Introduction
The status of lymph nodes in the neck is the most
important prognostic factor for oral squamous cell carcinoma
(OSCC). The rate of secondary neck metastases of OSSC is ~20–30%
(1–6).
Even with advanced modern imaging techniques, including computed
tomography (CT), magnetic resonance imaging (MRI), ultrasound (US)
and fluorodeoxyglucose positron emission tomography (FDG-PET), the
accuracy of current diagnostic imaging does not exceed 80%
(2).
The treatment strategies for early-stage oral cancer
clinically negative for neck metastasis (cN0) include performing
elective neck dissection (END) or opting for the watchful waiting
approach. END is currently the standard treatment for patients in
the absence of positive lymph nodes on imaging tests. Some reports
recommend END, as it reduces the risk of uncontrolled disease
(2,3).
Furthermore, a recent meta-analysis of randomized controlled trials
suggested a survival advantage with END (7). However, ≤70% of patients undergo
unnecessary neck dissection, resulting in decreased quality of life
(8,9).
Therefore, accurate detection of occult metastases
is crucial, as it allows for appropriate treatment planning.
With respect to sentinel node biopsy (SNB) in oral
cancer, large multi-institutional clinical trials have been
conducted (10,11) and numerous studies have demonstrated
that SNB is associated with predictably high accuracy in
identifying occult metastasis (10,12).
The objective of this study was to determine the
benefits of SNB for cN0 disease. We retrospectively compared
long-term survival following excision alone or excision and SNB in
patients with OSCC. Moreover, we analyzed the complications and
surgical stress of the SNB procedure, including limited range of
motion in the arm, size of the surgical scar and operative
time.
Patients and methods
Patient characteristics
A total of 125 patients with OSCC clinically staged
as N0 underwent tumor excision with/without SNB at the Department
of Oral and Maxillofacial Surgery of Kumamoto University (Kumamoto,
Japan) from 2006 to 2013. SNB was performed in patients who
consented to the procedure. The excision alone group included 78
patients, and the excision with SNB group included 47 patients. All
the patients were diagnosed with a primary oral tumor, and no
patients had received prior radiotherapy or chemotherapy.
Diagnostic imaging specialists comprehensively
diagnosed lymph node status with imaging techniques, including CT,
MRI, US and FDG-PET.
The study included 84 men and 41 women, with a mean
age of 65.6 years (range, 28–85 years). The primary tumor sites
included the tongue (n=79), lower gingiva (n=22), upper gingiva
(n=10), buccal mucosa (n=8) and oral floor (n=6). Regarding
T-classification, 48 cases were T1 and 77 were T2. The median
postoperative follow-up period was 43.6±24.7 months. Postoperative
radiotherapy was administered to 4 patients in the excision alone
group and 2 patients the excision with SNB group. The patient
characteristics did not differ significantly between the excision
alone and the excision with SNB groups (Table I).
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristics | Excision alone group
(n=78) | Excision with SNB
group (n=47) | P-value |
|---|
| Gender |
|
| 0.31a |
| Male,
n | 55 | 29 |
|
| Female,
n | 23 | 18 |
|
| Age, years |
|
| 0.97b |
| Mean ±
SD | 65.4±12.6 | 65.5±13.0 |
|
| Primary site |
|
| 0.94a |
|
Tongue | 50 | 29 |
|
| Lower
gingiva | 13 | 9 |
|
| Upper
gingiva | 7 | 3 |
|
| Buccal
mucosa | 5 | 3 |
|
| Oral
floor | 3 | 3 |
|
| T-classification |
|
| 0.12a |
| 1 | 34 | 14 |
|
| 2 | 44 | 33 |
|
| Follow-up period,
months |
|
| 0.07b |
| Mean ±
SD | 46.6±23.2 | 38.5±26.1 |
|
| Postoperative
radiotherapy |
|
| 0.82a |
| Yes,
n | 4 | 2 |
|
| No,
n | 74 | 45 |
|
Surgical procedure
On the day before surgery, the patients received
injections of 37 MBq 99mTc-phytate into 4 selected sites of the
submucosal layer surrounding the tumor.
Sentinel nodes (SNs) were identified by
single-photon emission CT/CT after 2 hours, and the operator
confirmed the anatomical position and number of nodes. At the time
of surgery, the SNs were removed with a hand-held gamma detector
probe. During the operation, all SNs were cut in 4-µm sections at
2-mm intervals and examined by hematoxylin and eosin staining. In
cases for which the rapid intraoperative diagnosis was positive,
radical neck dissection (RND) or modified radical neck dissection
(MRND) was performed. These SNs were further examined by
pathological investigation of paraffin-embedded sections.
Following discharge from the hospital, the patients
in the two groups were followed up every 2 weeks and carefully
examined by CT, MRI and US every 3 months.
We determined the number and distribution of the
detected SNs according to the American Academy of
Otolaryngology-Head and Neck Surgery classification (13). The secondary neck metastasis rate,
negative predictive value (NPV) and false-negative rate of SNB were
calculated (TN, 30 pts)/(FN + TN, 32 pts) and the false-negative
rate as (FN, 2 pts)/(TP + FN, 11 pts). Furthermore, overall
survival (OS) was compared between the excision alone and excision
with SNB groups.
In the excision with SNB group, we measured the time
required for the removal of SNs and the length of the surgical
scar, and assessed the surgical stress associated with the SNB
procedure.
Statistical analysis
All statistical analyses were performed using the
JMP9 statistical software (SAS Institute Inc., Cary, NC, USA). The
secondary metastasis rates of the two groups were compared using
the Chi-squared test. The 5-year OS rates were estimated using the
Kaplan-Meier method and the log-rank test was used for univariate
analysis. P-values <0.05 were considered to indicate
statistically significant differences.
Our retrospective study and clinical record reviews
were approved by the Review Board of our institution. Written
informed consent was obtained from all study patients. This
investigation was conducted according to the principles of the
Helsinki Declaration.
Results
SN detection
The SN detection rate was 100% and the average
number of removed SNs was 2.1 per patient (range, 1–5 nodes). In
46/47 patients, only ipsilateral SNs were removed. On the
ipsilateral side, 46 SNs were located at level I, 38 at level II,
10 at level III, 2 at level IV, and 1 at level V. On the
contralateral side, 1 SN was located at level II and 1 SN was
located at level III.
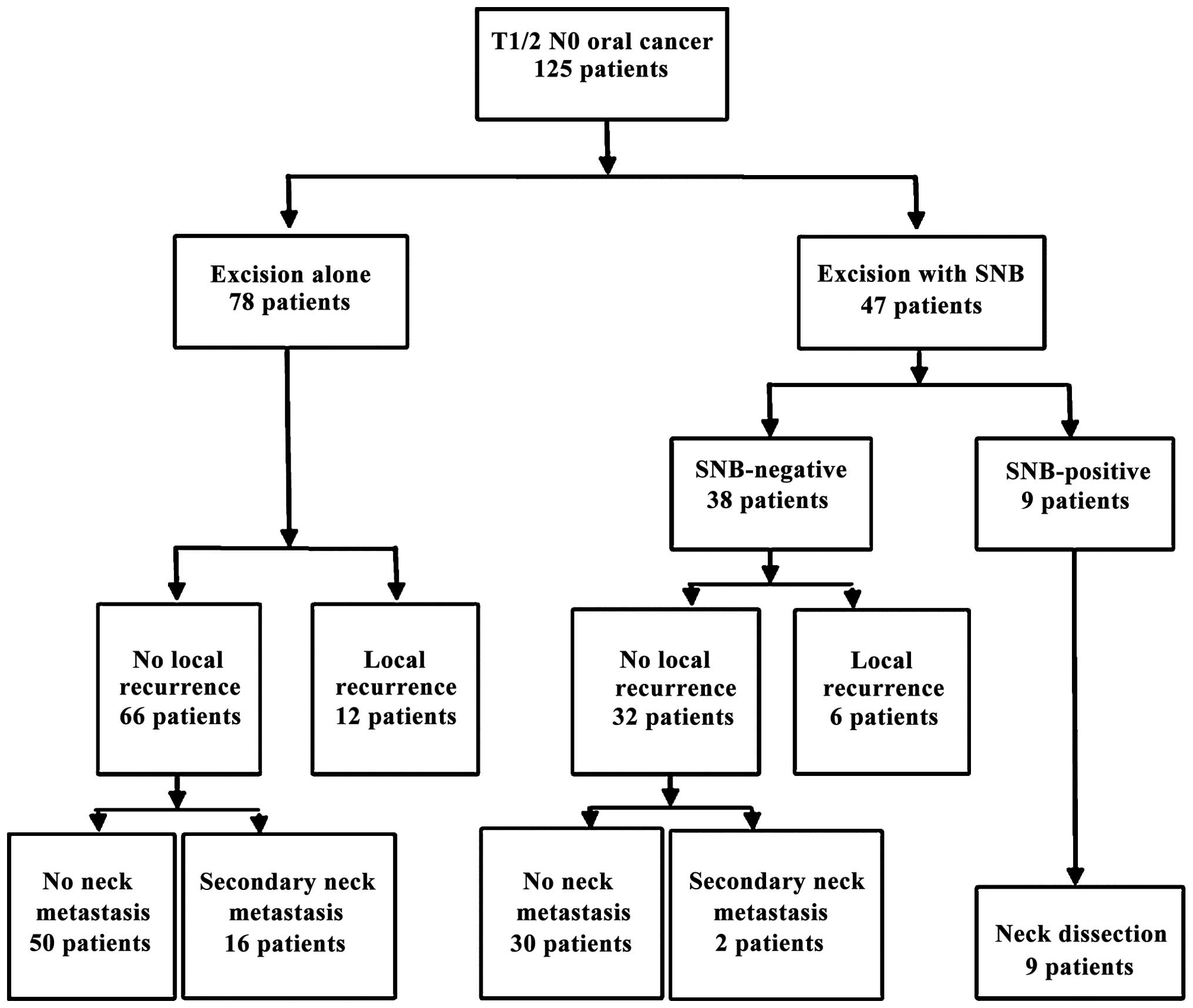
Follow-up
In the excision alone group (n=78), 12 local
recurrences of primary tumor and 16 secondary neck metastases
occurred during the follow-up period. Conversely, in the excision
with SNB group (n=47), intraoperative histopathological examination
of the SNs revealed micrometastases in 9 patients; 6 local
recurrences of primary tumor occurred, and secondary neck
metastasis appeared in 2 cases during the follow-up period. An RND
or MRND was performed in 9 SN-positive cases, and no further
metastatic lymph nodes were isolated from the dissected neck
tissue. The NPV, the false-negative rates and the SNB were
calculated while excluding local recurrences of primary tumor. The
NPV and false-negative rate of SNB were 94% (30/32) and 18% (2/11),
respectively (Fig. 1). The rate of
secondary neck metastasis was calculated. The rate of secondary
neck metastasis in the excision with SNB group was lower compared
with that in the excision alone group (4.9 vs. 24.2%, respectively;
P<0.05).
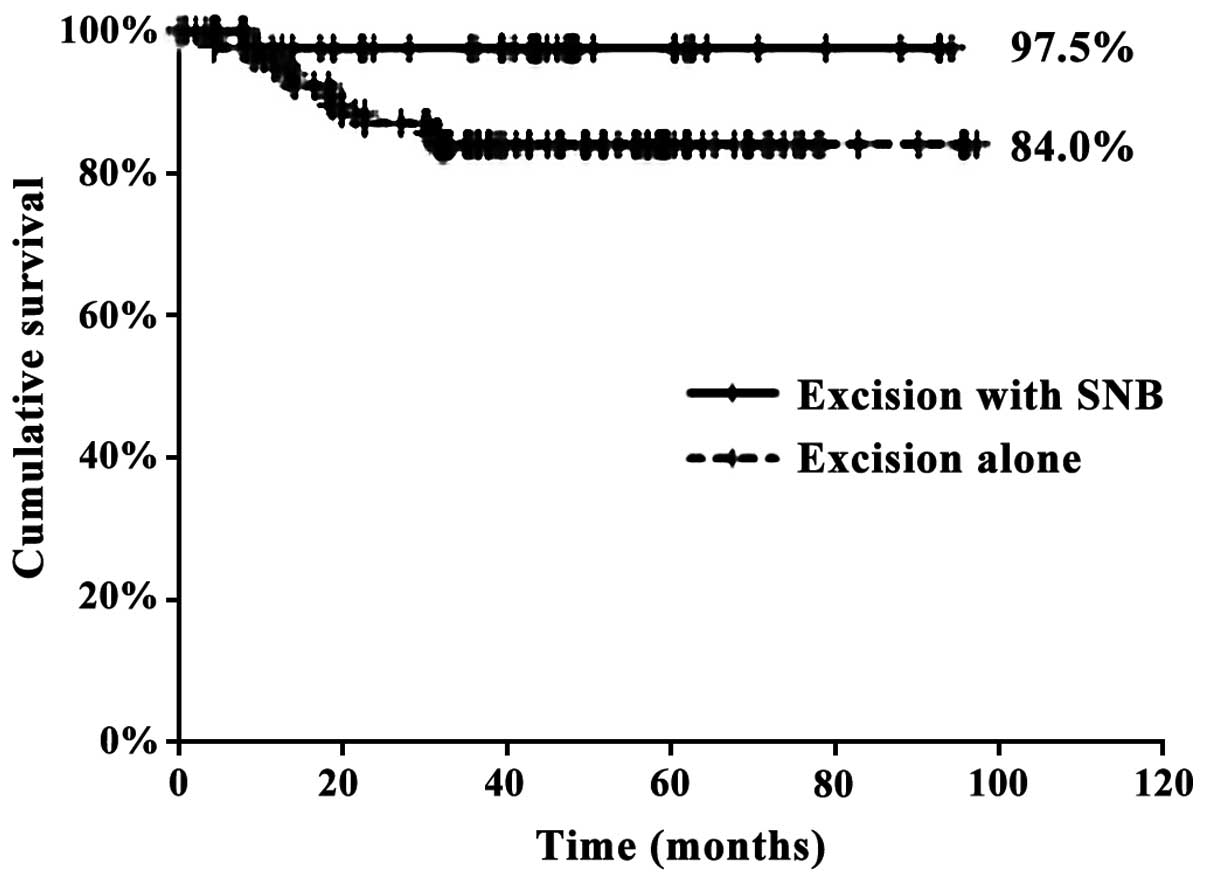
The number of deaths in the excision alone and
excision with SNB groups was 12 and 1, respectively. The 5-year OS
rates for the excision alone and excision with SNB groups were 84.0
and 97.5%, respectively (P<0.05) (Fig.
2).
In the excision with SNB group, the time required to
remove the SNs was 9.2 min per SN, and the length of the surgical
scar was 53 mm. The surgical stress associated with SNB was
minimal, and no complications, such as neck hematoma, facial palsy,
postoperative infection, or limited range of motion in the arm,
were observed.
Discussion
It has been well established that the presence or
absence of lymph node metastasis in the neck is the most important
prognostic factor for OSCC.
The prevalence of neck metastasis in cN0 early oral
carcinoma is relatively high, with rates ranging from 20 to 30%
(2,12). However, if all cN0 oral carcinoma
patients underwent END, this would result in overtreatment of
patients without metastasis. Currently, it remains controversial
whether END is necessary for the optimal management of patients
clinically negative for neck metastasis. Several reports have
recommended END, but there has been no definitive conclusion
(14–17).
SNB has attracted attention as a new diagnostic tool
that allows for the detection of micrometastasis in the neck lymph
nodes.
In multi-institutional trials, SNB has been shown to
exhibit a predictably high accuracy for identifying occult
metastasis (3,10,14,18,19).
A previous study by the American College of Surgeons
Oncology Group reported an NPV of 94% and a false-negative rate of
7% (8). In other reports, the NPV and
false-negative rates were 90–96 and 2.5–22%, respectively (3,10,18,20,21). In
the present study, the NPV and false-negative rates were 94 and
18%, respectively, which were similar to previously reported rates.
Thus, performing SNB is feasible, and this procedure may be used to
accurately predict neck metastasis in cN0 OSCC patients.
In our department, we have adopted the watchful
waiting approach to manage cN0 early OSCC. If the occurrence of
secondary neck metastasis becomes clinically apparent, RND or MRND
is immediately performed. Therefore, it is very important to detect
secondary metastases early, as this is directly associated with
patient prognosis. The patients were followed up every 2 weeks, and
carefully evaluated using CT, MRI and US every 3 months.
In the present study, SNs were detected in all the
cases, and the distribution of SNs was consistent with previous
reports (2). While evaluating neck
dissection tissue in the 9 SN-positive cases, we identified no
metastasis other than the one in the SN. On the basis of these
results, evaluating the SNs in oral cancer appears to be applicable
and feasible for the prediction of the status of neck lymph nodes
in cN0 early OSCC.
The rates of secondary neck metastasis in the
excision alone and excision with SNB groups were 4.9 and 24.2%,
respectively, and this difference was statistically significant.
Other reports have demonstrated that secondary neck metastasis
occurred in 0–6% of cases that underwent SNB, and our results were
similar (3,18,20,21).
Our study observed 5-year OS rates of 84.0 and 97.5%
for the excision alone and excision with SNB groups, respectively,
and this difference was statistically significant. Thus, SNB
reduced the rate of secondary neck metastasis and increased the
5-year OS rate. Other studies reported a 5-year OS rate of 80% and
a 2-year OS rate of 87–90%; our results are superior to those
findings (3,18,20,21),
suggesting that SNB is an effective approach in cN0 early OSCC.
However, there have been few previous reports comparing excision
alone to excision with SNB. Yamauchi et al reported that the
rate of secondary metastasis in the watchful waiting and SNB groups
was 27 and 9.1%, respectively, and this difference was not
statistically significant (21).
Our study included only a limited number of cases;
therefore, further large multi-institutional clinical trials are
required to investigate the long-term prognosis of patients who
undergo SNB.
In this study, the surgical stress and postoperative
complications of the SNB procedure were minimal. In this respect,
our findings were similar to those of other studies reporting that
postoperative complications of neck dissection, such as neck
hematoma, facial palsy, postoperative infection and limited range
of motion in the arm, rarely occur after SNB (20).
In conclusion, SNB is a minimally invasive and
highly reliable staging method, reduces the rate of secondary neck
metastasis and improves 5-year OS in patients with stage I and II
oral cancer.
Acknowledgements
We would like to thank Editage (www.editage.jp) for the English language editing.
Glossary
Abbreviations
Abbreviations:
|
CT
|
computed tomography
|
|
END
|
elective neck dissection
|
|
FDG-PET
|
fluorodeoxyglucose positron emission
tomography
|
|
MRI
|
magnetic resonance imaging
|
|
MRND
|
modified radical neck dissection
|
|
NPV
|
negative predictive value
|
|
OS
|
overall survival
|
|
OSCC
|
oral squamous cell carcinoma
|
|
RND
|
radical neck dissection
|
|
SN
|
sentinel node
|
|
SNB
|
sentinel node biopsy
|
|
US
|
ultrasound
|
References
|
1.
|
Bilde A, von Buchwald C, Therkildsen MH,
Mortensen J, Kirkegaard J, Charabi B and Specht L: Need for
intensive histopathologic analysis to determine lymph node
metastases when using sentinel node biopsy in oral cancer.
Laryngoscope. 118:408–414. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Hernando J, Villarreal P, Álvarez-Marcos
F, Gallego L, García-Consuegra L and Junquera L: Comparison of
related complications: Sentinel node biopsy versus elective neck
dissection. Int J Oral Maxillofac Surg. 43:1307–1312. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Samant S: Sentinel node biopsy as an
alternative to elective neck dissection for staging of early oral
carcinoma. Head Neck. 36:241–246. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Sloan P: Head and neck sentinel lymph node
biopsy: Current state of the art. Head Neck Pathol. 3:231–237.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Stoeckli SJ, Alkureishi LW and Ross GL:
Sentinel node biopsy for early oral and oropharyngeal squamous cell
carcinoma. Eur Arch Otorhinolaryngol. 266:787–793. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
von Buchwald C, Bilde A, Shoaib T and Ross
G: Sentinel node biopsy: The technique and the feasibility in head
and neck cancer. ORL J Otorhinolaryngol Relat Spec. 64:268–274.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Fasunla AJ, Greene BH, Timmesfeld N,
Wiegand S, Werner JA and Sesterhenn AM: A meta-analysis of the
randomized controlled trials on elective neck dissection versus
therapeutic neck dissection in oral cavity cancers with clinically
node-negative neck. Oral Oncol. 47:320–324. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Kuntz AL and Weymuller EA Jr: Impact of
neck dissection on quality of life. Laryngoscope. 109:1334–1338.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Nibu KI, Ebihara Y, Ebihara M, Kawabata K,
Onitsuka T, Fujii T and Saikawa M: Quality of life after neck
dissection: A multicenter longitudinal study by the Japanese
Clinical Study Group on Standardization of Treatment for Lymph Node
Metastasis of Head and Neck Cancer. Int J Clin Oncol. 15:33–38.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Civantos FJ, Zitsch RP, Schuller DE,
Agrawal A, Smith RB, Nason R, Petruzelli G, Gourin CG, Wong RJ,
Ferris RL, et al: Sentinel lymph node biopsy accurately stages the
regional lymph nodes for T1-T2 oral squamous cell carcinomas:
Results of a prospective multi-institutional trial. J Clin Oncol.
28:1395–1400. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Yuen AP, Wei WI, Wong YM and Tang KC:
Elective neck dissection versus observation in the treatment of
early oral tongue carcinoma. Head Neck. 19:583–588. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Stoeckli SJ: Sentinel node biopsy for oral
and oropharyngeal squamous cell carcinoma of the head and neck.
Laryngoscope. 117:1539–1551. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Robbins KT, Clayman G, Levine PA, Medina
J, Sessions R, Shaha A, Som P and Wolf GT: American Head and Neck
Society; American Academy of Otolaryngology-Head and Neck Surgery:
Neck dissection classification update: Revisions proposed by the
American Head and Neck Society and the American Academy of
Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck
Surg. 128:751–758. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Alvarez J, Bidaguren A, McGurk M,
Diaz-Basterra G, Brunsó J, Andikoetxea B, Martín JC, Barbier L,
Arteagoitia I and Santamaría JA: Sentinel node biopsy in relation
to survival in floor of the mouth carcinoma. Int J Oral Maxillofac
Surg. 43:269–273. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Bessell A, Glenny AM, Furness S, Clarkson
JE, Oliver R, Conway DI, Macluskey M, Pavitt S, Sloan P and
Worthington HV: Interventions for the treatment of oral and
oropharyngeal cancers: Surgical treatment. Cochrane Database Syst
Rev: Cd006205. 2011. View Article : Google Scholar
|
|
16.
|
Keski-Säntti H, Atula T, Törnwall J,
Koivunen P and Mäkitie A: Elective neck treatment versus
observation in patients with T1/T2 N0 squamous cell carcinoma of
oral tongue. Oral Oncol. 42:96–101. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Rodrigo JP, Shah JP, Silver CE, Medina JE,
Takes RP, Robbins KT, Rinaldo A, Werner JA and Ferlito A:
Management of the clinically negative neck in early-stage head and
neck cancers after transoral resection. Head Neck. 33:1210–1219.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Alkureishi LW, Ross GL, Shoaib T, Soutar
DS, Robertson AG, Thompson R, Hunter KD, Sorensen JA, Thomsen J,
Krogdahl A, et al: Sentinel node biopsy in head and neck squamous
cell cancer: 5-year follow-up of a European multicenter trial. Ann
Surg Oncol. 17:2459–2464. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Ross GL, Soutar DS, MacDonald Gordon D,
Shoaib T, Camilleri I, Roberton AG, Sorensen JA, Thomsen J, Grupe
P, Alvarez J, et al: Sentinel node biopsy in head and neck cancer:
Preliminary results of a multicenter trial. Ann Surg Oncol.
11:690–696. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Schiefke F, Akdemir M, Weber A, Akdemir D,
Singer S and Frerich B: Function, postoperative morbidity, and
quality of life after cervical sentinel node biopsy and after
selective neck dissection. Head Neck. 31:503–512. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Yamauchi K, Fujioka Y and Kohno N:
Sentinel node navigation surgery versus observation as a management
strategy for early tongue carcinoma. Head Neck. 34:568–572. 2012.
View Article : Google Scholar : PubMed/NCBI
|