Introduction
Temozolomide (TMZ) chemotherapy has been found to be
effective for malignant glioma. The reported median overall
survival (OS) at first relapse for anaplastic astrocytoma and
anaplastic mixed oligoastrocytoma was 13.6 months and the adverse
events were mild to moderate (1).
The overall survival (OS) of patients with newly diagnosed
anaplastic astrocytoma treated with 4 cycles of TMZ prior to
radiation therapy was 23.5 months (2). We herein report the case of a glioma
patient whose tumor had progressed to contrast-enhanced following
gadolinium (Gd) administration, and was histopathologically
diagnosed as anaplastic astrocytoma harboring the isocitrate
dehydrogenase 1 (IDH1) R132H mutation. The protein expression of
O6-methylguanine-DNA methyltransferase (MGMT) in the
tumor cells was negative. Consecutive TMZ treatment suppressed
tumor growth. However, after 108 cycles of TMZ treatment, the
patient succumbed to hemorrhage from the hemangiomas. No tumor
cells were detected on the post-mortem examination of the brain and
the tumor appeared to have regressed following long-term TMZ
treatment.
Case report
A 35-year-old man who experienced a convulsive
episode originating in the right side was referred to Kagoshima
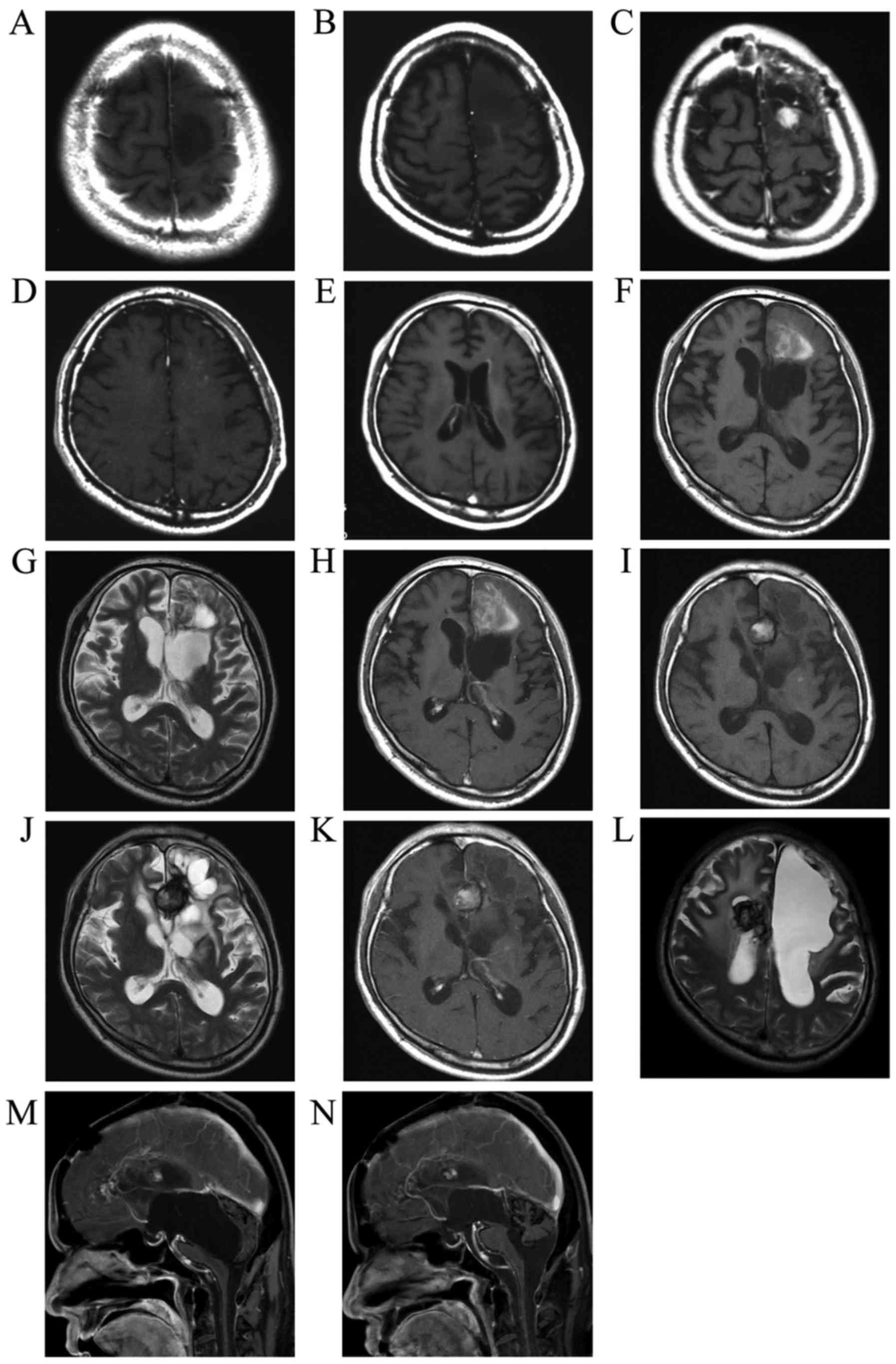
University Hospital (Kagoshima, Japan). Magnetic resonance imaging
(MRI) indicated the presence of a tumor in the left frontal lobe.
The hypointense tumor on T1-weighted images did not exhibit
contrast enhancement following Gd contrast medium administration
(Fig. 1A). The patient underwent the
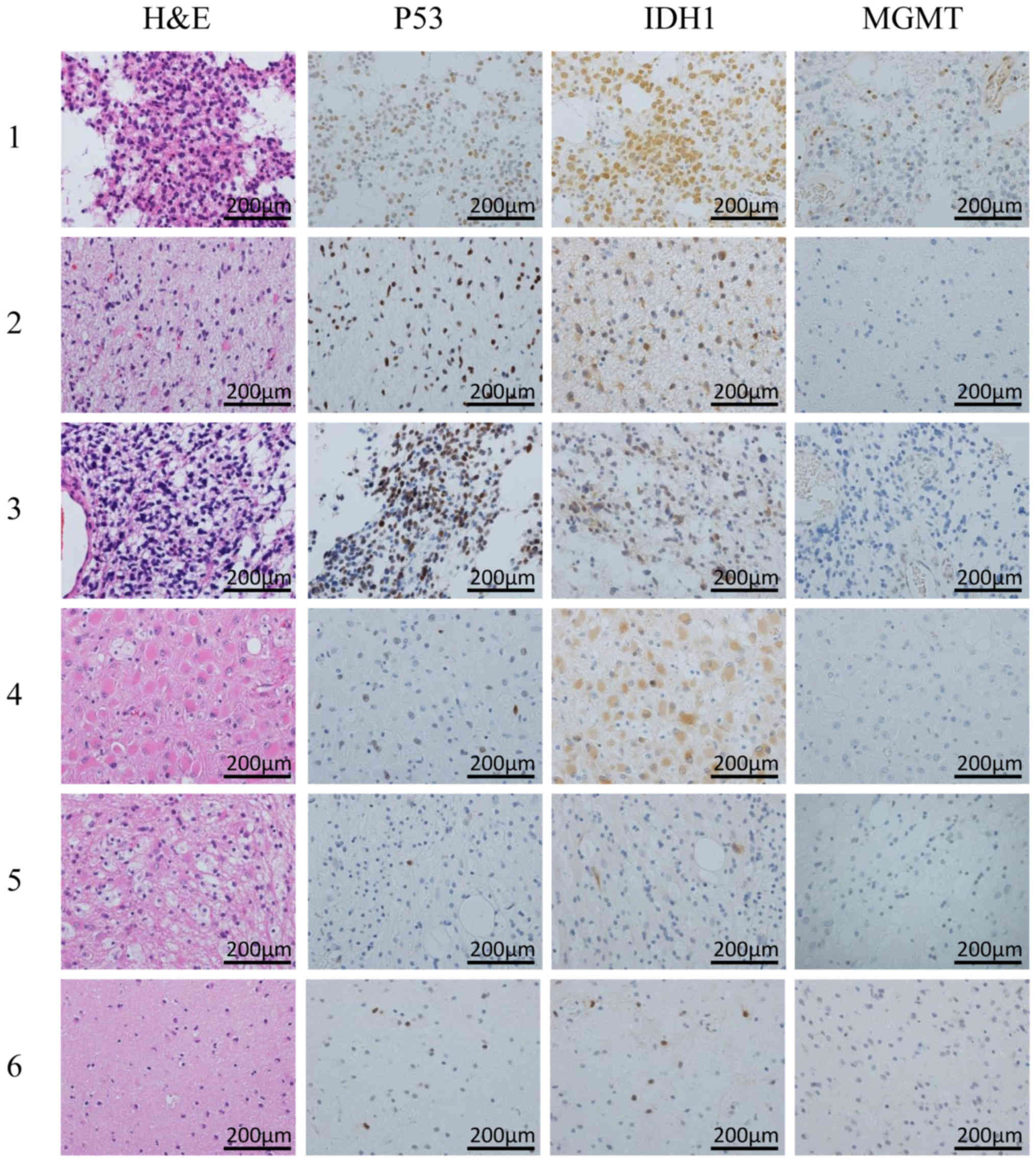
first tumor removal surgery in February, 1999, and the histological
diagnosis was anaplastic astrocytoma (Fig. 2, row 1). The retrospective analysis
for 1p/19q status by fluorescence in situ hybridization
revealed no co-deletion. A second surgery was performed 2 years and
5 months after the first surgery due to tumor recurrence in the
anterior wall of the removal cavity (Fig. 1B) and the histological diagnosis was
diffuse astrocytoma (Fig. 2, row 2).
At 3 years and 3 months after the first surgery, tumor recurrence
was detected as a mass displaying contrast enhancement following Gd
administration (Fig. 1C) and the
histological diagnosis of the specimens from the third surgery was
anaplastic astrocytoma (Fig. 2, row
3). The MIB-1 index of the specimen was ~30%. The patient
subsequently underwent radiotherapy (40 Gy of extended-field
irradiation and 20 Gy of local irradiation) and chemotherapy with
nimustine hydrochloride (ACNU) 100 mg on day 1 and vincristine 2 mg
on days 1, 21 and 42, every 6–8 weeks. After 2 cycles of
chemotherapy, a new lesion appeared in the deep frontal lobe
(Fig. 1D). The patient underwent a
fourth surgery 3 years and 8 months after the first surgery
(Fig. 2, row 4). Despite continuing
chemotherapy and additional CyberKnife treatment, an invasive tumor
extended into the wall of the left lateral ventricle (Fig. 1E) and the patient underwent a fifth
tumor removal surgery 4 years and 6 months after the first surgery
(Fig. 2, row 5).
At 5 years and 3 months after the first surgery,
ACNU was replaced with TMZ for 5 days every 4 weeks, as tumor
growth and invasion were not controlled by ACNU treatment. The
tumor continued to grow, extending to the right frontal lobe
through the corpus callosum after 6 cycles of TMZ treatment;
however, the tumor growth decelerated. By the 22nd cycle of TMZ
treatment, tumor growth had been arrested. TMZ treatment was
continued according to the wishes of the patient and his family. At
8 years and 8 months after the first surgery, the 41st cycle of TZM
treatment was administered and tumor progression was suppressed.
This patient's long-term, 41-cycle TZM treatment was previously
reported in the Japanese language CP Neurosurgery journal, as case
1 in an article reporting long-term TMZ treatment in two patients
with high-grade glioma (3). Prior to
the 42nd TZM treatment, hemorrhage occurred in the residual tumor
that displayed contrast enhancement following Gd administration in
the left frontal lobe (Fig. 1F-H).
The hemorrhagic lesion was converted to a circumscribed hematoma
and the size gradually increased (Fig.
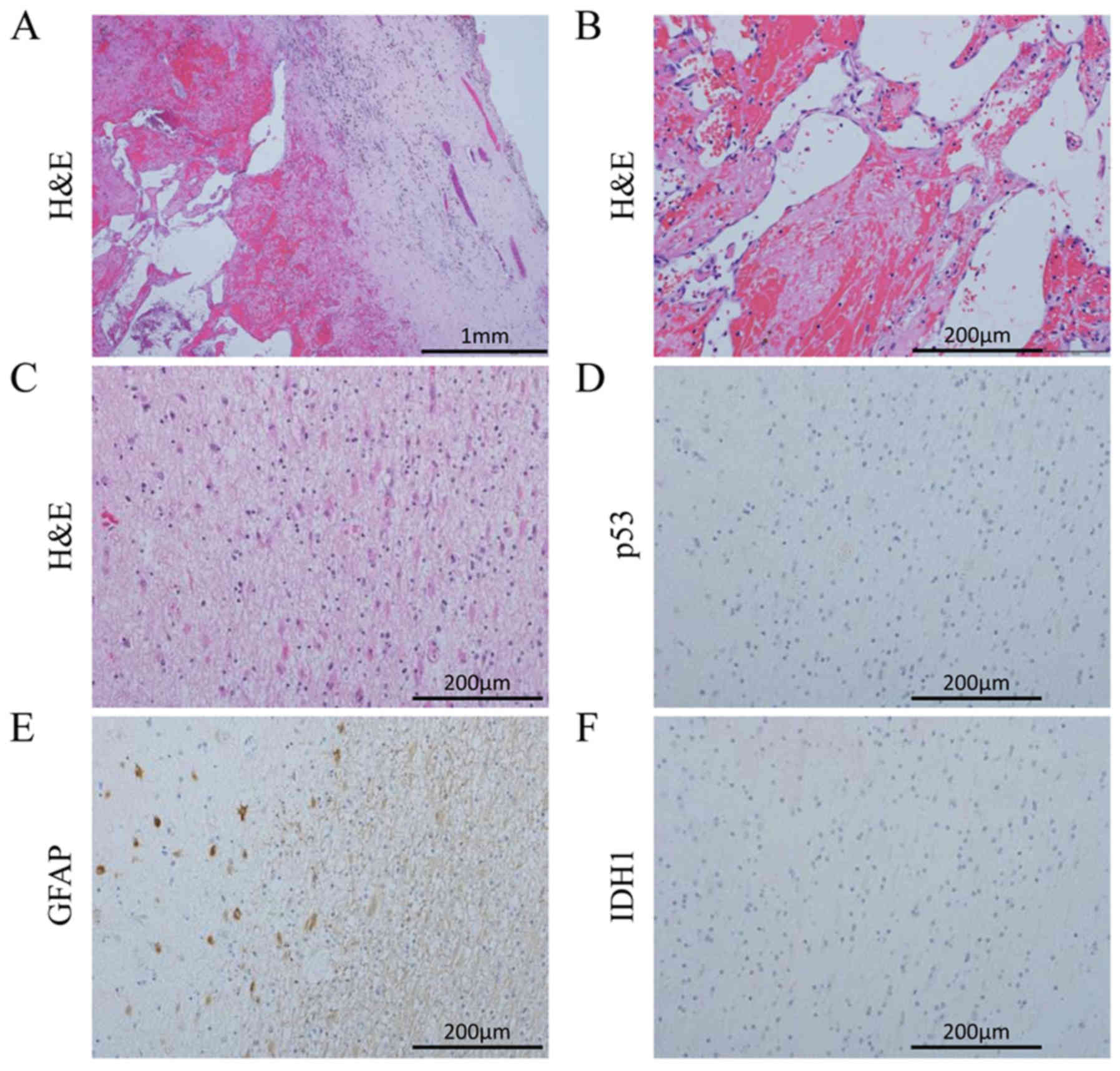
1I-K). The patient underwent a sixth surgery to remove the
hemorrhagic lesion 11 years and 3 months after the initial surgery.
The circumscribed hematoma (Fig. 3A and
B) and surrounding tissue (Fig.
2, row 6) were removed after the 69th TMZ treatment and TMZ
treatment was continued after this surgery. Additional new lesions
were detected in the right frontal lobe. According to the
continuous MRI observation, the T2 hypointense mass in the right
frontal lobe was diagnosed as a hemangioma, suspected to have
developed post-radiation therapy (Fig.
1L). Several new hemangiomas appeared, but no further lesions
indicating glioma recurrence. Eleven years and 7 months after the
first surgery, the patient was admitted to another hospital due to
deterioration of daily activities under continuing TMZ treatment;
he underwent neuroendoscopic surgery 13 years and 8 months after
the first surgery to treat the hydrocephalus (Fig. 1M) caused by continuous bleeding into
the ventricles from the hemangiomas. During the surgery, a cloudy
fluid was observed, with precipitation of the hematoma over the
aqueduct. Short-term recovery was achieved by relieving the
obstruction of the aqueduct and performing a third ventriculostomy
by endoscopic surgery (Fig. 1N), but
the patient succumbed to respiratory failure caused by severe
hydrocephalus with perpetual hemorrhage from the hemangiomas (14
years and 9 months from the first surgery). An autopsy was
performed and the brain tissue was carefully examined.
The TMZ treatment was continued until 3 months prior
to the patient's death, for a total of 108 cycles. The initial
dosage of TMZ treatment was 150 mg/m2 and was increased
to 200 mg/m2 from the second treatment onwards. The mean
TMZ dosage administered from the third to the 41st cycle was 175
mg/m2. From the 42nd cycle onwards, the dose was
adjusted to maintain the pretreatment white blood cell count
>2,000/µl, and the dose was finally decreased to ~130
mg/m2.
Pathological analysis
Surgically obtained specimens were promptly placed
in formaldehyde in the surgical room. The specimens were then
transferred to the Pathology laboratory and, after appropriate
fixation, embedded in paraffin. During the autopsy, the brain was
immediately removed, weighed and measured. Images were captured and
the 5 regions of interest were removed. These regions included the
left frontal, left and right occipital, right cerebellar and
intraventricular masses. These samples, as well as the whole brain,
were fixed in formaldehyde. Following fixation, brain specimens
were also prepared for microscopic examination (a total of 22
blocks). The specimens were finally embedded in paraffin, cut into
4-µm sections and stained with hematoxylin and eosin. The most
representative specimens were prepared for immunohistochemistry.
The sections were mounted on poly-L-lysine-coated glass slides and
stained for IDH1 (DIA H09 R132H, mouse IgG2a; Dianova GmbH,
Hamburg, Germany), p53 (DO-7, mouse IgG2b; Leica, Newcastle, UK),
MGMT (MT3.1, mouse IgG1; Millipore, CA, USA) and Ki-67 (MIB-1,
mouse IgG1; Dako, Glostrup, Denmark). Additional staining with
glial fibrillary acidic protein (GFAP; 6F2, mouse IgG1; Dako), CD68
(KP-1, mouse IgG1; Dako) and leukocyte common antigen (CD45;
2B11+PD7/26, mouse IgG1; Dako) was performed to observe reactive
changes following hemorrhage. The dilution rates and catalog
numbers for all the antibodies were as follows: IDH1 (1:20,
DIA-H09), MGMT (1:200, MAB16200), p53 (1:600, NCL-L-p53-DO7), Ki67
(1:50, M7240), GFAP (1:50, M0761), CD68 (1:50, M0814) and CD45
(1:50, M0701). The immunostained specimens were visualized using
3,3′-diaminobenzidine as a substrate and hematoxylin was used as a
nuclear counterstain. The immunohistochemistry results are
presented in Figs. 2 and 3.
IDH1 detection by quantitative
polymerase chain reaction (qPCR)
To confirm the wild-type and R132H mutation of IDH1,
the qPCR procedure was applied. Total RNA was extracted from 50-mg
paraffin-embedded specimens from the first surgery, the last
surgery and the autopsy, using the NucleoSpin totalRNA FFPE Mini
kit (Takara Bio Inc., Kusatsu, Japan) according to the
manufacturer's instructions. Each 6 µl of extract were used to make
cDNA by reverse transcription (ReverTra Ace® qPCR RT
Master mix with gDNA Remover, Toyobo Co., Ltd., Osaka, Japan). The
aliquot of cDNA (1.5 µg/µl) was used as template, and qPCR was
conducted (StepOnePlus™ Real-Time PCR System, Applied Biosystems,
USA, CA). The primer sets were as follows: GAPDH: Hs99999905_m1
GAPDH (TaqMan Gene Expression Assays); wild-type IDH1:
Hs00001019_rf IDH1_rf (TaqMan Mutation Detection Assays); and
mutant IDH1 (R132H): Hs00000981_mu IDH1_28746_mu (TaqMan Mutation
Detection Assays).
Histopathological findings
The staining for p53 and IDH1 was positive in all
six tumor specimens obtained from each surgery. In the specimens
from the sixth surgery, p53 and IDH1 positivity was found in the
tissue surrounding the hemangioma. The 21 slides prepared from the
specimens obtained from the 5 regions of interest and the 22 slides
from the brain specimen were not positive for p53 or IDH1. The
tissues from the masses in the lateral ventricles were organized
hematomas and consisted of fibroblasts, macrophages and
lymphocytes. In the periventricular zone of the left frontal lobe
(Fig. 3C-F), non-neoplastic
GFAP-positive astrocytes were observed, but these cells were
negative for Ki-67, p53 and IDH1. The autopsy specimens were
carefully examined, but cells expressing p53 or IDH1 were not
detected, leading to the conclusion that the tumor cells had been
eliminated from the brain. The MGMT expression was negative in all
tumor and autopsy specimens, apart from the blood vessels.
IDH1 message detection by qPCR
(Fig. 4)
Amplification of cDNA was detected for GAPDH,
wild-type IDH1 and mutant IDH1 in the samples from the first and
last surgeries. In the autopsy sample, amplification of cDNA for
GAPDH and wild-type IDH1 was detected, but that of mutant IDH1 was
not. A second PCR was then conducted using the first PCR products
as templates in autopsy. However, amplification of mutant IDH1 was
not found. This was compatible with the results of
immunohistochemistry.
Discussion
According to recent findings, IDH mutations are a
characteristic occurrence in low-grade gliomas (4,5) and
considered to be preserved in the glioma lineage.
Immunohistochemical identification of the IDH1 and p53 mutations
was observed in the specimens from the first surgery in our case;
however, the prevalence gradually decreased in the samples obtained
through to the sixth surgery, which followed the 69th TMZ
treatment, and these mutations were not detected in the autopsy
tissue. These results suggested that long-term TMZ treatment
eliminated the tumor cells. From an opposing viewpoint, this result
indicates that >69 courses of TMZ treatment were required to
eradicate the tumor cells. The R132H IDH1 mutation is found in ~90%
of all IDH1 mutations (5). The
antibody for R132H is an excellent marker, and Capper et al
emphasized its superiority compared with other established
antibodies for the differentiation of neoplastic from reactive
cells in grade II and III gliomas, allowing for the identification
of tumor cells in post-therapy specimens with extensive reactive
changes (6). To reconfirm the
results of immunohistochemistry, mRNA analysis was performed and
the qPCR results established the reliability of
immunohistochemistry. Thus, this antibody was found to be a useful
and reliable marker for the histopathological detection of tumor
cells.
The median OS for the first relapse of anaplastic
astrocytoma and anaplastic mixed oligoastrocytoma is 13.6 months,
with a response rate of 35% according to Yung et al
(1). The patients with anaplastic
astrocytoma reported by Gilbert et al exhibited a good
response rate of 39% (2). A
retrospective multicenter study by the Central Nervous System Study
Group (Italian Association of Radiation Oncology) reported a median
OS of 20.6 months for anaplastic astrocytoma treated by
radiotherapy and TMZ, with a survival rate at 4 years of 28.6%
(7). Long-term TMZ treatment is
feasible for glioma patients (8) and
a case with 85 cycles of TMZ at normal dosing levels was previously
reported (9). In our patient, the
dose was reduced to maintain regular treatment, with a total of 108
TMZ cycles administered. The IDH1 mutation is a good prognostic
factor in gliomas (10) and, in
recent chemoradiotherapy treatments, its presence was associated
with prolonged survival time of patients with malignant glioma,
even those with glioblastoma (11).
However, long-term survivors may suffer from
additional treatment-induced complications. Delayed neurotoxicity
by cranial irradiation includes disorders of cognitive function,
brain atrophy, radiation necrosis, neoplasms and vascular
accidents. Cavernous malformation are frequently reported following
radiation therapy in pediatric patients with brain tumors, mostly
those with medulloblastoma (12–16). The
cumulative incidence of cavernous angioma treated for
medulloblastoma was 5.6, 14 and 43%, at 3, 5 and 10 years,
respectively (17). Recent reports
have identified that a small number of cavernous angiomas occur
after treatment for astrocytic tumors (18,19).
This may be attributed to the increased number of long-term
astrocytic tumor survivors.
Summarizing the treatment course of our patient,
long-term TMZ treatment achieved elimination of tumor cells,
although the patient ultimately succumbed to the complications of a
cavernous angioma likely induced by radiotherapy. It is currently
considered that it is important to remove angiomas during the early
stages, in order to prevent continuous bleeding, as recent
treatments may significantly prolong the survival of glioma
patients.
This retrospective case report conformed to the
regulations of the Ethics Committee of Kagoshima University
Hospital (reference number 22–50, ‘A study of relationship between
prognosis and neuroimaging and pathologic findings in brain tumor’)
and was conducted in accordance with the ethical standards laid
down in the 1964 Declaration of Helsinki.
Acknowledgements
The authors are indebted to the patient who donated
his body to glioma research in his living will and grateful to his
family who supported his wishes and honored his will. Kazunori
Arita has received a Health and Labour Sciences Research Grant from
the Ministry of Health, Labour and Welfare of Japan, and the Kiban
Research Grant C from the Ministry of Education, Culture, Sports,
Science and Technology of Japan. Hirofumi Hirano has received the
Kiban Research Grant C from the Ministry of Education, Culture,
Sports, Science and Technology of Japan.
References
|
1
|
Yung WK, Prados MD, Yaya-Tur R, Rosenfeld
SS, Brada M, Friedman HS, Albright R, Olson J, Chang SM, O'Neill
AM, et al: Multicenter phase II trial of temozolomide in patients
with anaplastic astrocytoma or anaplastic oligoastrocytoma at first
relapse. Temodal brain tumor group. J Clin Oncol. 17:2762–2771.
1999.PubMed/NCBI
|
|
2
|
Gilbert MR, Friedman HS, Kuttesch JF,
Prados MD, Olson JJ, Reaman GH and Zaknoen SL: A phase II study of
temozolomide in patients with newly diagnosed supratentorial
malignant glioma before radiation therapy. Neuro Oncol. 4:261–267.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hirano H, Yunoue S and Arita K: Long-term
temozolomide treatment in two patients with high-grade glioma (in
Japanese with English abstract). CP Neurosurgery. 18:886–892.
2008.
|
|
4
|
Yan H, Parsons DW, Jin G, McLendon R,
Rasheed BA, Yuan W, Kos I, Batinic-Haberle I, Jones S, Riggins GJ,
et al: IDH1 and IDH2 mutations in gliomas. N Engl J Med.
360:765–773. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Arita H, Narita Y, Yoshida A, Hashimoto N,
Yoshimine T and Ichimura K: IDH1/2 mutation detection in gliomas.
Brain Tumor Pathol. 32:79–89. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Capper D, Sahm F, Hartmann C, Meyermann R,
von Deimling A and Schittenhelm J: Application of mutant IDH1
antibody to differentiate diffuse glioma from nonneoplastic central
nervous system lesions and therapy-induced changes. Am J Surg
Pathol. 34:1199–1204. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Scoccianti S, Magrini SM, Ricardi U, Detti
B, Krengli M, Parisi S, Bertoni F, Sotti G, Cipressi S, Tombolini
V, et al: Radiotherapy and temozolomide in anaplastic astrocytoma:
A retrospective multicenter study by the central nervous system
study group of AIRO (Italian Association of Radiation Oncology).
Neuro Oncol. 14:798–807. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hau P, Koch D, Hundsberger T, Marg E,
Bauer B, Rudolph R, Rauch M, Brenner A, Rieckmann P, Schuth J, et
al: Safety and feasibility of long-term temozolomide treatment in
patients with high-grade glioma. Neurology. 68:688–690. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mannas JP, Lightner DD, Defrates SR,
Pittman T and Villano JL: Long-term treatment with temozolomide in
malignant glioma. J Clin Neurosci. 21:121–123. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Takano S, Kato Y, Yamamoto T, Kaneko MK,
Ishikawa E, Tsujimoto Y, Matsuda M, Nakai K, Yanagiya R, Morita S,
et al: Immunohistochemical detection of IDH1 mutation, p53, and
internexin as prognostic factors of glial tumors. J Neurooncol.
108:361–373. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kawano H, Hirano H, Yonezawa H, Yunoue S,
Yatsushiro K, Ogita M, Hiraki Y, Uchida H, Habu M, Fujio S, et al:
Improvement in treatment results of glioblastoma over the last
three decades and beneficial factors. Br J Neurosurg. 29:206–212.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Novelli PM, Reigel DH, Gleason P Langham
and Yunis E: Multiple cavernous angiomas after high-dose
whole-brain radiation therapy. Pediatr Neurosurg. 26:322–325. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maeder P, Gudinchet F, Meuli R and de
Tribolet N: Development of a cavernous malformation of the brain.
AJNR Am J Neuroradiol. 19:1141–1143. 1998.PubMed/NCBI
|
|
14
|
Baumgartner JE, Ater JL, Ha CS, Kuttesch
JF, Leeds NE, Fuller GN and Wilson RJ: Pathologically proven
cavernous angiomas of the brain following radiation therapy for
pediatric brain tumors. Pediatr Neurosurg. 39:201–207. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Aguilera D, Tomita T, Goldman S and
Fangusaro J: Incidental resolution of a radiation-induced cavernous
hemangioma of the brain following the use of bevacizumab in a child
with recurrent medulloblastoma. Pediatr Neurosurg. 46:303–307.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chourmouzi D, Papadopoulou E, Kontopoulos
A and Drevelegas A: Radiation-induced intracranial meningioma and
multiple cavernomas. BMJ Case Rep. 2013:pii2013.
|
|
17
|
Lew SM, Morgan JN, Psaty E, Lefton DR,
Allen JC and Abbott R: Cumulative incidence of radiation-induced
cavernomas in long-term survivors of medulloblastoma. J Neurosurg.
104:(Suppl 2). S103–S107. 2006.
|
|
18
|
Furuse M, Miyatake SI and Kuroiwa T:
Cavernous malformation after radiation therapy for astrocytoma in
adult patients: Report of 2 cases. Acta Neurochir (Wien).
147:1097–1101. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fukushima S, Narita Y, Miyakita Y, Ohno M,
Takizawa T, Takusagawa Y, Mori M, Ichimura K, Tsuda H and Shibui S:
A case of more than 20 years survival with glioblastoma, and
development of cavernous angioma as a delayed complication of
radiotherapy. Neuropathology. 33:576–581. 2013.PubMed/NCBI
|