Introduction
With the advent of serum prostate-specific antigen
(PSA), a larger number of prostate cancers in the early phase have
been successfully detected. Although a decision to perform prostate
biopsy is routinely based on PSA levels, the PSA level is easily
influenced by benign prostatic hyperplasia, with poor specificity
(range, 4–10 ng/ml) (1).
Furthermore, the pathological stage advances with an increase in
PSA level, but considering that the range of the PSA level is so
wide, the PSA level alone cannot be relied upon to determine the
pathological stage. Therefore, although PSA incorporation into a
nomogram provides reasonably accurate predictions of the
pathological stage and PSA non-recurrence rates, novel alternative
markers are required.
Previous studies on PSA kinetics, such as the PSA
doubling time (PSADT), PSA slope, and PSA velocity (2–4), have
indicated that these may provide valuable information for diagnosis
and staging. The estimation of PSA kinetics, such as PSADT, is not
difficult; however, finding an important enough reason to wait for
>3 months to measure PSADT for staging prior to making a
decision regarding the treatment strategy is difficult.
Additionally, the prognostic values with respect to PSA recurrence
and cancer-specific mortality remain controversial (3–7).
To clarify the clinical significance of PSADT, in
the present study, the PSADTs prior to and following radical
prostatectomy were investigated. Patients with PSA failure were
also examined to assess how postoperative PSADT (post-PSADT) was
correlated with actual salvage therapy.
Patients and methods
Patients
A total of 488 patients with clinical stage
T1-3aN0M0 prostate cancer, who underwent radical prostatectomy and
bilateral pelvic lymphadenectomy between January 2001 and May 2009,
were retrospectively reviewed. None of the patients underwent
preoperative adjuvant hormonal or radiation therapy. It was
possible to calculate preoperative PSADT (pre-PSADT) in 204 of 488
patients by retrospectively reviewing their medical records. In
these patients, PSA measurements were made more than twice prior to
surgery, with >3-month intervals between the measurements.
Clinical T stage was assigned based on the findings of a digital
rectal examination performed using only the 2002 Union for
International Cancer Control (UICC) tumor-lymph nodes-metastasis
(TNM) staging system. Pathological information on biopsy and
radical prostatectomy specimens was obtained from official
reports.
Of the 488 patients, 111 exhibited PSA failure. PSA
failure was defined as an increase in the levels of PSA by ≥0.2
ng/ml, more than twice consecutively following surgery. Post-PSADT
was calculated in 51 patients who were not immediately treated
using salvage therapy.
PSADT calculation and analysis
For each patient, a linear regression of log PSA
against time was calculated, and PSADT was computed as log 2
divided by the slope: Ln2/rv, rv = d/dt {ln [PSA (t)]} (8). While evaluating PSADT, the value was
categorized into six groups: Stable (<0 month) and PSA 0–6
months, 6–12 months, 12–18 months, 18–24 months, and >24
months.
Statistical analysis
Clinical and pathological findings and PSADT were
analyzed using the Kruskal-Wallis, chi-square, and Mann-Whitney U
tests. PSA non-recurrence rates were determined using the
Kaplan-Meier methods, and the differences resulting from this
analysis were tested using the log-rank test. Univariate and
multivariate Cox regression analyses were used to predict PSA
recurrence following surgery. All analyses were performed using the
STATA version 10 software package (StataCorp LP, College Station,
TX, USA). P<0.05 was considered to indicate a statistically
significant value.
Results
The clinical and pathological features of the 204
patients are listed in Table I.
 | Table I.Association between
clinical/pathological features and preoperative PSADT in 204
patients with clinically localized prostate cancer. |
Table I.
Association between
clinical/pathological features and preoperative PSADT in 204
patients with clinically localized prostate cancer.
| Variable | Frequency, no. of
patients (%) | PSADT (months),
median (range) |
|---|
| Last measured serum
PSA level prior to surgery (ng/ml), median (range) |
| P<0.0005 |
|
<4.0 | 9 (4.4) | 19.38 (0–95.5) |
|
4.1–10.0 | 130 (63.7) | 7.76 (−28.2–286) |
|
10.1–20.0 | 43 (22.1) | 4.02
(−9.08–34.5) |
|
>20 | 22 (10.8) | 1.25 (−5.0–20.6) |
| Clinical stage |
| P=0.471 |
| T1c | 155 (76.0) | 6.0 (−28.1–286) |
| T2a | 29 (14.2) | 3.63
(−9.08–44.3) |
| T2b | 12 (5.9) | 8.21 (0.7–82.4) |
| T2c | 6 (2.9) | 1.61 (0–16.9) |
| T3a | 2 (1.0) | 5.1 (0–10.3) |
| Risk group |
| P<0.0005 |
| Low | 56 (27.4) | 9.47 (−6.5–95.5) |
|
Intermediate | 86 (42.2) | 5.91 (−28.1–286) |
| High | 62 (30.4) | 3.58 (−5–107) |
| Pathological
stage |
| P=0.01 |
| pT2 | 121 (59.3) | 6.63 (−28.1–286) |
| pT3a | 64 (31.4) | 5.13 (−4.5–83.2) |
| pT3b | 16 (7.8) | 3.23 (−0.2–20.5) |
| pN+ | 3 (1.5) | 1.13 (0.6–8.0) |
| Specimen Gleason
score |
| P=0.098 |
| 4–6 | 55 (27.0) | 8.86 (−9.0–83.2) |
| 7 | 94 (46.0) | 4.59 (−28.1–286) |
| 8–10 | 55 (27.0) | 6.0 (−4.2–26.7) |
Pre-PSADT
The median age of 51 patients at radical
prostatectomy was 68 years (range, 59–78 years). The median number
of preoperative PSA measurements in 204 patients was 3.5 (range,
2–26); PSA was measured for a median period of 11.9 months (range,
3–112.8 months) prior to the diagnosis by needle biopsy. The median
of the initial and final PSA levels was 5.5 ng/ml (range, 0.7–46.3
ng/ml) and 7.35 ng/ml (range, 1.1–65.5 ng/ml), respectively. The
calculated median PSADT in patients with increasing PSA levels was
5.93 months (range, −28.2–287 months). PSA levels increased during
the observation period in 169 of the 204 patients, whereas 35
(17.2%) of them had stable levels.
Associations between pathological findings and
pre-PSADT are shown in Table II.
Prostatectomy specimen analysis revealed more locally confined
cancer in patients with a PSADT of >24 months compared with
those with shorter PSADTs (P<0.05).
| Table II.Pathological features of cancer in
radical prostatectomy specimens according to pre PSADT. |
Table II.
Pathological features of cancer in
radical prostatectomy specimens according to pre PSADT.
|
| Pathological stage, n
(%) | Specimen Gleason
score, n (%) |
|---|
|
|
|
|
|---|
| Pre-PSADT
(months) | No of patients | pT2 | pT3a (EPE+) | pT3b (SV+) | pN+ (LV+) | 2–6 | 7 | 8–10 |
|---|
| Stable | 35 | 17 (49) | 14 (40) | 4 (11) | 0 | 8 (23) | 19 (54) | 8 (23) |
| <6 | 69 | 39 (57) | 21 (30) | 7 (10) | 2 (3) | 12 (17.4) | 37 (53.6) | 20 (29.0) |
| 6.0–11.9 | 42 | 26 (62.0) | 12 (28.5) | 3 (7.1) | 1 (2.4) | 12 (28.5) | 17 (40.5) | 13 (31.0) |
| 12.0–17.9 | 22 | 13 (59.1) | 8 (36.4) | 1 (4.5) | 0 | 8 (36.4) | 8 (36.4) | 6 (27.2) |
| 18.0–23.9 | 16 | 10 (62.5) | 5 (31.3) | 1 (6.2) | 0 | 4 (25.0) | 6 (37.5) | 6 (37.5) |
| ≥24.0 | 20 | 16
(80.0)a | 4 (20.0) | 0 | 0 | 11
(55.0)b | 7 (35.0) | 2 (10) |
Associations between Gleason scores and pre-PSADT
are also shown in Table II.
Patients with a Gleason score of 26 prostatic cancers exhibited a
significantly longer PSADT (>24 months) compared with those
without these characteristics (P=0.003; Table III).
| Table III.Association between the initial PSA
level and PSADT. |
Table III.
Association between the initial PSA
level and PSADT.
| Initial PSA
(ng/ml) | Νo. of patients | Preoperative PSADT
(month), median (range) | Nο. of PSA
measurements (times), median (range) | Period between PSA
measurements (month), median (range) |
|---|
| 0–3 | 29 | 16.2 (3–95.5) | 5 (2–26) | 48.6
(3.0–112.8) |
| 3.1–6 | 83 |
7.4
(−28.1–286) | 4 (2–24) | 12.9
(3.0–60.4) |
| 6.1–9 | 41 |
4.8
(−22.9–83.2) | 3 (2–16) | 8.7 (3.0–66.3) |
| 9.1–12 | 24 |
3.2
(−4.5–12.6) | 3 (2–9) | 5.5 (3.0–19.5) |
| 12.1–15 | 6 |
1.9
(−2.0–6.9) | 3.5 (2–8) | 7.1 (3.0–34.1) |
| >15 | 21 |
1.13
(−5.0–13.4) | 3 (2–6) | 4.6 (3.1–49.0) |
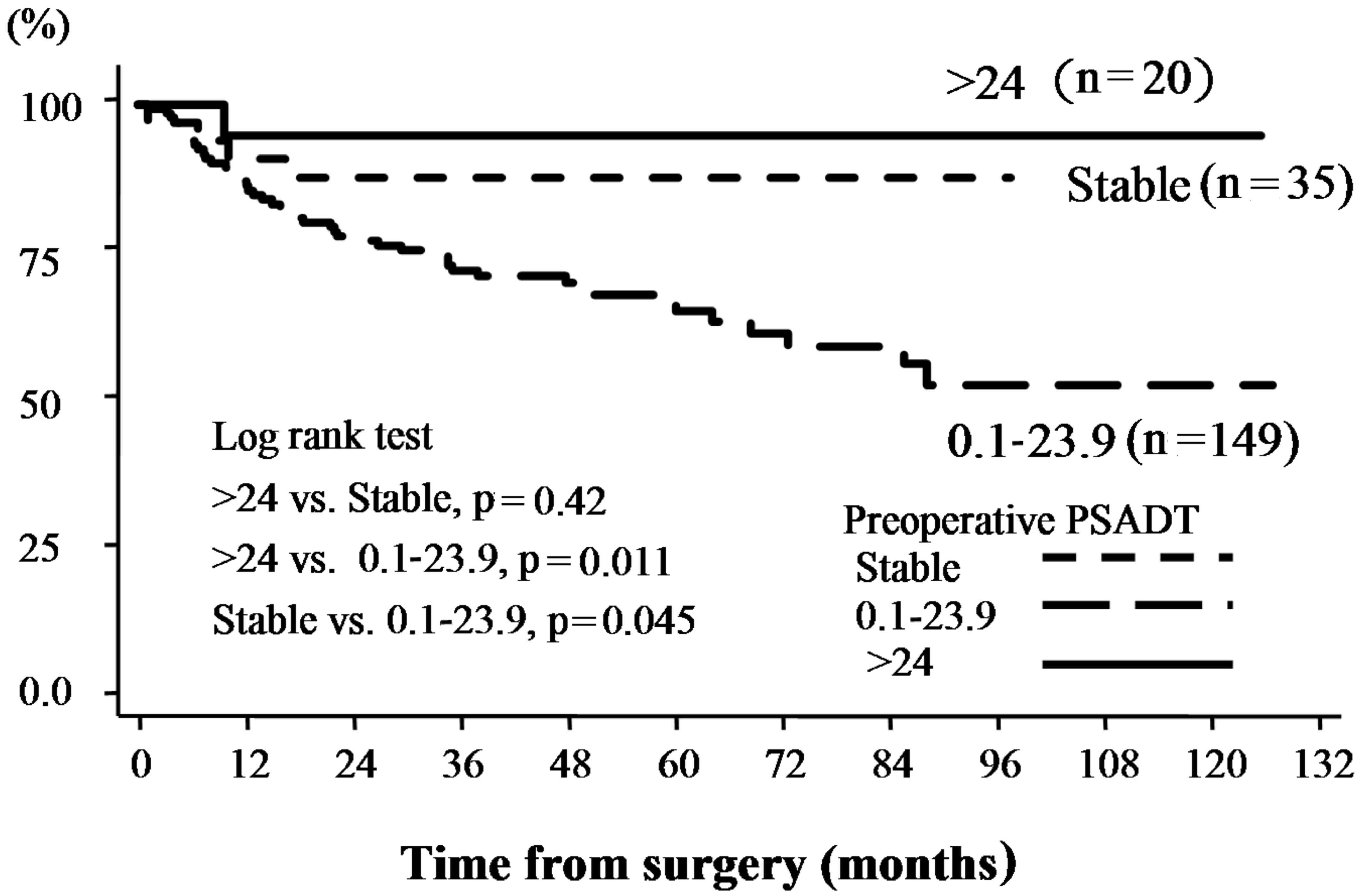
Relationships between PSA failure following
prostatectomy and pre-PSADT are shown in Table III. Pathological outcomes revealed
significantly lower PSA levels in 20 patients with a PSADT of
>24 months and stable PSADT compared with other groups. No
significant differences were identified among patients with a PSADT
<24 months (Fig. 1).
PSADTs >24 months and stable PSADTs were
associated with PSA recurrence following surgery based on
multivariate analysis with age, preoperative PSA, biopsy Gleason
score, and clinical stage (P=0.008; Table IV).
| Table IV.Univariate and multivariate Cox
regression analyses to predict PSA recurrence following
surgery. |
Table IV.
Univariate and multivariate Cox
regression analyses to predict PSA recurrence following
surgery.
|
| P-value (HR, 95%
CI)a |
|---|
|
|
|
|---|
| Variable | Univariate | Multivariate |
|---|
| Age | n.s. | – |
| Preoperative
PSA | 0.0029 (1.03,
1.00–1.060) | n.s. |
| Clinical T
stage | 0.001 (1.68,
1.23–2.29) | 0.009 (1.60,
1.12–2.29) |
| Biopsy Gleason
score | 0.002 (1.44,
1.14–1.81) | 0.005 (1.38,
1.10–1.75) |
| PSA doubling
time | 0.005 (2.82,
1.37–5.79) | 0.008 (2.76,
1.30–5.85) |
| (>24 months,
stable, 0.1–24 months) |
|
|
Post-PSADT
Of the 111 patients with PSA failure, 60 patients
underwent salvage hormonal or radiation therapy soon after their
diagnosis; therefore, post-PSADT could not be measured.
The median age of 51 patients at the time of radical
prostatectomy was 66 years (range, 50–77 years). The median period
from radical surgery to the diagnosis of PSA failure was 11.1
months (range, 0–125.4 months). The median preoperative serum PSA
level was 8.6 ng/ml (range, 4.3–65.5 ng/ml). The median number of
PSA recordings per patient following surgery was eight (range, 4–59
recordings). In total, 51 patients were clinically classified as
having stage T1c (30, 58.8%), T2a (10, 19.6%), T2b (6, 11.8%), T2c
(4, 7.8%), and T3a (1, 2.0%) tumors. The biopsy tumor grade was
classified based on Gleason scores as follows: Under 2–6 (13
patients, 25.5%), 7 (22 patients, 43.1%), and 8–10 (16 patients,
31.4%). In total, 21 (41.2%) patients were identified as having
locally advanced disease on final pathological examination;
extracapsular extension was observed in 20 (39.2%) patients,
seminal vesicle involvement was observed in 8 (15.7%) patients, and
lymph node involvement was positive in 2 (3.9%) patients. The
calculated median post-PSADT was 7.76 months (range, 0.1–177.1
months). Associations among the pathological findings and
post-PSADT are shown in Table IV.
Pathologically, 87.5% of the eight patients with a post-PSADT of
>24 months, and 32.5% of the 43 patients with a post-PSADT
<24 months had cancer confined to the prostate (P=0.004;
Table V). No clear association was
identified between the specimen Gleason scores and post-PSADT
(Table V).
| Table V.Pathological stage and Gleason score
according to postoperative PSADT in 51 patients with PSA
recurrence. |
Table V.
Pathological stage and Gleason score
according to postoperative PSADT in 51 patients with PSA
recurrence.
|
| Pathological stage,
n (%) | Specimen Gleason
score, n (%) |
|---|
|
|
|
|
|---|
| Post-PSADT
(months) | No. of
patients | pT2 | pT3a (EPE+) | pT3b (SV+) | pN+ (LV+) | 2–6 | 7 | 8–10 |
|---|
| <6 | 23 | 2 (8.7) | 11 (47.8) | 8 (34.8) | 2 (8.7) | 0 (0) | 11 (47.8) | 12 (52.2) |
| 6.0–11.9 | 13 | 8 (61.5) | 5 (38.5) | − | – | 3 (23.2) | 5 (38.4) | 5 (38.4) |
| 12.0–17.9 | 6 | 4 (66.7) | 2 (33.3) | − | – | 2 (33.3) | 2 (33.3) | 2 (33.3) |
| 18.0–23.9 | 1 | – | 1 (100) | − | – | – | – | 1 (100) |
| ≥24.0 | 8 | 7
(87.5)a | 1 (12.5) | 0 | 0 | 2 (25) | 4 (50) | 2 (25) |
The treatment after PSA failure is shown in Table VI. In total, 16 patients underwent
salvage hormonal and/or radiation therapy. Of those 16 patients,
eight underwent hormonal therapy, two underwent radiation therapy,
and six underwent both treatments (Table VI). None of the 15 patients with a
post-PSADT >12 months underwent a second treatment, with a
median follow-up period of 49.4 months. No association was
identified between pre- and post-PSADT.
| Table VI.Association between postoperative
PSADT and salvage treatments. |
Table VI.
Association between postoperative
PSADT and salvage treatments.
|
|
| Salvage
treatments |
|---|
|
|
|
|
|---|
| Postoperative PSADT
(months) | No. of
patients | Observation | Hormonal
therapy | Radiotherapy | Hormonal and
radiotherapy |
|---|
| <6 | 23 | 9 (39.1) | 6 (26.1) | 2 (8.7) | 6 (26.1) |
| 6.0–11.9 | 13 | 11 (84.6) | 2 (15.4) | 0 | 0 |
| ≥12.0 | 15 | 15 (100) | 0 | 0 | 0 |
Discussion
The significance of PSADT after each treatment is an
important prognostic factor (9–13).
Although previous studies have indicated that the diagnostic value
in patients with low PSA levels offers only limited advantages,
there may be certain advantages in predicting oncological outcomes
(14–17). Hanks et al (14) examined 99 patients with T1-3NXM0
prostate cancer who underwent external radiotherapy, and identified
that the pre-PSADT is an independent predictor of biochemical
freedom from disease. Overall, 89% patients with a PSADT of >12
months had no recurrence, whereas 50% of the patients with a PSADT
of <12 months had recurrence within 1.5 years (14). Shulman et al (18) studied 163 patients with
castration-resistant prostate cancer, and demonstrated that
patients with a PSADT >12 months exhibited an improved response
to deferred anti-androgen therapy compared with those with a PSADT
of <12 months. D'Amico et al (19) examined the association between
prostate cancer death and PSADT in 5,918 patients following
prostatectomy, and 2,751 patients following external radiotherapy,
and reported an association between a PSADT <3 months and death
due to cancer; therefore, hormonal therapy was recommended in cases
of PSA failure following surgical or radiation treatment where the
patients had a PSADT of <3 months (19). Thus, the importance of PSADT for
predicting oncological outcomes has been demonstrated, and the
cutoff of PSADT may vary, depending on different populations and
endpoints.
Several investigators have suggested PSADT may be
used to predict treatment outcome prior to radical prostatectomy.
Goluboff et al (8) examined
56 patients with three or more PSA levels prior to radical
prostatectomy, and calculated the pre-PSADT; they identified that
pre-PSADT did not correlate with PSA failure, final PSA, or the
Gleason score, but only with the pathological stage. However, in
their study, the median followup period following radical surgery
was only 17.3 months, which they reported was an improvement
compared with conducting a longer follow-up to examine the
correlation of pre-PSADT with the pathological stage and PSA
failure. Egawa et al (20)
retrospectively studied pre-PSADT in 62 patients with T1-3N0M0
prostate cancer, and reported that pre-PSADT is significantly
associated with the final pathological stage and PSA failure
following radical prostatectomy. Early PSA failure was revealed to
be more common in patients with rapid PSADT. However, they were not
able to identify any independent factor for predicting the
pathological stage and PSA failure in a multivariate logistic
regression analysis. The results in the present study are similar
to those mentioned by Egawa et al (20). In addition, in the present paper, it
has been demonstrated that pre-PSADT is an independent factor for
PSA failure, similar to the results obtained for the biopsy Gleason
score and clinical stage via the multivariate logistic regression
analysis (Table IV).
The consensus view is that a large number of
physicians consider PSADT to be useful. However, it is not popular
in clinical use, mainly due to the need to wait for >3 months in
order to calculate PSADT following cancer diagnosis, which is
problematical in view of the need to select a treatment option.
In the present study, 35 patients had a stable PSADT
with no change in PSA level over time. Initially, our consideration
was that these patients were similar to those with a long PSADT;
therefore, they should have favorable pathological results.
However, the patients were revealed to have worsened pathological
stages, similar to those of patients with a PSADT of <24 months.
This is due to the fact that the majority of patients with a stable
PSADT had a markedly higher initial PSA level; therefore, they
underwent surgery with few PSA measurements. Consequently, the
role, and importance, of PSADT where higher initial PSA levels are
involved may be restricted. Conversely, in the present study,
patients with a lower initial PSA level, e.g., <4 ng/ml, tended
to have a longer PSADT, as shown in Table III. Also, PSADT, along with the
biopsy Gleason score and clinical stage, is an independent factor
for predicting postoperative PSA failure (Table IV). Therefore, the authors of the
present study consider that patients with a lower initial PSA level
may be safely kept under observation to measure PSADT, which may
help a decision to be made on the requirement of observation
without an aggressive treatment. The present study only examined
cases of patients who were treated with radical prostatectomy;
however, if PSADT is applied for all patients with positive biopsy,
it may serve a more important role in actual clinical diagnosis.
McLaren et al (6) suggested
PSADT to be the strongest predictor of clinical progression in
patients treated with watchful waiting. They examined 113 patients
treated with watchful waiting, and reported that ~40% of T1
patients, and 51% of T2 patients, had a clinical progression by 2
years, which increased to 60% at 3 years. Multivariate analysis
revealed a strong correlation of PSADT with clinical progression,
stage progression, and time of treatment (6).
The method for treating patients with PSA failure
following radical prostatectomy remains controversial. A large
number of physicians use hormonal or radiation therapy immediately
after PSA failure, although certain patients may be followed up
with no immediate treatments. The present study included 51 such
patients. The decision to undergo no immediate treatment was
suggested by their physician, who would have considered the
pathological features in radical prostatectomy. However, as a
result, those with a post-PSADT of >12 months had cancer
confined to the prostate, and did not have a clinical recurrence
without salvage therapy for a lengthy time period (median, 73
months). Therefore, the results of the present study indicated
that, when considering early salvage therapy for PSA failure
following radical prostatectomy, it is possible not to administer a
salvage treatment if the cancer is pathologically confined to the
prostate and PSADT is slow (e.g., >12 months).
Conversely, use of the PSADT is limited, since
considering early salvage hormonal and radiation therapies is
necessary if patients have prostate cancer, particularly with lymph
node metastases, seminal vesicle invasion, or a Gleason score of
8–10. Our hypothesis is that it is necessary to clarify the
correlation between post-PSADT and the appearance of metastasis and
mortality due to prostate cancer to decide the therapy and its
initiation time.
Freedland et al (21) examined 379 patients with PSA
recurrence following radical prostatectomy for a median follow-up
period of 10 years, and reported that clinical parameters,
including PSADT, may help to identify the risk of cancerspecific
mortality. However, in the present study, pre-PSADT and post-PSADT
lacked any association.
The present study had certain limitations due to its
retrospective nature and the small number of patients who underwent
radical prostatectomy. Further investigation of the association
between metastasis and mortality due to prostate cancer is
currently under way.
In conclusion, a long PSADT, e.g., >24 months,
indicates that the cancer is confined to the prostate, and a lower
rate of PSA recurrence following surgery. This information may
assist in allowing clinical decisions to be made. In particular, in
prostate cancer with initial low PSA levels, the conservative
therapeutic method, including active surveillance, may be
considered if patients have a pre-PSADT of >24 months.
Therefore, it is considered that measuring pre-PSADT in such
patients could be informative. Furthermore, when considering early
salvage therapy for PSA failure following radical prostatectomy, if
the pathological stage of the specimen is cancer confined to the
prostate with a long post-PSADT, the patient may be provided with
an option of choosing observation without early salvage
therapy.
Acknowledgements
The authors would like to thank Enago™ English
Editing services (www.enago.jp), for reviewing the
English language of the original manuscript.
References
|
1
|
Catalona WJ, Smith DS, Ratliff TL, Dodds
KM, Coplen DE, Yuan JJJ, Petros JA and Andriole GL: Measurement of
prostate-specific antigen in serum as a screening test for prostate
cancer. N Engl J Med. 324:1156–1161. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Loeb S, Roehl KA, Helfand BT, Kan D and
Catalona WJ: Can prostate specific antigen velocity thresholds
decrease insignificant prostate cancer detection? J Urol.
183:112–116. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Carter HB, Morrell CH, Pearson JD, Brant
LJ, Plato CC, Metter EJ, Chan DW, Fozard JL and Walsh PC:
Estimation of prostatic growth using serial prostate-specific
antigen measurements in men with and without prostate disease.
Cancer Res. 52:3323–3328. 1992.PubMed/NCBI
|
|
4
|
Nam RK, Klotz LH, Jewett MAS, Danjoux C
and Trachtenberg J: Prostate specific antigen velocity as a measure
of the natural history of prostate cancer: Defining a ‘rapid riser’
subset. Br J Urol. 81:100–104. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
D'Amico AV and Hanks GE: Linear regressive
analysis using prostate-specific antigen doubling time for
predicting tumor biology and clinical outcome in prostate cancer.
Cancer. 72:2638–2643. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
McLaren DB, McKenzie M, Duncan G and
Pickles T: Watchful waiting or watchful progression?: Prostate
specific antigen doubling times and clinical behavior in patients
with early untreated prostate carcinoma. Cancer. 82:342–348. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee WR, Hanks GE, Corn BW and Schultheiss
TE: Observations of pretreatment prostate-specific antigen doubling
time in 107 patients referred for definitive radiotherapy. Int J
Radiat Oncol Biol Phys. 31:21–24. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Goluboff ET, Heitjan DF, DeVries GM, Katz
AE, Benson MC and Olsson CA: Pretreatment prostate specific antigen
doubling times: Use in patients before radical prostatectomy. J
Urol. 158:1876–1878; discussion 1878–1879. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Arlen PM, Bianco F, Dahut WL, D'Amico A,
Figg WD, Freedland SJ, Gulley JL, Kantoff PW, Kattan MW, Lee A, et
al: Prostate Specific Antigen Working Group: Prostate Specific
Antigen Working Group guidelines on prostate specific antigen
doubling time. J Urol. 179:2181–2185; discussion 2185–2186. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Egawa S, Matsumoto K, Suyama K, Iwamura M,
Kuwao S and Baba S: Observations of prostate specific antigen
doubling time in Japanese patients with nonmetastatic prostate
carcinoma. Cancer. 86:463–469. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gerber GS, Gornik HL, Goldfischer ER,
Chodak GW and Rukstalis DB: Evaluation of changes in prostate
specific antigen in clinically localized prostate cancer managed
without initial therapy. J Urol. 159:1243–1246. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Smith MR, Kabbinavar F, Saad F, Hussain A,
Gittelman MC, Bilhartz DL, Wynne C, Murray R, Zinner NR, Schulman
C, et al: Natural history of rising serum prostate-specific antigen
in men with castrate nonmetastatic prostate cancer. J Clin Oncol.
23:2918–2925. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Schmid H-P, McNeal JE and Stamey TA:
Observations on the doubling time of prostate cancer. The use of
serial prostate-specific antigen in patients with untreated disease
as a measure of increasing cancer volume. Cancer. 71:2031–2040.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hanks GE, Hanlon AL, Lee WR, Slivjak A and
Schultheiss TE: Pretreatment prostate-specific antigen doubling
times: Clinical utility of this predictor of prostate cancer
behavior. Int J Radiat Oncol Biol Phys. 34:549–553. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sandler HM, Dunn RL, McLaughlin PW, Hayman
JA, Sullivan MA and Taylor JM: Overall survival after
prostate-specific-antigen-detected recurrence following conformal
radiation therapy. Int J Radiat Oncol Biol Phys. 48:629–633. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Loberg RD, Fielhauer JR, Pienta BA,
Dresden S, Christmas P, Kalikin LM, Olson KB and Pienta KJ:
Prostate-specific antigen doubling time and survival in patients
with advanced metastatic prostate cancer. Urology 62 (Suppl 1).
128–133. 2003. View Article : Google Scholar
|
|
17
|
Semeniuk RC, Venner PM and North S:
Prostate-specific antigen doubling time is associated with survival
in men with hormone-refractory prostate cancer. Urology.
68:565–569. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shulman MJ, Karam JA and Benaim EA:
Prostate-specific antigen doubling time predicts response to
deferred antiandrogen therapy in men with androgen-independent
prostate cancer. Urology. 63:732–736. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
D'Amico AV, Moul JW, Carroll PR, Sun L,
Lubeck D and Chen MH: Surrogate end point for prostate
cancer-specific mortality after radical prostatectomy or radiation
therapy. J Natl Cancer Inst. 95:1376–1383. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Egawa S, Arai Y, Tobisu K, Kuwao S, Kamoto
T, Kakehi Y and Baba S: Use of pretreatment prostate-specific
antigen doubling time to predict outcome after radical
prostatectomy. Prostate Cancer Prostatic Dis. 3:269–274. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Freedland SJ, Humphreys EB, Mangold LA,
Eisenberger M, Dorey FJ, Walsh PC and Partin AW: Risk of prostate
cancer-specific mortality following biochemical recurrence after
radical prostatectomy. JAMA. 294:433–439. 2005. View Article : Google Scholar : PubMed/NCBI
|