Introduction
The hedgehog signaling pathway plays a pivotal role
in embryogenesis and is involved in the regulation of cell growth
and differentiation (1). There are 3
hedgehog ligands, among which sonic hedgehog (Shh) is the best
characterized. The hedgehog pathway is activated by binding of one
of those 3 ligands to the receptor patched-1 (Ptch). Unbound Ptch
acts as a tumor suppressor that binds to and represses the
proto-oncoprotein smoothened (Smo), thereby preventing it from
activating downstream transcription factors, particularly the
glioma-associated oncogene homolog 1 (Gli1). Activation of hedgehog
signaling has been demonstrated to be a key factor in the
development and progression of a number of human malignancies,
including skin, brain and gastrointestinal cancers (2). The malignancies in which hedgehog
signaling has been implicated also include hepatocellular carcinoma
(HCC) (3,4).
With >700,000 newly diagnosed cases annually, HCC
represents a major global health burden (5–7). In
carefully selected patients, liver transplantation (LT) represents
the most effective treatment for HCC (8,9).
Currently, criteria based on the number and size of HCC lesions are
used to select HCC patients for LT, referred to as Milan criteria.
However, a significant shortcoming of these criteria is defining
the risk of HCC recurrence following LT based on tumor morphology
rather than biology. In a study from our institution, we
demonstrated that using HCC volume as a static value inaccurately
reflects HCC tumor behavior (10).
Indeed, among patients with a tumor burden beyond the currently
adopted Milan criteria, there is a subset with favorable tumor
biology that may have positive outcomes if transplanted.
Combining novel tumor biomarkers with conventional
clinical indicators of prognosis should more accurately predict HCC
patient outcomes, enabling more appropriate therapeutic decisions.
The aim of this study was to investigate the tissue expression
patterns of Shh biomarkers in HCC and associate their expression
with the risk of HCC recurrence following LT.
Patients and methods
Study population
Adult patients diagnosed with stage T2 HCC who
underwent LT from cadaveric donors at the Cleveland Clinic between
January 1, 2002 and December 31, 2006 were randomly selected for
analysis. Demographic patient data, including underlying liver
disease (hepatitis B and/or C virus infection, alcoholic liver
disease and non-alcoholic steatohepatitis), laboratory values,
post-LT immunosuppression regimen, imaging studies and liver
explant pathology reports, were extracted from the electronic
medical database. Pathological tissue specimens of HCCs and
surrounding non-tumorous liver tissue were retrieved from the
explanted livers. All the transplanted patients were regularly
monitored following LT under the Cleveland Clinic liver transplant
service protocols: CT or MRI scans of the chest, abdomen and pelvis
were performed every 3 months during the first year after LT, every
6 months during the second year, and yearly thereafter. HCC
recurrence following LT was defined as months from LT to event or
censoring. The subjects were censored at the time of
re-transplantation or last follow-up. The patients were then
grouped according to HCC recurrence following LT.
Immunohistochemical analysis
Routine immunohistochemistry was used to evaluate
the different hedgehog pathway proteins in explanted liver tissue
(in tumor as well as in the surrounding non-tumorous liver
parenchyma). Briefly, paraffin-embedded tissue sections were
deparaffinized, using SAFE-CLEAR Clearant (EK Industries, Inc.,
Joliet, IL, USA), which is a xylene substitute, as the tissue
clearing agent. Ethanol hydration and serial dilution were
performed, followed by phosphate-buffered saline (PBS) washout.
Diluted sodium citrate buffer was then used to heat the specimens.
After cooling, donkey serum (10%) was added for 30 min, followed by
overnight incubation at 4°C with primary antibodies targeting Shh,
Ptch and Gli1; these were goat polyclonal anti-Shh antibody
(dilution, 1:100; N-19, sc-1194), rabbit polyclonal anti-Ptch
antibody (dilution, 1:200; H-267, sc-9016) and goat polyclonal
anti-Gli1 antibody (dilution, 1:100; N-16, sc-6153), all from Santa
Cruz Biotechnology, Inc., Dallas, TX, USA. Matched negative
controls were stained without the primary antibodies. PBS washout
was repeated, then secondary fluorescent antibodies were applied
for 60 min; these were donkey anti-goat IgG-CFL 488 (dilution,
1:100; sc-362255) or donkey anti-rabbit IgG-CFL 488 (dilution,
1:100; sc-362261), both from Santa Cruz Biotechnology, Inc. PBS and
then water washout were repeated. Finally, mounting was performed
with 4′,6-diamidino-2-phenylindole as the nuclear stain.
The presence and abundance of the three hedgehog
pathway proteins in all the specimens was evaluated using
computerized quantitative software analysis with the aid of an
experienced hepatopathologist. The tissue expression level of
hedgehog biomarkers in each HCC nodule was correlated with HCC
recurrence and disease-free survival following LT.
Statistical analysis
Continuous variables are expressed as mean ±
standard deviation and categorical variables as no. (%). Analysis
of variance was used to assess differences in tissue expression of
each Shh biomarker between HCC patients with and those without
tumor recurrence following LT. In addition, a time-to-event
analysis was performed to assess whether any of the hedgehog
biomarkers was associated with the risk of recurrence of HCC
following LT. A P-value of <0.05 was considered to indicate
statistically significant differences. All analyses were performed
with SAS software, version 9.3 (SAS Institute, Cary, NC, USA) and R
software, version 3.0.2 (R Foundation for Statistical Computing,
Vienna, Austria).
Results
Expression of Shh, Ptch and Gli1
proteins in HCC samples
A total of 53 tissue samples from 21 patients were
included in the analysis. The tissue samples included HCC nodules
(n=32) and surrounding non-tumorous cirrhotic liver (n=21). The
mean age of the patients was 57±8 years, 86% of the patients were
male, 86% were Caucasian and their mean calculated model for
end-stage liver disease (MELD) score was 15. A total of 62% of the
patients had hepatitis C virus infection, 14% had hepatitis B virus
infection and 43% had alcoholic cirrhosis (a proportion of the
patients had multiple underlying liver diseases). A total of 91% of
the patients had HCCs within the Milan criteria at the time of LT
based on radiological assessment, while all the tumors were
eventually determined to be within the Milan criteria based on
pathological examination following transplantation. The average
follow-up time after LT was 36±15 months, during which 19% of the
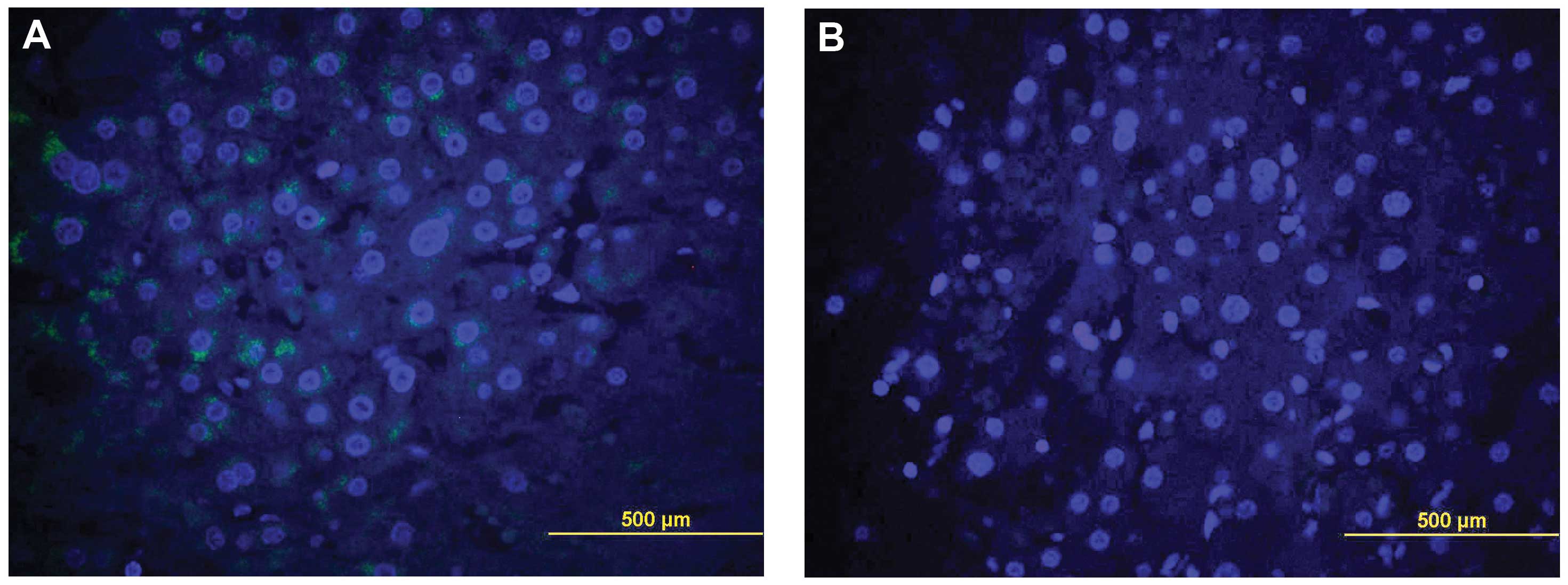
patients developed recurrence of HCC and 29% died (Table I). Shh, Ptch and Gli1 were detected in
the liver tissues of all the patients, within the tumor itself, as
well as in the surrounding non-tumorous cirrhotic tissues (Fig. 1). Ptch was overexpressed in HCC
compared with the surrounding non-tumorous liver tissue.
 | Table I.Patient characteristics (n=21). |
Table I.
Patient characteristics (n=21).
| Variables | Values |
|---|
| Age (years) | 56.6±8.0 |
| Male | 18 (85.7) |
| BMI
(kg/m2) | 31.6±4.0 |
| Caucasian | 18 (85.7) |
| Hepatitis C virus
infection | 13 (61.9) |
| Hepatitis B virus
infection | 3 (14.3) |
| Alcoholic liver
disease | 9 (42.9) |
| Non-alcoholic
steatohepatitis | 1 (4.8) |
| Pre-LT
α-fetoprotein | 85.7±179.5 |
| Radiology, number of
nodules |
|
| 0 | 5 (23.8) |
| 1 | 9 (42.9) |
| 2+ | 7 (33.3) |
| Radiology, within
Milan criteria | 19 (90.5) |
| Radiology, within
UCSF criteria | 20 (95.2) |
| Pathology, number of
nodules |
|
| 1 | 14 (66.7) |
| 2+ | 7 (33.3) |
| Pathology, within
Milan criteria | 21 (100.0) |
| Microvascular
invasion | 6 (28.6) |
| Grade |
|
|
Well-differentiated | 9 (42.9) |
|
Moderately-poorly
differentiated | 12 (57.1) |
| Biochemical MELD at
the time of LT | 15.4±5.6 |
| Shh expression
level |
|
|
Tumor | 126.2±30.2 |
| Cirrhotic
tissue | 130.7±32.4 |
| Gli1 expression
level |
|
|
Tumor | 5.6±0.88 |
| Cirrhotic
tissue | 5.8±0.93 |
| Ptch expression
level |
|
|
Tumor | 7.0±0.90 |
| Cirrhotic
tissue | 6.6±1.3 |
| Post-LT follow-up
(months) | 36.2±14.6 |
| HCC recurrence | 4 (19.0) |
| Deceased | 6 (28.6) |
Association of Shh, Ptch and Gli1
expression with HCC recurrence following LT
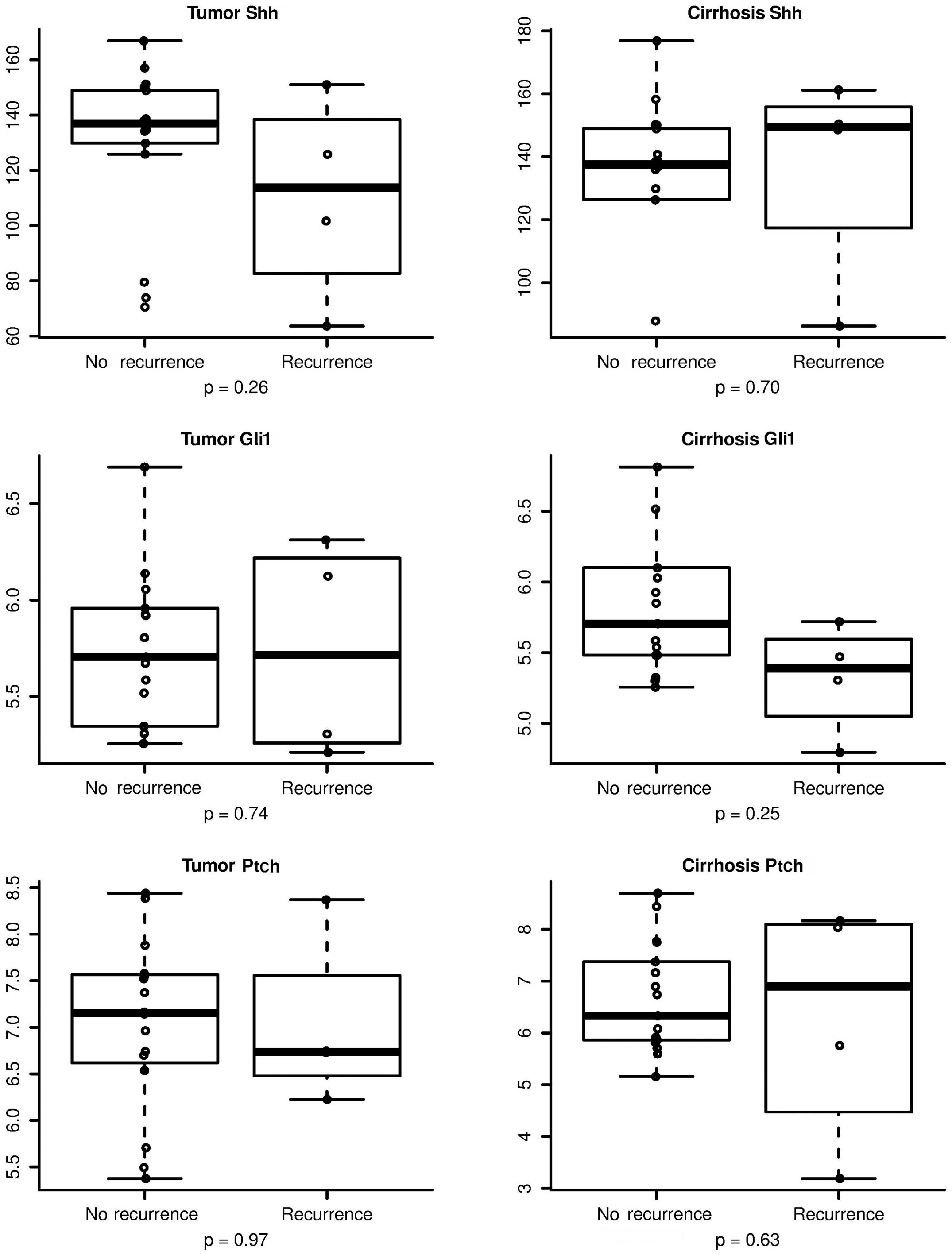
There was no evidence suggesting that any of the
hedgehog biomarkers was significantly associated with HCC
recurrence following LT (Fig. 2).
However, the time-to-event analysis demonstrated a trend toward
statistical significance for correlating Shh levels with HCC
recurrence following LT. These data indicate that a larger sample
size to enhance statistical power is required to confirm the HCC
recurrence results. Based on recurrence of HCC following LT,
Table II shows the association of
HCC recurrence with each hedgehog biomarker and Table III summarizes the hazard ratio of
HCC recurrence based on the expression of the hedgehog
biomarkers.
| Table II.Association of HCC recurrence with Shh
biomarkers. |
Table II.
Association of HCC recurrence with Shh
biomarkers.
| Biomarkers | No HCC recurrence
(tissue samples, n=42; patients, n=17) | HCC recurrence
(tissue samples, n=11; patients, n=4) | P-value |
|---|
| Shh |
|
|
|
|
Tumor | 129.9±28.4 | 110.5±37.2 | 0.26 |
| Cirrhotic
tissue | 129.3±32.9 | 136.6±34.1 | 0.70 |
| Gli1 |
|
|
|
|
Tumor |
5.6±0.95 |
5.7±0.56 | 0.74 |
| Cirrhotic
tissue |
5.9±0.99 |
5.3±0.39 | 0.25 |
| Ptch |
|
|
|
|
Tumor |
7.0±0.92 |
7.0±0.93 | 0.97 |
| Cirrhotic
tissue |
6.7±1.06 |
6.3±2.3 | 0.63 |
| Table III.Univariable Cox regression analysis of
the association between Shh biomarkers and HCC recurrence. |
Table III.
Univariable Cox regression analysis of
the association between Shh biomarkers and HCC recurrence.
| Biomarkers | Hazard ratio (95%
CI) | P-value |
|---|
| Shh |
|
|
|
Tumor |
0.98
(0.95–1.01) | 0.16 |
| Cirrhotic
tissue |
1.01
(0.97–1.05) | 0.64 |
| Gli-1 |
|
|
|
Tumor | 1.2 (0.35–3.9) | 0.82 |
| Cirrhotic
tissue | 0.49
(0.16–1.5) | 0.22 |
| Ptch |
|
|
|
Tumor | 0.79
(0.25–2.5) | 0.69 |
| Cirrhotic
tissue | 0.68
(0.32–1.5) | 0.34 |
Discussion
LT is currently the standard of care for HCC
patients with stage T2 tumors. The United Network for Organ Sharing
has adopted the restrictive Milan criteria to select patients with
HCC for LT. Based on preoperative imaging, the Milan criteria limit
LT to patients with a solitary HCC tumor <5.0 cm in diameter, or
2–3 HCC tumors <3.0 cm each. The 4-year survival rate of HCC
patients with tumors within the Milan criteria is ~85% following LT
(11). However, a serious
complication of LT for HCC is tumor recurrence. Even within the
Milan criteria, HCC recurrence rates following LT have been found
to be as high as 15% (12,13). In an era of organ shortage, organ
allocation policies are crucial to avoid graft misutilization.
Subsequently, tumor biomarkers that help characterize HCC biology
are sought to determine the most convenient therapeutic options for
these patients.
In this study, we evaluated the tissue expression of
several components within the hedgehog pathway in HCC tumors, and
attempted to determine whether the level of tissue expression
correlates with the aggressiveness of tumor behavior in terms of
tumor recurrence following LT. The hedgehog pathway is a highly
preserved cellular signaling pathway involved in the regulation of
cell differentiation, tissue polarity and cell proliferation
(14). This pathway has been
evaluated in the initiation and progression of several skin and
gastrointestinal malignancies, such as esophageal and gastric
cancer (15). It has been also shown
to lead to adverse outcomes in patients with HCC, including
increased risk of tumor recurrence following surgical resection,
and the increased expression of Gli1 has been suggested to be
associated with poor prognosis in HCC (4). More recently, components of the hedgehog
pathway have been targeted by specific inhibitors. For example,
vismodegib, an inhibitor of the smoothened receptor, was the first
hedgehog signaling pathway targeting agent to be approved by the
Food and Drug Administration in early 2012 for the treatment of
basal-cell carcinoma (16).
We documented the expression of Shh, Ptch and Gli1
proteins in human HCC and adjacent non-tumorous liver tissue by
immunohistochemistry. Our results demonstrated that, among the Shh
biomarkers, the expression level of Ptch was significantly higher
in HCC compared with that in adjacent non-tumorous liver tissue. We
observed a tendency for correlation of the level of Shh biomarker
tissue expression in HCC with the recurrence rate following LT;
however, this did not reach statistical significance. Those results
may be used to perform power analysis calculations in future
studies. While prior studies evaluated the association between Shh
biomarkers and HCC recurrence following surgical resection
(4,17), to the best of our knowledge, this
study is the first to report on correlating tissue expression of
Shh biomarkers with HCC recurrence following LT.
There has been recent debate regarding the selection
of HCC patients for LT, with arguments that the Milan criteria are
too restrictive and that the selection criteria may be expanded
without increasing the rate of HCC recurrence or compromising
survival outcomes following LT. We consider that we may have more
success in expanding the current LT selection criteria for HCC on
the basis of the biological behavior of the tumor, rather than
adjusting the number and size of tumors allowed. Several tumor
biological factors such as DNA aneuploidy, high tumor cell
proliferation index, high telomerase activity and mutation of the
p53 gene, have been associated with increased risk of
post-resection HCC recurrence (18–22).
However, the prognostic impact of these factors remains uncertain
following LT for HCC. Combining biomarkers that reflect tumor
biology, such as hedgehog proteins, with clinical indicators of
prognosis, such as the Milan criteria, is likely to more accurately
predict HCC patient outcomes.
In conclusion, this proof-of-concept study has
demonstrated higher levels of tissue expression of Ptch, among
other Shh biomarkers, within HCC tumor compared with the
surrounding non-tumorous liver tissue. The small sample size did
not allow demonstrating an association between Shh biomarkers and
HCC recurrence following LT. Further larger studies are required to
assess the prognostic value of these biomarkers in HCC patients to
fully elucidate their potential use in clinical practice. The
present study is hypothesis-generating and further prospective
analysis should be performed.
Acknowledgements
The present study was supported in part by the
Mikati Foundation Endowed Chair in Liver Diseases (to Nizar
Zein).
References
|
1
|
Shahi MH, Rey JA and Castresana JS: The
sonic hedgehog-GLI1 signaling pathway in brain tumor development.
Expert Opin Ther Targets. 16:1227–1238. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Parkin CA and Ingham PW: The adventures of
sonic hedgehog in development and repair. I. Hedgehog signaling in
gastrointestinal development and disease. Am J Physiol Gastrointest
Liver Physiol. 294:G363–G367. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jeng KS, Sheen IS, Jeng WJ, Lin CC, Lin
CK, Su JC, Yu MC and Fang HY: High expression of patched homolog-1
messenger RNA and glioma-associated oncogene-1 messenger RNA of
sonic hedgehog signaling pathway indicates a risk of postresection
recurrence of hepatocellular carcinoma. Ann Surg Oncol. 20:464–473.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Che L, Yuan YH, Jia J and Ren J:
Activation of sonic hedgehog signaling pathway is an independent
potential prognosis predictor in human hepatocellular carcinoma
patients. Chin J Cancer Res. 24:323–331. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
El-Serag HB and Rudolph KL: Hepatocellular
carcinoma: Epidemiology and molecular carcinogenesis.
Gastroenterology. 132:2557–2576. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
El-Serag HB and Mason AC: Rising incidence
of hepatocellular carcinoma in the United States. N Engl J Med.
340:745–750. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Llovet JM, Burroughs A and Bruix J:
Hepatocellular carcinoma. Lancet. 362:1907–1917. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bruix J and Sherman M: Practice Guidelines
Committee, American Association for the Study of Liver Diseases:
Management of hepatocellular carcinoma. Hepatology. 42:1208–1236.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Macaron C, Hanouneh IA, Lopez R, Aucejo F
and Zein NN: Total tumor volume predicts recurrence of
hepatocellular carcinoma after liver transplantation in patients
beyond Milan or UCSF criteria. Transplant Proc. 42:4585–4592. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mazzaferro V, Regalia E, Doci R, Andreola
S, Pulvirenti A, Bozzetti F, Montalto F, Ammatuna M, Morabito A and
Gennari L: Liver transplantation for the treatment of small
hepatocellular carcinomas in patients with cirrhosis. N Engl J Med.
334:693–699. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Toso C, Trotter J, Wei A, Bigam DL, Shah
S, Lancaster J, Grant DR, Greig PD, Shapiro AM and Kneteman NM:
Total tumor volume predicts risk of recurrence following liver
transplantation in patients with hepatocellular carcinoma. Liver
Transpl. 14:1107–1115. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Klintmalm GB: Liver transplantation for
hepatocellular carcinoma: A registry report of the impact of tumor
characteristics on outcome. Ann Surg. 228:479–490. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ingham PW and McMahon AP: Hedgehog
signaling in animal development: Paradigms and principles. Genes
Dev. 15:3059–3087. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Berman DM, Karhadkar SS, Maitra A, De
Montes Oca R, Gerstenblith MR, Briggs K, Parker AR, Shimada Y,
Eshleman JR, Watkins DN, et al: Widespread requirement for Hedgehog
ligand stimulation in growth of digestive tract tumours. Nature.
425:846–851. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sekulic A, Migden MR, Oro AE, Dirix L,
Lewis KD, Hainsworth JD, Solomon JA, Yoo S, Arron ST, Friedlander
PA, et al: Efficacy and safety of vismodegib in advanced basal-cell
carcinoma. N Engl J Med. 366:2171–2179. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zheng X, Yao Y, Xu Q, Tu K and Liu Q:
Evaluation of glioma-associated oncogene 1 expression and its
correlation with the expression of sonic hedgehog, E-cadherin and
S100a4 in human hepatocellular carcinoma. Mol Med Rep. 3:965–970.
2010.PubMed/NCBI
|
|
18
|
Poon Tung-Ping R, Fan ST and Wong J: Risk
factors, prevention, and management of postoperative recurrence
after resection of hepatocellular carcinoma. Ann Surg. 232:10–24.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chiu JH, Kao HL, Wu LH, Chang HM and Lui
WY: Prediction of relapse or survival after resection in human
hepatomas by DNA flow cytometry. J Clin Invest. 89:539–545. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ng IO, Lai EC, Fan ST, Ng M, Chan AS and
So MK: Prognostic significance of proliferating cell nuclear
antigen expression in hepatocellular carcinoma. Cancer.
73:2268–2274. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Suda T, Isokawa O, Aoyagi Y, Nomoto M,
Tsukada K, Shimizu T, Suzuki Y, Naito A, Igarashi H, Yanagi M, et
al: Quantitation of telomerase activity in hepatocellular
carcinoma: A possible aid for a prediction of recurrent diseases in
the remnant liver. Hepatology. 27:402–406. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hayashi H, Sugio K, Matsumata T, Adachi E,
Takenaka K and Sugimachi K: The clinical significance of p53 gene
mutation in hepatocellular carcinomas from Japan. Hepatology.
22:1702–1707. 1995. View Article : Google Scholar : PubMed/NCBI
|