Introduction
The most common cause of sciatica is intervertebral
disc herniation; thus, obscure causes are rarely considered in the
differential diagnosis. Malignant peripheral nerve sheath tumor
(MPNST) arising from the sciatic nerve is a relatively rare
malignant soft tissue tumor (1).
This tumor may produce severe radicular pain and sensorimotor
deficits, mimicking a disc herniation. Due to the rare incidence of
this disease, reports on intrapelvic MPNSTs are scarce and there
has been no systemic study of intrapelvic MPNSTs to date (2,3). In this
study, we reported a misdiagnosed case of giant intrapelvic MPNST
of the sciatic nerve mimicking disc herniation. Our aim was raise
awareness that intrapelvic MPNST is an unusual cause of sciatica,
which is usually misdiagnosed as disc herniation. The diagnosis,
treatment and prognosis of MPNSTs were also discussed.
Case report
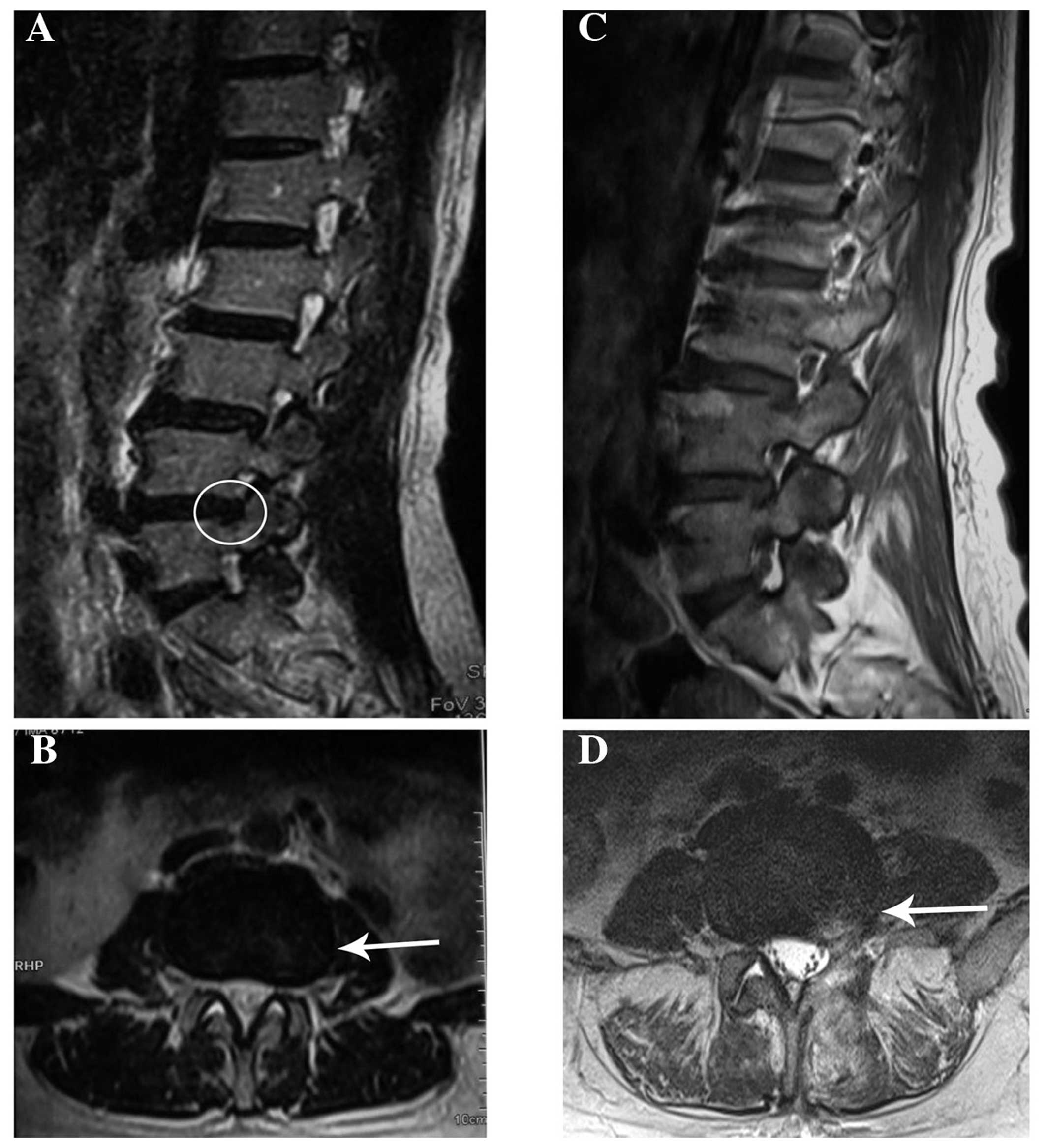
A 46-year old woman was admitted to another hospital
with a 3-month history of pain that radiated from the posterior
aspect of the left thigh to the lateral aspect of the leg and left
foot, and was associated with numbness of the left lower limb. The
patient had undergone a lumbar magnetic resonance imaging (MRI)
examination, which revealed a mild L4/5 intervertebral disk
herniation (Fig. 1A and B). A
clinical diagnosis of intervertebral disk herniation was made, and
L4/5 discectomy was performed (Fig. 1C
and D). However, there was little symptomatic improvement after
2 months. The patient was subsequently referred to our
institution.
On admission, the patient's neurological examination
revealed grade 3/5 weakness of the quadriceps femoris, grade 2/5
weakness of the triceps surae and grade 0/5 weakness of the
extensor hallucis longus and extensor digitorum longus, a decreased
sensation to light touch, decreased patellar reflex and Achilles
reflex on the left, and a positive straight leg raise test. The
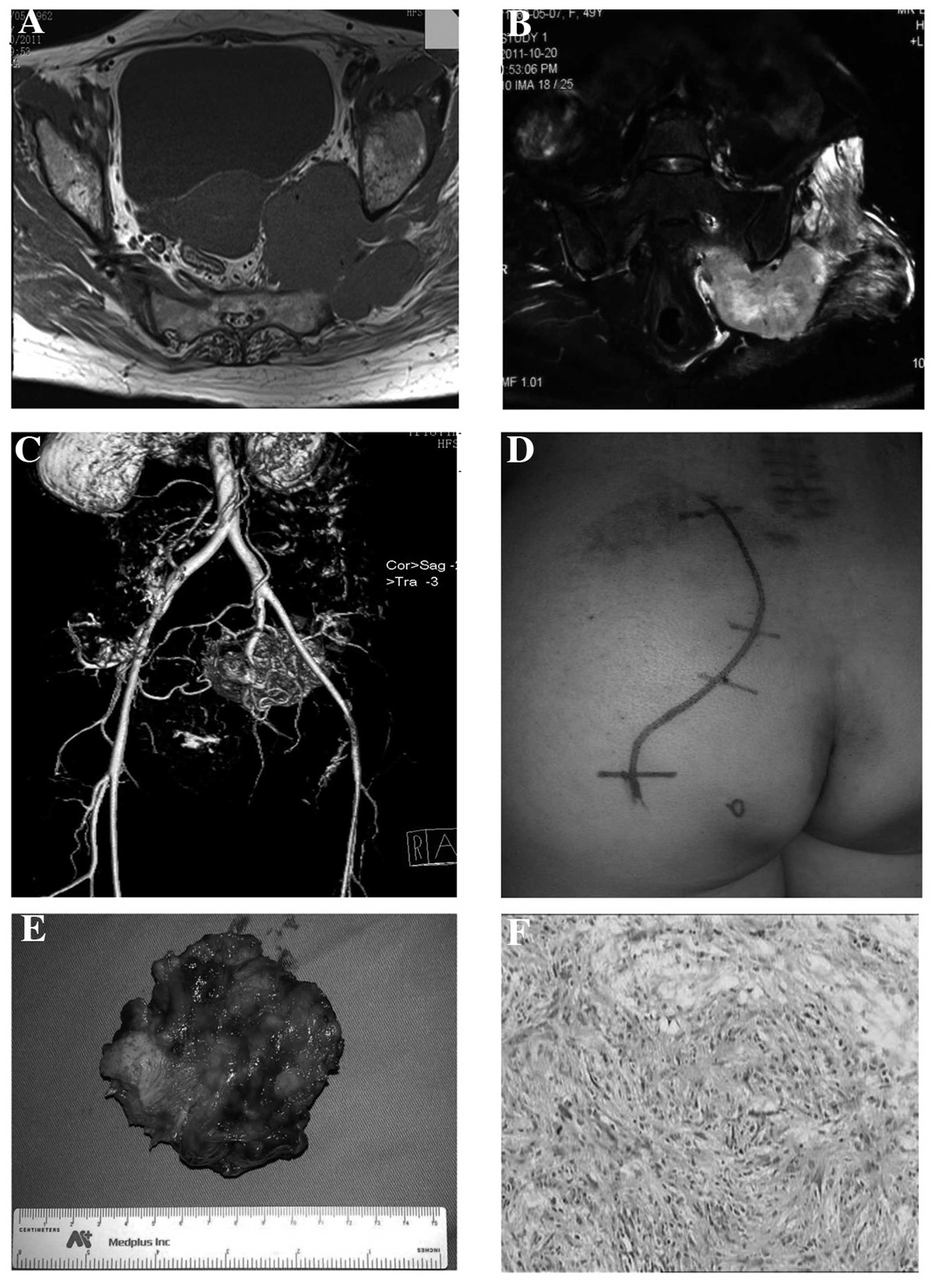
patient underwent further examination by MRI and magnetic resonance
angiogram (MRA). MRI and MRA of the pelvis revealed a mass sized
~7–8 cm within the pelvis involving the internal iliac artery
(Fig. 2A-C). A soft, smooth fixed
mass in the left side of the pelvis was identified.
Gynecological and urological consultations were
obtained. A decision was made to excise the tumor under general
anesthesia. The intrapelvic tumor was exposed through the posterior
approach (Fig. 2D). An incisional
biopsy with intraoperative frozen section examination was performed
from the extrapelvic part of the mass, and the result indicated a
malignant tumor. After being exposed from the greater sciatic
notch, a dumbbell mass was identified surrounding the sciatic
nerve. The tumor tightly enclosed the sciatic nerve and it was
difficult to separate the tumor from the nerve. Wide resection of
the tumor and the invaded part of the sciatic nerve was performed
from the proximal to the distal end (Fig. 2E). The final diagnosis of MPNST was
confirmed by histopathological examination (Fig. 2F). The patient experienced loss of
sensory and motor function below the left knee level after the
operation. She refused further adjunctive radiotherapy and
succumbed to pulmonary metastases 3 years postoperatively. Signed
consent was obtained from the patient's family regarding the
publication of the case details.
Discussion
MPNST is a rare soft tissue sarcoma, often
originating from Schwann cells. While accounting for 3–10% of all
soft tissue sarcomas (4), the
incidence of MPNST in the general population is 0.001% (5). The most important risk factor for MPNST
development is the presence of neurofibromatosis type 1 (NF1), and
30% of MPNST cases occur in patients with a history of NF1
(6). In addition, MPNST may also
develop as a result of therapeutic irradiation in populations that
have previously undergone radiotherapy for malignant disease
(7).
MPNSTs may occur anywhere along the peripheral
nerves in the deep tissues. The significance of intrapelvic MPNST
lies with its diagnostic difficulties in clinical practice. Pelvic
tumors grow slowly and cannot be palpated along the nerve course.
They are generally difficult to diagnose until they give rise to
symptoms. The most common clinical presentation of intrapelvic
MPNST consists of radicular and distal pain, paraesthesia and motor
deficiencies.
Since the symptoms are similar to sciatica due to a
herniated disk, while imaging of the spine may reveal discopathy,
intrapelvic MPNST of the sciatic nerve is easily misdiagnosed
(8,9). A misinterpretation of the findings may
result in incorrect treatment by discectomy, as reported in our
patient. However, when there is no improvement of the symptoms
following discectomy, the original diagnosis must be questioned
(10). Ultrasonography, pelvic CT
scan or MRI may be used to demonstrate the tumor along with the
nerve. MRI is the most useful diagnostic tool, which allows
assessment of the tumor's associations with adjacent structures.
Information on the enhancing quality of the tumor, combined with
its appearance on T1- and T2-weighted images, may offer some
benefit in terms of differentiating benign peripheral nerve sheath
tumors (BPNSTs) from MPNSTs. In the majority of the cases, central
low signal intensity with a peripheral ring of high signal
intensity on T2-weighted images are characteristic signs of a
benign lesion (11), whereas a
heterogeneous lesion due to necrosis and hemorrhage and patchy
contrast enhancement may suggest malignancy (12). Although MRI may offer useful
preoperative information, definitive diagnosis relies on pathology.
Open biopsy is more accurate compared with percutaneous biopsy. To
reduce the risk of contamination, the biopsy technique should be
carefully considered, including proper location of the biopsy
incision and meticulous hemostasis. The S-100 protein and Ki-67
index are widely used as immunohistochemical markers for MPNST.
Once the diagnosis of intrapelvic MPNST is
suspected, surgical excision is the mainstay of treatment. The aim
of surgery is complete removal of the lesion with tumor-free
margins. When pelvic tumors extend outside the pelvis through the
sciatic notch, a combined surgical approach, such as transabdominal
plus gluteal approach, should be considered. The majority of benign
pelvic tumors may be bluntly dissected after incising the
epineurium over the mass. Unfortunately, for MPNSTs that involve
the sciatic nerve or pelvic plexus, it is difficult to achieve
complete removal of the mass with tumor-free margins without
damaging the adjacent nerves. Wide local resection for MPNST
including the sciatic nerve or pelvic plexus is required (13), as reported in our patient.
Multimodality treatments, such as adjunctive radiotherapy and
chemotherapy, have been associated with improved survival outcomes
compared with previous reports (14,15).
However, only complete surgical excision prior to metastasis is
likely to result in a good prognosis.
Patients with MPNST have a poor prognosis. Adverse
prognostic factors include large size, high-grade tumor, proximal
location, surgical margin with tumor invasion and NF1 (16,17). The
5-year survival rates are associated with NF1. The reported 5-year
survival rate for patients without NF1 may be as high as 50%,
whereas they may as low as 10% in patients with NF1 (18). Systemic spread occurs most commonly
to the lungs, and pulmonary metastasis is the ultimate cause of
death in cases of MPNST.
In summary, we herein report a rare case of giant
intrapelvic MPNST misdiagnosed as intervertebral disc herniation.
Our goal was to emphasize that intrapelvic MPNST, although
infrequent, should be included in the differential diagnosis of
sciatica, as its symptomatology may mimic disc herniation.
Clinicians should consider the possibility of pelvic MPNST when
patients present with obscure sciatica. The standard treatment of
MPNST diagnosed early includes open biopsy, surgical treatment and
a multidisciplinary approach to improve patient prognosis.
References
|
1
|
Topsakal C, Akdemir I, Tiftikci M, Ozercan
I and Aydin Y: Malignant schwannoma of the sciatic nerve
originating in a spinal plexiform neurofibroma associated with
neurofibromatosis type 1-case report. Neurol Med Chir (Tokyo).
41:551–555. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kelso TB, Ferrari CJ and Frassica FJ:
Sciatica caused by a neurilemoma of the intrapelvic portion of the
sciatic nerve. A case report. J Bone Joint Surg Am. 75:603–605.
1993.PubMed/NCBI
|
|
3
|
Naraghi MA: Neurofibroma of the sciatic
nerve with neurofibromatosis type 1. Acta Med Iran. 49:480–482.
2011.PubMed/NCBI
|
|
4
|
Zhu B, Liu X, Yang S, Liao H, Jiang L and
Wei F: Malignant peripheral nerve sheath tumours of the spine:
Clinical manifestations, classification, treatment, and prognostic
factors. Eur Spine J. 21:897–904. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wanebo JE, Malik JM, VandenBerg SR, Wanebo
HJ, Driesen N and Persing JA: Malignant peripheral nerve sheath
tumors. A clinicopathologic study of 28 cases. Cancer.
71:1247–1253. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Scheithauer BW, Erdogan S, Rodriguez FJ,
Burger PC, Woodruff JM, Kros JM, Gokden M and Spinner RJ: Malignant
peripheral nerve sheath tumors of cranial nerves and intracranial
contents: A clinicopathologic study of 17 cases. Am J Surg Pathol.
33:325–338. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Amin A, Saifuddin A, Flanagan A, Patterson
D and Lehovsky J: Radiotherapy-induced malignant peripheral nerve
sheath tumor of the cauda equine. Spine (Phila Pa 1976).
29:E506–E509. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kralick F and Koenigsberg R: Sciatica in a
patient with unusual peripheral nerve sheath tumors. Surg Neurol.
66:634–637. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rekha A and Ravi A: Sciatic nerve
schwannoma. Int J Low Extrem Wounds. 3:165–167. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Richards JL and Matolo NM: Malignant
schwannoma: Report of a case mimicking lumbar disk disease. Am
Surg. 45:49–51. 1979.PubMed/NCBI
|
|
11
|
White W, Shiu MH, Rosenblum MK, Erlandson
RA and Woodruff JM: Cellular schwannoma. A clinicopathologic study
of 57 patients and 58 tumors. Cancer. 66:1266–1275. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kar M, Deo SV, Shukla NK, Malik A,
DattaGupta S, Mohanti BK and Thulkar S: Malignant peripheral nerve
sheath tumors (MPNST)-clinicopathological study and treatment
outcome of twenty-four cases. World J Surg Oncol. 4:552006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nawabi DH and Sinisi M: Schwannoma of the
posterior tibial nerve: The problem of delay in diagnosis. J Bone
Joint Surg Br. 89:814–816. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Baehring JM, Betensky RA and Batchelor TT:
Malignant peripheral nerve sheath tumor: The clinical spectrum and
outcome of treatment. Neurology. 61:696–698. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Stucky CC, Johnson KN, Gray RJ, Pockaj BA,
Ocal IT, Rose PS and Wasif N: Malignant peripheral nerve sheath
tumors (MPNST): The Mayo Clinic experience. Ann Surg Oncol.
19:878–885. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Angelov L, Davis A, O'Sullivan B, Bell R
and Guha A: Neurogenic sarcomas: Experience at the University of
Toronto. Neurosurgery. 43:56–65. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Anghileri M, Miceli R, Fiore M, Mariani L,
Ferrari A, Mussi C, Lozza L, Collini P, Olmi P, Casali PG, et al:
Malignant peripheral nerve sheath tumors: Prognostic factors and
survival in a series of patients treated at a single institution.
Cancer. 107:1065–1074. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Doorn PF, Molenaar WM, Buter J and
Hoekstra HJ: Malignant peripheral nerve sheath tumors in patients
with and without neurofibromatosis. Eur J Surg Oncol. 21:78–82.
1995. View Article : Google Scholar : PubMed/NCBI
|