Introduction
Calcifying fibrous pseudotumors (CFP) are rare,
benign soft tissue neoplasms. These lesions are characterized by
hypocellular, densely hyalinized collagenization with variably
prominent mononuclear inflammatory infiltrate and scattered
psammomatous and/or dystrophic calcification (1). The etiology of CFT is unknown. A few
were considered to evolve from inflammatory myofibroblastic tumors
(IMTs), but larger studies have failed to confirm this, and
ultrastructural studies revealed fibroblastic features (2,3). CFPs do
not have a propensity to metastasize, and are often treated by
local excision with clear margins (4). Although there is a low risk for
recurrence, consideration should be given to re-excision, should
this occur. Prognoses have been observed to be excellent with
surgical treatment alone (5).
The aim of the present study was to present a
further case of CFP of the adrenal gland, and to provide useful
information on this rare type of tumor.
Case presentation
A 32-year-old male presented to our hospital with a
tumor-like lesion in the area of the left adrenal gland detected by
ultrasound during a routine check-up several days prior. There were
no clinical symptoms or positive signs on physical examination.
There was no family history or relevant medical history. The
adrenal hormones including catecholamines, cortisol,
adrenocorticotropic hormone, renin, angiotensin and aldosterone,
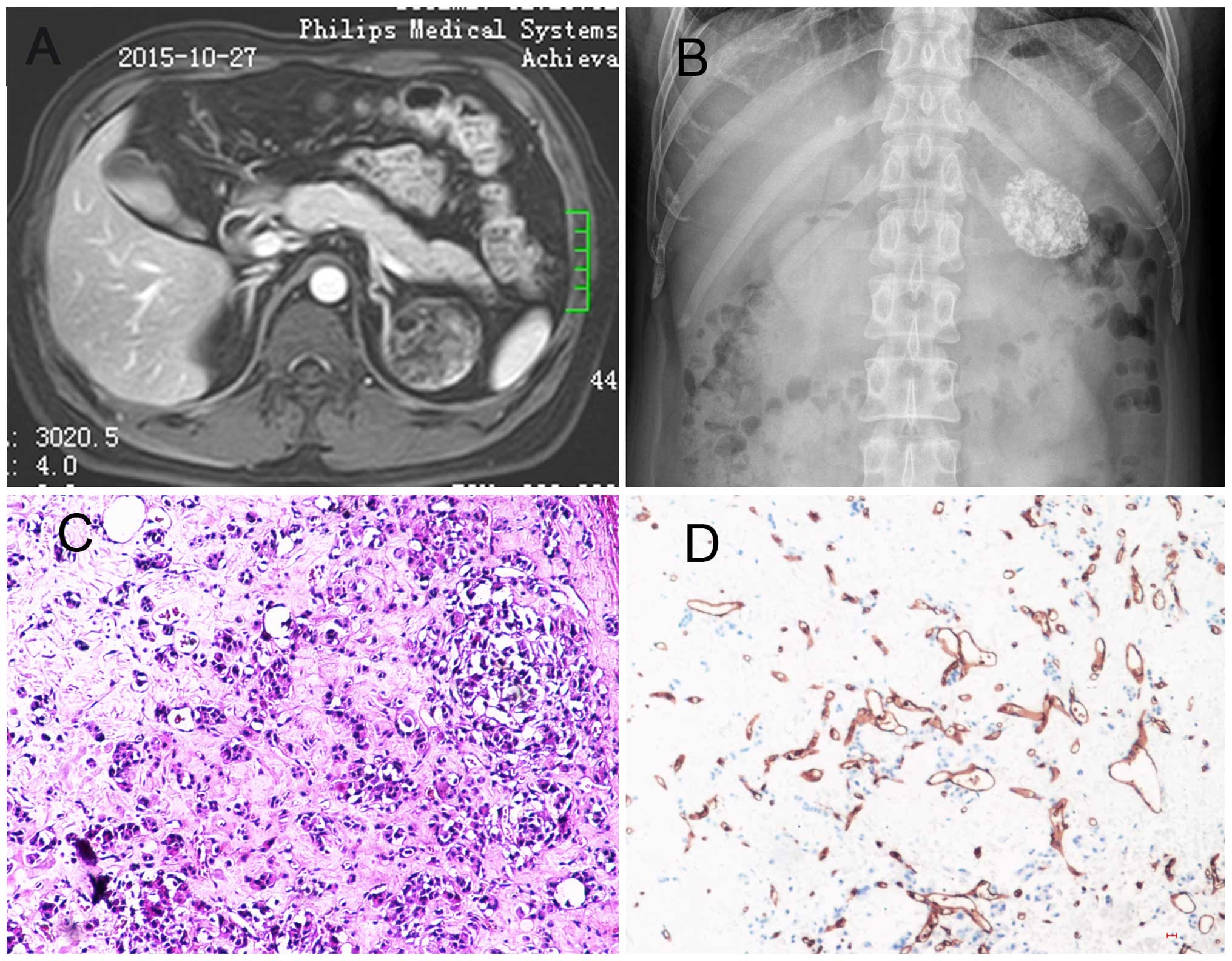
were all within the normal range. Contrast-enhanced magnetic
resonance imaging revealed a solitary, well-circumscribed mass,
sized 4.4×4.6×4.1 cm, in close proximity to the medial arterial
branch of the left adrenal gland. T1-weighted images showed a
mixture of low and equal signal intensity. T2-weighted images with
fat suppression showed areas of low and high signal intensity. On
enhanced T1-weighted images, the mass exhibited significant
heterogeneous enhancement (Fig. 1A).
A kidney/ureter/bladder X-ray showed a large stone or calcified
lesion in the left adrenal area (Fig.
1B). Other routine investigations, including a chest
radiograph, were normal. The patient underwent left retroperitoneal
laparoscopic adrenalectomy. Histological examination showed that
the tumor consisted of sheets of varying amountS of inflammatory
cells; interstitial fibrosis and psammomatous calcifications were
also observed (Fig. 1C).
Immunohistochemical examination revealed diffuse staining for CD34,
CD31, cytokeratin, synapsin and partially for inhibin (Fig. 1D). The cells were negative for all
other antibodies tested, including chromogranin A, calretenin and
Ki67. These results confirmed the diagnosis of CFP of the adrenal
gland. After treatment, the patient remained recurrence-free at 3
months.
Discussion
CFP is a rare benign lesion histologically
characterized by dense hyalinization, fibrous proliferation,
inflammatory infiltration by mononuclear cells and scattered
psammomatous and/or dystrophic calcificationS (6–8). A review
of the literature reveals that CFPS are rare, with the sites of
involvement limited to the lung, mediastinum, myocardium, pleura
and adrenal gland (2,9–11). To the
best of our knowledge, this is the third case of this type of
lesion occurring in the adrenal gland published in the english
literature. The previous two cases were reported in 2007 and 2001
(12,13). One of those cases was a 10-year-old
female patient with intermittent frontal headaches and a
retroperitoneal mass. The pathological findings revealed a
spindle-cell neoplasm forming irregular bundles and fascicles,
without microscopic atypia. Chronic lymphoplasmocytic inflammatory
cells forming prominent focal aggregates were also present
(13); the other case was a
32-year-old female patient who presented with a chief complaint of
vague abdominal discomfort. The identified lesion was
well-circumscribed and was composed of dense, poorly cellular
collagenous tissue, scattered spindle cells, an inflammatory
infiltrate consisting of plasma cells and lymphocytes, and
dystrophic calcifications (12).
Following surgical resection, the second patient remained
recurrence-free at 22 months; however, there are no follow-up data
on the first case. CFP should be distinguished from other tumor
occurring in the adrenal gland. The principal consideration in the
differential diagnosis of CFP of the adrenal gland is IMT. Although
originally described in the lung, IMT has also been recognized in a
wide variety of extrapulmonary sites, including the adrenal gland
(7,14). The differentiation diagnosis between
them has demonstrated chromosomal rearrangements involving the
anaplastic lymphoma kinase gene located at 2p23 in a significant
subset of cases (14). CFP should
also be differentiated from other uncommon mesenchymal tumors that
may originate in the adrenal gland, including benign peripheral
nerve sheath tumors and solitary fibrous tumor (14). Immunohistochemistry is suitable for
the purpose of differentiation, since CFP lacks S-100 protein
reactivity (14). The aim of the
present study was to present another case of CFP of the adrenal
gland and provide useful information on this rare type of
tumor.
References
|
1
|
Fetsch JF, Montgomery EA and Meis JM:
Calcifying fibrous pseudotumor. Am J Surg Pathol. 17:502–508. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nascimento AF, Ruiz R, Hornick JL and
Fletcher CD: Calcifying fibrous ‘pseudotumor’: clinicopathologic
study of 15 cases and analysis of its relationship to inflammatory
myofibroblastic tumor. Int J Surg Pathol. 10:189–196. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jaiswal SS, Agrawal A, Sahai K and Nair
SK: Large retroperitoneal calcifying fibrous tumor. Med J Armed
Forces India. 69:1842013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mangat A, Schiller C, Mengoni P, Reynolds
C and Jeruss JS: Calcifying fibrous pseudotumor of the breast.
Breast J. 15:299–301. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Maeda A1, Kawabata K and Kusuzaki K: Rapid
recurrence of calcifying fibrous pseudotumor (a case report).
Anticancer Res. 22:1795–1797. 2001.
|
|
6
|
Rosenthal NS and Abdul-Karim FW: Childhood
fibrous tumor with psammoma bodies. Clinicopathologic features in
two cases. Arch Pathol Lab Med. 112:798–800. 1988.PubMed/NCBI
|
|
7
|
Lau SK and Weiss LM: Calcifying fibrous
tumor of the adrenal gland. Hum Pathol. 38:656–659. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Eftekhari F, Ater JL, Ayala AG and
Czerniak BA: Case report: Calcifying fibrous pseudotumour of the
adrenal gland. Br J Radiol. 74:452–454. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shinohara N, Nagano S, Yokouchi M,
Arishima Y, Tabata K, Higashi M, Kitajima S, Yonezawa S and Komiya
S: Bilobular calcifying fibrous pseudotumor in soleus muscle: A
case report. J Med Case Rep. 5:4872011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Minerowicz C, Jagpal S, Uppaluri L, Deen M
and Langenfeld J: Calcifying fibrous pseudotumor of the pleura. Am
J Respir Crit Care Med. 192:e57–e58. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Özkan S, Demiraǧ F, Yekeler E and
Karaoǧlanoǧlu N: Calcifying fibrous pseudotumor of lungs. Turk J
Med Sci. 44:901–903. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chang JW, Kim JH and Maeng YH: Calcifying
fibrous pseudotumor of the anterior mediastinum. Korean J Thorac
Cardiovasc Surg. 44:318–320. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chan JK1, Cheuk W and Shimizu M:
Anaplastic lymphoma kinase expression in inflammatory pseudotumors.
Am J Surg Pathol. 25:761–768. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Van Dorpe J, Ectors N, Geboes K, D'Hoore A
and Sciot R: Is calcifying fibrous pseudotumor a late sclerosing
stage of inflammatory myofibroblastic tumor? Am J Surg Pathol.
23:329–335. 1999. View Article : Google Scholar : PubMed/NCBI
|