Introduction
Bone marrow metastasis from malignant solid tumors
may be occasionally encountered, particularly with cancers of the
breast, stomach and prostate gland (1). Decreased blood cell count and abnormal
coagulation status are often observed in cases with bone marrow
metastasis from malignant tumors, and disseminated intravascular
coagulation (DIC) or thrombotic thrombocytopenic purpura (TTP)
occasionally develop. Supportive therapy against the abnormal
coagulation status alone is inadequate in patients with DIC
precipitated by malignancy, and simultaneous appropriate
chemotherapy against the tumor is required to improve the
coagulation abnormalities. Specific chemotherapeutic regimens
against bone marrow metastasis have not been developed, and the
majority of such patients have a poor prognosis (2–4).
Colorectal cancer (CRC) is the third cause of
cancer-related mortality worldwide (5). Approximately 40% of CRC patients
present with distant metastases, either at diagnosis or during the
course of treatment. Metastasis frequently affects the liver,
abdominal lymph nodes, lungs and peritoneum. Systemic chemotherapy
is employed as a standard therapy and the effectiveness of
chemotherapy has recently improved in association with the use of
cytotoxic and molecular-targeted agents.
However, a limited number of CRC cases were reported
to clinically exhibit bone marrow metastases (6–10). The
majority of these cases displayed hematological disorders,
including thrombocytopenia, DIC, TTP and microangiopathic hemolytic
anemia. The general condition of the patients tended to be poor and
metastasis was also observed in organs other than the bone marrow,
such as the liver, lymph nodes and lungs. The efficacy of systemic
chemotherapy against CRC with bone marrow metastasis appears to be
poor, and the prognosis for such patients is unfavourable. Only 10
cases of CRC with bone marrow metastasis have been reported
(6) and the common molecular
characteristics of these cases have not been identified.
Our patient presented with metastasis of sigmoid
colon cancer to the bone marrow and systemic chemotherapy achieved
satisfactory disease control. We herein present the
immunohistochemical and molecular biological analyses of the
primary and metastatic sites in this case and compare the findings
with those of previous reports.
Case report
A 60-year-old man presented with a 4-week history of
persistent lower back pain, anorexia and difficulty defecating. The
patient visited a local doctor complaining of abdominal pain and
blood in the stool. He had a 40-pack-year history of smoking and a
drinking history of 1 glass of beer per day; his medical history
was otherwise non-significant. The family history included lung and
gastric cancer in his father, and pancreatic cancer in his mother.
Due to the presence of severe thrombocytopenia and
erythroblastosis, suggesting a hematological malignancy, the
patient was referred to the National Hospital Organization Kyushu
Cancer Center (Fukuoka, Japan) in December, 2014. The Eastern
Cooperative Oncology Group performance status (PS) was 2 and the
axillary temperature was 37.9°C. Other vital signs were within the
normal range. Lower abdominal pain was present, without
subcutaneous hemorrhage. Blood testing revealed a decreased red
blood cell count of 3.05×106/µl, a decreased hemoglobin
level of 9.6 g/dl, an increased white blood cell of
13.85×103/µl and a decreased platelet count at
5×103/µl. Analysis of the coagulation system revealed a
prolonged prothrombin time-international normalization ratio (1.39)
and increased levels of fibrin/fibrinogen degradation product-P
(209.02 µg/ml) and D-dimer (168.17 µg/ml). DIC was diagnosed based
on a score of 9 according to the criteria of the Ministry of
Health, Labour and Welfare of Japan (11). Serum biochemistry revealed elevated
levels of lactate dehydrogenase at 1,359 IU/l and C-reactive
protein at 14.91 mg/dl. The serum levels of carcinoembryonic
antigen (CEA; 46.4 ng/ml), soluble interleukin 2 receptor (1,364
U/ml) and cytokeratin 19 fragment (CYFRA; 78.3 ng/ml) were also
elevated.
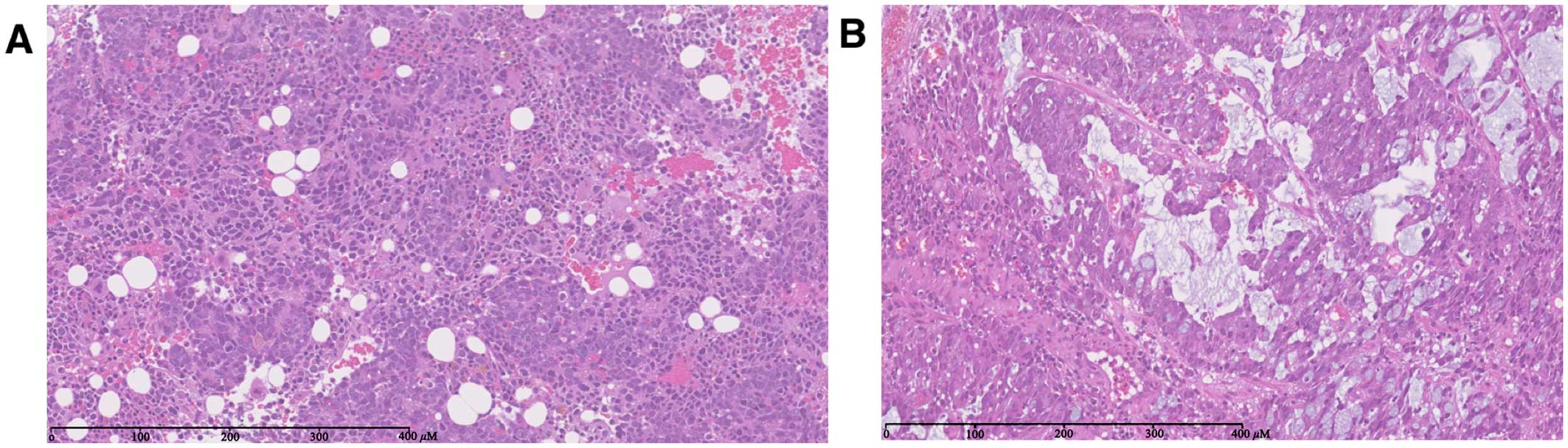
Although hematological malignancy was suspected, an
aspiration biopsy from the bone marrow revealed moderately to
poorly differentiated adenocarcinoma, without leukemic cells
(Fig. 1A). Immunohistochemical
examination revealed that the tumor cells were negative for
cytokeratin (CK) 7 and positive for CK20 and caudal type homeobox
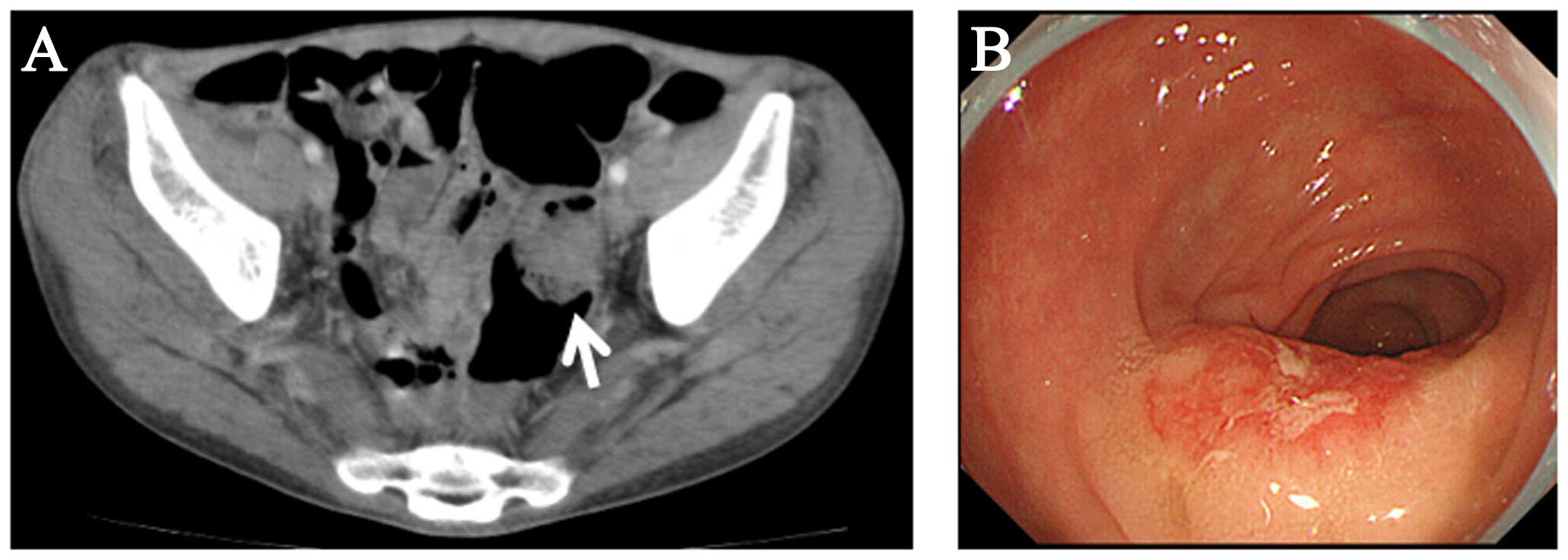
transcription factor 2 (CDX2). Computed tomography (CT) revealed
thickening of the sigmoid colon wall and para-aortic, hilar,
mediastinal and right supraclavicular lymphadenopathy (Fig. 2A). Moreover, osteolytic lesions were
detected diffusely in all the vertebrae and the ilium. Although
colonoscopy was not performed due to severe thrombocytopenia,
sigmoid colon cancer with metastases to the lymph nodes and bone
marrow was diagnosed. Chemotherapy using a modified FOLFOX6
(mFOLFOX6) regimen for advanced sigmoid colon cancer was promptly
initiated, but the dose of the chemotherapeutic agents was reduced
to 75% due to worsening of the thrombocytopenia. Supportive
therapies comprising transfusion of thrombocytes and administration
of gabexate mesilate to control DIC were performed simultaneously.
Bevacizumab was not initially administered due to the risk of
hemorrhagic events. The number of thrombocytes increased to
61×103/µl after 3 cycles of chemotherapy and the serum
CEA and CYFRA levels decreased to 5.4 and 2.4 ng/ml, respectively.
Common Terminology Criteria of Adverse Events v.4.0 grade 3
neutropenia and grade 3 anemia appeared, but resolved within a few
days (12). The patient underwent
colonoscopy following recovery from DIC. A sigmoid colon tumor was
detected (Fig. 2B) and biopsy of the
tumor revealed poorly differentiated adenocarcinoma (Fig. 1B), without mutations of the
RAS, BRAF or PIK3CA oncogenes. On
immunohistochemical analysis, the tumor cells were negative for CK7
and positive for CK20 and CDX2. The patient was treated with 3
cycles of mFOLFOX6, followed by 5 cycles of CapeOX (oral
capecitabine at 2,000 mg/day on days 1–14 and intravenous
oxaliplatin at 130 mg/m2 on day 1, every 3 weeks),
achieving shrinkage of the tumor. However, a new lesion was
detected at the ninth thoracic vertebra on CT after 150 days of
treatment. Subsequently, combination chemotherapy using irinotecan
and panitumumab was initiated. The PS improved, but progression of
the primary lesion and lymphadenopathy was observed after 8 cycles.
Although third-line treatment with trifluridine/tipiracil
hydrochloride (110 mg/day per os on days 1–5 and 8–13, every
4 weeks) was initiated, the disease progressed and the patient
succumbed to the disease 10 months after the diagnosis. Informed
consent was obtained from the patient for the publication of the
case details prior to treatment initiation.
Discussion
Malignant solid tumors may invade the bone marrow,
particularly in patients with cancer of the breast, stomach and
prostate gland (1). Only a small
percentage of breast cancer cases present with bone marrow
metastasis at initial diagnosis, but 36% develop this complication
during the course of the disease (13). Poorly differentiated adenocarcinoma
or signet ring cell carcinoma of the stomach often invade the bone
marrow, and 1.4% of surgically resected gastric cancers were
reported to exhibit bone marrow invasion (14). Similar to the present case, patients
with bone marrow metastases from breast or gastric cancer tend to
develop DIC. The main treatments for this disease are considered to
be chemotherapy and intensive supportive therapy. Reliable
molecular markers predictive of bone marrow metastasis have yet to
be identified.
Bone marrow metastasis from CRC is rarely observed,
with only 10 cases of CRC with bone marrow metastasis reported to
date (6). Although 24% of autopsy
cases of CRC were reported to have bone marrow metastases, they may
not be apparent on standard radiological examination and as a
coagulation disorder. In cases with clinically apparent bone marrow
metastases of CRC in association with DIC, chemotherapy was mainly
performed against the tumor, with intensive supportive therapy for
DIC appended. The majority of the reported cases employed
combination chemotherapy with FOLFOX plus molecular-targeted
agents, but survival was generally poor (≤7 months) (6). One of the reasons for unfavorable
survival was suggested to be the poor general condition of the
patients, as DIC hinders the administration of sufficiently
intensive chemotherapy. Another possibility may be primary
resistance of the CRC cells to chemotherapy as a common
characteristic of bone marrow metastasis; however, the molecular
mechanisms underlying the resistance of the CRC cells have not been
elucidated.
A specific explanation as to why bone metastases
often occur in cancers of the breast and stomach, but not in cancer
of the large bowel, has yet to be provided. On histological
examination of the present case, the primary tumor was a poorly
differentiated adenocarcinoma with mucin production, whereas the
metastasized cells in the bone marrow exhibited the characteristics
of moderately to poorly differentiated adenocarcinoma, suggesting
that tumor cells from different lesions displayed similar
histological characteristics. There have been a few reports on
histological and molecular biological analyses of CRC cells
metastasizing to the bone marrow. A unique case of CRC metastasis
to the bone marrow reported by Shah et al involved a poorly
differentiated adenocarcinoma of the ascending colon, with a
CK7-positive, CK20-negative phenotype on immunohistochemical
analysis, wild-type KRAS and positive for a BRAF
V600E mutation (6). CRCs with the
BRAF V600E mutation are known to respond poorly to
chemotherapy and are closely associated with certain
characteristics, including location in the right colon,
hypermutation, a microsatellite-unstable type and mucinous pattern
(15). These characteristics support
the hypothesis that a trait of bone marrow metastasis may be
involved.
Although our case also exhibited mucinous histology
at the primary site, wild-type RAS, BRAF and
PIK3CA genes were detected in the CRC cells. Wild-type
RAS and BRAF are favorable predictive factors of
anti-epidermal growth factor receptor (EGFR) treatment for CRC
(16), whereas CRC harboring
mutations of PIK3CA and wild-type RAS is resistant to
anti-EGFR drugs (17). However, the
association between bone marrow metastasis and tumor type, such as
gene mutations, was unclear.
Cytokeratin is an intermediate filament protein,
mainly detected in differentiated epithelial cells. In the
cytoplasm, intermediate filament proteins play a role in supporting
cell morphology through attachment to desmosomes and
hemidesmosomes. Moreover, it was recently demonstrated that
intermediate filament proteins were able to bind to signaling
proteins and modulate their activity (18). The majority of breast cancers easily
metastasize to the bone marrow and express CK7, but not CK20.
Conversely, CRC cells express CK20, but not CK7, and a
CK7-positive, CK20-negative phenotype reportedly appears in only 2%
of CRCs (19–20). As mentioned above, Shah et al
reported that CK7-expressing CRCs exhibited a bone marrow-invading
phenotype (6); however the present
case exhibited a common CK7-negative, CK20-positive phenotype.
Interestingly, in this case there was also an increased level of
CYFRA. CYFRA is a fragment of CK19 and is often increased in lung
squamous cell carcinoma, ovarian cancer and breast cancer, but not
in colorectal cancer. Pierga et al reported that elevated
levels of CYFRA correlated with detection of micrometastasis of
breast cancer to the bone marrow (21). Although the underlying mechanisms
remain unclear, different CK expressions may affect signaling
pathways in CRC cells leading to bone marrow metastasis.
CDX2 is a major regulator of intestine-specific
genes involved in cell growth and differentiation and plays a role
in early embryonic development of the intestinal tract. A recent
study reported longer relapse-free survival of stage II/III
CDX2-positive CRC (22). The present
case displayed CDX2-positive CRC cells, but whether CDX2 is
associated with survival in stage IV CRC and with bone marrow
metastasis has not been elucidated.
Compared with previous reported cases, the treatment
in our patient exhibited favorable efficacy, possibly because the
patient was relatively young and in a good general condition,
experienced no serious complications associated with organ
metastases, and was able to tolerate a full course of FOLFOX
therapy and intensive supportive therapy for DIC. Although several
CRC patients with bone marrow metastasis were treated with the
anti-EGFR antibody cetuximab (9),
the effects of cetuximab were not clearly demonstrated. In the
subsequent therapy of this patient, panitumumab was beneficial and
the therapy was continued for 8 cycles.
We herein reported a rare case of sigmoid colon
cancer harboring bone marrow metastasis in association with DIC.
The immunohistochemical and molecular biological characteristics of
the CRC differed from those in previously reported cases. Further
research is required to elucidate the mechanisms of bone marrow
metastasis of CRC and to establish efficient biomarkers that are
able to predict a high risk of bone marrow invasion and coagulation
disorder.
Acknowledgements
We would like to thank Dr Shinya Oda (Department of
Cancer Biology, National Hospital Organization Kyushu Cancer
Center) and the medical staff of the National Hospital Organization
Kyushu Cancer Center for their contribution to patient diagnosis
and treatment.
References
|
1
|
Papac RJ: Bone marrow metastases. A
review. Cancer. 74:2403–2413. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hayes DF: Prognostic and predictive
factors revisited. Breast. 14:493–499. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kobayashi M, Okabayashi T, Sano T and
Araki K: Metastatic bone cancer as a recurrence of early gastric
cancer-characteristics and possible mechanisms. World J
Gastroenterol. 11:5587–5591. 2005.PubMed/NCBI
|
|
4
|
Wiedswang G, Borgen E, Kåresen R, Kvalheim
G, Nesland JM, Qvist H, Schlichting E, Sauer T, Janbu J, Harbitz T
and Naume B: Detection of isolated tumor cells in bone marrow is an
independent prognostic factor in breast cancer. J Clin Oncol.
21:3469–3478. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Haggar FA and Boushey RP: Colorectal
cancer epidemiology: Incidence, mortality, survival, and risk
factors. Clin Colon Rectal Surg. 22:191–197. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shah SM, Rosenthal MH, Griffin GK,
Jacobsen ED and McCleary NJ: An aggressive presentation of
colorectal cancer with an atypical lymphoproliferative pattern of
metastatic disease: A case report and review of the literature.
Clin Colorectal Cancer. 13:e5–e11. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee JL, Lee JH, Kim MK, Cho HS, Bae YK,
Cho KH, Bae SH, Ryoo HM, Lee KH and Hyun MS: A case of bone marrow
necrosis with thrombotic thrombocttopenic purpura as a
manifestation of occult colon cancer. Jpn J Clin Oncol. 34:476–480.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pleyer L, Went P, Russ G, Prinz E, Faber
V, Röwert HJ, Karlbauer R and Greil R: Massive infiltration of bone
marrow in colon carcinoma after treatment with activated protein C.
Wiener Klinische Wochenschrift. 119:254–258. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang YC, Chang PY and Yao NS: Bone marrow
necrosis caused by metastatic colon cancer. J Clin Oncol.
27:e482009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Song JY and Dwyre DM: Metastatic
adenocarcinoma involving the bone marrow. Blood. 120:31702012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wada H, Gabazza EC, Asakura H, Koike K,
Okamoto K, Maruyama I, Shiku H and Nobori T: Comparison of
diagnostic criteria For Disseminated Intravascular Coaglation
(DIC): Diagnostic criteria of the International Society of
Thrombosis and Hemostasis (ISTH) and of the Japanese Ministry of
Health and Welfare for Overt DIC. Am J Hematol. 74:17–22. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
National Cancer Institute, . Common
Terminology Criteria for Adverse Events v4.0. NIH Publication:
Number 10-5410. 2010.
|
|
13
|
Braun S, Pantel K, Müller P, Janni W, Hepp
F, Kentenich CR, Gastroph S, Wischnik A, Dimpfl T, Kindermann G, et
al: Cytokeratin-positive cells in the bone marrow and survival of
patients with stage I, II, or III breast cancer. N Engl J Med.
342:525–533. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Iguchi H: Recent aspects for disseminated
carcinomatosis of the bone marrow associated with gastric cancer:
What has been done for the past, and what will be needed in future?
World J Gastroenterol. 21:12249–12260. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pai RK, Jayachandran P, Koong AC, Chang
DT, Kwok S, Ma L, Arber DA, Balise RR, Tubbs RR, Shadrach B and Pai
RK: BRAF-mutated, microsatellite-stable adenocarcinoma of the
proximal colon: An aggressive adenocarcinoma with poor survival,
mucinous differentiation, and adverse morphologic features. Am J
Surg Pathol. 36:744–752. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Therkildsen C, Bergmann TK,
Henrichsen-Schnack T, Ladelund S and Nilbert M: The predictive
value of KRAS, NRAS, BRAF, PIK3CA and PTEN for anti-EGFR treatment
in metastatic colorectal cancer: A systematic review and
meta-analysis. Acta Oncol. 53:852–864. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sartore-Bianchi A, Martini M, Molinari F,
Veronese S, Nichelatti M, Artale S, Di Nicolantonio F, Saletti P,
De Dosso S, Mazzucchelli L, et al: PIK3CA mutations in colorectal
cancer are associated with clinical resistance to EGFR-targeted
monoclonal antibodies. Cancer Res. 69:1851–1857. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Coulombe PA and Wong P: Cytoplasmic
intermediate filaments revealed as dynamic and multipurpose
scaffolds. Nat Cell Biol. 6:699–706. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bayrak R, Yenidünya S and Haltas H:
Cytokeratin 7 and cytokeratin 20 expression in colorectal
adenocarcinomas. Pathol Res Pract. 207:156–160. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Park SY, Kim BH, Kim JH, Lee S and Kang
GH: Panels of immunohistochemical markers help determine primary
sites of metastatic adenocarcinoma. Arch Pathol Lab Med.
131:1561–1567. 2007.PubMed/NCBI
|
|
21
|
Pierga JY, Deneux L, Bonneton C,
Vincent-Salomon A, Nos C, Anract P, Magdelénat H, Pouillart P and
Thiery JP: Prognostic value of cytokeratin 19 fragment (CYFRA 21-1)
and cytokeratin-positive cells in bone marrow samples of breast
cancer patients. Int J Biol Markers. 19:23–31. 2004.PubMed/NCBI
|
|
22
|
Dalerba P, Sahoo D, Paik S, Guo X, Yothers
G, Song N, Wilcox-Fogel N, Forgó E, Rajendran PS, Miranda SP, et
al: CDX2 as a prognostic biomarker in stage II and stage III colon
cancer. N Engl J Med. 374:211–222. 2016. View Article : Google Scholar : PubMed/NCBI
|