Introduction
The majority of malignant pancreatic tumors are
primary pancreatic neoplasms. Pancreatic metastases are very
uncommon (1,2) and usually originate from the kidney,
lung, breast, gastrointestinal tract, or from melanoma. Metastasis
from the ovary is extremely rare. Most patients with metastatic
pancreatic tumors have widespread disease and are, therefore, not
candidates for resection. A previous study determined that,
although patients with metastatic pancreatic tumors originating
from renal-cell cancer can survive for a long time following
metastasectomy, survival is less favorable for other primary
tumors, including ovarian cancer (3).
Only a few cases of ovarian cancer metastasizing to the pancreas
have been reported in the literature (4,5).
Differences exist in the treatment of patients with
primary ovarian cancer and those with primary pancreatic cancer.
Therefore, it is important to confirm the precise diagnosis when
ovarian and pancreatic tumors are discovered simultaneously. The
present study reported a patient with serous carcinoma of the ovary
that metastasized to the tail of the pancreas. This diagnosis was
confirmed by needle-aspiration biopsy of the ovarian tumor,
endoscopic ultrasound (EUS) fine-needle aspiration (FNA) biopsy of
the pancreatic tumor and computed tomography (CT)-guided paraaortic
lymph-node biopsy.
Case report
A 73-year-old, gravidity 2 parity 2, presented to an
outside institution complaining of abdominal distension. The
patient had a history of interstitial pneumonia and was taking
prednisolone. No other significant past medical or surgical history
was known. Written informed consent was obtained from the patient
and a general physical examination revealed normal results. The
hemoglobin level was 6.6 g/dl and her cancer antigen (CA)125 level
was highly elevated at 382 ng/ml. The carbohydrate antigen 19-9 and
carcinoembryonic antigen (CEA) levels were slightly elevated at 52
U/ml and 15.7 ng/ml, respectively.
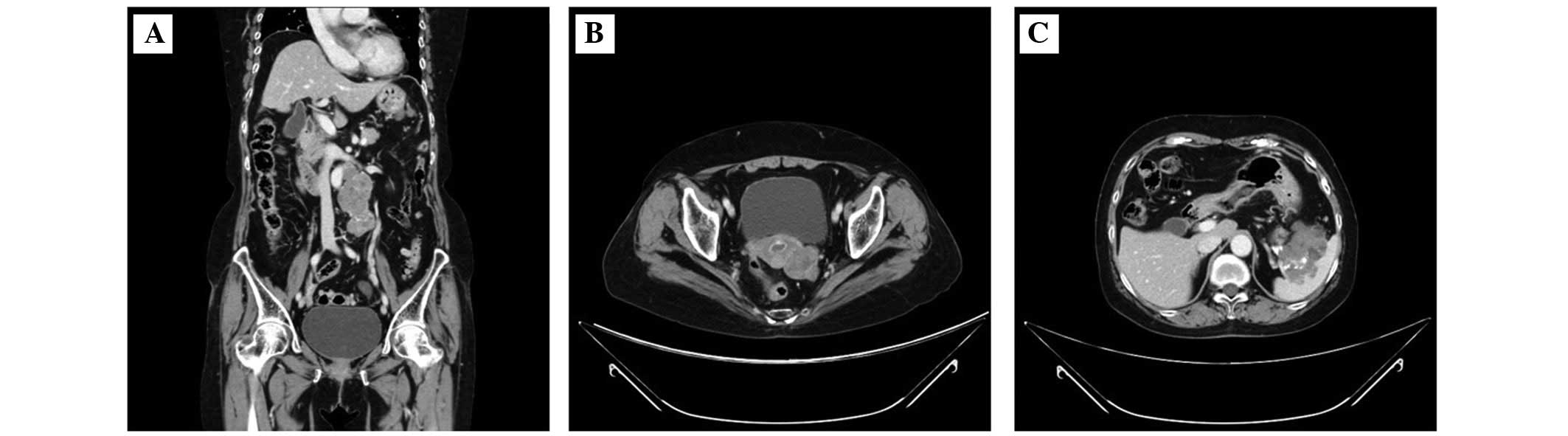
Contrast-enhanced CT revealed paraaortic
lymphadenopathy, a left ovarian mass and a 6 cm pancreatic mass
(Fig. 1). The patient underwent a
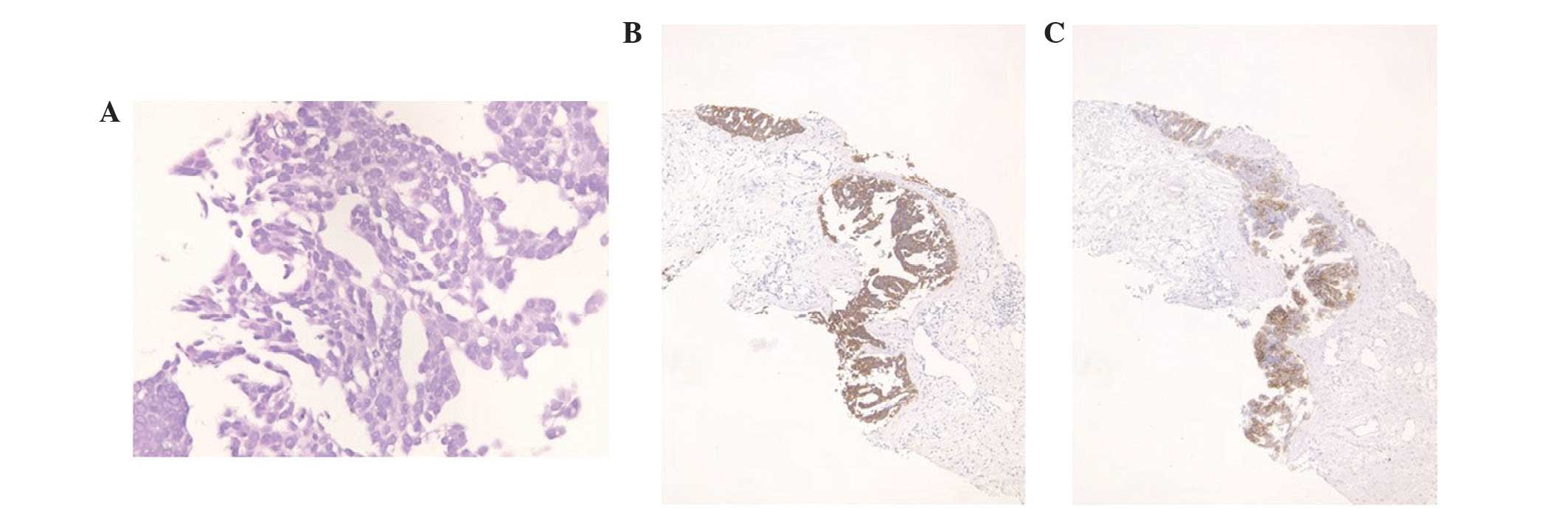
CT-guided paraaortic lymph-node biopsy. This revealed a background
of sclerotic and edematous stoma, the tumor cells proliferated with
papillary and glandular structures, and exhibited hyperchromatic
nuclei, heterogeneity in nuclear shape and size with conspicuous
nucleoli (Fig. 2A). Taken together,
these findings were consistent with a diagnosis of grade 2 serous
carcinoma. The cells were positive for cytokeratin (CK)7 (Fig. 2B), CA125 (Fig. 2C), estrogen receptors (ER), BerEP4 and
Wilms' tumor protein (WT)-1. They were negative for CK20, CK5/6,
caudal type homeobox (CDX)2, thyroid transcription factor-1,
carbohydrate antigen 19-9, progesterone receptors (PR), p53,
calretinin, and gross cystic disease fluid protein 15. These
immunohistochemical findings were consistent with an ovarian tumor
origin.
The patient was referred to Shimane University
Faculty of Medicine for further examination and treatment. Magnetic
resonance imaging (MRI) and a metastatic workup, including positron
emission tomography (PET) were performed. PET-CT revealed abnormal
fluorodeoxyglucose uptake in the area of the paraaortic lymph
nodes, the ovarian tumor and the pancreatic tumor. MRI revealed a 6
cm complex cystic mass in the area of the tail of the pancreas. The
possible diagnoses included primary ovarian carcinoma with a
metastatic pancreatic tumor, primary pancreatic cancer with a
metastatic ovarian tumor, and double primary cancers of the ovary
and pancreas.
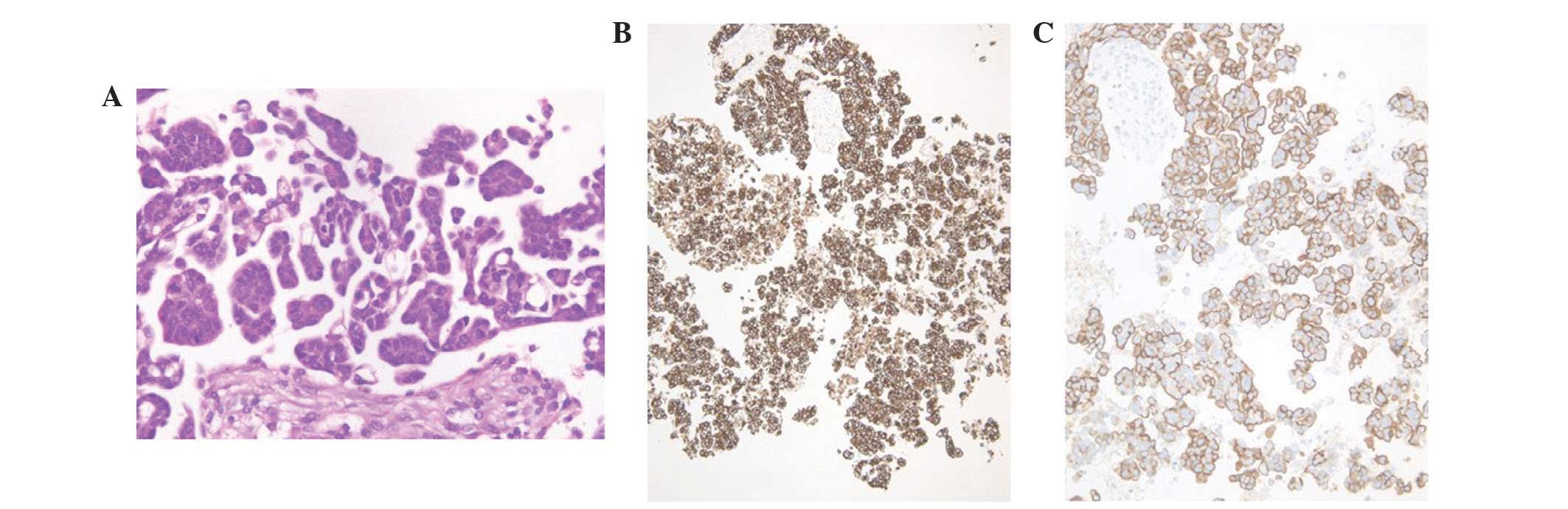
EUS-guided FNA cytology was performed in order to
further evaluate the pathology of the pancreatic mass. This
revealed a background of coagulation necrosis, that the tumor cells
proliferated with papillary to micropapillary and small tubular
structures. Psammoma bodies were also observed. Nuclei of tumor
cells are hyperchromatic, with an irregular shape and size, with
conspicuous nucleoli (Fig. 3A). The
tumor cells stained positive for CK7 (Fig. 3B), CK20, CA125 (Fig. 3C) and ER. PR and WT-1 were weakly
positive, and carbohydrate antigen 19-9 and CD10 were partially
expressed. The cells were negative for maspin, CDX2 and CEA.
Notably, these findings were consistent with an ovarian origin.
Together with the paraaortic findings, the likely diagnosis
appeared to be grade 2 serous carcinoma from an ovarian origin.
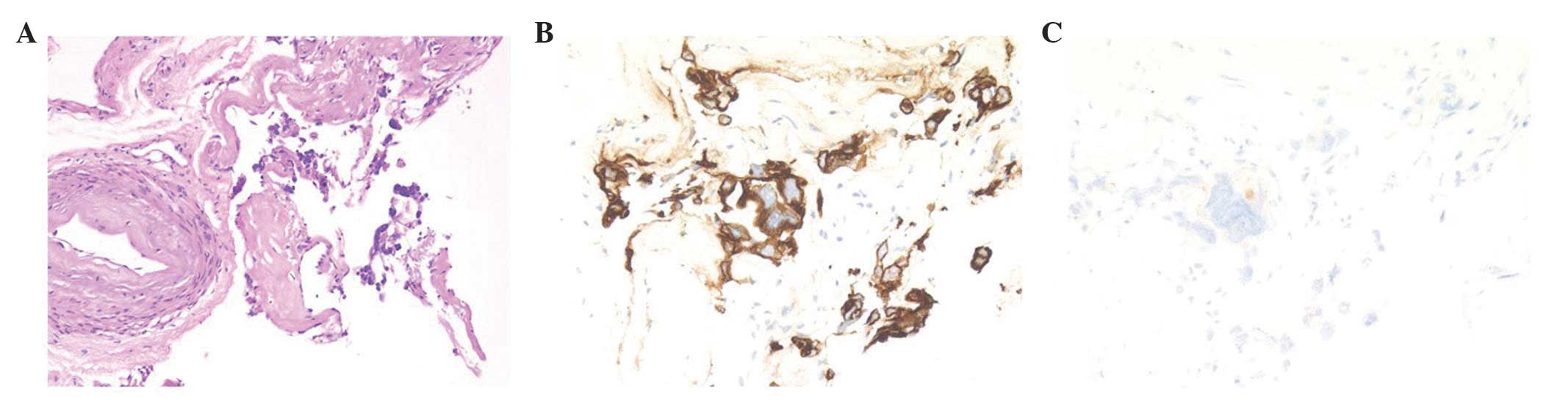
To confirm the origin of these malignancies, a
needle biopsy of the ovarian tumor was performed. The smear
revealed serous carcinoma (Fig. 4A)
and the results of immunostaining were similar to those of the
paraaortic lymph node. The tumor cells were stained positive for
CK7 (Fig. 4B), and weakly positive
for CK20, CA125 (Fig. 4C), CA19-9,
WT-1, and CD10. The cells were negative for p53, maspin, CDX2 and
CEA. These pathological and immunohistochemical findings proved to
be a match for the ovarian tumor. It was concluded that the mass
most likely originated from the ovary and not the pancreas.
Curative surgical therapy was contraindicated in
this patient as a result of the location of the metastasis, the
tail of the pancreas, an area very difficult to surgically resect.
The patient was treated with taxol and carboplatin chemotherapy. At
the time of this report, the patient is alive and tolerating her
chemotherapy well.
Discussion
Ovarian cancer is the most commonly fatal
gynecological malignancy in Europe and the United States (6). These tumors can metastasize by the
intraperitoneal route, the hematogenous route and through lymphatic
channels (7), with common metastasis
sites, including the pleura, liver, skin, lungs, central nervous
system, spleen, bone and breast. It is very rare for ovarian
cancer, or for any cancer, to metastasize to the pancreas (1,2). When
pancreatic metastases do occur, they usually originate from the
kidney, lung, breast, gastrointestinal tract, or from melanoma.
It is highly important to confirm whether a
pancreatic tumor is primary or secondary, since treatment differs
according to the origin of the malignancy. However, given the low
incidence of pancreatic metastasis, it is very difficult to
differentiate a primary pancreatic neoplasm from a metastatic
malignancy. The symptoms and signs are similar, and radiological
imaging is unable to differentiate primary from secondary lesions
(8).
In the present patient, pathological and
immunohistochemical examination of a needle-aspiration biopsy of
the ovarian tumor, CT-guided paraaortic lymph biopsy and EUS-guided
FNA biopsy of the pancreatic tumor were helpful to confirm the
diagnosis. A biopsy of a metastatic tumor can reveal a highly
likely place of origin; however, it is not precise. To confirm the
origin of a tumor, biopsy of the likely culprit is required.
Unfortunately, performing an ovarian-tumor biopsy is generally
contraindicated owing to the risk of disseminating malignant cells.
In the present patient, an ovarian origin would mean that the
carcinoma was International Federation of Gynecology and Obstetrics
stage IV. Therefore, dissemination would not change the staging,
and the present study was comfortable performing a biopsy of the
ovarian tumor to obtain a definitive diagnosis.
It is rare that pancreatic resection is indicated
for a metastatic tumor (3). The
procedure has not been shown to improve survival or quality of life
(3). In the present patient with
ovarian cancer and a metastatic pancreatic tumor, chemotherapy was
selected as the primary treatment as a result of the great
difficulty in surgically resecting the metastatic location, the
tail of the pancreas.
Pathological and immunohistochemical examination of
a lymph-node biopsy, an EUS-guided FNA biopsy of the pancreatic
tumor and needle-aspiration biopsy of the suspected primary tumor
is useful to make an exact diagnosis and determine the proper
treatment in patients with simultaneous pancreatic and other-site
tumors. This is particularly true when it cannot be determined
whether the pancreatic tumor is primary or secondary in origin.
References
|
1.
|
Hiotis SP, Klimstra DS, Conlon KC and
Brennan MF: Results after pancreatic resection for metastatic
lesions. Ann Surg Oncol. 9:675–679. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Nakamura E, Shimizu M, Itoh T and Manabe
T: Secondary tumors of the pancreas: Clinicopathological study of
103 autopsy cases of Japanese patients. Pathol Int. 51:686–690.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Konstantinidis IT, Dursun A, Zheng H,
Wargo JA, Thayer SP, Fernandez-del Castillo C, Warshaw AL and
Ferrone CR: Metastatic tumors in the pancreas in the modern era. J
Am Coll Surg. 211:749–753. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Gunay Y, Demiralay E and Demirag A:
Pancreatic metastasis of high-grade papillary serous ovarian
carcinoma mimicking primary pancreas cancer: A case report. Case
Rep Med. 2012:9432802012.PubMed/NCBI
|
|
5.
|
Hadzri MH and Rosemi S: Pancreatic
metastases from ovarian carcinoma-diagnosis by endoscopic
ultrasound-guided fine needle aspiration. Med J Malaysia.
67:210–211. 2012.PubMed/NCBI
|
|
6.
|
Wingo PA, Tong T and Bolden S: Cancer
statistics, 1995. CA Cancer J Clin. 45:8–30. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Rose PG, Piver MS, Tsukada Y and Lau TS:
Metastatic patterns in histologic variants of ovarian cancer. An
autopsy study. Cancer. 64:1508–1513. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Charnsangavej C and Whitley NO: Metastases
to the pancreas and peripancreatic lymph nodes from carcinoma of
the right side of colon: CT findings in 12 patients. AJR Am J
Roentgenol. 160:49–52. 1993. View Article : Google Scholar : PubMed/NCBI
|