Introduction
Richter's transformation represents an aggressive
evolution of chronic lymphocytic leukemia (CLL) (1). High-grade B-cell non-Hodgkin lymphoma
(B-NHL) is the most common histological type of Richter's
transformation (2). However, other
histological types, such as classical Hodgkin lymphoma (cHL)
(2–4),
lymphoblastic lymphoma (5), hairy
cell leukemia (6) and high-grade
T-cell NHL (7,8) have been reported previously. B-CLL and
cHL can be clonally related or independent lymphomas (9,10).
Different therapy modalities are reviewed in the
present study regarding the optimal treatment strategy for Hodgkin
transformation. However, despite the different chemotherapeutic
regiments, the prognosis remains poor compared to de novo
Hodgkin's lymphoma (4) and new
therapeutic approaches shoud be considered in the future.
Case report
A 70-year-old male presented with right thoracic
pain. A computer tomography (CT) scan showed thoracic and
retroperitoneal lymphadenopathy with a maximal diameter of 21 mm,
and a pleural effusion at the right side. Routine blood
investigations showed normal erythrocyte, platelet and leukocyte
counts.
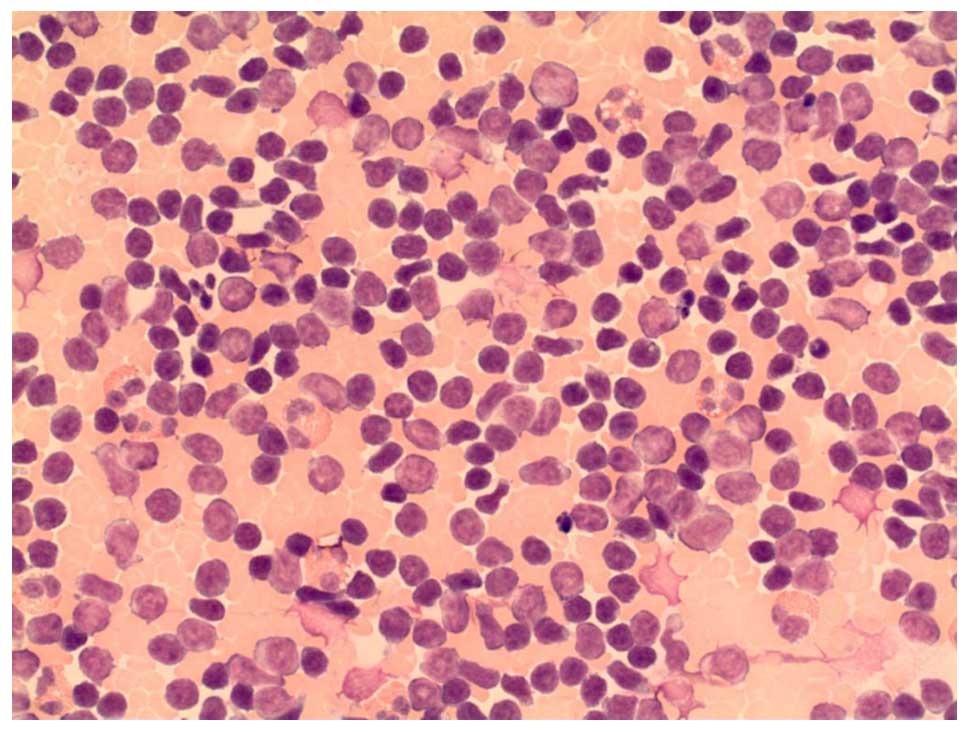
The cytology of the pleural effusion revealed an
atypical B-cell population consistent with B-CLL (Fig. 1). Bone marrow aspiration confirmed the
diagnosis of CLL, stage Binet B. Fluorescence in situ
hybridisation (FISH) analyses of bone marrow excluded trisomy 12,
and deletions of 11q22.3, 13q14 and 17p13. FISH experiments were
performed using commercially available probes from Abbott (Abbott
Park, IL, USA), according to the manufacturer's protocol. A
watch-and-wait approach was applied. During the following months
the patient suffered from repeated infections due to
hypogammaglobulinemia with immunoglobulin G (IgG) <3 g/l, and
therefore, immunoglobulin substitution and antibiotic therapy was
repeatedly necessary.
Two months later the patient complained of fever,
cough, right thoracic pain and fatigue. A repeated CT scan of the
thorax showed a pleural effusion again. In order to exclude pleural
empyema, video-assisted thoracoscopic surgery with pleurectomy was
performed. Histological analysis revealed a marked pleural fibrosis
with scattered cellular lymphoid nodules. The latter contained a
variable mixture of small B- and T-cell lymphocytes, histiocytes,
fibroblasts, eosinophils and scattered atypical blasts
corresponding to Hodgkin cells and Reed-Sternberg (HRS) cells. The
B-cell lymphocytes were cluster of differentiation (CD)
20-positive, but did not co-express CD5 or CD23, as assessed using
monoclonal antibodies recognizing these antigens in
paraffin-embedded tissue. Therefore, the small aggregates of the
B-cells did not fulfil the diagnostic criteria for a B-CLL
infiltration. HRS-blasts proved to be CD20-negative, but showed
expression of CD30, CD15 and PAX5. Additionally, in situ
hybridization for Ebstein-Barr virus (EBV) was positive.
Accordingly, diagnosis of nodular sclerosis-type classical
Hodgkin's lymphoma was rendered. The disease was staged as IV due
to the pleural involvement.
Comparative molecular analyses of the IgH of
selected tissue compartments of the pleural biopsy and of
peripheral blood B-lymphocytes were performed using multiplex
polymerase chain reaction (PCR) with BIOMED-2 primer sets, as
previously described (11). The
resulting PCR amplicons showed identical sizes indicating the same
IgH heavy chain rearrangement in both lymphoma manifestations, and
thus a common clonal origin of CLL and cHL.
Chemotherapy with 25 mg/m2 doxorubicin,
10 mg/m2 bleomycine, 6 mg/m2 vinblastine and
375 mg/m2 dacarbazine on days 1 and 15 was introduced,
for a total of 8 cycles. A complete remission was achieved.
Discussion
Approximately 2–8% of all patients diagnosed with
CLL transform into more aggressive lymphoma known as Richter's
syndrome (1). The most common is the
transformation of CLL into a high-grade B-NHL (2). Transformation to HL is thought to occur
in ~0.4% of all CLL patients (3,4). Other
histological types of Richter's transformation have also been
described, including lymphoblastic lymphoma (5), hairy cell leukemia (6) and high-grade T-cell NHL (7,8).
A published small series suggested that tumor cells
in B-NHL and cHL can be clonally related to B-CLL clone or arise as
an independent, secondary lymphoma (9,10).
Additionally, it has been postulated that immunosuppressive therapy
in CLL, particularly fludarabin, may increase the risk of Richter's
transformation to cHL (12,13).
EBV infection is only infrequently detected in CLL
by conventional diagnostic approaches. However, it has been shown
that EBV persistence in the lymphocytes of patients with CLL may
lead to the more aggressive disease and Richter's transformation
into cHL (14,15). Several studies showed that EBV small
non-coding RNA (EBERs) expressed in latently infected cells have a
critical role in B-cell transformation and induction of resistance
to apoptosis, which may lead to CLL progression (16).
According to the largest series of published Hodgkin
transformation in CLL, in 3 out of 4 analysed patients (75%), EBV
was detected (4). In the patient
reported in the present study, Hodgkin cells were also
EBV-positive, as documented by EBER in situ hybridisation.
However, the role of antiviral therapy in the treatment of Hodgkin
transformation in CLL remains to be elucidated.
Bone marrow cytogenetics revealed a normal karyotype
in 42% of the cases in one study (4),
wheres abnormalities, including −Y, 11q-, del (13), t(9;15), trisomy 12, −11 and −17, were
identified in <40% of the cases (4). FISH analyses of the bone marrow in the
present patient were negative for trisomy 12, deletion 11q22.3,
deletion 13q14 or deletion 17p13.
cHL transformation in CLL has a poor outcome
compared to the de novo Chl (4). The administration of different therapy
modalities to the patients with HL as Richter's transformation has
been described previously (Table I).
However, the median overall survival, according to the largest
series of published Hodgkin transformation in CLL, was only 8
months (4).
 | Table I.Most common described treatment
options of Hodgkin's transformation of CLL (4,11). |
Table I.
Most common described treatment
options of Hodgkin's transformation of CLL (4,11).
| Treatment | Specific drugs and
therapy |
|---|
| ABVD | Doxorubicin,
bleomycin, vinblastine and dacarbazine |
| CVPP ± involved field
radiation | Cyclophosphamide,
vinblastine, procarbazine and prednisone ± involved field
radiation |
| MOPP | Mecholrethamine,
oncovin, procarbazine and prednisone |
| CHOP ± R | Cyclophosphamide,
doxorubicin, vincristine and prednisone ± rituximab |
| FCR | Fludarabine,
cyclophosphamide and rituximab |
| Other | Mitoxantrone,
vincristine, vinblastine and prednisone; rituximab; or
cidofovir |
More effective treatment is required for patients
who develop Hodgkin transformation of CLL. The role of high-dose
chemotherapy with autologous stem cell transplantation in these
patients is not well defined. However, this more aggressive
approach may not be feasible in elderly groups of patients.
References
|
1
|
Rossi D, Cerri M, Capello D, Deambrogi C,
Rossi FM, Zucchetto A, De Paoli L, Cresta S, Rasi S, Spina V, et
al: Biological and clinical risk factors of chronic lymphocytic
leukaemia transformation to Richter syndrome. Br J Haematol.
142:202–215. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tsimberidou AM and Keating MJ: Richter
syndrome: Biology, incidence and therapeutic strategies. Cancer.
103:216–228. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nemets A, Ben Dor D, Barry T, Ducach A,
Blumental R, Ben Alon D and Lugassy G: Variant Richter's syndrome:
A rare case of classical Hodgkin's lymphoma developing in a patient
with chronic lymphocytic leukemia treated with fludarabine. Leuk
Lymphoma. 44:2151–2154. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tsimberidou AM, O'Brien S, Kantarjian HM,
Koller C, Hagemeister FB, Fayad L, Lerner S, Bueso-Ramos CE and
Keating MJ: Hodgkin transformation of chronic lymphocytic leukemia:
The M. D. Anderson cancer center experience. Cancer. 107:1294–1302.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pistoia V, Roncella S, Di Celle PF,
Sessarego M, Cutrona G, Cerruti G, Boccaccio GP, Grossi CE, Foà R
and Ferrarini M: Emergence of a B-cell lymphoblastic lymphoma in a
patient with B-cell chronic lymphocytic leukemia: Evidence for the
single-cell origin of the two tumors. Blood. 78:797–804.
1991.PubMed/NCBI
|
|
6
|
Duchayne E, Delsol G, Kuhlein E, Klein B,
Zhang XG, Attal M, Cassard G and Laurent G: Hairy cell
transformation of a B-cell chronic lymphocytic leukemia: A
morphological, cytochemical, phenotypic and molecular study.
Leukemia. 5:150–155. 1991.PubMed/NCBI
|
|
7
|
Strickler JG, Amsden TW and Kurtin PJ:
Small B-cell lymphoid neoplasms with coexisting T-cell lymphomas.
Am J Clin Pathol. 98:424–429. 1992.PubMed/NCBI
|
|
8
|
Lee A, Skelly ME, Kingma DW and Medeiros
LJ: B-cell chronic lymphocytic leukemia followed by high grade
T-cell lymphoma. An unusual variant of Richter's syndrome. Am J
Clin Pathol. 103:348–352. 1995.PubMed/NCBI
|
|
9
|
Mao Z, Quintanilla-Martinez L, Raffeld M,
Richter M, Krugmann J, Burek C, Hartmann E, Rudiger T, Jaffe ES,
Müller-Hermelink HK, et al: IgVH mutational status and clonality
analysis of Richter's transformation: Diffuse large B-cell lymphoma
and Hodgkin lymphoma in association with B-cell chronic lymphocytic
leukemia (B-CLL) represent 2 different pathways of disease
evolution. Am J Surg Pathol. 31:1605–1614. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
van den Berg A, Maggio E, Rust R, Kooistra
K, Diepstra A and Poppema S: Clonal relation in a case of CLL, ALCL
and Hodgkin composite lymphoma. Blood. 100:1425–1429.
2002.PubMed/NCBI
|
|
11
|
van Dongen JJ, Langerak AW, Brüggemann M,
Evans PA, Hummel M, Lavender FL, Delabesse E, Davi F, Schuuring E,
et al: Design and standardization of PCR primers and protocols for
detection of clonal immunoglobulin and T-cell receptor gene
recombinations in suspect lymphoproliferations: report of the
BIOMED-2 Concerted Action BMH4-CT98-3936. Leukemia. 17:2257–2317.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bockorny B, Codreanu I and Dasanu CA:
Hodgkin lymphoma as Richter transformation in chronic lymphocytic
leukaemia: A retrospective analysis of world literature. Br J
Haematol. 156:50–66. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dasanu CA: Intrinsic and treatment-related
immune alterations in chronic lymphocytic leukaemia and their
impact for clinical practice. Expert Opin Pharmacother.
9:1481–1494. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dolcetti R and Carbone A: Epstein-Barr
virus infection and chronic lymphocytic leukemia: A possible
progression factor? Infect Agent Cancer. 5:222010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rubin D, Hudnall SD, Aisenberg A, Jacobson
JO and Harris NL: Richter's transformation of chronic lymphocytic
leukemia with Hodgkin's-like cells is associated with Epstein-Barr
virus infection. Mod Pathol. 7:91–98. 1994.PubMed/NCBI
|
|
16
|
Iwakiri D and Takada K: Role of EBERs in
the pathogenesis of EBV infection. Adv Cancer Res. 107:119–136.
2010. View Article : Google Scholar : PubMed/NCBI
|