Introduction
Serous cystadenoma of pancreas (SCA) is a benign
epithelial neoplasm of uncertain origin. Immunohistochemical and
ultrastructural studies have suggested that SCA may originate from
centroacinar or intercalated duct cells. It can occur in any region
of the pancreas, predominantly in older females (1). According to the literature, the majority
of SCAs are small (<1 cm) and are identified incidentally.
Grossly, SAC is a well-circumscribed mass within numerous small
cysts (‘honeycomb’ appearance) on cut surface with a central
fibrotic scar. Histologically, majority of SACs are ‘microcystic’
with numerous cysts exhibiting a diameter <2 cm and rarely with
calcification in the fibrous septa. Lesions with a diameter >2
cm were defined as macrocystic serous cystadenoma (2,3). The
cystic fluid is watery clear or straw-colored without mucin
production. The cysts are lined by low cuboidal cells with clear to
eosinophilic cytoplasm without cytological atypia. Clear cytoplasm
is caused by rich glycogen that is positive for PAS stain.
Microcystic SCA has been associated with von Hippel-Lindau gene
mutations. The present study reported a classical microcytic serous
cystadenoma of the pancreas with atypical clinical
manifestations.
Case report
A 60 year-old female with a history of hypertension
and cerebral infarction presented with recurrent bilateral lower
back discomfort for 3 months. The lower back discomfort was not
associated with jaundice or weight loss. The patient had no
significant family history of cancer and had not been previously
admitted for these symptoms. An abdominal ultrasonography revealed
multiple pancreatic cysts and liver cysts. Serum amylase and cancer
biomarkers, including cancer antigen (CA)19-9, carcinoembryonic
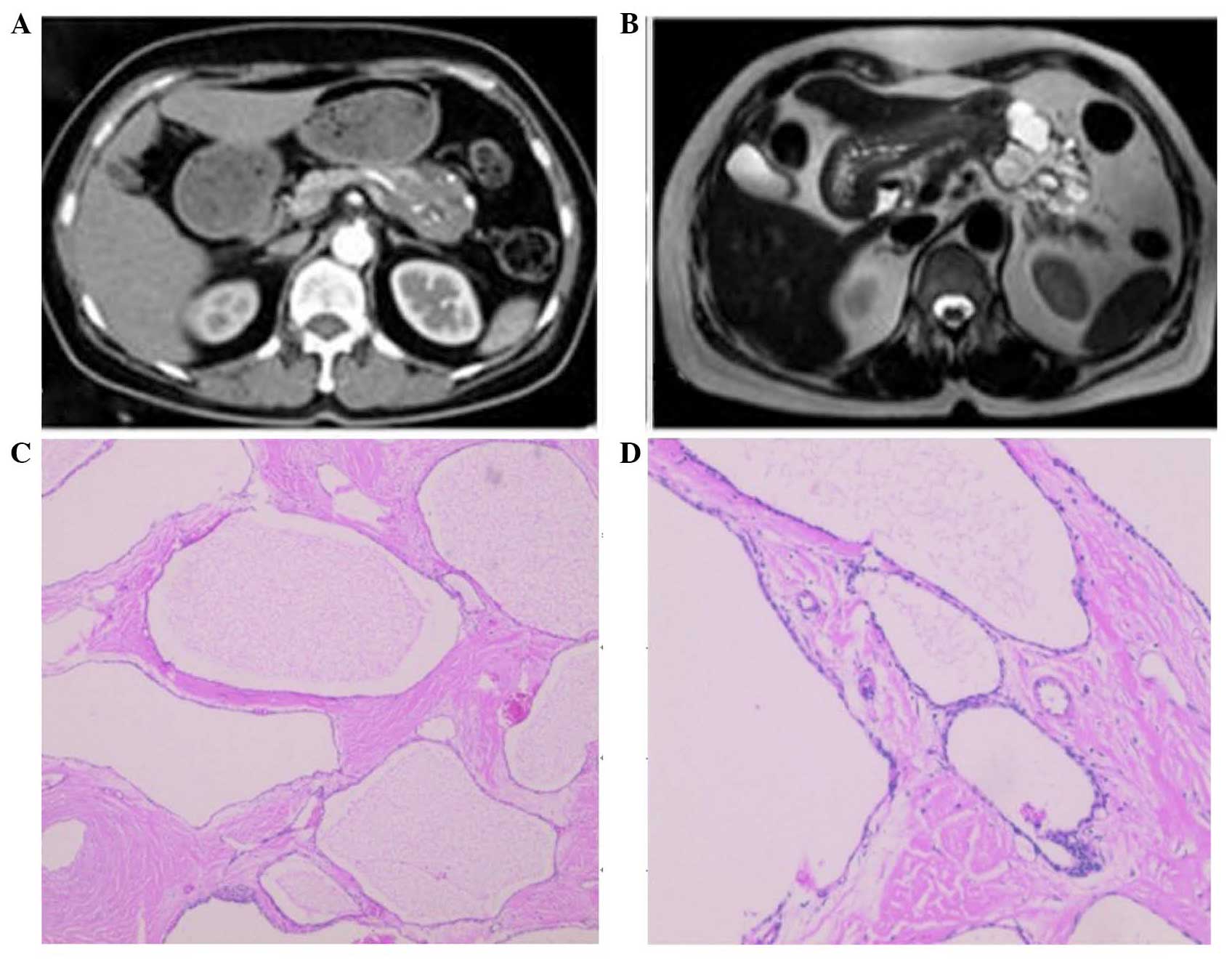
antigen (CEA) and CA125, were within normal range. A multiphasic
contrast-enhanced computed tomography (CT) scan revealed a 4.8 cm
cystic solid mass with unequal moderate enhancement and multiple
calcification foci in the pancreatic body (Fig. 1A). Furthermore, magnetic resonance
imaging (MRI) revealed a similar cystic solid mass in the
pancreatic body without dilatation of the pancreatic duct (Fig. 1B). Combined with the imaging data, a
clinical impression of solid-pseudopapillary neoplasms was created.
An abdominal exploration was performed and revealed splenic vessels
encased by the mass, similar to invasion observed in malignant
tumors. Distal pancreatectomy with splenectomy was subsequently
performed. The patient's postoperative course was uneventful and
she was discharged 15 days after the surgery. Grossly, the tumor
was firm and consisted of numerous small cysts on cut surface with
a central fibrotic scar. Histopathological examination of the
cystic solid mass revealed classical features of microcytic serous
cystadenoma of the pancreas with septa centrally coalesced into a
‘stellate scar’ with calcification and encasing the splenic vessels
(Fig. 1C and D).
Discussion
Serous cystadenoma of the pancreas was first
described by Compagno and Oertel in 1978 (1). Morphological features include numerous
cysts with variable diameter lined by a single layer of cuboidal
epithelium producing watery fluid similar to serum. SCA occurs most
frequently in females ranging between 56 and 62 years of age
(4,5).
SCA can occur in any section of the pancreas, although
predominantly in the head and body region (6). SCA is associated with von Hippel-Lindau
disease and can have diffuse and multiple lesions over the entire
pancreas at a younger age in this setting (7). CT and MRI are the most common diagnostic
methods for SCA. CT and MRI imaging of SCA typically reveals a
lobulated contour, uneven low density, thin wall/capsule and
absence of wall enhancement. Atypical imaging features include
multiple septations, wall enhancement and/or calcification, wall
thickness, and presence of mural nodules or papillary projections
(2). However, these features cannot
differentiate SCA from other pancreatic cystic tumors.
Approximately 60% of the SCAs can be diagnosed by CT and/or MRI.
When imaging features reported by CT and/or MRI are insufficient to
differentiate cystic lesions, endoscopic ultrasonography (EUS) with
or without EUS-guided fine-needle aspiration (FNA) can provide
additional and useful information, and notably improves the
sensitivity of diagnosis for SCA to 76% (8). Although EUS with FNA increases the
detection rate of SCA, FNA is somehow limited due to a high rate of
insufficient sampling and potential tumor seeding of the needle
tract for cases when malignancy cannot be ruled out. Serum CEA and
CA19.9 are non-specific biomarkers for pancreatic lesions.
Almost all SCAs are benign and to date, no patient
has succumbed to SCA or associated reasons (9,10).
Therefore, surgical resection for serous cystic neoplasms should be
limited to those with clinical symptoms and large tumor size. A
previous study indicated that a tumor >6 cm is the cornerstone
for operation (11). Based on our
experience, the present study suggested that asymptomatic patients
with a small lesion (<4 cm) require imaging surveillance every 2
years. However, tumors >4 cm require surgical resection, since
these tumors are more frequently symptomatic and faster growing
(12). When multiphasic contrast
enhanced CT scan and MRI imaging studies reveal a low diagnostic
power to differentiate SCA from mucinous cystic neoplasm and
intraductal papillary mucinous neoplasm, early surgical treatment
must be taken into account with growing experience and advanced
surgical techniques.
Surgical resection is considered curative for SCA.
The location of SCA in the pancreas determines the method of
resection, which is used. The appropriate methods for this case
include distal pancreatectomy with spleen-preserving or with
splenectomy. Spleen-preserving distal pancreatectomy includes the
Warshaw procedure, which conserves the spleen by blood flow from
the short gastric vessels and the Kimura procedure, which preserves
the spleen with splenic vessels (13). Since the Warshaw procedure has a high
incidence of complications and subsequent splenectomies, distal
pancreatectomy with splenectomy is often required, particularly
when the splenic vessels are encased by SCA, as in this case.
Therefore, when no recurrence is observed following radical
surgery, post-operation follow-up is unnecessary in these
patients.
In the previous decade, non-surgical management for
patients with SCA is rising. EUS-guided treatment has been
reported, particularly for patients unfit for surgery. Cyst
ablation with the injection of ethanol followed by paclitaxel was
considered as another promising technique and has revealed complete
resolution in certain patients, although long-term follow-up is
still required (14,15).
In conclusion, with the most recent imaging
techniques, a large proportion of patients with SCA cannot be
definitively diagnosed prior to operation, particularly with
atypical imaging findings. Although SCA is a benign pancreatic
cystic neoplasm, the patient can be symptomatic, particularly when
the cyst is >4 cm and surgical treatment is particularly
important to manage these patients.
References
|
1
|
Compagno J and Oertel JE: Microcystic
adenomas of the pancreas (glycogen-rich cystadenomas): A
clinicopathologic study of 34 cases. Am J Clin Pathol. 69:289–298.
1978. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Choi JY, Kim MJ, Lee JY, Lim JS, Chung JJ,
Kim KW and Yoo HS: Typical and atypical manifestations of serous
cystadenoma of the pancreas: Imaging findings with pathologic
correlation. AJR Am J Roentgenol. 193:136–142. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kehagias D, Smyrniotis V, Gouliamos A and
Vlahos L: Cystic pancreatic neoplasms: Computed tomography and
magnetic resonance imaging findings. Int J Pancreatol. 28:223–230.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Galanis C, Zamani A, Cameron JL, Campbell
KA, Lillemoe KD, Caparrelli D, Chang D, Hruban RH and Yeo CJ:
Resected serous cystic neoplasms of the pancreas: A review of 158
patients with recommendations for treatment. J Gastrointest Surg.
11:820–826. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bassi C, Salvia R, Molinari E, Biasutti C,
Falconi M and Pederzoli P: Management of 100 consecutive cases of
pancreatic serous cystadenoma: Wait for symptoms and see at imaging
or vice versa? World J Surg. 27:319–323. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kimura W, Moriya T, Hirai I, Hanada K, Abe
H, Yanagisawa A, Fukushima N, Ohike N, Shimizu M, Hatori T, et al:
Multicenter study of serous cystic neoplasm of the Japan pancreas
society. Pancreas. 41:380–387. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Charlesworth M, Verbeke CS, Falk GA, Walsh
M, Smith AM and Morris-Stiff G: Pancreatic lesions in von
hippel-lindau disease? A systematic review and meta-synthesis of
the literature. J Gastrointest Surg. 16:1422–1428. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khashab MA, Kim K, Lennon AM, Shin EJ,
Tignor AS, Amateau SK, Singh VK, Wolfgang CL, Hruban RH and Canto
MI: Should we do EUS/FNA on patients with pancreatic cysts? The
incremental diagnostic yield of EUS over CT/MRI for prediction of
cystic neoplasms. Pancreas. 42:717–721. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Malleo G, Bassi C and Salvia R: Appraisal
of the surgical management for pancreatic serous cystic neoplasms.
Surg Endosc. 27:2646–2647. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Abe H, Kubota K, Mori M, Miki K, Minagawa
M, Noie T, Kimura W and Makuuchi M: Serous cystadenoma of the
pancreas with invasive growth: Benign or malignant? Am J
Gastroenterol. 93:1963–1966. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pravisani R, Intini SG, Girometti R,
Avellini C, Leo CA, Bugiantella W and Risaliti A: Macrocystic
serous cystadenoma of the pancreas: Report of 4 cases. Int J Surg.
21:S98–S101. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tseng JF, Warshaw AL, Sahani DV, Lauwers
GY, Rattner DW and Fernandez-del Castillo C: Serous cystadenoma of
the pancreas: Tumor growth rates and recommendations for treatment.
Ann Surg. 242:413–419. 2005.PubMed/NCBI
|
|
13
|
Dina I, Ginghina O, Iacobescu C, Vrabie C,
Gidea C, Munteanu R, Iosifescu R and Iordache N: Spleen
preservation in a caudal pancreatic serous cystadenoma-case report.
J Med Life. 8:106–108. 2015.PubMed/NCBI
|
|
14
|
Oh HC, Seo DW, Kim SH, Min B and Kim J:
Systemic effect of endoscopic ultrasonography-guided pancreatic
cyst ablation with ethanol and paclitaxel. Dig Dis Sci.
59:1573–1577. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Oh HC, Seo DW, Song TJ, Moon SH, Park Do
H, Lee Soo S, Lee SK, Kim MH and Kim J: Endoscopic
ultrasonography-guided ethanol lavage with paclitaxel injection
treats patients with pancreatic cysts. Gastroenterology.
140:172–179. 2011. View Article : Google Scholar : PubMed/NCBI
|