Introduction
Endometrial cancer is the most common gynecological
cancer type in developed countries (1). According to the pathological, hormonal
and molecular characteristics, it is classified into two types:
Type 1 includes grade 1 (G1) and grade 2 (G2) endometrioid
adenocarcinomas, while type 2 includes grade 3 (G3) endometrioid
adenocarcinoma and other types with a specific histology, including
serous and clear cell carcinoma (2).
In addition, carcinosarcoma is currently defined as one particular
subtype of epithelial endometrial carcinoma that shares similar
behavior with type 2 endometrial cancer (3) and, thus, carcinosarcoma must be staged
according to the International Federation of Gynecology and
Obstetrics (FIGO) staging system for carcinoma of the endometrium,
not for uterine sarcoma.
While endometrial cancer patients with stage I–II
disease achieve a favorable outcome with surgery alone, patients
with advanced disease or recurrence show poor survival. Several
clinicopathological factors are used for the classification of
relapse risks, including the histological type, grade, depth of
myometrial invasion, lymph node metastasis and lymph-vascular space
involvement (LVSI) (2). Furthermore,
previous studies revealed that carcinosarcoma, even with
early-stage disease, is associated with a much lower survival rate
compared with those of endometrioid adenocarcinoma (4,5). For
patients belonging to high-risk groups defined by
clinicopathological parameters, either adjuvant chemotherapy or
radiotherapy has been applied. However, the criteria for selecting
patients that should receive adjuvant therapy remain controversial
(2,6).
Therefore, the identification of additional prognostic markers may
be helpful for the individualization of adjuvant therapy and for
improving the survival of patients with endometrial cancer and
carcinosarcoma.
18F-fluoro-2-deoxy-D-glucose-positron
emission tomography (FDG-PET) with computed tomography (CT) is a
well-established imaging modality for diagnosing and staging
numerous types of cancer. In gynecological malignancies, previous
studies revealed that the maximum standardized uptake value
(SUVmax), a quantitative measurement of the tissue
deoxyglucose metabolic rate measured on FDG-PET/CT, may be a useful
parameter, not only for evaluating malignancy, but also for
assessing the prognosis of patients with ovarian (7,8) and
cervical cancer (9,10). In endometrial neoplasms, several
previous reports demonstrated the usefulness of SUVmax
for preoperative risk stratification (11,12),
although its prognostic impact remains controversial (13–16), and
it remains to be sufficiently studied in patients with uterine
carcinosarcoma.
The present study investigated the SUVmax
of primary tumors measured by preoperative FDG-PET/CT in patients
with endometrial cancer and uterine carcinosarcoma, and attempted
to clarify whether the SUVmax is an indicator for risk
stratification and prognosis determination in these patients.
Patients and methods
Patient selection
A total of 75 patients with endometrial neoplasms
who underwent preoperative FDG-PET/CT at Wakayama Minami Radiology
Clinic (Wakayama, Japan), followed by the surgical resection of
tumors at Wakayama Medical University Hospital (Wakayama, Japan)
between January 2008 and January 2013, were included in the present
study. All patients underwent a total abdominal hysterectomy and
bilateral salpingo-oophorectomy, followed by surgical staging,
including peritoneal washing cytology and pelvic and/or para-aortic
lymph-node dissection. The median age of the patients was 59 years
(range, 37–85 years). All patients were staged according to FIGO
2008 criteria: 50 were stage I (39 were IA, 11 were IB), 8 were
stage II, 13 were stage III and 4 were stage IV. The postoperative
pathological diagnosis was assigned according to the criteria of
the World Health Organization classification: 31 were G1, 19 were
G2 and 5 were G3 endometrioid adenocarcinoma, 8 were specific types
of histology including 3 serous, 3 clear cell and 2 mucinous
carcinomas, and 12 were carcinosarcoma. The evaluation of the
pathological factors, including lymph node metastasis, LVSI and the
depth of myometrial invasion, was also performed by pathologists.
In the present study, patients with FIGO stage IA with specific
histological types or carcinosarcoma and all patients with FIGO
stage IB or more advanced-stage disease received postoperative
adjuvant chemotherapy with six cycles of paclitaxel plus
carboplatin. Patients who underwent any form of radiation therapy
were excluded from the present study. The present study was
approved by the Ethics Committee of Wakayama Medical University
(approval no. 1792).
FDG-PET/CT and imaging analysis
PET studies were performed with a PET scanner
(SET-3000BCT/L; Shimadzu, Kyoto, Japan) with an axial resolution of
3.9 mm and a 20 cm field of view, as described in our previous
study (8). At the time of the tracer
injection, all patients had fasted for at least 5 h and had blood
glucose levels <150 mg/dl. Images were captured from the top of
the head to the mid-thigh 50 min after the intravenous injection of
18F-FDG (2.6 MBq/kg body weight). Following the
completion of PET, CT images were obtained using a multidetector
row CT scanner (Brilliance 64; Philips Medical Systems, Best, The
Netherlands). Fusion images of PET and CT were made using a
Workstation (EV Insite; PSP Corporation, Tokyo, Japan). FDG-PET/CT
images were evaluated by a nuclear medicine physician/radiologist.
For each study, the SUVmax of the primary tumor was
measured. SUV is a semi-quantitatively analyzed value of
radiotracer uptake and is defined as the ratio of radiotracer
activity per milliliter of tissue to the activity in the injected
dose corrected for decay and the patient's body weight.
Data analysis
The SUVmax among the groups were compared
using the Mann-Whitney U test. Receiver operating characteristic
(ROC) curve analysis was performed in order to determine the
cut-off values of the SUVmax. The overall survival (OS)
was calculated from the date of surgery until the patient succumbed
to mortality, and the progression-free survival (PFS) was
calculated from the date of surgery until that of recurrence. The
median follow-up period was 26.4 months, ranging between 3 and 59
months. Survival analyses were performed according to the
Kaplan-Meier method. A comparison of the survival between groups
was performed using the log-rank test. The Cox proportional-hazard
regression model was used for multivariate analyses to explore the
impact of individual variables on survival. P<0.05 was
considered to indicate a statistically significant difference.
Results
Correlation between the
SUVmax of the primary tumor and clinicopathological
factors
Clinicopathological characteristics of the 75
patients and the median SUVmax of the primary tumor in
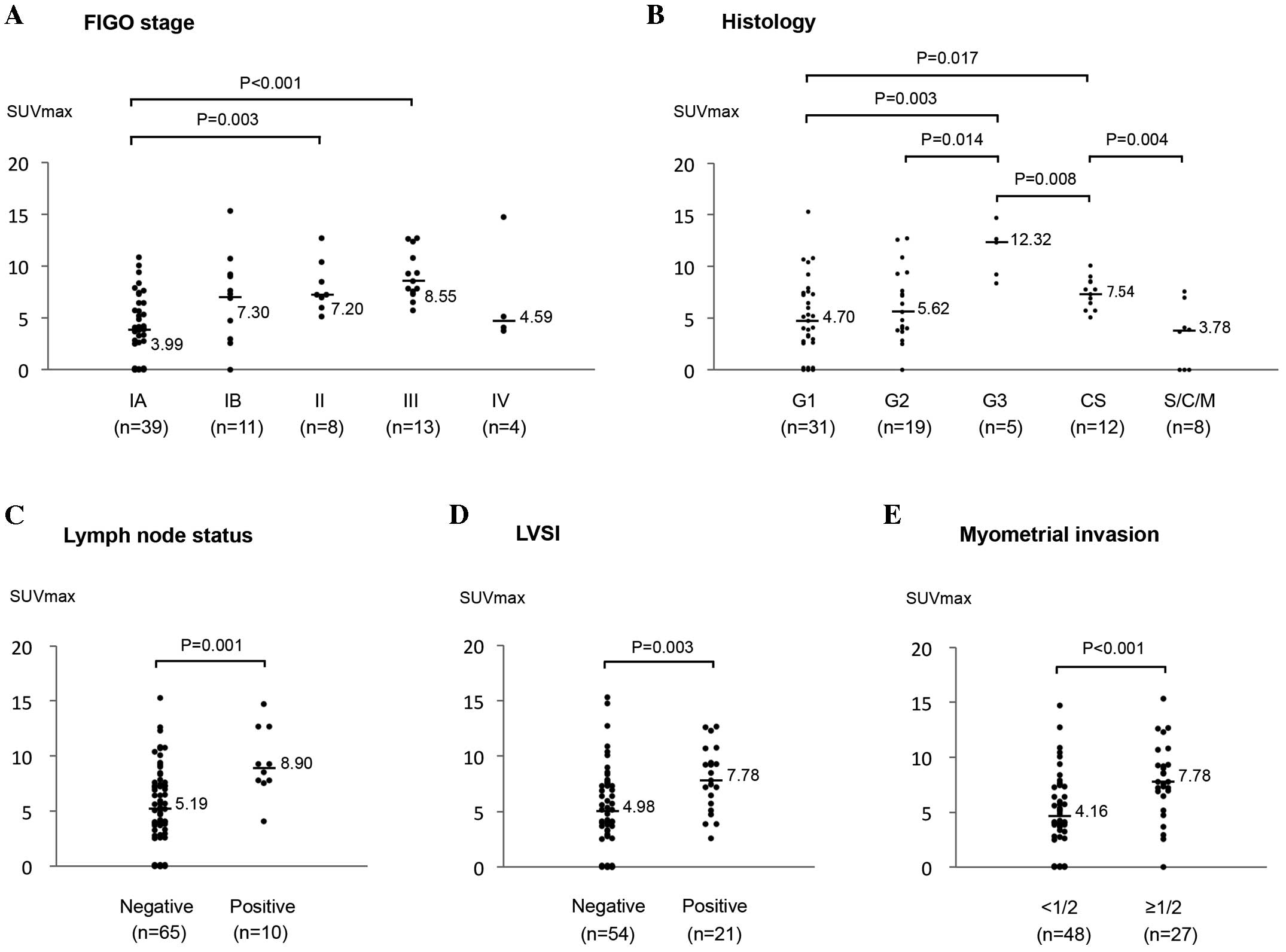
each group are shown in Table I. As
shown in Fig. 1A, the
SUVmax values for stage II and III were significantly
higher compared with those for stage IA (P=0.003 and P<0.001,
respectively), however, not those for stage IB. No significant
difference in the SUVmax was observed between patients
with stage IV and the others, although the number of stage IV
patients was only 4.
 | Table I.Clinicopathological characteristics
and the median SUVmax in 75 patients with endometrial
cancer and uterine carcinosarcoma. |
Table I.
Clinicopathological characteristics
and the median SUVmax in 75 patients with endometrial
cancer and uterine carcinosarcoma.
| Characteristic | Patient number
(%) | Median
SUVmax |
|---|
| Total | 75 | 5.71 |
| Age |
|
|
|
<60 | 41 (54.7) | 5.33 |
|
≥60 | 34 (45.3) | 6.70 |
| FIGO stage |
|
|
| IA | 39 (52.0) | 3.99 |
| IB | 11 (14.7) | 7.30 |
| II | 8
(10.7) | 7.20 |
|
III | 13 (17.3) | 8.55 |
| IV | 4 (5.3) | 4.59 |
| Histology |
|
|
| G1 | 31 (41.3) | 4.70 |
| G2 | 19 (25.3) | 5.62 |
| G3 | 5 (6.7) | 12.32 |
|
S/C/M | 8 (10.7) | 3.78 |
| CS | 12 (16.0) | 7.54 |
| LN status |
|
|
|
Negative | 65 (86.7) | 5.19 |
|
Positive | 10 (13.3) | 8.90 |
| LVSI |
|
|
|
Negative | 54 (72.0) | 4.98 |
|
Positive | 21 (28.0) | 7.78 |
| Myometrial
invasion |
|
|
|
<1/2 | 48 (64.0) | 4.16 |
|
≥1/2 | 27 (36.0) | 7.78 |
Next, the correlation between the SUVmax
and histology was investigated (Fig.
1B). The SUVmax for G3 endometrioid adenocarcinoma
was significantly higher compared with those for stage G1 and G2
(P=0.003 and P=0.014, respectively). The SUVmax for
carcinosarcoma was also significantly higher compared with those
for stage G1 (P=0.017), and, it was significantly lower compared
with those for G3 (P=0.008). The SUVmax for patients
with specific histological types, including serous, clear cell and
mucinous carcinoma, was lower (median, 3.78), although the number
of patients in this group was low (n=8).
The SUVmax was significantly higher in
patients with a pathologically positive lymph node status (P=0.001;
Fig. 1C) and a positive LVSI
(P=0.003; Fig. 1D). In addition, the
SUVmax in patients with deep (≥1/2) myometrial invasion
was significantly higher compared with those in patients with
<1/2 (P<0.001; Fig. 1E).
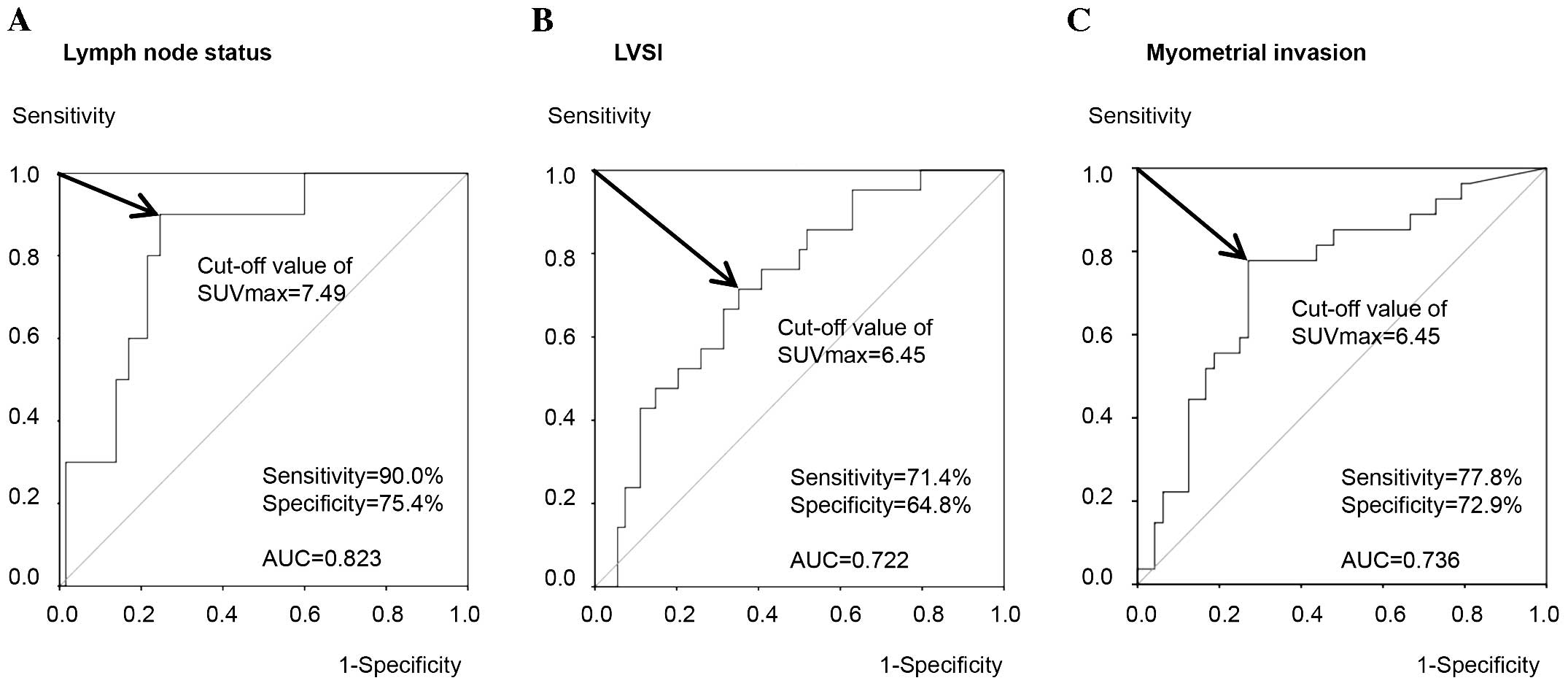
Cut-off values of the
SUVmax for predicting the presence of risk factors
The present study attempted to determine the optimal
cut-off values of the SUVmax for risk stratification.
ROC curve analysis demonstrated that the optimal cut-off value of
the SUVmax for predicting a pathologically positive
lymph node status was 7.49, with a sensitivity of 90.0%,
specificity of 75.4% and AUC of 0.823 (Fig. 2A). By contrast, the cut-off value of
the SUVmax for predicting a positive LVSI was 6.45, with
a sensitivity of 71.4%, specificity of 64.8% and AUC of 0.722
(Fig. 2B). Similarly, ROC curve
analysis revealed that the optimal cut-off values of the
SUVmax for myometrial invasion of ≥1/2 was 6.45 with a
sensitivity of 77.8%, specificity of 72.9% and AUC of 0.736
(Fig. 2C). These results indicated
that the primary tumor SUVmax may be predictive for the
presence of these clinicopathological risk factors using optimal
cut-off values with relatively high sensitivity and
specificity.
Correlation of the SUVmax
of the primary tumor with patient survival
Firstly, the present study compared the OS and PFS
rates among the five groups with G1, G2, G3 endometrioid
adenocarcinoma, a specific histology, and carcinosarcoma (Fig. 3). The OS in patients with
carcinosarcoma was significantly lower compared with in those with
G1 (P<0.001), G2 (P<0.001) or a specific histology (P=0.024),
however, not those with G3 (P=0.307). Similarly, the PFS in
patients with carcinosarcoma was significantly lower compared with
that in those with G1 (P<0.001), G2 (P<0.001) or a specific
histology (P=0.028), and there was a trend toward a lower PFS in
carcinosarcoma as compared with that in G3, although it did not
reach a significant difference (P=0.134).
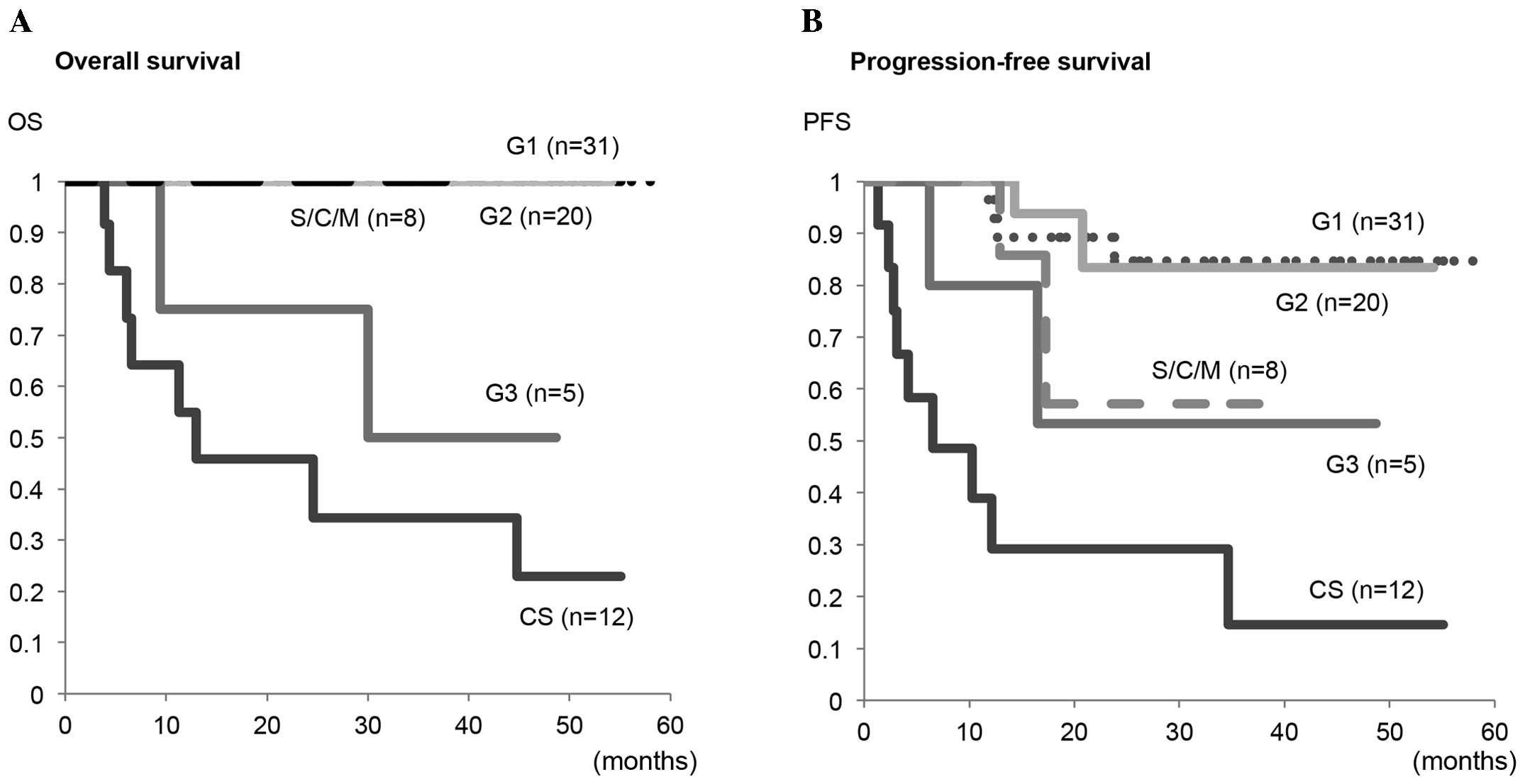 | Figure 3.Kaplan-Meier plots for (A) OS and (B)
PFS in G1, G2 and G3 endometrioid adenocarcinomas, S/C/M and CS.
S/C/M included serous (n=3), clear cell (n=3) and mucinous
adenocarcinomas (n=2). Significant differences in the OS were
observed in CS vs. G1 (P<0.001), CS vs. G2 (P<0.001) and CS
vs. S/C/M (P=0.024), however, not in CS vs. G3 (P=0.307).
Significant differences in PFS were observed in CS vs. G1
(P<0.001), CS vs. G2 (P<0.001) and CS vs. S/C/M (P=0.028),
however, not in CS vs. G3 (P=0.134). OS, overall survival; PFS,
progression-free survival; S/C/M, serous/clear cell/mucinous
adenocarcinoma; CS, carcinosarcoma. |
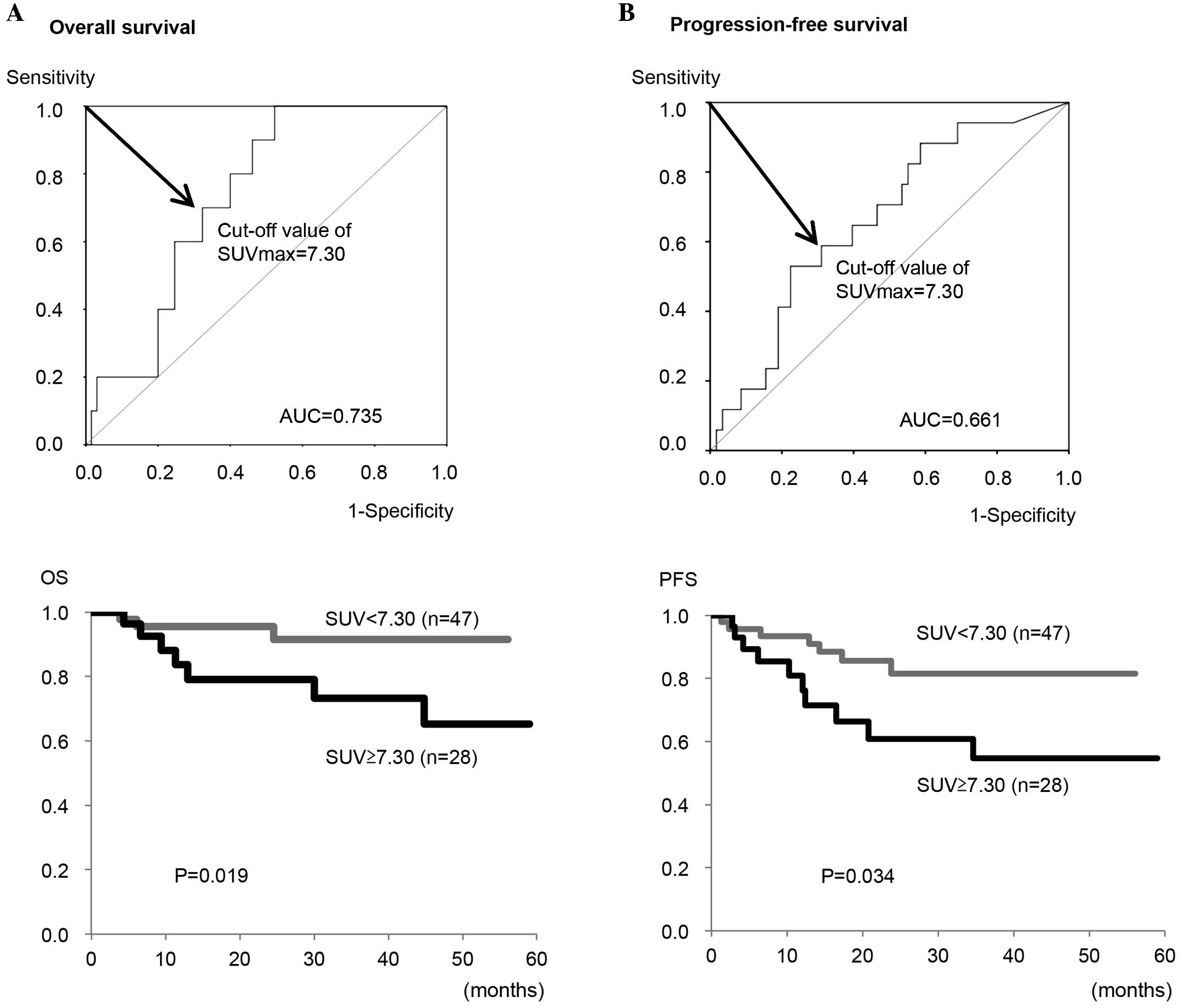
Next, the optimal cut-off value of the
SUVmax for predicting OS and PFS in all patients was
determined to be 7.30 from the ROC curve analysis (Fig. 4). Using this cut-off value, the OS
rate of patients with a high SUVmax (≥7.30) was
significantly lower compared with patients with a low
SUVmax (<7.30) (P=0.019; Fig. 4A). Similarly, the PFS rate of the
patients with a high SUVmax (≥7.30) was significantly
lower compared with the patients with a low SUVmax
(<7.30) (P=0.034; Fig. 4B).
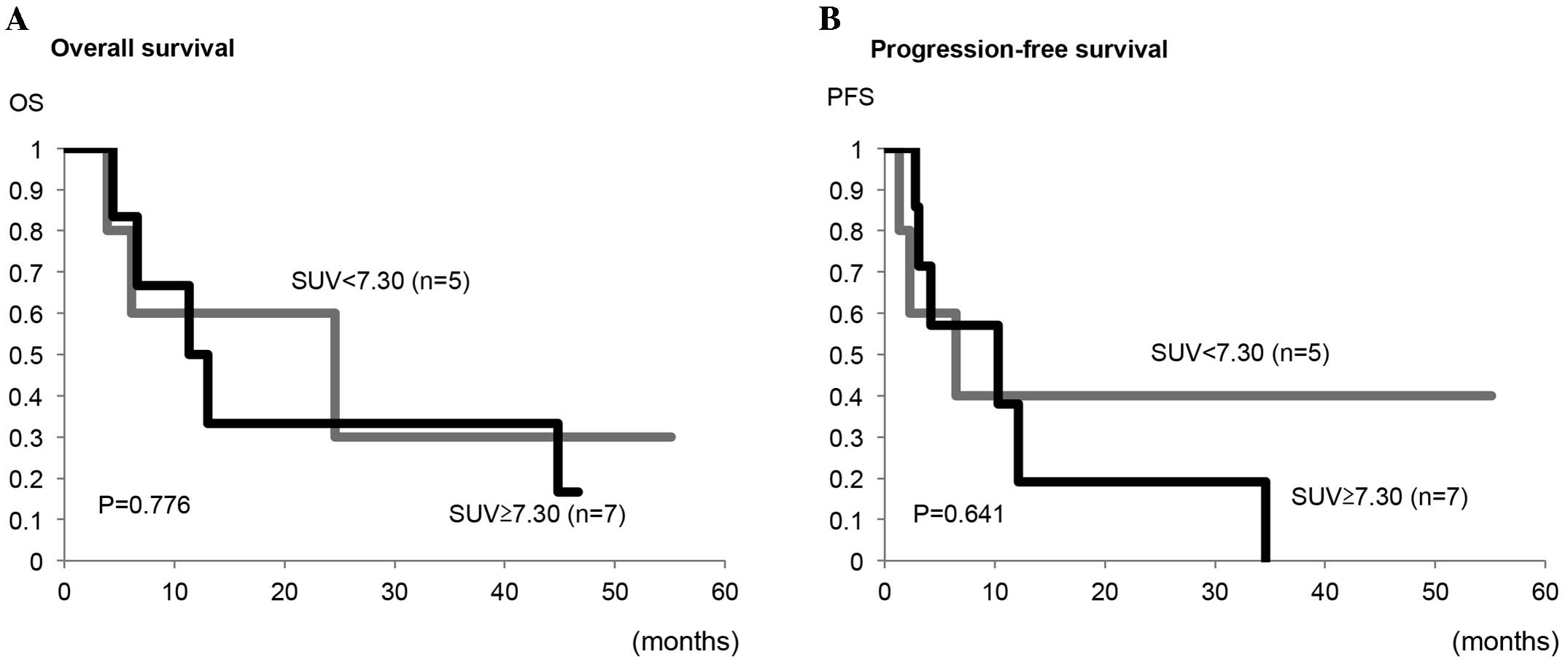
Furthermore, the present study analyzed the impact of the
preoperative SUVmax on the prognosis of patients with
carcinosarcoma alone. As shown in Fig.
5, no significant differences in the OS or PFS rates between
patients with a high SUVmax and those with a low
SUVmax were observed (P=0.776 and P=0.641,
respectively).
Finally, to clarify whether the SUVmax
can be an independent prognostic factor, multivariate analyses were
performed. As shown in Table II,
multivariate analysis demonstrated that the FIGO stage, histology
and myometrial invasion, however, not SUVmax, were
independent prognostic factors for impaired PFS in all 75 patients,
including any adenocarcinomas and carcinosarcomas. By contrast,
when analyzed in 55 endometrioid adenocarcinoma (G1, G2 and G3)
patients alone (Table III), a high
SUVmax was an independent prognostic factor for
predicting impaired PFS (hazard ratio=12.453; P=0.002).
| Table II.Univariate and multivariate analyses
of the clinicopathological factors and SUVmax for
progression-free survival in all 75 patients. |
Table II.
Univariate and multivariate analyses
of the clinicopathological factors and SUVmax for
progression-free survival in all 75 patients.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Characteristic | P-value | Hazard ratio | 95% CI | P-value |
|---|
| Age |
|
| <60
vs. ≥60 |
0.242 | 2.092 | 0.679–6.446 | 0.198 |
| FIGO stage |
|
| I/II
vs. III/IV | <0.001 | 4.969 | 1.699–14.527 | 0.003 |
| Histology |
|
| G1/G2
vs. G3/SCM/CS | <0.001 | 2.956 | 1.004–8.703 | 0.049 |
| LN status |
|
|
Negative vs. positive | <0.001 | 1.283 | 0.320–5.139 | 0.725 |
| LVSI |
|
|
Negative vs. positive |
0.029 | 1.107 | 0.356–3.445 | 0.860 |
| Myometrial
invasion |
|
| <1/2
vs. ≥1.2 | <0.001 | 3.070 | 1.114–8.457 | 0.030 |
|
SUVmax |
|
|
<7.30 vs. ≥7.3 |
0.034 | 0.984 | 0.311–3.118 | 0.978 |
|
≥7.30 |
|
| Table III.Univariate and multivariate analyses
of the clinicopathological factors and SUVmax for
progression-free survival in 55 patients with endometrioid
adenocarcinoma. |
Table III.
Univariate and multivariate analyses
of the clinicopathological factors and SUVmax for
progression-free survival in 55 patients with endometrioid
adenocarcinoma.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Characteristic | P-value | Hazard ratio | 95% CI | P-value |
|---|
| Age |
|
| <60
vs. ≥60 |
0.600 |
3.234 | 0.438–23.892 | 0.250 |
| FIGO stage |
|
| I/II
vs. III/IV | <0.001 |
1.961 | 0.115–33.412 | 0.642 |
| Histology |
|
| G1/G2
vs. G3/SCM/CS |
0.050 |
0.876 | 0.082–9.405 | 0.913 |
| LN status |
|
|
Negative vs. positive | <0.001 |
2.288 | 0.245–21.376 | 0.468 |
| LVSI |
|
|
Negative vs. positive | <0.005 |
2.515 | 0.208–30.412 | 0.468 |
| Myometrial
invasion |
|
| <1/2
vs. ≥1/2 | <0.017 |
2.090 | 0.168–26.049 | 0.567 |
|
SUVmax |
|
|
<7.30 vs. ≥7.30 | <0.001 | 12.453 | 2.501–62.016 | 0.002 |
Discussion
Previous studies demonstrated that a high FDG uptake
within the primary tumors evaluated by the SUVmax on
PET-CT can be associated with clinicopathological factors and
aggressive biological characteristics in endometrial cancer
(11,12), although its impact on disease
recurrence or OS remains controversial (13–16).
Nakamura et al (11) reported
that the SUVmax of the primary tumor was correlated with
the histological grade. Antonsen et al (12) showed that a high SUVmax was
predictive of risk factors, including deep myometrial invasion, an
advanced FIGO stage and lymph node metastasis in patients with
endometrial cancer. In terms of the prognostic impact, Nakamura
et al (13) reported that the
SUVmax was an independent prognostic factor for OS,
based on multivariate analysis, however, not for disease-free
survival (DFS), in 106 patients with endometrial cancer, including
9 carcinosarcomas. Similarly, Walentowicz-Sadlecka et al
(14) revealed that the preoperative
SUVmax was an independent prognostic factor of OS in 101
endometrial cancer patients. By contrast, Kitajima et al
(15) demonstrated that the
SUVmax was an independent factor for DFS on multivariate
analysis in 57 patients with G1-G3 endometrioid carcinoma.
Ghooshkhanei et al (16)
showed in their review that the usefulness of the SUVmax
for classifying patients with endometrial cancer into pre-defined
risk groups appears to be limited. To further clarify the clinical
significance of the primary tumor SUVmax on preoperative
PET/CT not only in endometrioid adenocarcinomas, but also in
specific histological types, including carcinosarcoma, the present
study investigated its clinicopathological and prognostic impacts
on these patients.
These results demonstrated that a high
SUVmax of the primary tumor was significantly correlated
with the presence of conventional clinicopathological risk factors,
including histology of G3 or carcinosarcoma, positive lymph node
metastasis, positive LVSI and deep myometrial invasion.
Furthermore, it demonstrated the individual cut-off values of the
SUVmax for predicting the presence of each risk factor
with high sensitivity and specificity based on the ROC curve
analysis. These findings suggested that the preoperative
SUVmax of the primary tumor may be useful for predicting
clinicopathological risk factors and tumor aggressiveness using
optimal cut-off values. In the present study, the SUVmax
in patients with specific histological types, including serous,
clear cell and mucinous carcinomas, was rather low despite their
aggressive characteristics and less favorable prognosis, although
the number of patients in this group was very low (n=8). Our
previous study demonstrated that SUVmax was lower in
patients with ovarian cancer with a clear cell or mucinous
histology (8). Further studies are
required to clarify the FDG uptake and its clinicopathological
significance in specific histological types.
In the present study, based on the results of ROC
curve analysis, it was demonstrated that both the OS and PFS in
patients with a higher (≥7.30) SUVmax were significantly
lower compared with those with a lower (<7.30)
SUVmax. This cut-off value may be easy to use and
helpful for preoperative risk stratification in each patient as an
index, although it may vary among the institutions due to its
dependence on the setting of PET conditions and method of imaging
analysis in each institution. Notably, the multivariate analyses
demonstrated that a high SUVmax was an independent
prognostic factor for impaired PFS when analyzed in G1-G3
endometrioid adenocarcinomas without a specific histology or
carcinosarcoma, however, not when analyzed in all 75 patients
including those specific types. Furthermore, no significant
differences were observed between high and low SUVmax
groups with carcinosarcoma, although the total number of
carcinosarcoma patients eligible for our study was low (n=12).
These findings suggested that the SUVmax of the primary
tumor can be a prognostic indicator of endometrioid adenocarcinoma,
and may be a promising non-invasive biomarker to evaluate the risk
of recurrence, as shown in other previous studies (15,16), while
its prognostic impact on patients with carcinosarcoma or a specific
histology remains to be confirmed. Both the OS and PFS rates in
carcinosarcoma were markedly lower, even in patients with
early-stage disease, as shown in the present study (Fig. 3) and previous studies (4–6). This may
be the reason why the SUVmax was difficult to use to
stratify the recurrence risk in this disease. Further studies on
the prognostic impact of the primary tumor SUVmax in a
large number of carcinosarcoma patients are required.
Previously, several novel metabolic parameters of
FDG-PET/CT, in addition to the SUVmax, were shown to be
useful in endometrial cancer. Kitajima et al (17) demonstrated that the metabolic tumor
volume (MTV) and total lesion glycolysis (TLG) of the primary
tumors were correlated with clinicopathological features and useful
for differentiating high- from low-risk endometrial cancer.
Consistently, Chung et al (18) reported that MTV was an independent
prognostic factor for disease recurrence in endometrial cancer and
Husby et al (19) also showed
that MTV was useful for the identification of patients with
high-risk endometrial carcinoma. Lee et al (20) revealed that preoperative TLG was
associated with recurrence in 28 patients with carcinosarcoma. As
the primary tumors have intratumoral FDG metabolic heterogeneity
(21), the present study, focusing
only on the simple and easy to measure SUVmax, may have
limitations. Further studies using multi-metabolic parameters of
FDG-PET/CT, including the SUVmax, MTV and TLG, in
combination with other non-invasive biomarkers, are required to
clarify the optimal prognostic parameter for patients with
endometrial cancer and uterine carcinosarcoma.
In conclusion, the present study demonstrated that a
high SUVmax on preoperative PET/CT correlates with
clinicopathological risk factors and less favorable clinical
outcomes in patients with endometrial cancer. These findings
suggested that the SUVmax of the primary tumor may be a
promising prognostic indicator for risk stratification in patients
with this disease, although its usefulness in specific histological
types, including carcinosarcoma, requires clarification by further
studies.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Morice P, Leary A, Creutzberg C, AbuRustum
N and Darai E: Endometrial cancer. Lancet. 387:1094–1108. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Singh R: Review literature on uterine
carcinosarcoma. J Cancer Res Ther. 10:461–468. 2014.PubMed/NCBI
|
|
4
|
Zhang C, Hu W, Jia N, Li Q, Hua K, Tao X,
Wang L and Feng W: Uterine carcinosarcoma and high-risk endometrial
carcinomas: A clinicopathological comparison. Int J Gynecol Cancer.
25:629–636. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhu J, Wen H, Bi R and Wu X:
Clinicopathological characteristics, treatment and outcomes in
uterine carcinosarcoma and grade 3 endometrial cancer patients: A
comparative study. J Gynecol Oncol. 27:e182016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cantrell LA, Havrilesky L, Moore DT,
O'Malley D, Liotta M, Secord AA, Nagel CI, Cohn DE, Fader AN,
Wallace AH, et al: A multi-institutional cohort study of adjuvant
therapy in stage I–II uterine carcinosarcoma. Gynecol Oncol.
127:22–26. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nakamura K, Hongo A, Kodama J and
Hiramatsu Y: The pretreatment of maximum standardized uptake values
(SUVmax) of the primary tumor is predictor for poor
prognosis for patients with epithelial ovarian cancer. Acta Med
Okayama. 66:53–60. 2012.PubMed/NCBI
|
|
8
|
Tanizaki Y, Kobayashi A, Shiro M, Ota N,
Takano R, Mabuchi Y, Yagi S, Minami S, Terada M and Ino K:
Diagnostic value of preoperative SUVmax on FDG-PET/CT
for the detection of ovarian cancer. Int J Gynecol Cancer.
24:454–460. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kidd EA, Siegel BA, Dehdashti F and
Grigsby PW: The standardized uptake value for F-18
fluorodeoxyglucose is a sensitive predictive biomarker for cervical
cancer treatment response and survival. Cancer. 110:1738–1744.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee YY, Choi CH, Kim CJ, Kang H, Kim TJ,
Lee JW, Lee JH, Bae DS and Kim BG: The prognostic significance of
the SUVmax (maximum standardized uptake value for F-18
fluorodeoxyglucose) of the cervical tumor in PET imaging for early
cervical cancer: Preliminary results. Gynecol Oncol. 115:65–68.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nakamura K, Kodama J, Okumura Y, Hongo A,
Kanazawa S and Hiramatsu Y: The SUVmax of 18F-FDG PET
correlates with histological grade in endometrial cancer. Int J
Gynecol Cancer. 20:110–115. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Antonsen SL, Loft A, Fisker R, Nielsen AL,
Andersen ES, Høgdall E, Tabor A, Jochumsen K, Fagö-Olsen CL,
Asmussen J, et al: SUVmax of 18FDG PET/CT as a predictor
of high-risk endometrial cancer patients. Gynecol Oncol.
129:298–303. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nakamura K, Hongo A, Kodama J and
Hiramatsu Y: The measurement of SUVmax of the primary
tumor is predictive of prognosis for patients with endometrial
cancer. Gynecol Oncol. 123:82–87. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
WalentowiczSadlecka M, Malkowski B,
Walentowicz P, Sadlecki P, Marszalek A, Pietrzak T and Grabiec M:
The preoperative maximum standardized uptake value measured by
18F-FDG PET/CT as an independent prognostic factor of overall
survival in endometrial cancer patients. Biomed Res Int.
2014:2348132014.PubMed/NCBI
|
|
15
|
Kitajima K, Kita M, Suzuki K, Senda M,
Nakamoto Y and Sugimura K: Prognostic significance of
SUVmax (maximum standardized uptake value) measured by
[18F]FDG PET/CT in endometrial cancer. Eur J Nucl Med Mol Imaging.
39:840–845. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ghooshkhanei H, Treglia G, Sabouri G,
Davoodi R and Sadeghi R: Risk stratification and prognosis
determination using (18)F-FDG PET imaging in endometrial cancer
patients: A systematic review and meta-analysis. Gynecol Oncol.
132:669–676. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kitajima K, Suenaga Y, Ueno Y, Maeda T,
Ebina Y, Yamada H, Okunaga T, Kubo K, Sofue K, Kanda T, et al:
Preoperative risk stratification using metabolic parameters of
(18)F-FDG PET/CT in patients with endometrial cancer. Eur J Nucl
Med Mol Imaging. 42:1268–1275. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chung HH, Lee I, Kim HS, Kim JW, Park NH,
Song YS and Cheon GJ: Prognostic value of preoperative metabolic
tumor volume measured by 18F-FDG PET/CT and MRI in patients with
endometrial cancer. Gynecol Oncol. 130:446–451. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Husby JA, Reitan BC, Biermann M, Trovik J,
Bjørge L, Magnussen IJ, Salvesen ØO, Salvesen HB and Haldorsen IS:
Metabolic tumor volume on 18F-FDG PET/CT improves preoperative
identification of high-risk endometrial carcinoma patients. J Nucl
Med. 56:1191–1198. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lee JW, Heo EJ, Moon SH, Lee H, Cheon GJ,
Lee M, Kim HS and Chung HH: Prognostic value of total lesion
glycolysis on preoperative 18F-FDG PET/CT in patients with uterine
carcinosarcoma. Eur Radiol. Feb 16–2016.(Epub ahead of print).
View Article : Google Scholar
|
|
21
|
Kidd EA and Grigsby PW: Intratumoral
metabolic heterogeneity of cervical cancer. Clin Cancer Res.
14:5236–5241. 2008. View Article : Google Scholar : PubMed/NCBI
|