Introduction
Breast cancer (BC) is the most frequently diagnosed
type of cancer and the leading cause of cancer-associated mortality
in women worldwide (1). The molecular
profiling of BC, based on gene expression, is useful to
characterize this heterogeneous disease. The molecular subtypes of
BC provide important predictive and prognostic information. BC can
be classified into human epidermal growth factor receptor
(HER)2-positive/enriched, hormone-receptor (estrogen and/or
progesterone) positive (luminal), positive for both (luminal HER2)
or triple negative BC (negative for estrogen and progesteron
receptors, and HER2) (2). The
treatment strategy for metastatic BC is designed according to a
several factors, including the performance status, site of
metastasis and the molecular subtype of the disease (3). The present report described a case of
gastric metastasis from BC, which showed repeated changes of the
molecular subtype, making it difficult to select the appropriate
treatments.
Case report
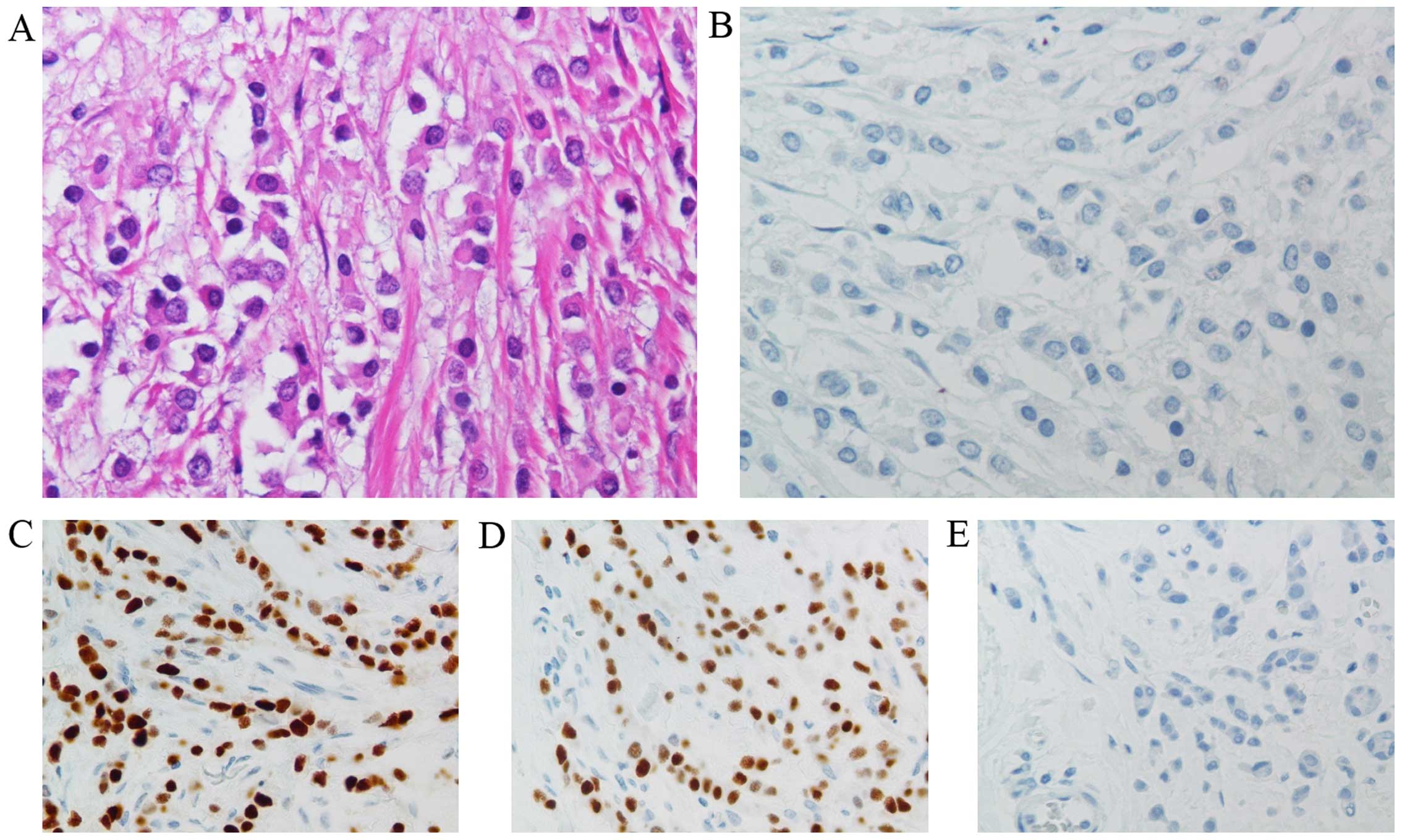
A 42-year-old woman underwent a mastectomy with
axillary lymph node dissection for the left BC in August 2006. The
primary tumor was pathologically diagnosed as invasive lobular
carcinoma (Fig. 1A and B), 4.5 cm in
diameter, and lymph node metastasis was observed in 37/51 harvested
nodes. The disease was stage IIIC, according to the UICC Tumor Node
Metastasis (TNM) classification for BC (T3 N3 M0) (4). Immunohistochemical examinations revealed
that the hormone receptors were positive, while HER2 status was
negative (Fig. 1C–E). At 2 months
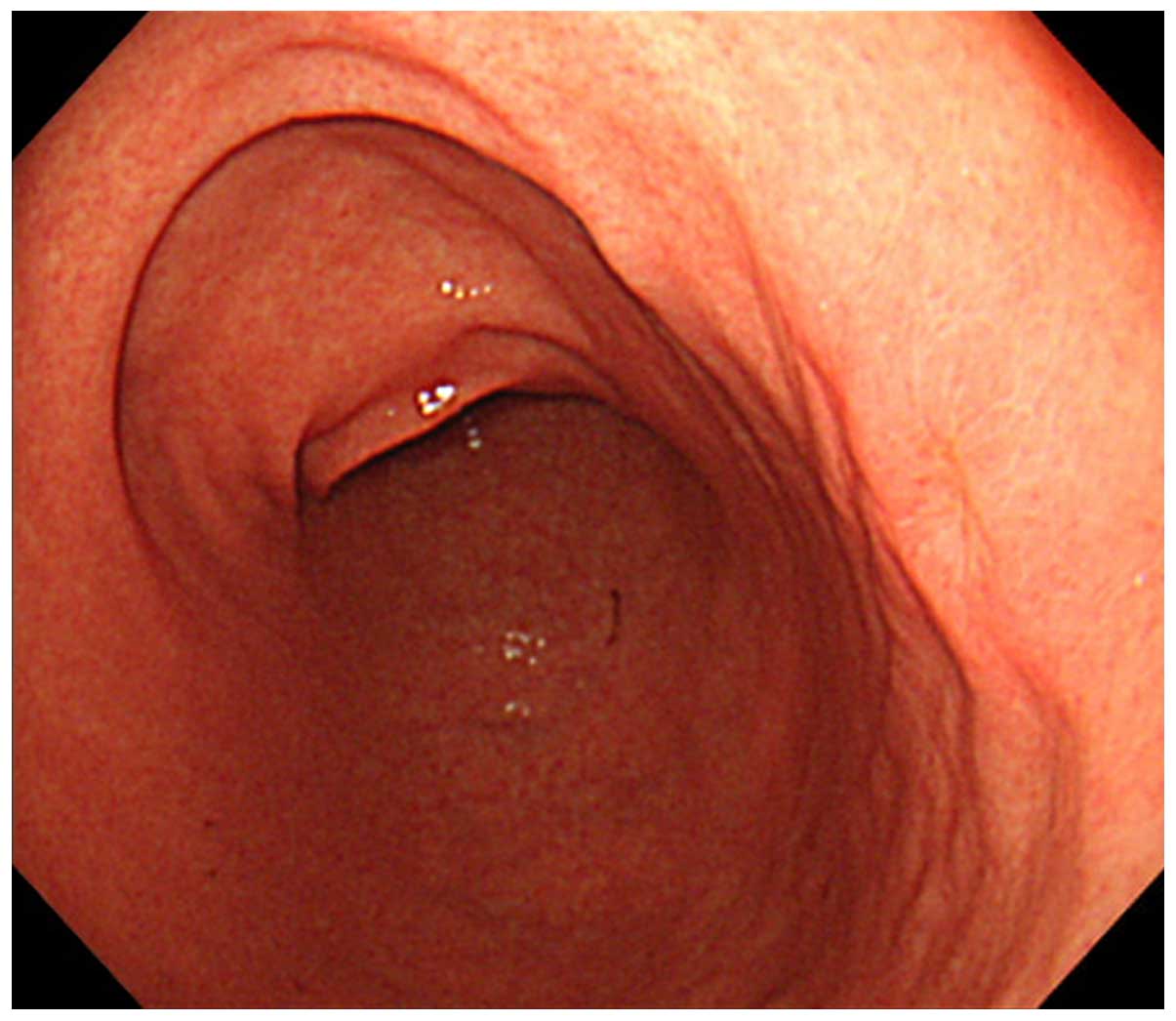
following the operation, the patient underwent an endoscopic
examination for a complaint of an epigastric pain, which occurred
during the postoperative adjuvant chemotherapy. The gastroscopy
revealed an erosive lesion at the posterior wall of the gastric
body (Fig. 2). A biopsy specimen
obtained from the gastric lesion contained lobular carcinoma, which
was morphologically similar to signet ring cell carcinoma, as
frequently exhibited in primary gastric cancer. The
immunohistochemical examinations (Fig.
3A) revealed positive staining for hormone receptors,
mammaglobin and gross cystic disease fluid protein (GCDFP)-15,
which was similar to the findings observed in the primary BC
lesion. These findings suggested that the gastric lesion was a
metastatic disease from the BC.
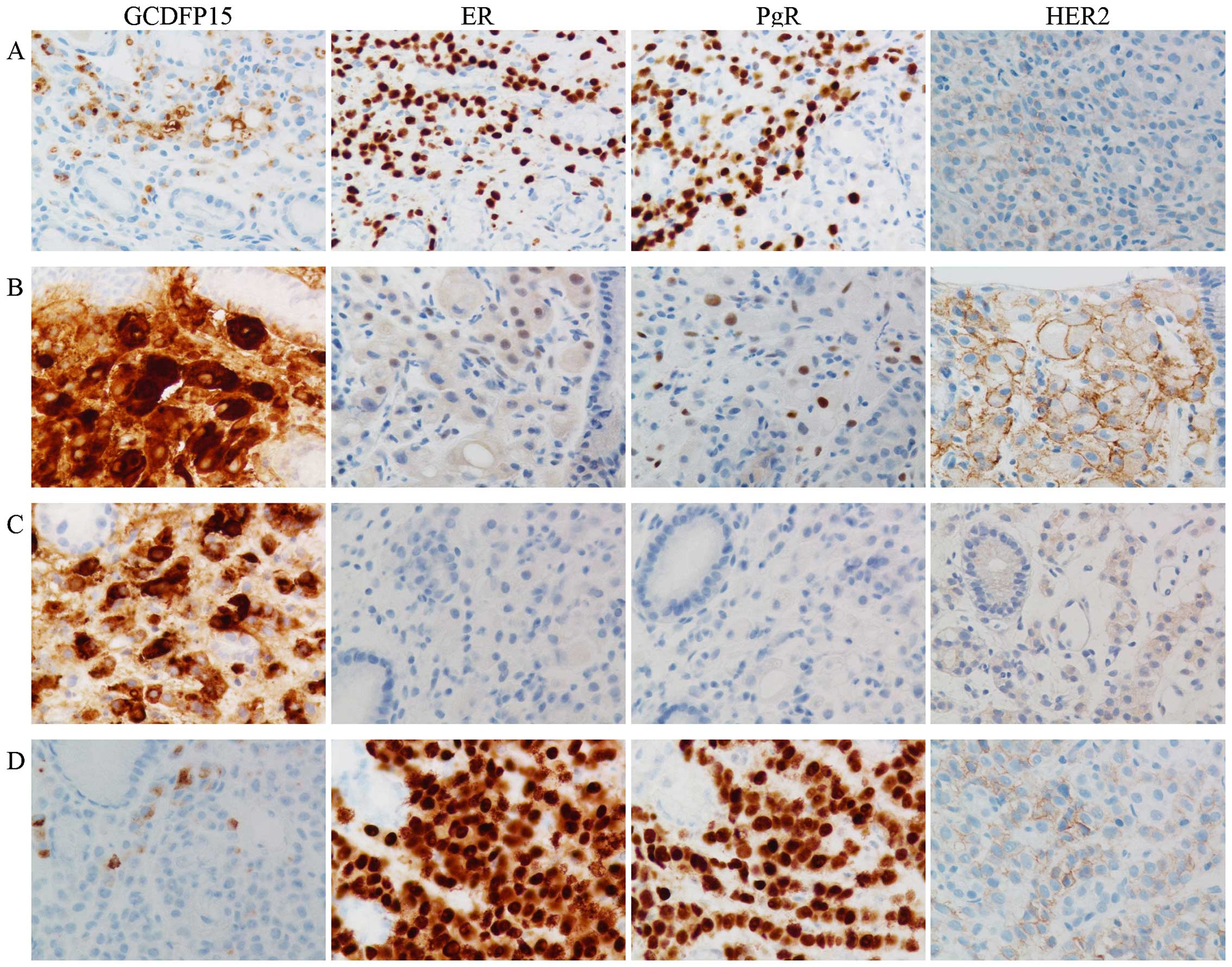 | Figure 3.IHC of the biopsy specimens obtained
from the gastric lesions. (A) IHC series in October 2006. Focally
positive for GCDFP15 staining was observed. ER and PgR were
markedly expressed and HER2 staining status was negative (HER2
score, 1+). (B) IHC series in March 2009. Cancer cells exhibited
markedly positive staining for GCDFP15. Hormone receptors were
focally positive and HER2 staining status was positive (HER2 score,
3+). (C) IHC series in July 2012. Cancer cells exhibited marked
staining of GCFDP15 and the absence of ER, PgR and HER2 (HER2
score, 1+). (D) IHC series in December 2014. Focally positive for
GCDFP15 staining was observed. The staining status of hormone
receptors are diffusely positive for both ER and PgR. The staining
score of HER2 was 2+. HER2 scores were according to the American
Society of Clinical Oncology/College of American Pathologists
guidelines for HER2 testing. Magnification, ×400. IHC,
immunohistochemistry; PgR, progesterone receptor; HER, human
epidermal growth factor receptor; ER, estrogen receptor; GCDFP,
gross cystic disease fluid protein. |
The patient received hormone therapy using an
aromatase inhibitor following the completion of the adjuvant
chemotherapy. About 2 years later, in July 2008, the gastric lesion
disappeared successfully by the treatments described above.
However, the patient had to restart chemotherapy again in March
2009 due to a relapse of the disease at the fundus, angle and
antrum beside the previous body lesion on the stomach. In addition,
the molecular subtype of the relapsed lesions had changed to the
luminal HER2 type (Fig. 3B) from the
luminal type; therefore, chemotherapy, including trastuzumab, was
selected. Subsequently, in July 2012, as the molecular subtype of
the disease changed again to the triple negative type (Fig. 3C), the patient was administered
chemotherapy alone. Although she was treated with chemotherapy
until May 2014, the accumulating side effects of the treatment made
it difficult for her to receive any additional chemotherapy.
Surgical resection of the stomach was considered as a therapeutic
option since the recurrent disease had only been observed only in
the stomach for ~8 years. Laparoscopic total gastrectomy was
planned in July 2014; however, only an exploratory laparoscopy was
performed due to the disseminated disease on peritoneum in the
entire abdomen, which was not diagnosed preoperatively.
Chemotherapy was restarted following the operation and the
molecular subtype of the disease had changed into luminal type
(Fig. 3D) from the triple negative
type in December 2014.
A total of 8.5 years have passed since the
mastectomy and the patient is still receiving chemotherapy for the
gastric metastases and the peritoneal dissemination without
occurrence of any other novel lesion.
Discussion
The rate of gastrointestinal (GI) metastasis from BC
is considered to be <1% in the clinical setting (5,6), which is
markedly lower compared with the 8–35% observed in the autopsy
series (7,8). Therefore, GI metastasis from BC may
often be overlooked due to the lack of serious symptoms.
Furthermore, Borst and Ingold (6)
demonstrated that the rate of GI metastasis was significantly
higher in patients with invasive lobular carcinoma compared with
invasive ductal carcinoma (4.5 vs. 0.5%). Similar to the present
case, if the gastric lesion appears to be lobular carcinoma,
determining the primary site of disease is required for further
treatment planning. In such a case, immunohistochemical staining
for mammaglobin and GCDFP-15 are useful to distinguish between
primary gastric cancer and the metastatic disease from the BC
(9,10). Estrogen receptor (ER) and progesterone
receptor expression are observed in 32 and 12% of primary gastric
cancers, respectively, indicating that their specificity is low
(11–13). The treatment recommendation for
gastric metastases from BC is typically a systemic treatment based
on their molecular subtype; however, surgical intervention should
be limited to palliation or for certain cases of solitary
metastases (14).
The present case was initially treated with hormone
therapy following adjuvant chemotherapy. Both the original
molecular subtypes of the primary BC and gastric metastases were
the luminal type; therefore, treatment using an aromatase inhibitor
was selected. Although the metastatic lesions once disappeared, the
relapsed lesions were transformed into the luminal HER2 type. The
mechanisms contributing to hormone resistance are hypothesized to
include loss or modification of the ER expression, regulation of
alternative signal transduction pathways, altered expression of
specific microRNAs, changes in the balance of co-regulatory
proteins and genetic polymorphisms involved in tamoxifen metabolic
activity (15). In the present case,
the lesions initially negative for HER2 expression shifted to
positive expression. It was therefore suggested that activation of
the HER2 signaling pathway was the predominant mechanism underlying
the acquired resistance to hormone therapy. A recent study using a
mouse xenograft model also demonstrated that 3/26 (11%) tumors
originally negative for HER2 became amplified and/or overexpressed
upon the acquisition of hormone resistance (16). Furthermore, Yang et al
(17) reported that a HER2 status
shift was observed in 17/113 (15.0%) patients who received
neoadjuvant chemotherapy (NAC). Among this series, a gain of HER2
was observed in 8/17 patients. The molecular subtype of the patient
in the present report further changed to the triple negative type
from luminal HER2 type during the treatment. The loss of ER
expression is another mechanism associated with hormone resistance,
as described above. Whereas, the mechanisms that contribute to
trastuzumab resistance include obstacles preventing trastuzumab
binding to HER2, upregulation of signaling pathways downstream of
HER2, signaling through alternate pathways and failure to trigger
an immune-mediated mechanism to destroy tumor cells (18). Previously, two independent studies
reported that the loss of HER2 expression following NAC was
observed in 20–27.5% of patients who initially expressed the HER2
protein (19,20). It was hypothesized that a change in
the molecular subtype in the present case may indicate the
acquisition of resistance to the treatment via the activation of an
alternative receptor pathway, including pathways involving
insulin-like growth factor-1R, epidermal growth factor receptor and
c-Met. Another explanation of the subtype change may be that the
HER2-positive component of BC was suppressed by trastuzumab and the
remaining section of the tumor showed progression. In other words,
the subtype change reflected the heterogeneity of BC. In any case,
clinicians must carefully monitor the molecular behavior of BC to
select the optimal treatment.
In conclusion, it is important to consider the
possibility of a subtype change if treatment failure occurs.
Repeated biopsies must be performed during the course of the
treatment when the primary BC and/or metastatic lesions are
available.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
van't Veer LJ, Dai H, van de Vijver MJ, He
YD, Hart AA, Mao M, Peterse HL, van der Kooy K, Marton MJ,
Witteveen AT, et al: Gene expression profiling predicts clinical
outcome of breast cancer. Nature. 415:530–536. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Guarneri V and Conte P: Metastatic breast
cancer: Therapeutic options according to molecular subtypes and
prior adjuvant therapy. Oncologist. 14:645–656. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Greene FL: Breast tumours. TNM
classification of malignant tumours. Sobin LH, Gospodarowicz MK and
Wittekind C: (7th ed). Wiley-Blackwell. (Oxford). 181–93. 2009.
|
|
5
|
Hoff J, Portet R, Becue J, Fourtanier G
and Bugat R: Digestive tract metastases of breast cancers. Ann
Chir. 37:281–284. 1983.(In French). PubMed/NCBI
|
|
6
|
Borst MJ and Ingold JA: Metastatic
patterns of invasive lobular versus invasive ductal carcinoma of
the breast. Surgery. 114:637–641; discussion 641–642.
1993.PubMed/NCBI
|
|
7
|
Washington K and McDonagh D: Secondary
tumors of the gastrointestinal tract: Surgical pathologic findings
and comparison with autopsy survey. Mod Pathol. 8:427–433.
1995.PubMed/NCBI
|
|
8
|
Caramella E, Bruneton JN, Roux P, Aubanel
D and Lecomte P: Metastases of the digestive tract. Report of 77
cases and review of the literature. Eur J Radiol. 3:331–338.
1983.PubMed/NCBI
|
|
9
|
Wang Z, Spaulding B, Sienko A, Liang Y, Li
H, Nielsen G, Gong Yub G, Ro JY and Zhai Jim Q: Mammaglobin, a
valuable diagnostic marker for metastatic breast carcinoma. Int J
Clin Exp Pathol. 2:384–389. 2009.PubMed/NCBI
|
|
10
|
Takeda Y, Tsuta K, Shibuki Y, Hoshino T,
Tochigi N, Maeshima AM, Asamura H, Sasajima Y, Ito T and Matsuno Y:
Analysis of expression patterns of breast cancer-specific markers
(mammaglobin and gross cystic disease fluid protein 15) in lung and
pleural tumors. Arch Pathol Lab Med. 132:239–243. 2008.PubMed/NCBI
|
|
11
|
Raju U, Ma CK and Shaw A: Signet ring
variant of lobular carcinoma of the breast: A clinicopathologic and
immunohistochemical study. Mod Pathol. 6:516–520. 1993.PubMed/NCBI
|
|
12
|
Wick MR, Lillemoe TJ, Copland GT, Swanson
PE, Manivel JC and Kiang DT: Gross cystic disease fluid protein-15
as a marker for breast cancer: Immunohistochemical analysis of 690
human neoplasms and comparison with alpha-lactalbumin. Hum Pathol.
20:281–287. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Schwarz RE, Klimstra DS and Turnbull AD:
Metastatic breast cancer masquerading as gastrointestinal primary.
Am J Gastroenterol. 93:111–114. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pectasides D, Psyrri A, Pliarchopoulou K,
Floros T, Papaxoinis G, Skondra M, Papatsibas G, Macheras A,
Athanasas G, Arapantoni-Datioti P and Economopoulos T: Gastric
metastases originating from breast cancer: Report of 8 cases and
review of the literature. Anticancer Res. 29:4759–4763.
2009.PubMed/NCBI
|
|
15
|
García-Becerra R, Santos N, Díaz L and
Camacho J: Mechanisms of resistance to endocrine therapy in breast
cancer: Focus on signaling pathways, miRNAs and genetically based
resistance. Int J Mol Sci. 14:108–145. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gutierrez MC, Detre S, Johnston S, Mohsin
SK, Shou J, Allred DC, Schiff R, Osborne CK and Dowsett M:
Molecular changes in tamoxifen-resistant breast cancer:
Relationship between estrogen receptor, HER-2 and p38
mitogen-activated protein kinase. J Clin Oncol. 23:2469–2476. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yang YF, Liao YY, Li LQ, Xie SR, Xie YF
and Peng NF: Changes in ER, PR and HER2 receptors status after
neoadjuvant chemotherapy in breast cancer. Pathol Res Pract.
209:797–802. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pohlmann PR, Mayer IA and Mernaugh R:
Resistance to trastuzumab in breast cancer. Clin Cancer Res.
15:7479–7491. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Guarneri V, Dieci MV, Barbieri E,
Piacentini F, Omarini C, Ficarra G, Bettelli S and Conte PF: Loss
of HER2 positivity and prognosis after neoadjuvant therapy in
HER2-positive breast cancer patients. Ann Oncol. 24:2990–2994.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hirata T, Shimizu C, Yonemori K, Hirakawa
A, Kouno T, Tamura K, Ando M, Katsumata N and Fujiwara Y: Change in
the hormone receptor status following administration of neoadjuvant
chemotherapy and its impact on the long-term outcome in patients
with primary breast cancer. Br J Cancer. 101:1529–1536. 2009.
View Article : Google Scholar : PubMed/NCBI
|