Introduction
Lung cancer is the leading cause of
malignancy-related deaths worldwide, and non-small-cell lung cancer
(NSCLC) accounts for ~80% of all types of lung cancer (1). Approximately two-thirds of NSCLC cases
present as locally advanced or metastatic disease, and systemic
chemotherapy, including molecular-targeted therapy, plays a key
role in the treatment of such patients. However, the prognosis of
such cases remains poor; thus, there is a pressing need for more
effective, tolerable and individualized treatments to improve
clinical outcome.
In the 2000s, anticancer agents were administered to
patients with advanced or metastatic NSCLC, regardless of their
specific biological characteristics, in an ‘unselected’ manner. At
that time, platinum-based chemotherapies, including carboplatin and
paclitaxel, were widely recognized as standard treatments for
advanced or metastatic NSCLC. In previous randomized phase III
studies, the response rates to a combination of carboplatin and
paclitaxel ranged from 17 to 32.4%, with median survival times
(MST) of 8.1–12.3 months (2,3).
In 2002, the first molecular-targeted agent,
gefitinib, was approved for advanced or metastatic NSCLC in Japan,
prior to its approval in other countries. However, predictive
biomarkers, such as mutations in the gene encoding epidermal growth
factor receptor (EGFR) had not been identified, and the response
rates among unselected patients ranged from 12 to 18%, with MSTs of
7.0–7.6 months, in earlier phase II studies (IDEAL 1 and 2)
(4,5). However, the discovery of EGFR
mutations as predictive biomarkers of an antitumor response to
gefitinib greatly elucidated the indication for gefitinib treatment
in patients with advanced or metastatic NSCLC (6,7). The
response rates to gefitinib among EGFR-mutant patients were
~70% (8,9) and gefitinib, as well as erlotinib and
afatinib, are currently established as standard first-line
treatment for patients with advanced or metastatic NSCLC harboring
EGFR mutations.
Although the combination of carboplatin and
paclitaxel, as well as gefitinib, were considered to be effective
for the treatment of advanced or metastatic NSCLC, the optimal
order of these two treatments had not been determined by 2002.
Accordingly, from 2003 to 2005, we conducted a randomized phase II
study to compare a combination of carboplatin and paclitaxel
followed by gefitinib monotherapy, with gefitinib monotherapy
followed by a combination of carboplatin and paclitaxel in
chemotherapy-naïve patients with advanced or metastatic NSCLC. The
objective of this study was to select a candidate arm for further
investigation. After obtaining long-term follow-up data, we herein
report the final analysis of this study.
Patients and methods
Patient selection
Patients with histologically and/or cytologically
confirmed NSCLC were eligible for this study. The eligibility
criteria were as follows: Clinical stage IV or IIIB (including only
patients without indications for curative radiotherapy, such as
malignant pleural effusion or dissemination, malignant pericardiac
effusion, or metastatic lesion in the same lobe as the primary
lesion) based on the fifth Union for International Cancer Control
TNM classification (http://www.uicc.org/resources/tnm); no prior systemic
chemotherapy; no prior surgery and/or radiotherapy at the primary
site; age 20–74 years; Eastern Cooperative Oncology Group
performance status (ECOG-PS) of 0 or 1; at least 1 measurable
lesion ≥1 cm; and adequate organ function (white blood cell count
≥4,000/mm3, neutrophil count ≥2,000/mm3,
hemoglobin level ≥9.5 g/dl, platelet count ≥100,000/mm3,
serum creatinine level ≤1.5 mg/dl, aspartate aminotransferase level
≤2 times the upper limit of normal, alanine aminotransferase level
≤2 times the upper limit of normal, total bilirubin level ≤1.5
mg/dl and partial arterial oxygen pressure ≥60 Torr). The exclusion
criteria were as follows: Serious concomitant illness (severe heart
disease, uncontrolled diabetes mellitus, uncontrolled hypertension,
or active infection); obvious interstitial pneumonia or pulmonary
fibrosis on chest X-ray; pericardial or pleural effusion requiring
drainage; synchronous active malignancy; severe drug allergy; and
pregnancy or breastfeeding. Patients with brain metastases were
eligible for enrollment if they were asymptomatic and did not
require steroid or anticonvulsant therapy.
Written informed consent was obtained from all the
participating patients and the study protocol was approved by the
Institutional Review Board of the National Cancer Center (Tokyo,
Japan).
Study design
The aim of this randomized phase II study aimed to
select a candidate arm for further development in a phase III study
by investigating the optimal order of cytotoxic chemotherapy
(carboplatin and paclitaxel) and molecular-targeted therapy
(gefitinib) administration in chemotherapy-naïve patients with
advanced or metastatic NSCLC. The primary endpoint was overall
survival, and the secondary endpoints were response rate and
prevalence of adverse events. The patients were randomly assigned
in a 1:1 manner to either arm A (carboplatin and paclitaxel
followed by gefitinib) or arm B (gefitinib followed by carboplatin
plus paclitaxel) (Fig. 1). Random
assignment was stratified according to gender (female vs. male) and
histology (adenocarcinoma vs. others).
Treatment
The treatment plan for arm A included 4 cycles of
carboplatin and paclitaxel at 3-week intervals, followed by
gefitinib monotherapy. Gefitinib monotherapy was administered from
day 22 to day 50, or after the fourth cycle of carboplatin and
paclitaxel, even if the patients had stable disease. If patients in
arm A experienced disease progression or unacceptable toxicities
before the 4 cycles of treatment were completed, gefitinib
monotherapy was subsequently initiated within the 4-week drug
holiday. Gefitinib monotherapy was continued until development of
disease progression or unacceptable toxicity. Arm B patients
received gefitinib monotherapy, which continued until disease
progression or development of unacceptable toxicity, followed by 4
cycles of carboplatin and paclitaxel at 3-week intervals.
In both arms, paclitaxel was administered
intravenously on day 1 at a dose of 200 mg/m2 over a 3-h
period, followed by carboplatin at a dose calculated to produce an
area under the concentration-time curve of 6.0 mg/min/ml. Gefitinib
was orally administered at a once-daily dose of 250 mg. Subsequent
treatments were not restricted in either arm of this study.
Study evaluations
The pretreatment evaluation included a complete
medical history, physical examination, complete and differential
blood cell counts, routine chemistry measurement, urinalysis, chest
radiography, chest computed tomography (CT) scan, brain CT or
magnetic resonance imaging, abdominal ultrasonography and/or CT,
and electrocardiogram. Complete and differential blood cell counts
and routine chemistry measurements were performed at least weekly
during the first carboplatin and paclitaxel cycle, or within 4
weeks after the initiation of gefitinib monotherapy. A chest
radiograph was obtained weekly during the first carboplatin and
paclitaxel cycle or gefitinib monotherapy to evaluate potential
pulmonary toxicity, and as needed thereafter.
The overall survival duration was assessed from the
date of registration to the date of death from any cause. If death
did not occur, data were censored based on the last date the
patient was known to be alive.
The objective tumor response was evaluated in all
eligible patients according to the Response Evaluation Criteria in
Solid Tumors (10). Toxicities were
graded according to the National Cancer Institute Common Toxicity
Criteria (NCI-CTC), version 2.0 (http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm).
Evaluation of EGFR mutation
status
The EGFR mutation status was analyzed in 41
patients with available tumor samples. DNA was extracted from
archived Papanicolaou-stained cytological slides and/or
formalin-fixed, paraffin-embedded (FFPE) tissues using the QIAamp
DNA Micro kit (Qiagen, Venlo, The Netherlands). The two major
hotspots for EGFR mutations, an in-frame deletion including
amino acids at codons 747–749 (DEL) in exon 19 and a missense
mutation at codon 858 (L858R) in exon 21, were analyzed via
high-resolution melting analysis, as previously described (11,12).
Polymerase chain reaction was performed using primers designed to
amplify a region containing E746-I759 or L858 of EGFR and LC
Green Idye (Roche Diagnostics, Indianapolis, IN, USA). Melting
curves were obtained using HR-1 (Idaho Technology, Salt Lake City,
UT, USA) and the curves produced for samples and controls were
compared.
Statistical analysis
As overall survival was the primary endpoint of this
study, the required sample size was calculated according to the
selection designs of survival-based pilot studies (13). The required total sample size was
determined to be 87 with the following assumptions: i) The survival
curve was exponential; ii) the MST of the worse arm was 9 months
and that of the better arm was 9 months ×1.4; iii) the correct
selection probability was 90%; and iv) the additional follow-up (in
years) after the end of accrual was 1 year. After assuming a 10%
non-evaluable rate, a total of 96 patients and an accrual period of
3 years were required to evaluate this study. The survival
distribution was estimated using the Kaplan-Meier method.
A two-sided P-value of ≤0.05 was considered to
indicate statistically significant differences. All statistical
analyses were performed using JMP software, version 11.2 (SAS
Institute, Inc., Cary, NC, USA).
Results
Patient characteristics
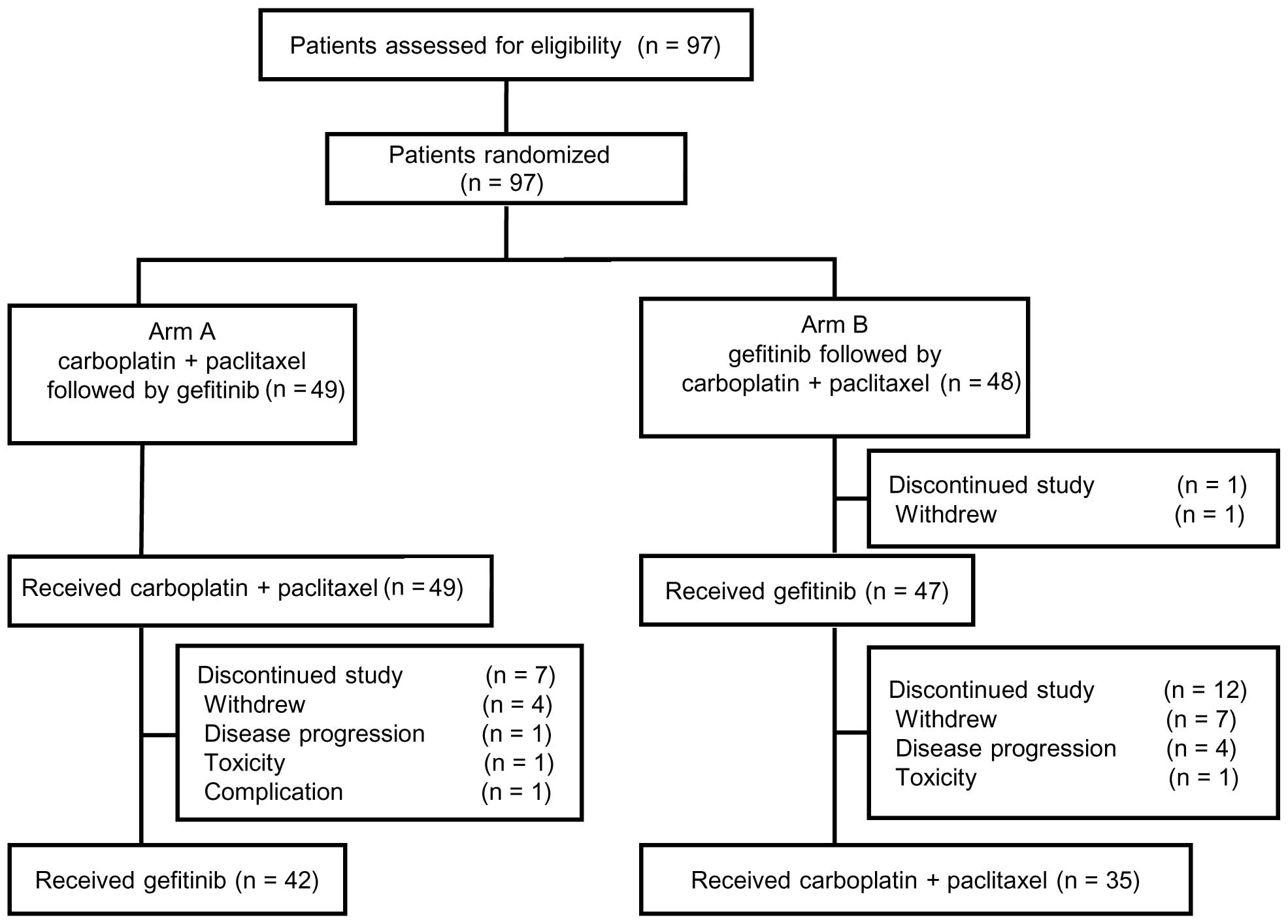
A total of 97 patients were enrolled between June,
2003 and October, 2005, of whom 49 were randomly assigned to arm A
(carboplatin and paclitaxel followed by gefitinib) and 48 to arm B
(gefitinib followed by carboplatin and paclitaxel). The CONSORT
diagram of this study is shown in Fig.
1. The patient characteristics were well balanced between the
two treatment arms, with median ages of 63 (range, 32–74) and 61
(range, 45–73) years, male/female ratios of 28/21 and 28/20,
ECOG-PS 0/1 ratios of 23/26 and 24/24, and stage IIIB/IV ratios of
11/38 and 11/37 in arms A and B, respectively (Table I). A total of 85 (88%) patients were
diagnosed with adenocarcinoma. One patient in arm B withdrew
consent and, therefore, did not receive the study treatment
(gefitinib). The remaining 96 patients were evaluable for toxicity
and antitumor response following first-line treatment (i.e.,
carboplatin and paclitaxel in arm A, gefitinib in arm B) and
overall survival.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristics | Arm A (n=49) No.
(%) | Arm B (n=48) No.
(%) |
|---|
| Age, years |
|
|
| Median
(range) | 63 (32–74) | 61 (45–73) |
| Gender |
|
|
| Male | 28 (57.1) | 28 (58.3) |
|
Female | 21 (42.9) | 20 (41.7) |
| ECOG PS |
|
|
| 0 | 23 (46.9) | 24 (50.0) |
| 1 | 26 (53.1) | 24 (50.0) |
| Histology |
|
|
|
Adenocarcinoma | 43 (87.8) | 42 (87.5) |
| Squamous
cell | 2 (4.1) | 1 (2.1) |
| NSCLCa | 4 (8.2) | 5 (10.4) |
| Stage |
|
|
| IIIB | 11 (22.4) | 11 (22.9) |
| IV | 38 (77.6) | 37 (77.1) |
| Smoking status |
|
|
| Current
and/or past | 27 (55.1) | 28 (58.3) |
|
Never | 22 (44.9) | 20 (41.7) |
| Previous
treatment |
|
|
| No | 38 (77.6) | 39 (81.3) |
| Yes | 11 (22.4) | 9 (18.8) |
|
Radiotherapy for
bone | 2 | 4 |
|
Radiotherapy for
brain | 3 | 2 |
|
Surgery for
brain | 0 | 1 |
|
Drainage | 6 | 4 |
Administered treatment
In arm A, 49 patients received carboplatin and
paclitaxel, with a median number of 4 (range, 1–5) treatment
cycles, and 42 transitioned to gefitinib monotherapy (Fig. 1). The main reasons for transitioning
to gefitinib monotherapy were progressive disease (PD; n=34) and
toxicity (n=8). A total of 7 patients did not receive gefitinib
monotherapy due to the following reasons: Consent withdrawal,
(n=4); disease progression (n=1); pneumonitis after palliative
radiotherapy (n=1); and prolonged toxicity from carboplatin and
paclitaxel (n=1). The median duration of gefitinib monotherapy was
73 days (range, 46–154 days).
In arm B, 47 of 48 patients received gefitinib
monotherapy, and 35 of 47 patients transitioned to carboplatin and
paclitaxel, with a median of 4 (range, 1–4) treatment cycles. The
median gefitinib monotherapy duration was 87 days (range, 34–137
days). The main reasons for transitioning to carboplatin and
paclitaxel were PD (n=32) and toxicity (n=3). Of the 47 patients,
12 did not transition to carboplatin and paclitaxel treatment due
to the following reasons: Consent withdrawal (n=7); PD (n=4); and
toxicity (n=1).
Efficacy
The response rates to carboplatin and paclitaxel
were 34.8% [95% confidence interval (CI): 21.0–48.5] and 26.5% (95%
CI: 11.6–41.3) in arms A and B, respectively (Table II). The response rate to gefitinib
was 35.7% (95% CI: 18.0–53.5) and 33.3% (95% CI: 19.6–47.1) in arm
A and B, respectively. The rate did not differ significantly
between the treatment arms.
| Table II.Response to treatment. |
Table II.
Response to treatment.
| A, Response to first
treatment |
|---|
|
|---|
|
| Arm A (n=49) | Arm B (n=48) |
|---|
|
|
|
|
|---|
| Type of response | Carboplatin+PTX | Gefitinib |
|---|
| Assessable cases,
n | 49 | 47 |
| CR | 0 | 0 |
| PR | 16 | 15 |
| SD | 20 | 11 |
| PD | 10 | 19 |
| NE | 3 | 2 |
| RR, % (95% CI) | 34.8 (21.0–48.5) | 33.3 (19.6–47.1) |
|
| B, Response to second
treatment |
|
| Type of
response | Gefitinib |
Carboplatin+PTX |
|
| Assessable cases,
n | 29 | 35 |
| CR | 0 | 1 |
| PR | 10 | 8 |
| SD | 5 | 17 |
| PD | 13 | 8 |
| NE | 1 | 1 |
| RR, % (95% CI) | 35.7
(18.0–53.5) | 26.5
(11.6–41.3) |
The median overall follow-up duration was 65.1
months (range, 28.7–75.1 months). The median progression-free
survival durations with gefitinib monotherapy were 2.4 (95% CI:
1.5–5.1) and 2.9 (95% CI: 1.1–4.6) months in arms A and B,
respectively; the difference was not statistically significant.
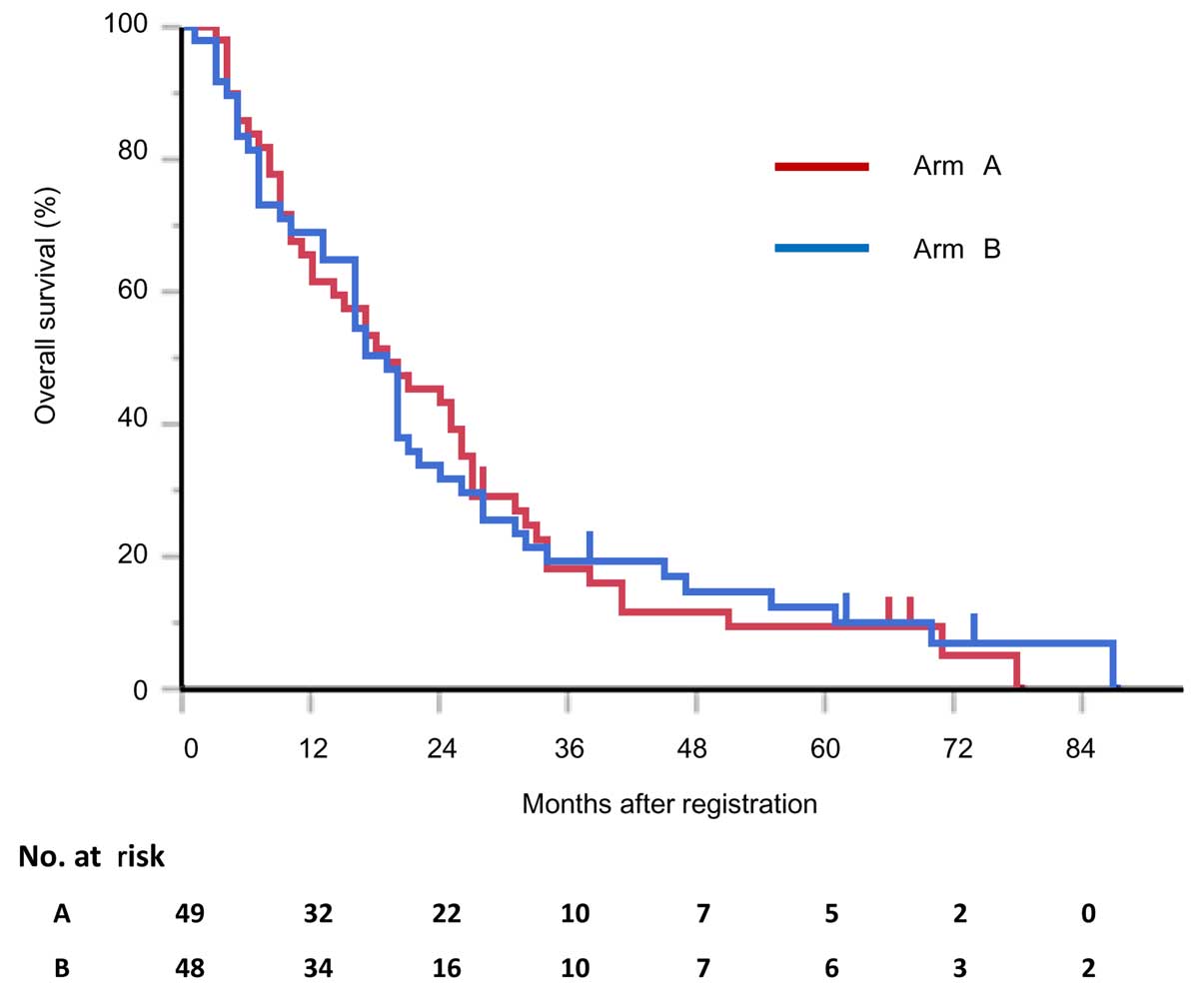
At the time of the most recent update (February 17,
2015), 91 of the 97 patients had succumbed to the disease, and 6
had been lost to follow-up. The MSTs were 19.1 (95% CI: 11.7–26.0)
and 18.2 (95% CI: 13.5–21.6) months in arms A and B, respectively
(P=0.971; Fig. 2). The respective 1-
and 2-year survival rates were 61.2% (95% CI: 47.0–73.7) and 42.8%
(95% CI: 29.9–56.9) in arm A, and 68.7% (95% CI: 54.4–80.1) and
31.3% (95% CI: 19.8–45.6) in arm B (Fig.
2). The treatment arms did not significantly differ with
respect to the MSTs or 1- and 2-year survival rates.
Toxicity
The toxicity profiles of the two treatment arms are
shown in Table III. In both arms,
the major toxicities associated with carboplatin and paclitaxel
were neutropenia, leukopenia, peripheral neuropathy, arthralgia and
nausea, whereas diarrhea, rash, and hepatic dysfunction were
associated with gefitinib. The frequency and severity of these
toxicities did not differ significantly between the treatment
arms.
| Table III.Toxicity profiles. |
Table III.
Toxicity profiles.
| A, Carboplatin +
paclitaxel |
|---|
|
|---|
|
| Arm A (n=49) | Arm B (n=35) |
|---|
|
|
|
|
|---|
|
| Grade, n (%) | Grade, n (%) |
|---|
|
|
|
|
|---|
| Toxicity | 1–2 | 3 | 4 | 1–2 | 3 | 4 |
|---|
| Leukopenia | 28 (57) | 14 (29) | 1 (2) | 16 (44) | 14 (40) | 0 (0) |
| Neutropenia | 8 (17) | 17 (35) | 19 (39) | 5 (11) | 10 (29) | 15 (43) |
|
Thrombocytopenia | 24 (49) | 6 (12) | 0 (0) | 16 (45) | 8 (22) | 0 (0) |
| Anemia | 40 (82) | 5 (10) | 1 (2) | 23 (63) | 9 (26) | 2 (6) |
| AST increased | 25 (51) | 1 (2) | 0 (0) | 18 (51) | 1 (3) | 0 (0) |
| ALT increased | 26 (53) | 2 (5) | 0 (0) | 18 (51) | 5 (14) | 0 (0) |
| Bilirubin
increased | 16 (33) | 0 (0) | 0 (0) | 12 (34) | 0 (0) | 0 (0) |
|
Nausea/vomiting | 23 (46) | 2 (5) | 0 (0) | 22 (62) | 0 (0) | 0 (0) |
|
Arthralgia/myalgia | 38 (77) | 1 (2) | 0 (0) | 25 (71) | 0 (0) | 0 (0) |
| Neuropathy | 33 (67) | 2 (4) | 0 (0) | 18 (51) | 3 (9) | 0 (0) |
| Infection | 6 (12) | 0 (0) | 0 (0) | 7 (20) | 0 (0) | 0 (0) |
| Febrile
neutropenia | 0 (0) | 7 (14) | 0 (0) | 0 (0) | 2 (5) | 0 (0) |
| Interstitial lung
disease | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (2) | 0 (0) |
|
| B, Gefitinib |
|
|
| Arm A (n=42) | Arm B (n=47) |
|
|
|
|
|
| Grade, n (%) | Grade, n (%) |
|
|
|
|
| Toxicity | 1–2 | 3 | 4 | 1–2 | 3 | 4 |
|
| AST increased | 12 (28) | 4 (9) | 0 (0) | 22 (46) | 4 (8) | 0 (0) |
| ALT increased | 18 (42) | 3 (7) | 0 (0) | 21 (44) | 9 (19) | 0 (0) |
| Bilirubin
increased | 3 (7) | 0 (0) | 0 (0) | 6 (12) | 0 (0) | 0 (0) |
|
Nausea/vomiting | 6 (14) | 0 (0) | 0 (0) | 4 (8) | 1 (2) | 0 (0) |
| Rash | 30 (71) | 0 (0) | 0 (0) | 36 (76) | 1 (2) | 0 (0) |
| Dry skin | 6 (14) | 0 (0) | 0 (0) | 4 (8) | 0 (0) | 0 (0) |
| Diarrhea | 20 (47) | 0 (0) | 0 (0) | 22 (55) | 0 (0) | 0 (0) |
| Stomatitis | 4 (9) | 0 (0) | 0 (0) | 9 (19) | 0 (0) | 0 (0) |
| Infection | 4 (9) | 0 (0) | 0 (0) | 1 (2) | 0 (0) | 0 (0) |
| Interstitial lung
disease | 0 (0) | 1 (2) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Two patients experienced interstitial lung disease
(ILD) in this study. One patient developed ILD on day 51 of
gefitinib monotherapy in arm A, and this case was considered to be
strongly associated with gefitinib. The other patient developed
possible treatment-related ILD after the second cycle of
carboplatin and paclitaxel in arm B. Both patients required steroid
therapy to recover from ILD. The patient from arm B succumbed to
perforative peritonitis on day 36 after initiating gefitinib
monotherapy, although this event was not considered to be
treatment-related, but rather due to tumor progression.
Exploratory analysis
FFPE samples suitable for mutation analysis were
available from 41 of the 96 patients in this study (21 in arm A and
20 in arm B). EGFR mutations were detected in 13 (61.9%)
patients in arm A (9 in DEL and 4 in L858R), and 7 (35%) in arm B
(4 in DEL and 3 in L858R). Seven of the 13 (53.8%) and 6 of the 7
(85.7%) patients with EGFR mutations in arms A and B,
respectively, achieved a partial response to gefitinib monotherapy.
In both arms, the survival of patients harboring EGFR
mutations tended to be longer compared with that of patients
without EGFR mutations, although these differences were not
statistically significant (data not shown).
Discussion
The aim of this randomized phase II study was to
determine the optimal order of cytotoxic chemotherapy (i.e.,
carboplatin and paclitaxel) and gefitinib administration for the
treatment of NSCLC, regardless of the EGFR mutation status,
for use in a subsequent phase III study comparing chemotherapy with
the better regimen of this phase II study. In this study, overall
survival did not differ significantly between the two treatment
arms. The response rate to carboplatin and paclitaxel in both
treatment arms (i.e., arm A + arm B) was 31.2% (95% CI: 21.1–41.4),
and the response rate to gefitinib was 34.2% (95% CI: 23.4–45.1).
The major toxicities associated with carboplatin and paclitaxel
were neutropenia and leukopenia, and their incidences were almost
equal between the two treatment arms. The major toxicities
associated with gefitinib were rash and liver dysfunction, which
also occurred at nearly equal rates in the two treatment arms. We
decided upon arm A (carboplatin and paclitaxel followed by
gefitinib) as a candidate arm for a subsequent phase III study, as
carboplatin and paclitaxel was an established first-line treatment
for advanced NSCLC at the time of study planning.
Immediately after completing patient enrollment in
our study, a large-scale Asian randomized phase III study of
treatment for advanced NSCLC (IPASS) was launched (14). The patients in that study were
selected using more strict clinical criteria (i.e., Asian
population, adenocarcinoma only, and light or never-smokers).
During patient enrollment for our randomized phase II study, we
remained aware of the favorable clinical characteristics of
patients who may benefit from gefitinib, specifically female
patients with adenocarcinoma who were light or never-smokers. In
our study, the proportions of patients with adenocarcinoma and
never-smokers were higher compared with those in previous
randomized phase III studies (2,3). The
IPASS study was conducted in a global setting, and our institute
had joined this study; thus, we did not conduct our previously
planned phase III study. From a different viewpoint, our randomized
phase II study may be considered as a beginning stage of the IPASS
study. In the IPASS study, the overall survival rates between the
two treatment arms (carboplatin and paclitaxel followed by
gefitinib vs. gefitinib followed by carboplatin and paclitaxel) did
not differ significantly. However, progression-free survival was
significantly better in the experimental arm (gefitinib followed by
carboplatin and paclitaxel). By contrast, our study was not
designed to assess progression-free survival between the two
treatment arms, as subsequent gefitinib monotherapy was initiated
in arm A following the completion of 4 cycles of carboplatin and
paclitaxel, without confirmation of disease progression.
An activating somatic EGFR mutation was
discovered in 2004 (6,7). After this landmark discovery, treatment
strategies changed dramatically from phenotype- to genotype-based.
Currently, the EGFR mutation status is initially determined
from biopsy samples and used to determine the use of EGFR-TKIs.
Accordingly, several randomized phase III studies have been
conducted to investigate the most favorable order of cytotoxic
chemotherapy and EGFR-TKI administration. The NEJ002 study compared
carboplatin and paclitaxel followed by gefitinib with gefitinib
followed by carboplatin and paclitaxel in patients with
EGFR-mutant NSCLC, but failed to observe a significant
difference in overall survival (9).
Similarly, the WTJOG3405 study compared cisplatin and docetaxel
followed by gefitinib with gefitinib followed by cisplatin and
docetaxel in patients with EGFR-mutant NSCLC, and did not
observe significantly different survival outcomes (8). Other global phase III studies (e.g.,
OPTIMAL and EURTAC) also compared cytotoxic chemotherapy and
EGFR-TKI as first-line treatments for EGFR-mutant NSCLC
(15,16). Although overall survival did not
differ between cytotoxic chemotherapy and EGFR-TKI in those
studies, progression-free survival was significantly better in the
EGFR-TKI arms of all studies (NEJ002, WTJOG3405, OPTIMAL and
EURTAC). These reproducible and favorable outcomes indicate a
progression-free survival advantage and higher response rate
associated with EGFR-TKIs, contributing to the recommendation of
these agents as first-line treatment for patients with
EGFR-mutant NSCLC.
When we planned this randomized phase II study in
2002, favorable clinical pretreatment factors (i.e., female gender,
adenocarcinoma and light or never-smokers) or the EGFR
mutation status had not been clearly established with regard to
patient selection for clinical studies incorporating EGFR-TKIs.
Although the survival outcome in our study appears to be similar to
that of the subsequent large-scale IPASS phase III study, we are
unable to apply the results of our study into the current routine
clinical practice. However, our results may also be considered an
initial step toward a subsequent large-scale phase III study.
Currently, the individualization of EGFR-TKI
treatment is becoming more precise. For example, the
second-generation EGFR-TKI afatinib conferred a survival advantage
over cytotoxic chemotherapy to patients with EGFR exon 19
deletion in an integrated survival analysis of Lux-Lung-3 and −6
(17). Moreover, global studies are
investigating the ability of third-generation EGFR-TKIs to overcome
the resistant EGFR-T790M mutation, and the approval of these agents
is expected (18–20). In the near future, additional
individualized treatments may be established for the treatment of
EGFR-mutant NSCLC.
In conclusion, overall survival did not
significantly differ between the two arms of our study in patients
with advanced NSCLC, regardless of their EGFR mutation
status; accordingly, we selected carboplatin and paclitaxel
followed by gefitinib for a subsequent phase III study. Our study
results may represent an important step toward a subsequent phase
III study.
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ohe Y, Ohashi Y, Kubota K, Tamura T,
Nakagawa K, Negoro S, Nishiwaki Y, Saijo N, Ariyoshi Y and Fukuoka
M: Randomized phase III study of cisplatin plus irinotecan versus
carboplatin plus paclitaxel, cisplatin plus gemcitabine and
cisplatin plus vinorelbine for advanced non-small-cell lung cancer:
Four-arm cooperative study in Japan. Ann Oncol. 18:317–323. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schiller JH, Harrington D, Belani CP,
Langer C, Sandler A, Krook J, Zhu J and Johnson DH: Eastern
Cooperative Oncology Group: Comparison of four chemotherapy
regimens for advanced non-small-cell lung cancer. N Engl J Med.
346:92–98. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kris MG, Natale RB, Herbst RS, Lynch TJ
Jr, Prager D, Belani CP, Schiller JH, Kelly K, Spiridonidis H,
Sandler A, et al: Efficacy of gefitinib, an inhibitor of the
epidermal growth factor receptor tyrosine kinase, in symptomatic
patients with non-small cell lung cancer: A randomized trial. JAMA.
290:2149–2158. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fukuoka M, Yano S, Giaccone G, Tamura T,
Nakagawa K, Douillard JY, Nishiwaki Y, Vansteenkiste J, Kudoh S,
Rischin D, et al: Multi-institutional randomized phase II trial of
gefitinib for previously treated patients with advanced
non-small-cell lung cancer (The IDEAL 1 Trial) [corrected]. J Clin
Oncol. 21:2237–2246. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lynch TJ, Bell DW, Sordella R,
Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat
SM, Supko JG, Haluska FG, et al: Activating mutations in the
epidermal growth factor receptor underlying responsiveness of
non-small-cell lung cancer to gefitinib. N Engl J Med.
350:2129–2139. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Paez JG, Jänne PA, Lee JC, Tracy S,
Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, et
al: EGFR mutations in lung cancer: Correlation with clinical
response to gefitinib therapy. Science. 304:1497–1500. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mitsudomi T, Morita S, Yatabe Y, Negoro S,
Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et
al: Gefitinib versus cisplatin plus docetaxel in patients with
non-small-cell lung cancer harbouring mutations of the epidermal
growth factor receptor (WJTOG3405): An open label, randomised phase
3 trial. Lancet Oncol. 11:121–128. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al: Gefitinib or chemotherapy for non-small-cell lung cancer
with mutated EGFR. N Engl J Med. 362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van
Oosterom AT, Christian MC and Gwyther SG: New guidelines to
evaluate the response to treatment in solid tumors. European
Organization for Research and Treatment of Cancer, National Cancer
Institute of the United States, National Cancer Institute of
Canada. J Natl Cancer Inst. 92:205–216. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nomoto K, Tsuta K, Takano T, Fukui T,
Fukui T, Yokozawa K, Sakamoto H, Yoshida T, Maeshima AM, Shibata T,
et al: Detection of EGFR mutations in archived cytologic specimens
of non-small cell lung cancer using high-resolution melting
analysis. Am J Clin Pathol. 126:608–615. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Takano T, Ohe Y, Tsuta K, Fukui T,
Sakamoto H, Yoshida T, Tateishi U, Nokihara H, Yamamoto N, Sekine
I, et al: Epidermal growth factor receptor mutation detection using
high-resolution melting analysis predicts outcomes in patients with
advanced non small cell lung cancer treated with gefitinib. Clin
Cancer Res. 13:5385–5390. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liu PY, Dahlberg S and Crowley J:
Selection designs for pilot studies based on survival. Biometrics.
49:391–398. 1993. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mok TS, Wu YL, Thongprasert S, Yang CH,
Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, et
al: Gefitinib or carboplatin-paclitaxel in pulmonary
adenocarcinoma. N Engl J Med. 361:947–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhou C, Wu YL, Chen G, Feng J, Liu XQ,
Wang C, Zhang S, Wang J, Zhou S, Ren S, et al: Erlotinib versus
chemotherapy as first-line treatment for patients with advanced
EGFR mutation-positive non-small-cell lung cancer (OPTIMAL,
CTONG-0802): A multicentre, open-label, randomised, phase 3 study.
Lancet Oncol. 12:735–742. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rosell R, Carcereny E, Gervais R,
Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R,
Pallares C, Sanchez JM, et al: Erlotinib versus standard
chemotherapy as first-line treatment for European patients with
advanced EGFR mutation-positive non-small-cell lung cancer
(EURTAC): A multicentre, open-label, randomised phase 3 trial.
Lancet Oncol. 13:239–246. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yang JC, Wu YL, Schuler M, Sebastian M,
Popat S, Yamamoto N, Zhou C, Hu CP, O'Byrne K, Feng J, et al:
Afatinib versus cisplatin-based chemotherapy for EGFR
mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6):
Analysis of overall survival data from two randomised, phase 3
trials. Lancet Oncol. 16:141–151. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Walter AO, Sjin RT, Haringsma HJ, Ohashi
K, Sun J, Lee K, Dubrovskiy A, Labenski M, Zhu Z, Wang Z, et al:
Discovery of a mutant-selective covalent inhibitor of EGFR that
overcomes T790M-mediated resistance in NSCLC. Cancer Discov.
3:1404–1415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cross DA, Ashton SE, Ghiorghiu S, Eberlein
C, Nebhan CA, Spitzler PJ, Orme JP, Finlay MR, Ward RA, Mellor MJ,
et al: AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated
resistance to EGFR inhibitors in lung cancer. Cancer Discov.
4:1046–1061. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jiang T and Zhou C: Clinical activity of
the mutant-selective EGFR inhibitor AZD9291 in patients with EGFR
inhibitor-resistant non-small cell lung cancer. Transl Lung Cancer
Res. 3:370–372. 2014.PubMed/NCBI
|