Introduction
Schwannomas are benign, encapsulated and slowly
growing neoplasms which are composed exclusively of Schwann cells.
Schwannomas usually occur in the upper extremities, trunk, head and
neck, retroperitoneum, mediastinum, and pelvis (1). It has been reported to occasionally
occur in the rectum, pancreas, bile duct and stomach; however,
schwannomas arising from the liver parenchyma are extremely
uncommon. Hepatic schwannoma may cause non-specific clinical
symptoms. Since hepatic schwannoma is such a rare finding, a
definitive diagnosis by radiological methods is difficult and they
are sometimes misinterpreted as liver metastases or primary liver
cancer. Surgery is typically required in order to establish the
diagnosis and treatment (2).
The present study found only 30 cases reported in
the literature to date after carefully excluding those papers which
are duplicated and with insufficient clinical data. The present
study described a case of hepatic schwannoma and provide a
pertinent review of the literature.
Case report
On March 12th 2015, a 64-year-old Chinese
male was referred to The First Affiliated Hospital of Zhejiang
University (Hangzhou, China), with complaints of upper abdominal
pain for a month. A month ago, the patient suffered from upper
abdominal pain without obvious reasons and no chills, no fever, no
vomiting, no cough or other symptoms. No family history or obvious
evidence of neurofibromatosis was present. The abdominal physical
examination revealed no marked findings and all laboratory data
were normal, including tumor markers and liver function. The
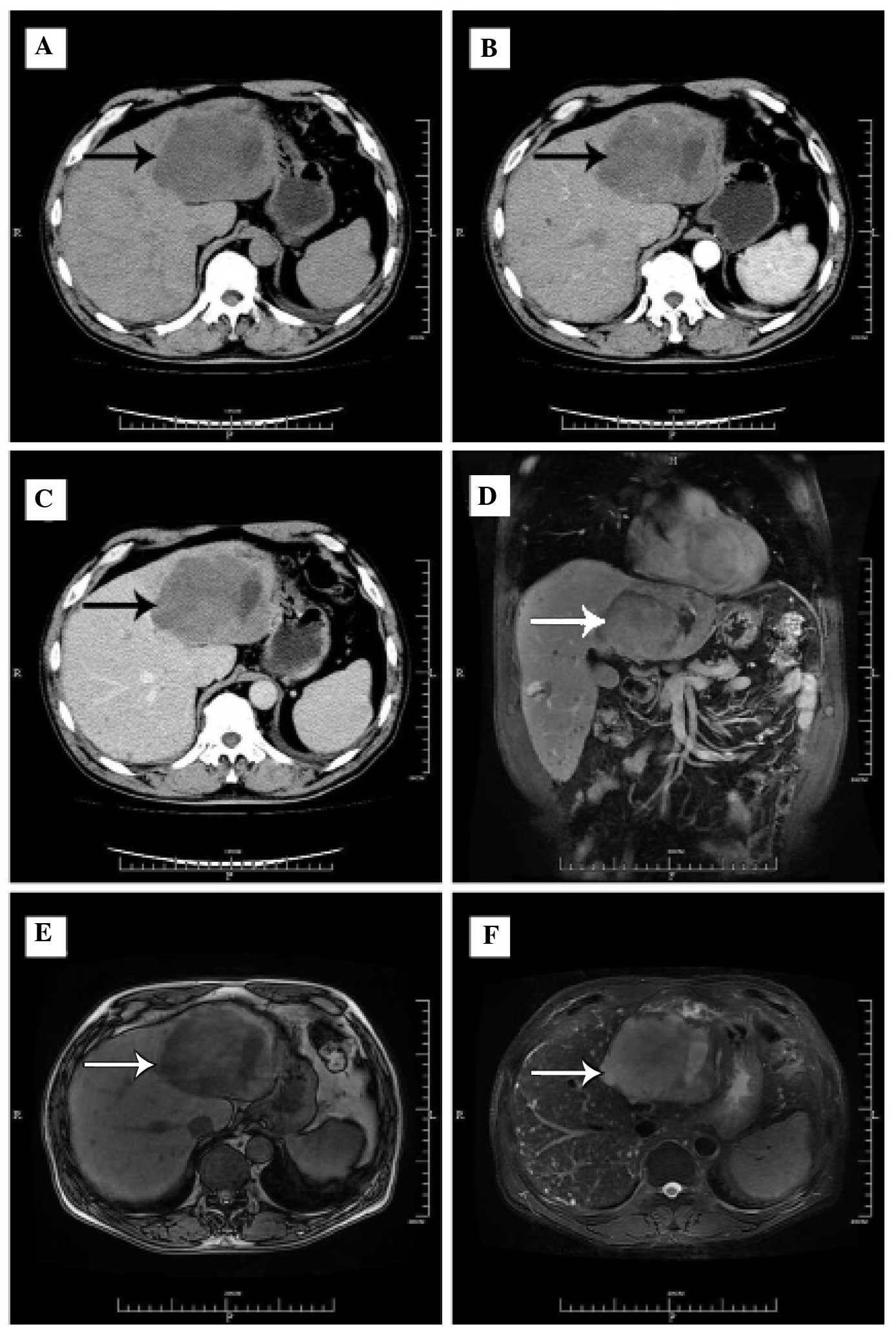
computed tomography (CT) scan (Fig.
1A–C) revealed an 11.5×9.5 cm mass in the left liver, slightly
enhanced in the arterial phase, progressive enhanced in the portal
and equilibrium phase, and the left branch of the portal was not
visible. The hilar and retroperitoneal area revealed a shadow of
multiple lymph nodes. So cholangiocarcinoma was considered
initially with the left portal vein branch violation. Magnetic
resonance imaging (MRI) (Fig. 1D–F)
also revealed an 11.5×9.5 cm mass, with a low signal on T1-weighted
images and higher signal on T2-weighted images. The left portal
vein branch was not observed. According to the history and
radiographic examination of the patient, surgical resection was
selected for diagnosis and cure together by the patient and the
treatment team in various departments, including those of
Hepatobiliary Surgery, Radiology and Chemotherapy. During the
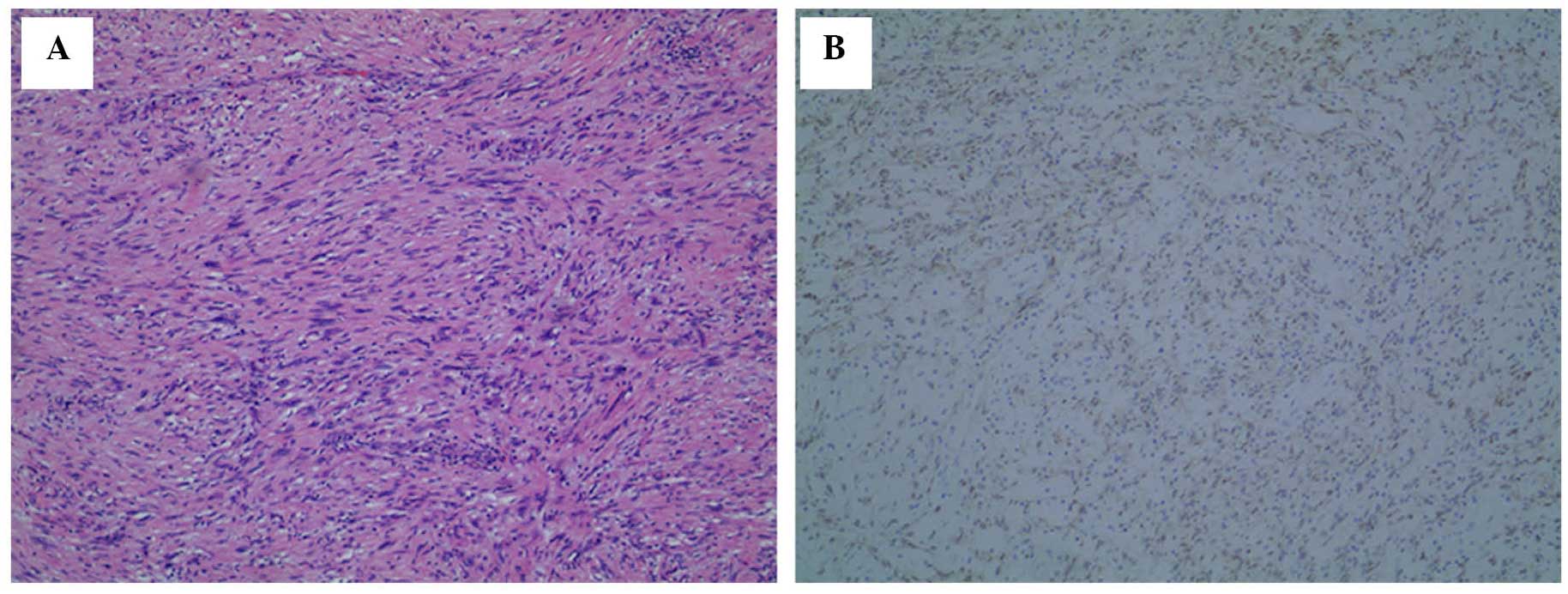
laparotomy, a hard protruding mass with a size of ~11.5×9 cm was
observed on the II, III and IV segment of the liver. Therefore, a
left hepatectomy and post-operative detailed histopathological
examination was performed, and revealed hepatic benign schwannoma
(Fig. 2): cytokeratin (pan)(−),
Vimentin(+), CD117(−), S-100(+), Desmin(−), CD34(−) and smooth
muscle actin [(SMA)-]. The patient was discharged on postoperative
day 14. Until now, no symptoms of recurrence were observed in the
patient.
Literature review
PubMed (https://www.ncbi.nlm.nih.gov/pubmed), MEDLINE
(http://webofknowledge.com/MEDLINE),
EMBASE (https://www.embase.com), The Cochrane
center (https://china.cochrane.org), The
Chinese Biology and Medicine Database (http://sinomed.imicams.ac.cn/zh/), The Chinese Wanfang
Database (http://g.wanfangdata.com.cn) and The
China Hospital knowledge Database (http://www.chkd.cnki.net) were searched for cases of
primary hepatic parenchyma schwannoma between January 1974 and
December 2014. Reports which are duplicated or lacked clinical data
were carefully excluded and 30 cases, along with the current case
report, were identified (Table
I).
 | Table I.Summary of cases with hepatic
schwannoma. |
Table I.
Summary of cases with hepatic
schwannoma.
| Author | Country | Sex/age | Presenting
symptoms | Examination | Primary
diagnosis | Size (cm) | Location | Treatment | Histology | Outcome | Ref |
|---|
| Current case | China | M/64 | RUG pain | US/CT/MRI | ICC | 11.5 | Left | Surgery | Benign | Survival | – |
| Hytiroglou et
al, 1993 | USA | F/57 | Right flank and back
pain | US/CT | Liver tumor | 13.0 | Right | Surgery | Benign | Survival | (1) |
| Ozkan et al,
2010 | Turkey | M/56 | Epigastric pain | US/CT | Liver hydatid
cyst | 15.0 | Left | Surgery | Benign | Survival | (2) |
| Ota et al,
2012 | Japan | F/72 | Incidental
finding |
US/CT/MRI/PET/CEUS | BCAC or ICC | 4.5 | Left | Surgery | Benign | Survival | (5) |
| Heffron et al,
1993 | USA | F/38 | RUG pain | CT/Biopsy | Schwannoma | 5.0 | Left | Surgery | Benign | Survival | (7) |
| Iddings et al,
2008 | USA | M/83 | Incidental
finding | CT/Biopsy | Myxoid
liposarcoma | 7.0 | Right | Surgery | Malignant | Survival | (8) |
| Kobori et al,
2008 | Hungary | F/22 | RUG pain/Edema | CT/Biopsy | Atypical malignant
tumor | 2.6 | Both | Surgery | Malignant | Survival | (9) |
| Morikawa et
al, 1995 | Japan | M/63 | Abdominal pain | CT | ICC | 20.0 | Right | Autopsy | Malignant | Death | (10) |
| Zhang et al,
2008 | China | F/59 | Incidental
finding | US/CT | ICC | 8.0 | Left | Surgery | Benign | Survival | (11) |
| Wada et al,
1998 | Japan | F/64 | Asymptomatic | US/CT/MRI | Liver tumor | 4.0 | Left | Surgery | Benign | Survival | (12) |
| Wada et al,
1998 | Japan | F/69 | Asymptomatic | US/CT | Liver tumor | 15.0 | Left | Surgery | Benign | Survival | (12) |
| Akin et al,
2009 | Turkey | F/66 | Incident finding | US/CT | Breast cancer
metastasis | 4.4 | Left | Surgery | Benign | Survival | (13) |
| Kim et al,
2010 | South Korea | M/52 | Incident
finding | US/CT | Malignant or
inflam-matory tumor (liver) |
3.0 | Left | Surgery | Benign | Survival | (14) |
| Xu et al,
2007 | China | F/43 | RUG pain | CT | GIST
metastasis |
5.0 | Left | Surgery | Benign | Survival | (15) |
| Piao et al,
2009 | China | F/43 | RUG pain | US/CT | Liver tumor |
4.2 | Left | Surgery | Benign | Survival | (16) |
| Hayashi et
al, 2012 | Japan | M/64 | Incident
finding | US/CT/MRI/PET | GIST
metastasis |
2.3 | Left | Surgery | Benign | Survival | (17) |
| Kapoor et
al, 2005 | India | F/mid-aged | Epigastric lump and
dull pain | US/CT | Liver adenoma | 23.0 | Left | Surgery | Benign | Survival | (18) |
| Yoshida et
al, 1994 | Japan | F/56 | Epigastrium and
chest discomfort | US/CT | Liver tumor | 16.0 | Right | Surgery | Benign | Survival | (19) |
| Flemming et
al, 1998 | Germany | F/57 | Upper abdominal
pain | US/CT | Hydatid
disease | Huge | Right | Surgery | Benign | Survival | (20) |
| Jin et al,
2001 | China | M/42 | RUG pain and
fever | CT/MRI/Biopsy | Hepatapostema |
6.7 | Right | Surgery | Benign | Survival | (21) |
| Momtahen et
al, 2008 | USA | F/52 | Back pain | CT/MRI/Biopsy | Schwannoma |
4.4 | Right | Surgery | Benign | Survival | (22) |
| Liu et al,
2005 | China | F/27 | RUG lump and dull
pain | US/CT/Biopsy | Spindle tumor | 30.0 | Right | LT | Benign | Survival | (23) |
| Lee et al,
2008 | South Korea | F/38 | Vague epigastric
pain | US/CT/Biopsy | Mesenchymal
tumor |
5.0 | Right | Surgery | Benign | Survival | (24) |
| Young et al,
1975 | England | M/23 | RUG/Jaundice | Biopsy | Liver tumor | 20.0 | Both | Autopsy | Malignant | Death | (25) |
| Lederman et
al, 1987 | USA | M/21 | RUG pain/Shaking
chills | US/HA | NF | 30.0 | Both | HAE/Autopsy | Malignant | Death | (26) |
| Yu et al,
1999 | China | F/55 | RUG pain | US/CT | Huge liver
cyst | 26.0 | Right | Surgery | Malignant | Death | (27) |
| Fiel et al,
1996 | USA | F/49 | Obstructive
jaundice | CT/Biopsy | Spindle tumor | 14.0 | Right | Surgery | Malignant | Survival | (28) |
| Fang et al,
1999 | China | M/42 | Abdominal pain
after trauma | CT | Intrahepatic
hematoma | 14.0 | Right | Surgery | Malignant | Death | (29) |
| Li et al,
2009 | China | F/40 | RUG pain | CT | Schwannoma | Huge | Right | TACE | Malignant | Death | (30) |
Discussion
Verocay (3) first
reported schwannoma as a true neoplasm in 1990. The name schwannoma
is often termed differently in primary research, including
neurilemmoma, neuroma, neurinoma and nerve sheath tumor. The latest
4th edition of the World Health Organization pathology
classification put the peripheral nerve tumors, which included
schwannomas, into the soft tissue tumor types, which further
demonstrated the understanding of schwannomas (4).
Generally speaking, schwannomas are benign,
encapsulated and slowly growing neoplasms, which are composed
exclusively of Schwann cells. Schwannomas usually occur in the
upper extremities, trunk, head and neck, retroperitoneum,
mediastinum and pelvis. It has been reported that occasionally,
schwannomas occur in the rectum, pancreas, bile duct and stomach;
however, schwannomas arising from the liver parenchyma are
extremely uncommon (1). Only 30 cases
were found to be reported in the literature to date, following the
careful exclusion of those papers which are duplicated and with
insufficient clinical data.
Schwannomas occur at all ages, but are most common
in individuals aged between 30 and 60-years-old, and the ratio
between genders is ~1:1 (2). In the
present study, the mean age of the 30 patients was 51.7 (range,
21–83 years), which was consistent with the previous report and
~2/3 was female. A total of 18 patients were from Asia, 6 from
Europe and 6 from North-America, which may represent that hepatic
schwannoma was more common in Asian; however, more evidence is
required.
As described previously, the majority of patients
were admitted with the complaint of pain or discomfort in the upper
abdomen or epigastrium (5). In the
present study, 8 patients were asymptomatic, whose liver tumors
were found during routine examination or the follow-up when
combined with other diseases. A total of 22 patients were
symptomatic and symptoms included abdominal pain (91%), back pain
(9%), chill and fever (9%), abdominal mass (9%), jaundice (9%),
edema (5%), and weight loss (5%).
To differentiate from other primary liver tumors,
including hepatocellular carcinoma and intrahepatic
cholangiocarcinoma, liver metastases when the patient suffered
certain types of malignant tumor, and hydatid disease of the liver
when cystic transformation were present, auxiliary examinations
including ultrasonography (US), CT, MRI and even positron emission
tomography (PET)-CT are required. These techniques can determine
tumor position, size, and an appropriate staging of the tumor
extension and involved structures, which is of great assistance to
diagnose and design an operation scheme. However, since hepatic
schwannoma is such a rare finding, a definitive diagnosis by
radiological methods is difficult. Liver biopsy may be useful for
accurate preoperative diagnosis (5,6).
In the present study, 28 patients received CT for
diagnosis in 30 cases with auxiliary examinations. US, MRI or
PET-CT was also selected in certain cases. A total of 9 cases
selected preoperative biopsy for diagnosis. Even though the imaging
examination is more precise, only 2 patients had the exact
diagnosis and other 28 patients were misdiagnosed with other
diseases or no confirmed diagnosis.
The final diagnosis of depends on the pathology and
immunohistochemistry. Microscopically, a typical schwannoma is
composed of Antoni A and Antoni B areas. The Antoni A area is a
hypercellular area, which contains a large number of closely packed
spindle cells. By contrast, the Antoni B area is a loose myxoid
structure with a few sparse cells. The proportion of the two
components can shift gradually or change suddenly (7). Cystic degeneration, including
calcification or hemorrhage, is often recognized in the Antoni B
area, which may result from vascular thrombosis and subsequent
necrosis. Immunohistochemical analysis is necessary to distinguish
hepatic schwannoma from metastatic gastrointestinal stromal tumor
types and other soft tissue tumor types. A schwannoma is usually
positive for S-100, negative for both CD34 and CD117. However,
metastatic gastrointestinal stromal tumors are positive for S-100,
and positive for either CD34 or CD117. A leiomyoma would be
negative for S-100 and positive for desmin or SMA (8). When the hepatic schwannoma presented
with numerous sub-foci around or grown rapidly or associated with a
highly-aggressive course of recurrence during follow-up, it almost
certainly was the malignant type (9).
In the present statistics, of the 9 malignant
schwannoma cases, 1 was semi-malignant and 20 were benign. Although
the tumor in certain cases was reported to be S-100 negative, other
characteristics of it proved the malignant nature (9). When the patient wants to take a
conservative treatment, the pathology and immunohistochemistry of
the liver tumor tissue must be performed to exclude the malignant
transformation, since survival with observation alone for malignant
schwannoma is poor (10).
Since discriminating between a schwannoma and
malignant liver neoplasm is difficult, surgery is typically
recommended. In order to better observe the difference in the
treatment and prognosis between the benign and malignant primary
hepatic schwannoma, the 30 patients were divided into two groups.
In the benign group, 13/20 cases with liver tumors were located in
the left lobe and 7/20 were distributed in the right lobe. The
maximal diameter of the tumors reported varied between 2.3 and 30
cm. All patients in the benign group underwent surgical treatment
and survived until the last follow-up, of whom 19 received complete
resection. The tumor of the remaining patient was too large (the
maximal diameter was 30 cm) to be removed surgically, so that
patient underwent liver transplantation and no recurrence was
observed during the follow-up of 4 months. In the malignant group
(10 cases, including one semi-malignant case), the location of
hepatic schwannoma in 6/10 cases was the right lobe and in 4/10 was
both lobes. The size ranged between 2.6 and 30 cm. However, only 3
cases who underwent surgical resection survived at the last
follow-up. The other 7 cases succumbed to mortality; 4 patients
deteriorated prior to operation, and in the 3 cases with
hepatectomy, 1 succumbed to liver dysfunction at 21 days
postoperatively and 2 succumbed to recurrences at 18 and 23 months
postoperatively. These results suggested that hepatic schwannoma
must be resected regardless of the admission diagnosis of benign or
malignant, since if schwannomas are benign, surgical treatment can
lead to long-term survival and if malignant, enucleation should be
oncologically adequate and once radical surgery is impossible,
palliative resection is still recommended. To detect recurrence, a
CT scan every 3 months for the initial 2 years, every 6 months for
2–5 years and annually thereafter, is generally recommended.
In conclusion, hepatic schwannoma is a rare benign
disease with a good prognosis. However, this disease deserves
attention with regards to the differential diagnosis of liver
tumors. Preoperative diagnosis is highly difficult and complete
resection is the mainstay for cure, with liver transplantation
sometimes being necessary.
Acknowledgements
The authors would like to thank the entire staff of
the Departments of Hepatobiliary and Pancreatic Surgery, Pathology,
and Radiology at The First Affiliated Hospital of Zhejiang
University, School of Medicine (Zhejiang, China) for helpful
assistance.
References
|
1
|
Hytiroglou P, Linton P, Klion F, Schwartz
M, Miller C and Thung SN: Benign schwannoma of the liver. Arch
Pathol Lab Med. 117:216–218. 1993.PubMed/NCBI
|
|
2
|
Ozkan EE, Guldur ME and Uzunkoy A: A Case
report of benign schwannoma of the liver. Intern Med. 49:1533–1536.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Verocay J: Zur Kenntnis der ‘Neurofibrome.
’ Beitr Pathol Anat Allg Pathol. 48:1–69. 1910.(In German).
|
|
4
|
Fletcher CD, Bridge JA, Hogendoorn PC and
Mertens: World Health Organization classification of soft tissue
and bone tumours. Lyon-IARC Press. 2013.
|
|
5
|
Ota Y, Aso K, Watanabe K, Einama T, Imai
K, Karasaki H, Sudo R, Tamaki Y, Okada M, Tokusashi Y, et al:
Hepatic schwannoma: Imaging findings on CT, MRI and
contrast-enhanced ultrasonography. World J Gastroenterol.
18:4967–4972. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ortega-Candil A, Rodríguez-Rey C,
Cabrera-Martín MN, García García-Esquinas M, Lapeña-Gutiérrez L and
Carreras-Delgado JL: 18FDG PET/CT imaging of schwannoma mimicking
colorectal cancer metastasis. Rev Esp Med Nucl Imagen Mol.
32:332–333. 2013.PubMed/NCBI
|
|
7
|
Heffron TG, Coventry S, Bedendo F and
Baker A: Resection of primary schwannoma of the liver not
associated with neurofibromatosis. Arch Surg. 128:1396–1398. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Iddings DM, Wright BE and Bilchik A: A
rare cause of primary hepatic neoplasm: Malignant peripheral nerve
sheath tumor in the age of modern liver surgery. Am Surg. 74:47–50.
2008.PubMed/NCBI
|
|
9
|
Kobori L, Nagy P, Mathe Z, Hartmann E,
Doros A, Paku S, Dezso K and Sápi Z: Malignant peripheral nerve
sheath tumor of the liver: A case report. Pathol Oncol Res.
14:329–332. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Morikawa Y, Ishihara Y, Matsuura N,
Miyamoto H and Kakudo K: Malignant schwannoma of the liver. Dig Dis
Sci. 40:1279–1282. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhang L, Yu R and Chen Y: Primary hepatic
benign schwannoma: Case report. Chin J Radiol. 42:10682008.(In
Chinese).
|
|
12
|
Wada Y, Jimi A, Nakashima O, Kojiro M,
Kurohiji T and Sai K: Schwannoma of the liver: Report of two
surgical cases. Pathol Int. 48:611–617. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Akin M, Bozkirli B, Leventoglu S, Unal K,
Kapucu LO, Akyurek N and Sare M: Liver schwannoma incidentally
discovered in a patient with breast cancer. Bratisl Lek Listy.
110:298–300. 2009.PubMed/NCBI
|
|
14
|
Kim YC and Park MS: Primary hepatic
schwannoma mimicking malignancy on fluorine-18
2-fluoro-2-deoxy-D-glucose positron emission tomography-computed
tomography. Hepatology. 51:1080–1081. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Xu L, Zhou X and Qian H: Small bowel
stromal tumors associated with hepatic schwannoma: Case report.
Chin J Bases Clin General Surg. 14:7422007.(In Chinese).
|
|
16
|
Piao G: One Case: Liver Schwannoma. J
Pract Radiol. 25:13432009.(In Chinese).
|
|
17
|
Hayashi M, Takeshita A, Yamamoto K and
Tanigawa N: Primary hepatic benign schwannoma. World J Gastrointest
Surg. 4:73–8. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kapoor S, Tevatia MS, Dattagupta S and
Chattopadhyay TK: Primary hepatic nerve sheath tumor. Liver Int.
25:458–9. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yoshida M, Nakashima Y, Tanaka A, Mori K
and Yamaoka Y: Benign schwannoma of the liver: A case report. Nihon
Geka Hokan. 63:208–214. 1994.PubMed/NCBI
|
|
20
|
Flemming P, Frerker M, Klempnauer J and
Pichlmayr R: Benign schwannoma of the liver with cystic changes
misinterpreted as hydatid disease. Hepatogastroenterology.
45:1764–1766. 1998.PubMed/NCBI
|
|
21
|
Jin L and Zhou Y: A case of hepatic
schwannoma misdiagnosed as liver abscess. Chin J Dig. 22:62002.
|
|
22
|
Momtahen AJ, Akduman EI, Balci NC, Fattahi
R and Havlioglu N: Liver schwannoma: Findings on MRI. Magn Reson
Imaging. 26:1442–1445. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu Y: A case of huge hepatic schwannoma
for liver transplantation. Chin network dynamics of infectious
diseases. 45. 2005.(In Chinese).
|
|
24
|
Lee WH, Kim TH, You SS, Choi SP, Min HJ,
Kim HJ, Lee OJ and Ko GH: Benign schwannoma of the liver: A case
report. J Korean Med Sci. 23:727–730. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Young SJ: Primary malignant neurilemmona
(schwannoma) of the liver in a case of neurofibromatosis. J Pathol.
117:151–153. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lederman SM, Martin EC, Laffey KT and
Lefkowitch JH: Hepatic neurofibromatosis, malignant schwannoma and
angiosarcoma in von Recklinghausen's disease. Gastroenterology.
92:234–239. 1987.PubMed/NCBI
|
|
27
|
Yu C, Li S and Zhang Z and Zhang Z: A case
of massive hepatic malignant schwannoma. Chin J Pract Oncol.
308:1999.(In Chinese).
|
|
28
|
Fiel MI, Schwartz M, Min AD, Sung MW and
Thung SN: Malignant schwannoma of the liver in a patient without
neurofibromatosis: A case report and review of the literature. Arch
Pathol Lab Med. 120:1145–1147. 1996.PubMed/NCBI
|
|
29
|
Fang X and Li C: Primary malignant
schwannoma of the liver: Case report. J Hepatopancreatbiliary
Surgery. 11:2021999.(In Chinese).
|
|
30
|
Tengfei Li, Zhen Wu, Gang Wu and Han X:
Hepatic malignant schwannoma in von Recklinghausen's disease: Case
report. Chin J CT and MRI. 7:77–78. 2009.(In Chinese).
|