasmas’ or ‘circulating.’ To acquire additional relevant studies,
conference summaries, letters and other types of studies were
scanned in the initial search and certain authors were even
contacted to obtain additional information when necessary.
Selection criteria
Two reviewers (Y.W. and W.Z.H.) independently
assessed the literature extracted by the search strategy. Whenever
they had different opinions, the reviewers discussed until a
consensus was reached. The inclusion criteria were as follows: i)
CRC was diagnosed by pathological confirmation; ii) circulating
miR-21 concentration was tested; iii) no treatment, such as
radiotherapy or chemotherapy, was performed prior to blood
collection for miR-21 testing; iv) the data were sufficient to form
two-by-two tables; and v) healthy individuals or patients with
benign disease were included in the control group. The exclusion
criteria were as follows: i) Duplicate publications; ii)
unqualified data; and iii) reviews, letters and meetings. Studies
that met the above criteria were considered eligible.
Data extraction and quality
assessment
Two investigators (Y.W. and W.Z.H.) independently
identified and retrieved data from each study. The data extracted
for this systematic review included first author, publication year,
number of patients, ethnicity, country, test method, diagnostic
results and others.
Two investigators (Y.W. and W.Z.H.) scored the
quality of each study independently in accordance with the Quality
Assessment of Diagnostic Accuracy Studies (QUADAS) (12) tool (Table
I).
 | Table I.QUADAS assessment for the eligible
studies. |
Table I.
QUADAS assessment for the eligible
studies.
|
|
|
| Ogata-Kawata | Wang and | Basati |
| Toiyama | Kanaan | Zhang |
|
|---|
| Item no. | Description | Liu et al
(21) | et al
(22) | Zhang (20) | et al
(19) | Luo et al
(23) | et al
(24) | et al
(25) | et al
(26) | Du et al
(27) |
|---|
| 1 | Was the spectrum of
patients representative of the patients who will receive the test
in practice? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 2 | Were selection
criteria clearly described? | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 3 | Is the reference
standard likely to correctly classify the target condition? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 4 | Is the time period
between reference standard and index test short enough to be
reasonably sure that the target condition did not change between
the two tests? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 5 | Did the whole
sample or a random selection of the sample receive verification
using a reference standard? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 6 | Did patients
receive the same reference standard regardless of the index test
result? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 7 | Was the reference
standard independent of the index test (i.e., the index test did
not form part of the reference standard)? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 8 | Was the execution
of the index test described in sufficient detail to permit
replication of the test? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 9 | Was the execution
of the reference standard described in sufficient detail to permit
its replication? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 10 | Were the index test
results interpreted without knowledge of the results of the
reference standard? | No | No | No | No | No | No | No | No | No |
| 11 | Were the reference
standard results interpreted without knowledge of the results of
the index test? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 12 | Were the same
clinical data available when test results were interpreted as would
be available when the test is used in practice? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 13 | Were
uninterpretable/intermediate test results reported? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 14 | Were withdrawals
from the study explained? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Statistical analysis
For the diagnostic meta-analysis, true positive,
false positive, true negative and false negative were extracted as
bivariate data directly or through recalculation on the basis of
relative data from each eligible study. Subsequently, the bivariate
model was employed to analyze these data (13). A forest plot of sensitivity and
specificity was constructed; the positive-likelihood ratio (PLR),
negative-likelihood ratio (NLR), and diagnostic odds ratio (DOR)
were calculated; and the summary receiver operator characteristic
(SROC) curve was generated. The accuracy of the results was further
verified by applying the hierarchical summary receiver operating
characteristics (HSROC) model and subsequently presented the HSROC
curve (14). The HSROC curve
overcomes some of the deficiencies of the traditional SROC curve
reported by Moses et al (15).
Furthermore, the HSROC curve is closely associated with the
bivariate random-effect model. Heterogeneity between studies was
tested by χ2 and I2 statistics (16). The null hypothesis that the eligible
studies are homogeneous was rejected if P<0.05 or I2
>50% (17). Six factors that may
cause heterogeneity between studies were incorporated in the
bivariate model as covariates to explore the source of
heterogeneity by meta-regression analysis. Subgroup and sensitivity
analyses were also conducted to explore the source of heterogeneity
when necessary. The presence of publication bias was analyzed by
Deeks' funnel plot asymmetry test. Statistical significance was
considered, i.e., publication bias was present, at P<0.1. To
explore the threshold effect, the ROC plane and Spearman
correlation coefficient were employed. All the analyses were
conducted by Meta-DiSc and Stata SE12.0 software (18).
Results
Included studies
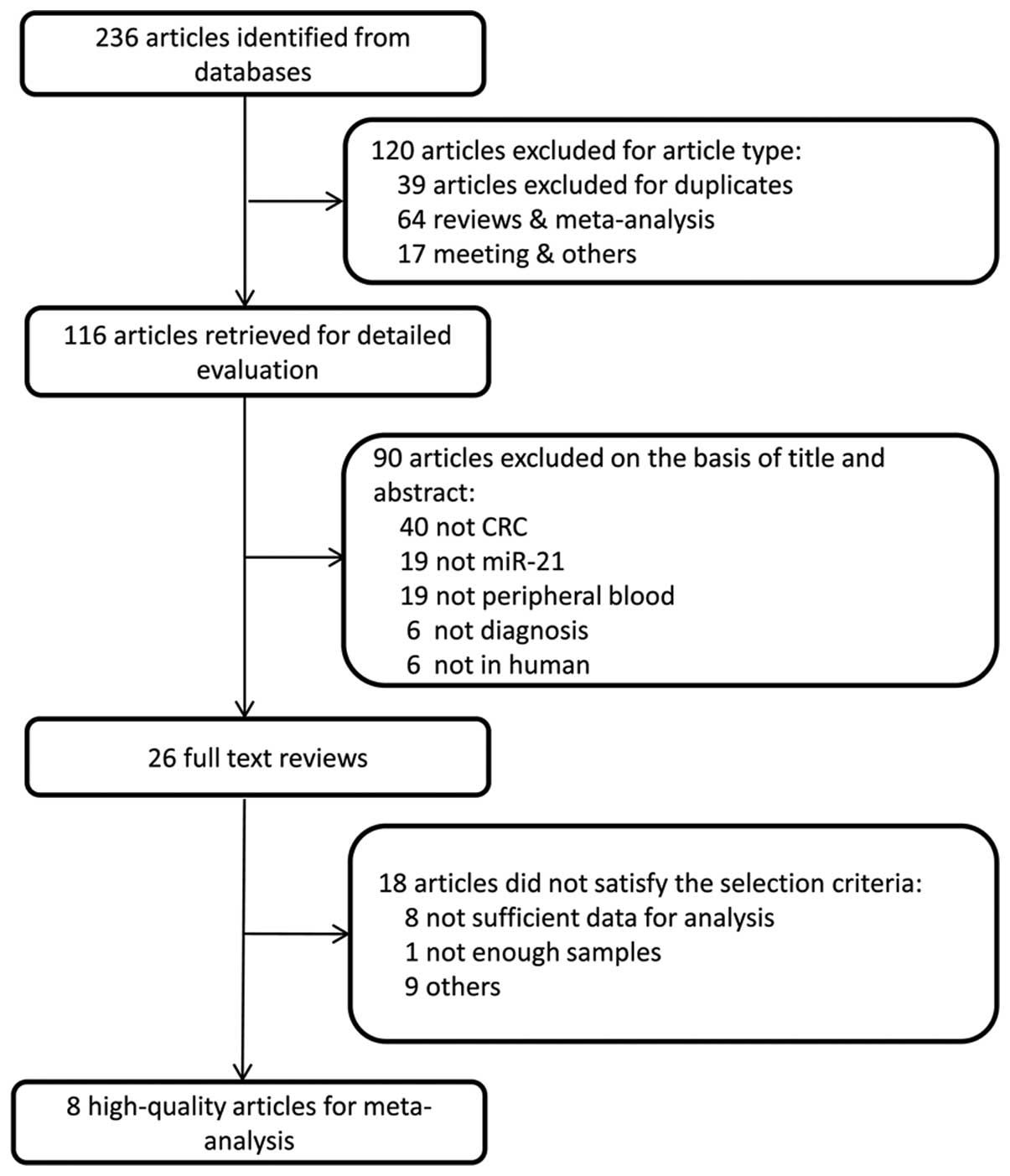
A total of 237 studies were initially retrieved.
Considering the study type, we excluded 120, including 39
duplicates, 64 reviews and meta-analyses, and 17 meetings and
others. A total of 117 studies were retained for the subsequent
evaluation. A total of 90 manuscripts were excluded on the basis of
the title and abstract, including 40 studies that did not focus on
CRC, 19 that did not focus on miR-21, 19 that did not focus on
blood samples, 6 unrelated to diagnosis, and 6 laboratory studies.
As a result, 27 adequate studies remained for the full text review.
Following reading the whole text, a further 18 studies were
excluded, 8 of which contained insufficient information. Finally, 9
studies (19–27) containing 1,222 samples remained for
the meta-analysis (Fig. 1).
Study characteristics and quality
assessment
In these selected studies, the 746 CRC patients had
been pathologically confirmed. Furthermore, the 476 control
individuals were healthy volunteers or patients with benign disease
who had never been diagnosed with malignancy. The studies enrolled
in the systemic review were conducted in China, Japan, Iran,
Germany and the USA. Among the 9 studies included, 6 were conducted
in Asian populations and 3 in Caucasian populations. The 9 studies,
which were published between 2012 and 2014, investigated the
diagnostic value of miR-21 for CRC. Furthermore, 8 of the 9 studies
used reverse transcription-quantitative polymerase chain reaction
(RT-qPCR) to assess the expression of miR-21. Among them, 6 used
TaqMan probe, 2 used the SYBR-Green assay, and 1 used an miRNA
microarray. The main characteristics of the eligible studies are
presented in Table II. The QUADAS
assessment tool was used to assess the quality of the 9 studies.
None of the studies conformed to the criteria that the index test
results should be interpreted without knowledge of the results of
the reference standard (item 10). One of the 9 studies did not
clearly describe their selection criteria (item 2) (Table I).
| Table II.Main characteristics of the eligible
studies. |
Table II.
Main characteristics of the eligible
studies.
| First author,
year | Patients, n
(controls, n) | Ethnicity | Country | RNA extraction
kits | Test method | AUC | QUADAS scores | Se% | Sp% | (Refs.) |
|---|
| Liu, 2013 | 200 (80) | Asian | China | Trizol-LS | RT-qPCR
(Taqman) | 0.802 | 13 | 65 | 85 | (21) |
| Ogata-Kawata,
2014 | 88 (11) | Asian | Japan | Trizol-LS | miRNA
microarray | 0.798 | 12 | 61.4 | 90.9 | (22) |
| Toiyama, 2013 | 186 (53) | Asian | Japan | miRNeasy RNA | RT-qPCR (Taqman)
isolation kits | 0.927 | 13 | 82.8 | 90.6 | (24) |
| Kanaan, 2012 | 30 (30) | Caucasian | America | Trizol-LS | RT-qPCR
(Taqman) | 0.82 | 13 | 90 | 90 | (25) |
| Wang, 2012 | 32 (39) | Asian | China | Trizol-LS | RT-qPCR
(SYBR-Green) | 0.85 | 13 | 87.5 | 74.4 | (20) |
| Basati, 2014 | 40 (40) | Caucasian | Iran | mirVana | RT-qPCR
(SYBR-Green) PARIS kit | 0.87 | 13 | 77 | 78 | (19) |
| Luo, 2013 | 80 (144) | Caucasian | Germany | Combination of
Trizol LS and miRNeasy mini kit | RT-qPCR
(Taqman) | 0.6528 | 13 | 51.7 | 80.7 | (23) |
| Zhang, 2014 | 41 (30) | Asian | China | Trizol-LS | RT-qPCR
(Taqman) | 0.657 | 13 | 51.2 | 79 | (26) |
| Du, 2014 | 49 (49) | Asian | China | Trizol-LS | RT-qPCR
(Taqman) | 0.877 | 13 | 76.2 | 93.2 | (27) |
Data analysis
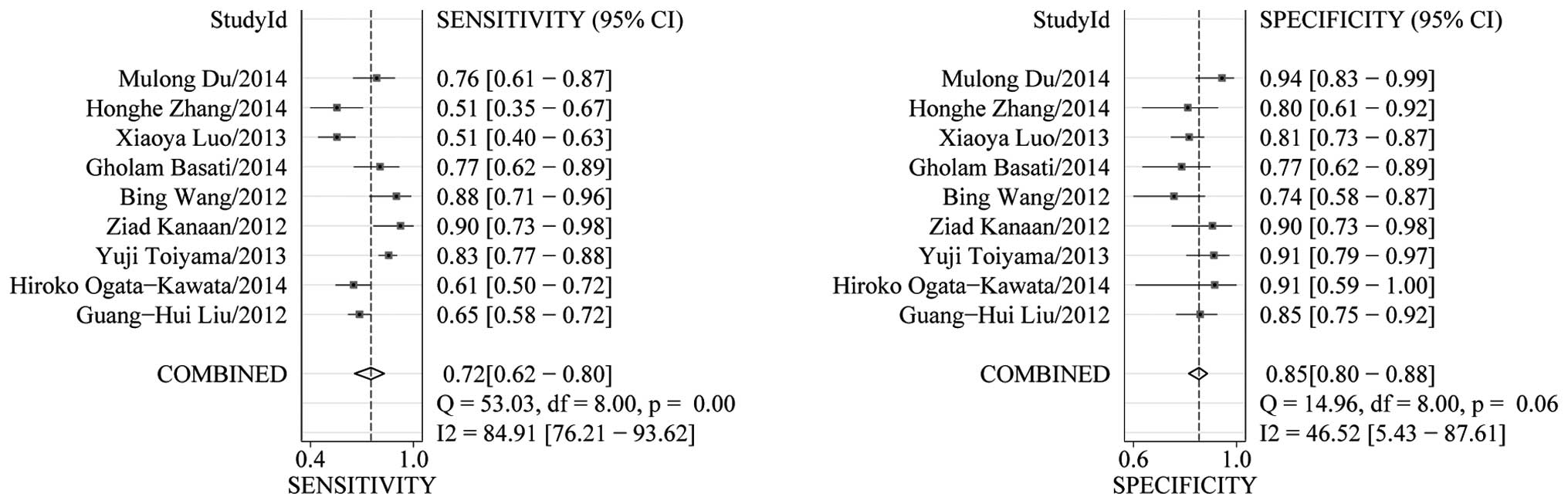
Heterogeneity in sensitivity and specificity was
detected in the 9 studies (I2=84.91% and
I2=46.52%, respectively), suggesting significant
heterogeneity in sensitivity and mild heterogeneity in specificity
(Fig. 2). Therefore, the random
effects model was employed in this study. The analysis results
showed that the pooled sensitivity and specificity of miR-21 for
CRC diagnosis were 72% (95% CI, 62–80) and 85% (95% CI, 80–88),
respectively.
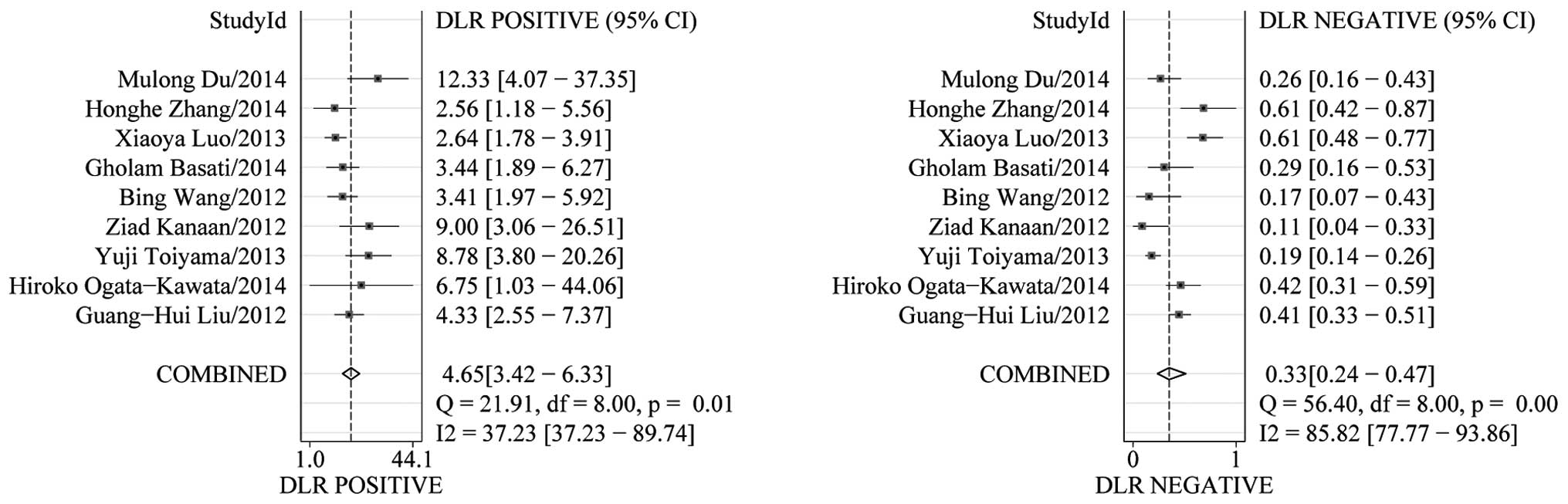
The PLR and NLR of serum miR-21 were calculated for
the likelihood ratio; these parameters have been considered more
clinically valuable compared to the specificity and sensitivity
(28). PLR >10 or NLR <0.1
suggests high diagnostic accuracy. In the present study, the pooled
PLR is 4.65 (95% CI, 3.42–6.33; I2=37.23%), indicating
that the CRC patients have more than a four-fold probability to
express miR-21 in comparison to healthy individuals. The pooled NLR
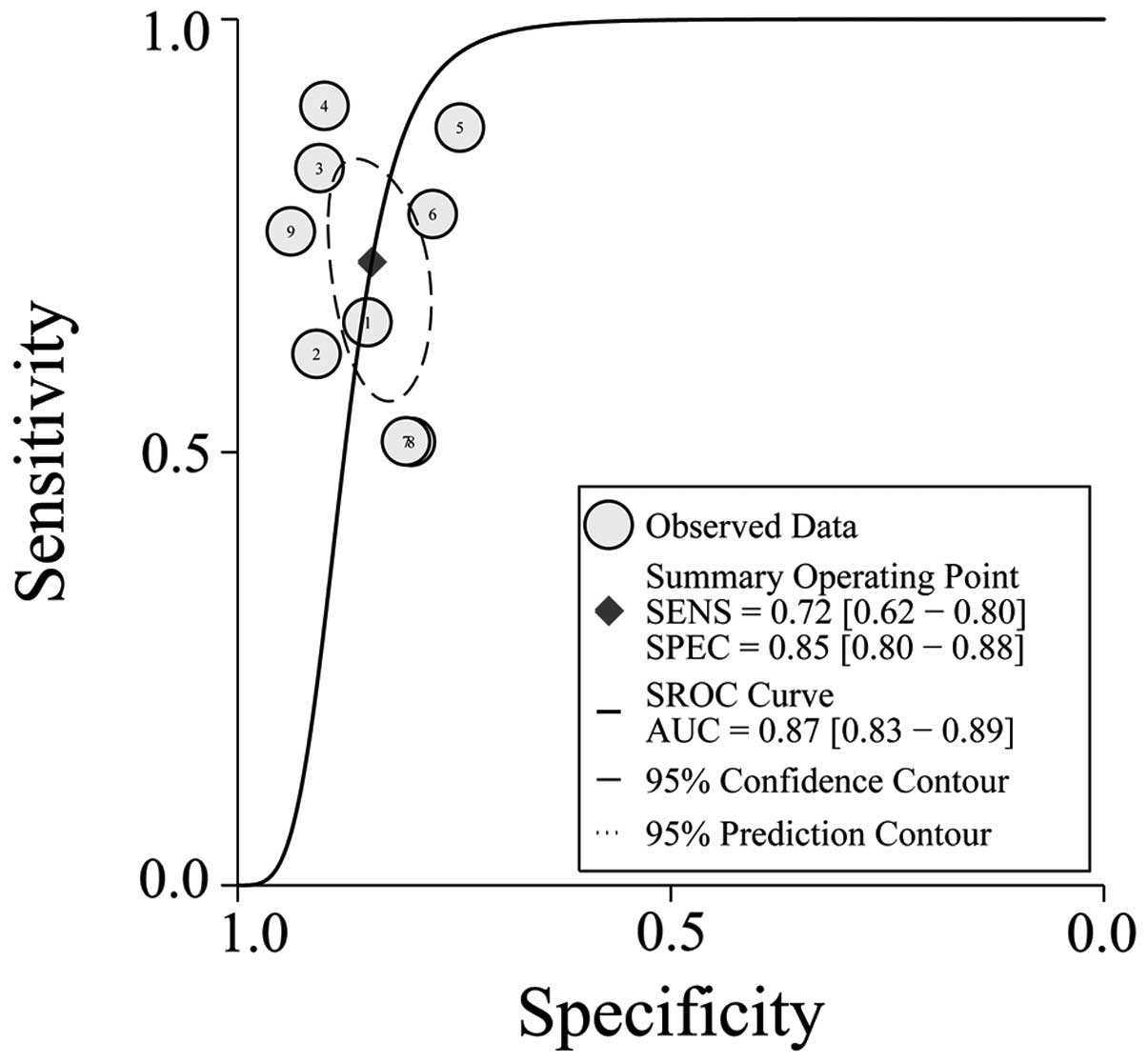
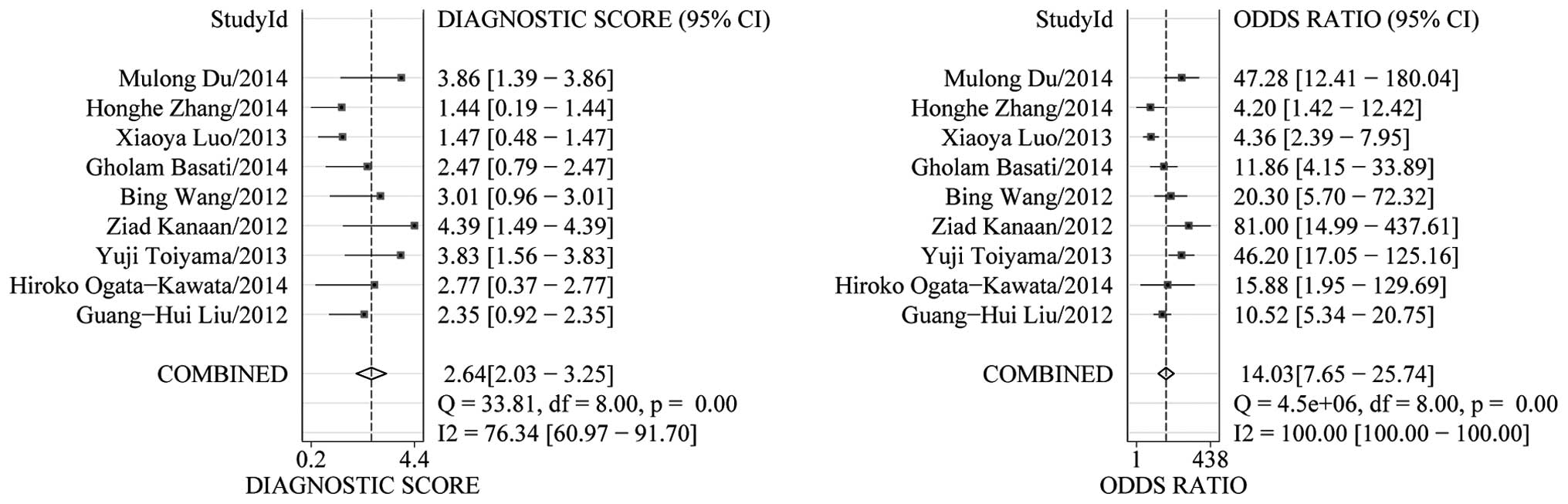
was 0.33 (95% CI, 0.24–0.47; I2=85.82%) (Fig. 3). The SROC curve of the selected
studies is shown in Fig. 4. The AUC
was 0.87 (95% CI, 0.83–0.89). The DOR value was 14.03 (95% CI,
7.65–25.74), indicating that miR-21 can be used as a good marker
for CRC diagnosis (Fig. 5).
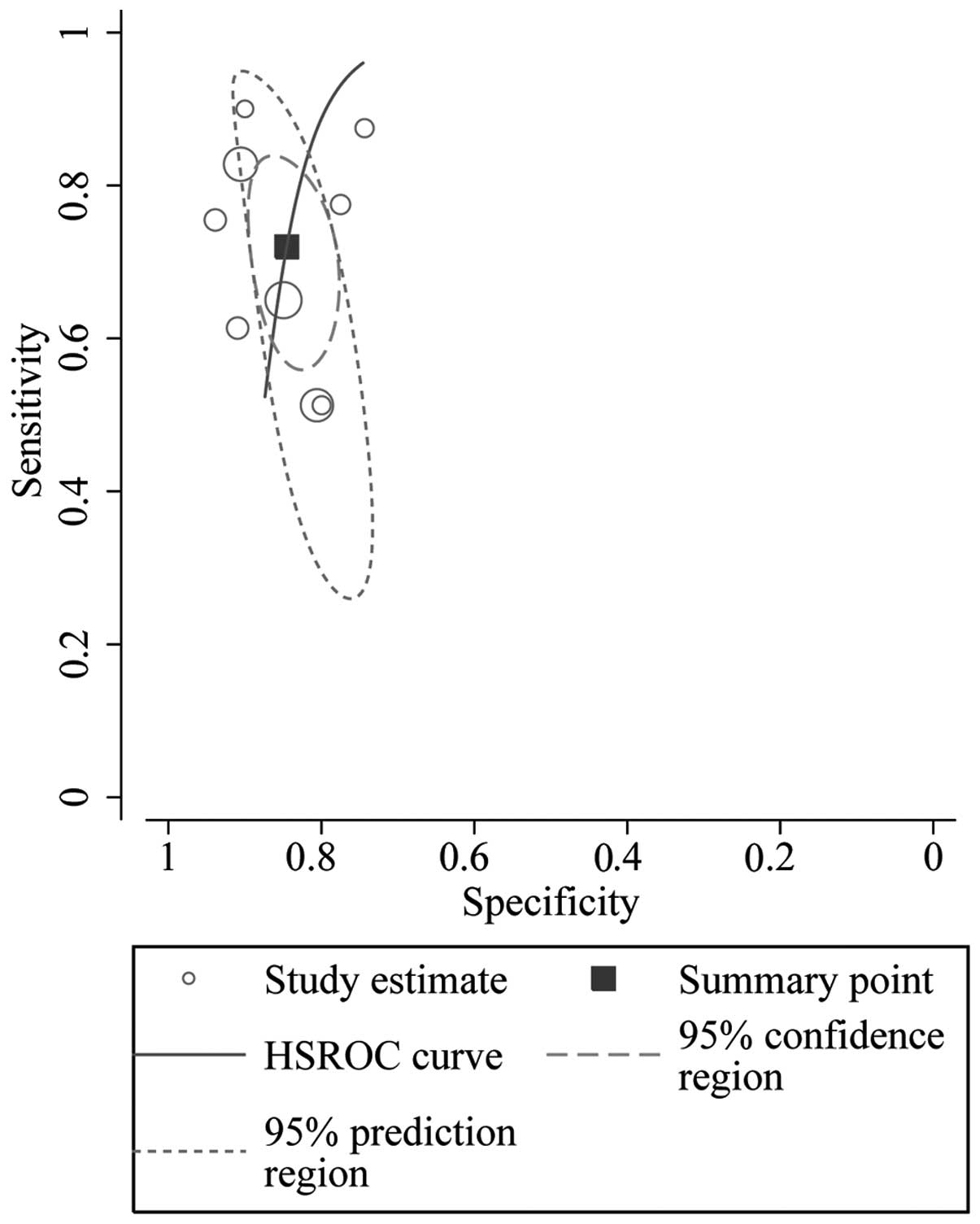
The HSROC curve of the selected studies is shown in
Fig. 6, which is consistent with the
results from the bivariate model. The summary operating point
estimate of sensitivity and specificity is also presented. The 95%
prediction and 95% CI are also plotted. The cut-off point was
located near the upper left corner of the HSROC curve. The value of
β was −1.28, and the P-value was 0.152. This result indicates that
the HSROC is symmetrical. The value of γ, which helps distinguish
CRC patients from healthy individuals, was 3.941 (2.295–5.588).
This result indicates that circulating miR-21 is a relatively
accurate diagnostic marker for CRC.
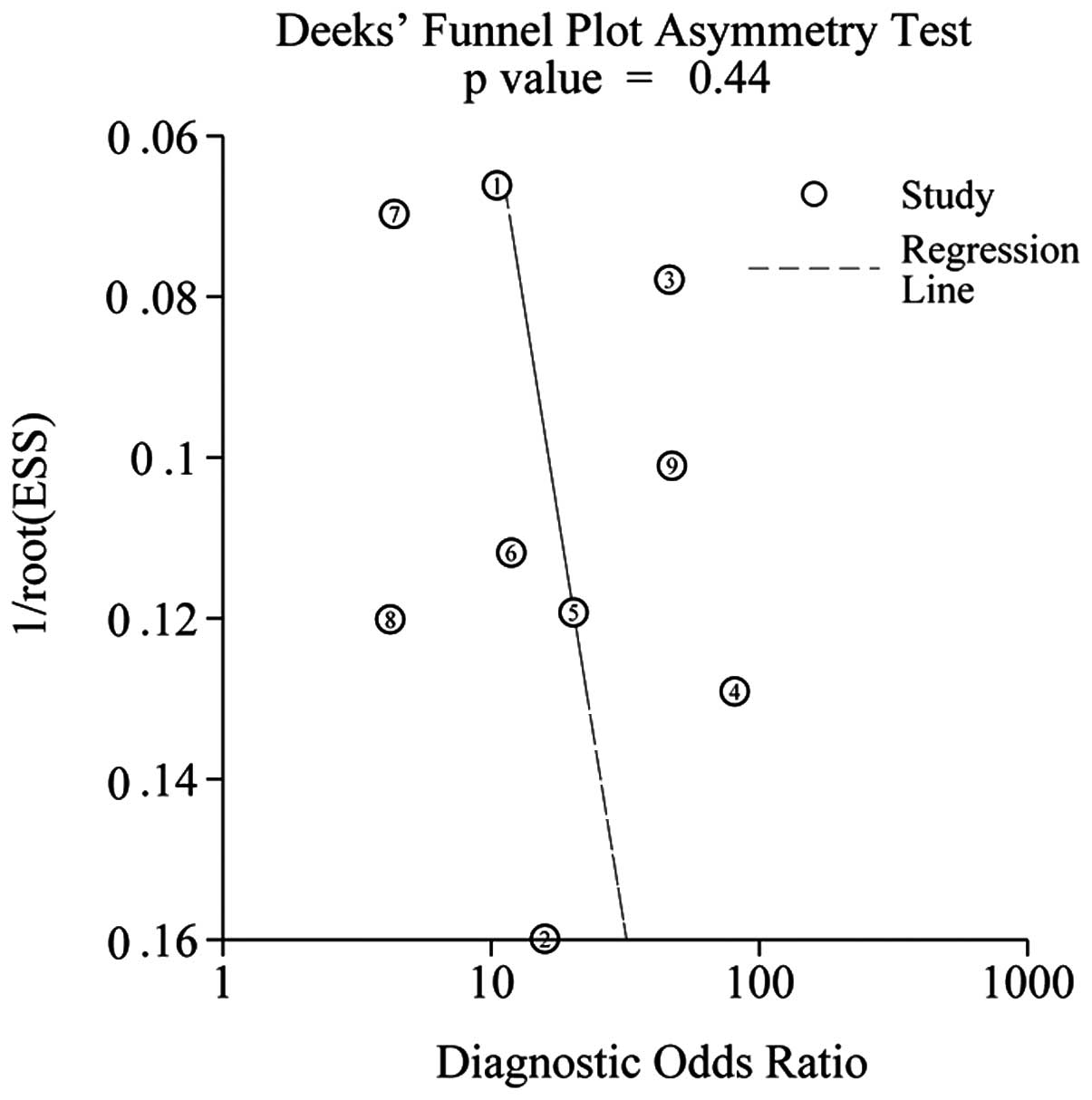
Publication bias
Deeks' funnel plots were used to evaluate the
presence of publication bias in this meta-analysis. The funnel plot
presents no asymmetry (Fig. 7). The
P-value was 0.44, indicating the absence of publication bias in the
meta-analysis. However, concluding whether or not publication bias
exists is difficult due to the limited number of studies involved
in the current meta-analysis.
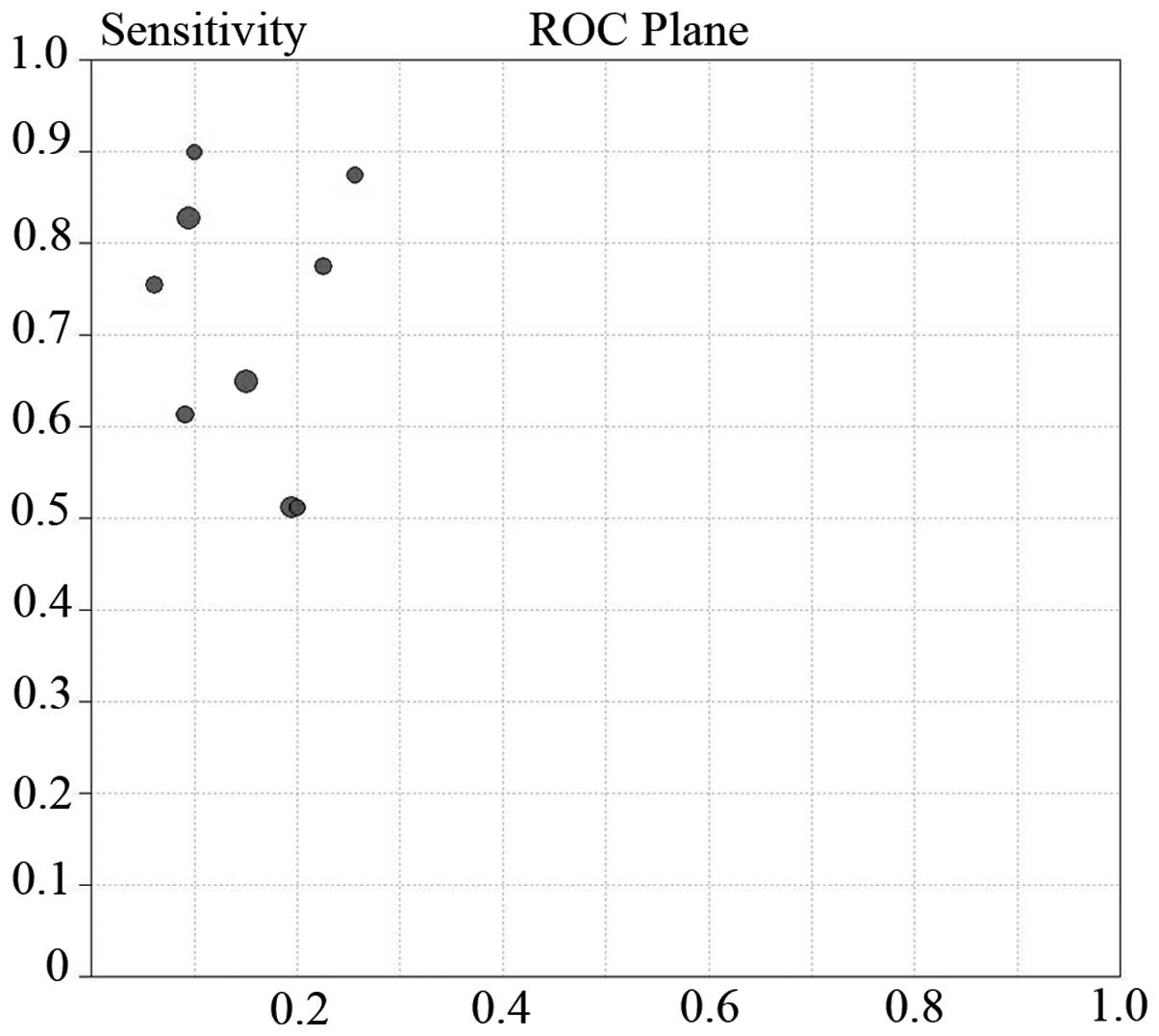
Threshold effect and
heterogeneity
Differences in cut-off values cause the threshold
effect. The ROC plane and Spearman rank correlation test is a good
approach to assess the threshold effect (18). In the present study, the
representation of the sensitivity against the specificity of each
study is shown in an ROC space (Fig.
8), which can be used to detect the threshold effect. The
pattern of the points in this figure does not suggest a
‘shoulder-arm’ shape, indicating the absence of the threshold
effect. A Spearman rank correlation was conducted and the absence
of heterogeneity was validated from the threshold effect [Spearman
correlation coefficient=0.033; P=0.932 (P>0.05)].
The I2 of the heterogeneity test is 59%,
suggesting moderate heterogeneity. The publication year, test
method, RNA extraction kits, ethnicity, patient number and QUADAS
score may contribute to heterogeneity. Meta-regression analysis
suggests that the above factors are not the sources of
heterogeneity in this study. Subsequently, a subgroup analysis was
performed on ethnicity, test method and RNA extraction kits;
however, the sources of heterogeneity could not be identified. A
sensitivity analysis was also performed, but failed to find the
sources of heterogeneity.
Discussion
Recent studies have revealed novel diagnostic
biomarkers for CRC, including miR-21. miR-21 is an important
oncogenic microRNA that participates in tumor initiation,
progression and metastasis. Therefore, the present meta-analysis
was performed to provide an integrated and up-to-date evaluation of
the diagnostic and clinical values of miR-21 as a serum marker for
CRC.
In the present meta-analysis, the combined
sensitivity and specificity were 72% (95% CI, 62–80) and 85% (95%
CI, 80–88), respectively, which imply moderate sensitivity and good
specificity. The 2014 NCCN Guidelines for CRC screening highlighted
that any positive stool test requires follow-up with a colonoscopy.
miR-21 can potentially replace FOBT or serve as a powerful
diagnostic tool for CRC. The DOR value reflects the extent of the
association between the diagnostic results and the disease. DOR
>1 means better discrimination of the index test. DOR <1
means healthy individuals are more likely to be diagnosed as
positive by the index test compared to CRC patients. DOR=1 means
the index test cannot discriminate healthy individuals and CRC
patients. In the present meta-analysis, the DOR value was 14.03,
suggesting that miR-21 can serve as a promising diagnostic
biomarker for CRC. When the threshold effect exists among studies,
the SROC curve appears to be a better method to assess the summary
diagnostic accuracy of the test rather than pooled sensitivity,
pooled specificity, pooled PLR or pooled DOR. AUC is usually
calculated to assess the accuracy of the selected indicator. The
closer the value of AUC is to 1, the better the diagnostic accuracy
of the test. By contrast, the closer the value of AUC is to 0.5,
the worse the diagnostic accuracy of the test. In the present
study, the AUC was 0.87, which indicates that miR-21 demonstrates
good accuracy for CRC diagnosis. The HSROC model yields similar
sensitivity (72.0%) and specificity (84.5%). This result further
demonstrates the reliability of the meta-analysis. Overall, miR-21
has a moderate sensitivity and good specificity for CRC
diagnosis.
Heterogeneity is a potential problem that can
influence the incorporation effect and the interpretation of the
meta-analysis results. Although strict inclusion and exclusion
criteria were set to gain eligible studies, heterogeneity exists
due to the existence of certain potential confounding factors.
However, a broad range of sensitivity and specificity was reported.
One cause of heterogeneity is the threshold effect, which arises
due to different cut-off values used in different studies to define
a negative or positive test result. Considering that the 9 studies
used different cut-off values, the ROC plane and Spearman rank
correlation test were employed to analyze the threshold effect. The
ROC plane suggests no ‘shoulder-arm’ shape, and the Spearman
correlation coefficient was 0.033 (P=0.932 and >0.05). This
result demonstrates that threshold effect is not the source of
heterogeneity. The patients involved in the present meta-analysis
were from different ethnicities and populations. Not all the
detection methods for miR-21 are based on RT-PCR and RT-qPCR.
Ogata-Kawata et al (22) used
miRNA microarray. Even with RT-qPCR, 6 studies used TaqMan probes
and 2 used the SYBR-Green assay. The RNA extraction kits and
normalizers also varied. Heterogeneity may result from different
laboratories using different methods to quantify miR-21. Therefore,
a meta-regression analysis was conducted to evaluate the
contribution of the factors above. However, no heterogeneity was
detected from these factors. Subsequently, a subgroup analysis was
conducted on the ethnicity, test method and RNA extraction kits. In
every subgroup, heterogeneity remained, indicating that these
factors were not the sources of heterogeneity.
Zhang et al (26) and Du et al (27) also conducted a meta-analysis on the
diagnostic value of miR-21 for CTC. Zhang et al (26) reported a pooled sensitivity of 76% and
a pooled specificity of 81%. Du et al (27) reported a pooled sensitivity of 76% and
a pooled specificity of 82%. The present results were similar to
theirs, but not identical. They included only 6 studies, whereas 9
were included in the present meta-analysis. Du et al
(27) retained 2 studies of Toiyama
et al (24), but 1 of them
appears to be a poster presentation. Additionally, the 2 studies
were published with an interval of 1 year, which make them
potential duplicates or overlapping data. Thus, 1 of these 2
studies was excluded in the present meta-analysis. Zhang et
al (26) reported that different
cut-off values of miR-21 expression across studies may be a source
of heterogeneity. However, they did not demonstrate it further. In
the present meta-analyses, ROC plane and Spearman rank correlation
were performed, and verified that the threshold effect was not a
source of heterogeneity.
miR-21 is overexpressed in numerous other solid
types of tumor, indicating that its biology is relevant to numerous
types of cancer (29,30). Zeng et al (31) reported that miR-21 had a sensitivity
of 66.5% and a specificity of 83.1% in gastric cancer. Yang et
al (32) summarized that the
sensitivity and specificity of miR-21 in lung cancer were 71% and
84%, respectively. Other studies reported that miR-21 is
upregulated in breast cancer, esophageal cancer, pancreatic cancer
and glioblastoma (20). miR-21 is
unlikely to become a useful blood-based biomarker for diagnosing
CRC as an individual miRNA as it is also dysregulated in other
diseases (33). Overall, miR-21 is
not a special biomarker in CRC; it requires to be combined with
another tool for enhanced specificity.
Certain limitations exist in the present study.
First, the majority of these studies are retrospective analyses on
historical cohorts, which limit the conclusions due to inherent
study bias. Therefore, prospective studies that investigate the
association between miR-21 and CRC are necessary. Second, evidence
that demonstrates the existence of publication bias (P=0.436 for
Deeks' test) by funnel plots is lacking. However, the independent
patient data of several studies with negative results could not be
collected, despite extensively searching other associated
references and contacting authors via fax and e-mail. These may
have been missed in the meta-analysis, indicating that publication
bias may remain. However, current evidence indicates that
circulating miR-21 has moderate sensitivity and good specificity as
a diagnostic marker for CRC diagnosis. Large-scale prospective
studies must be conducted in the future for verification. In
addition, improving the diagnostic accuracy of circulating miR-21
and exploring new biomarkers with high diagnostic accuracy in CRC
should still be considered in the future. miR-21-related
diagnostics have substantial potential for the prevention and
treatment of CRC.
Acknowledgements
The present study was funded by the National Natural
Science Foundation of China [contract nos. 81071823 and 81201811]
and Zhejiang University Research foundation, China [contract no.
11-491020-110].
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
O'Connell JB, Maggard MA and Ko CY: Colon
cancer survival rates with the new American joint committee on
cancer sixth edition staging. J Natl Cancer Inst. 96:1420–1425.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Collins JF, Lieberman DA, Durbin TE and
Weiss DG: Veterans Affairs Cooperative Study #380 Group: Accuracy
of screening for fecal occult blood on a single stool sample
obtained by digital rectal examination. A comparison with
recommended sampling practice. Ann Intern Med. 142:81–85. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Calin GA and Croce CM: MicroRNA signatures
in human cancers. Nat Rev Cancer. 6:857–866. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Esquela-Kerscher A and Slack FJ:
Oncomirs-microRNAs with a role in cancer. Nat Rev Cancer.
6:259–269. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wiemer EA: The role of microRNAs in
cancer: N o small matter. Eur J Cancer. 43:1529–1544. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lu J, Getz G, Miska EA, Alvarez-Saavedra
E, Lamb J, Peck D, Sweet-Cordero A, Ebert BL, Mak RH, Ferrando AA,
et al: MicroRNA expression profiles classify human cancers. Nature.
435:834–838. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mitchell PS, Parkin RK, Kroh EM, Fritz BR,
Wyman SK, Pogosova-Agadjanyan EL, Peterson A, Noteboom J, O'Briant
KC, Allen A, et al: Circulating microRNAs as stable blood-based
markers for cancer detection. Proc Natl Acad Sci USA.
105:10513–10518. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Duttagupta R, Jiang R, Gollub J, Getts RC
and Jones KW: Impact of cellular miRNAs on circulating miRNA
biomarker signatures. PloS one. 6:e207692011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schetter AJ and Harris CC: Plasma
microRNAs: A potential biomarker for colorectal cancer? Gut.
58:1318–1319. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Whiting P, Rutjes AW, Reitsma JB, Bossuyt
PM and Kleijnen J: The development of QUADAS, A tool for the
quality assessment of studies of diagnostic accuracy included in
systematic reviews. BMC Med Res Methodol. 3:252003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Reitsma JB, Glas AS, Rutjes AW, Scholten
RJ, Bossuyt PM and Zwinderman AH: Bivariate analysis of sensitivity
and specificity produces informative summary measures in diagnostic
reviews. J Clin Epidemiol. 58:982–990. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rutter CM and Gatsonis CA: A hierarchical
regression approach to meta-analysis of diagnostic test accuracy
evaluations. Stat Med. 20:2865–2884. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Moses LE, Shapiro D and Littenberg B:
Combining independent studies of a diagnostic test into a summary
ROC curve, Data-analytic approaches and some additional
considerations. Stat Med. 12:1293–1316. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dinnes J, Deeks J, Kirby J and Roderick P:
A methodological review of how heterogeneity has been examined in
systematic reviews of diagnostic test accuracy. Health Technol
Assess. 9(iii): 1–113. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zamora J, Abraira V, Muriel A, Khan K and
Coomarasamy A: Meta-DiSc: A software for meta-analysis of test
accuracy data. BMC Med Res Methodol. 6:312006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Basati G, Razavi Emami A, Abdi S and
Mirzaei A: Elevated level of microRNA-21 in the serum of patients
with colorectal cancer. Medical Oncol. 31:2052014. View Article : Google Scholar
|
|
20
|
Wang B and Zhang Q: The expression and
clinical significance of circulating microRNA-21 in serum of five
solid tumors. J Cancer Res Clin Oncol. 138:1659–1666. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Liu GH, Zhou ZG, Chen R, Wang MJ, Zhou B,
Li Y and Sun XF: Serum miR-21 and miR-92a as biomarkers in the
diagnosis and prognosis of colorectal cancer. Tumour Biol.
34:2175–2181. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ogata-Kawata H, Izumiya M, Kurioka D,
Honma Y, Yamada Y, Furuta K, Gunji T, Ohta H, Okamoto H, Sonoda H,
et al: Circulating exosomal microRNAs as biomarkers of colon
cancer. PloS one. 9:e929212014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Luo X, Stock C, Burwinkel B and Brenner H:
Identification and evaluation of plasma microRNAs for early
detection of colorectal cancer. PloS One. 8:e628802013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Toiyama Y, Takahashi M, Hur K, Nagasaka T,
Tanaka K, Inoue Y, Kusunoki M, Boland CR and Goel A: Serum miR-21
as a diagnostic and prognostic biomarker in colorectal cancer. J
Natl Cancer Inst. 105:849–859. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kanaan Z, Rai SN, Eichenberger MR, Roberts
H, Keskey B, Pan J and Galandiuk S: Plasma miR-21: A potential
diagnostic marker of colorectal cancer. Ann Surg. 256:544–551.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhang H, Li P, Ju H, Pesta M, Kulda V, Jin
W, Cai M, Liu C, Wu H, Xu J, et al: Diagnostic and prognostic value
of micro RNA-21 in colorectal cancer: An original study and
individual participant data meta-analysis. Cancer Epidemiol
Biomarkers Prev. 23:2783–2792. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Du M, Liu S, Gu D, Wang Q, Zhu L, Kang M,
Shi D, Chu H, Tong N, Chen J, et al: Clinical potential role of
circulating microRNAs in early diagnosis of colorectal cancer
patients. Carcinogenesis. 35:2723–2730. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Rosenfeld RM and Shiffman RN: Clinical
practice guidelines: A manual for developing evidence-based
guidelines to facilitate performance measurement and quality
improvement. Otolaryngol Head Neck Surg. 135((Suppl 4)): S1–S28.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Volinia S, Calin GA, Liu CG, Ambs S,
Cimmino A, Petrocca F, Visone R, Iorio M, Roldo C, Ferracin M, et
al: A microRNA expression signature of human solid tumors defines
cancer gene targets. Proc Natl Acad Sci USA. 103:2257–2261. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Selcuklu SD, Donoghue MT and Spillane C:
miR-21 as a key regulator of oncogenic processes. Biochem Soc
Trans. 37:918–925. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zeng Z, Wang J, Zhao L, Hu P, Zhang H,
Tang X, He D, Tang S and Zeng Z: Potential role of microRNA-21 in
the diagnosis of gastric cancer, A meta-analysis. PloS One.
8:e732782013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yang X, Guo Y, Du Y, Yang J, Li S, Liu S,
Li K and Zhang D: Serum microRNA-21 as a diagnostic marker for lung
carcinoma, A systematic review and meta-analysis. PloS One.
9:e974602014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Krichevsky AM and Gabriely G: miR-21: A
small multi-faceted RNA. J Cell Mol Med. 13:39–53. 2009. View Article : Google Scholar : PubMed/NCBI
|