Introduction
Synchronous primary genital cancer is an uncommon
occurrence. In a retrospective study of 3,863 patients with female
genital malignancies, 26 (0.7%) patients with synchronous primaries
were identified (1). The concomitant
malignancies are frequently diagnosed as metastatic disease. In the
majority of the cases, the patients with >1 gynecological
neoplasms present with synchronous endometrial and ovarian cancer
(1), whereas synchronous primary
malignancies of the uterus are even rarer (2,3). We
herein present an unusual case of cervical squamous cell carcinoma
and endometrial adenocarcinoma occurring simultaneously. The aim of
this case report was to evaluate the diagnosis and treatment of
synchronous cancers of the cervix and endometrium.
Case report
A 48-year-old Chinese female patient (body mass
index, 26.8 kg/m2, gravida 2, para 2), who had a history
of a sterilization operation, presented in July, 2013 at the First
Affiliated Hospital of Xi'an Jiaotong University (Xi'an, China)
with irregular vaginal spotting for 5 months. The patient's last
menstrual period was on July 7, 2013. Other past history and family
history were unremarkable. After attending a regional hospital for
spotted vaginal bleeding, the patient underwent a cervical biopsy
during colposcopy due to a 0.3-cm cauliflower-like lesion in the
anterior cervical lip, and fractional curettage of the endometrium.
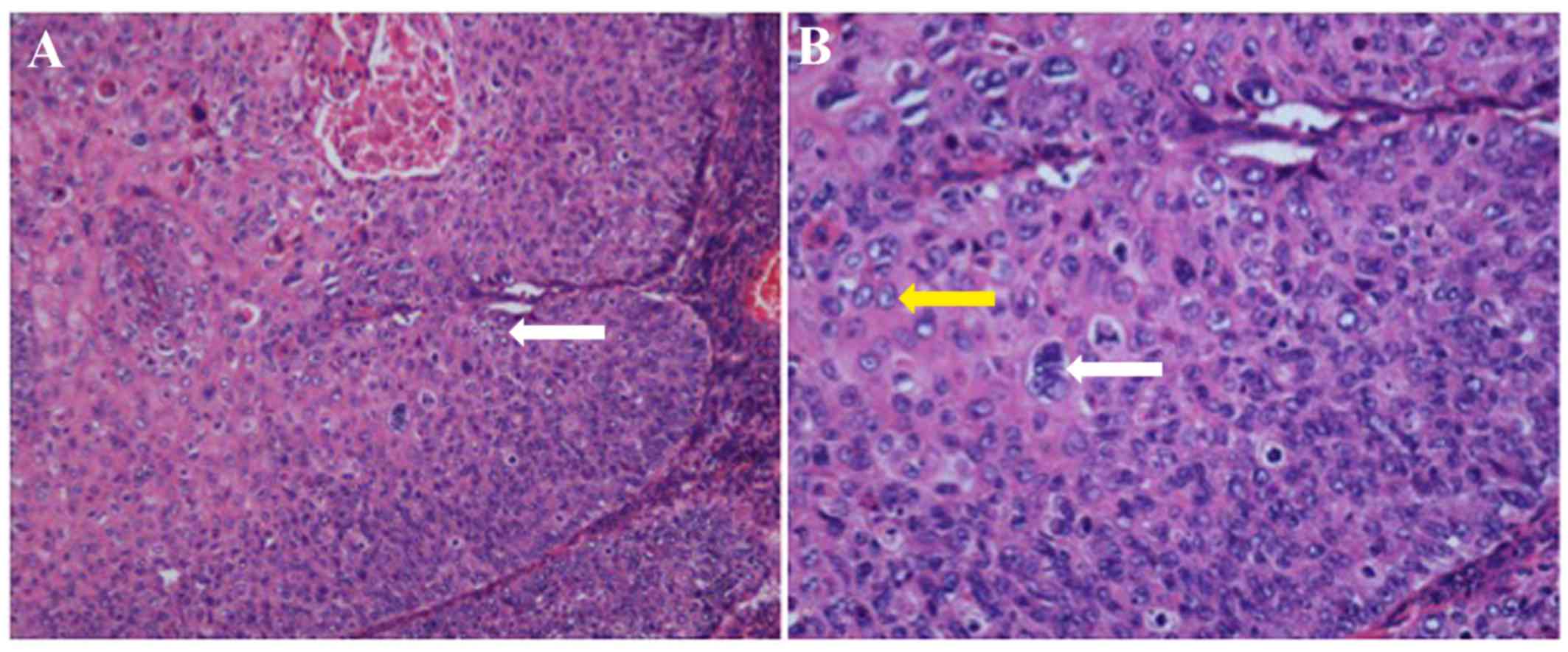
The pathological examination of the bioptic material in our
pathology department revealed a poorly differentiated squamous cell
carcinoma in the cervix (Fig. 1) and
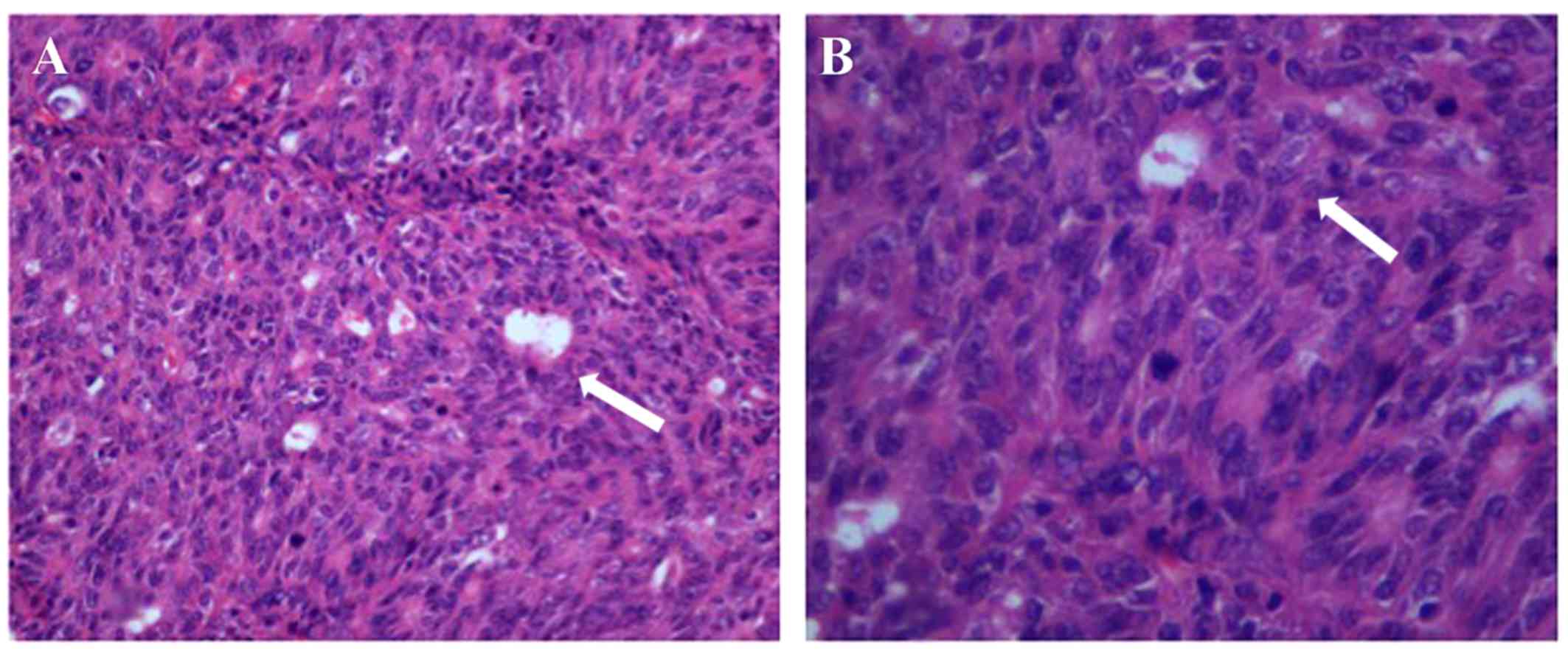
a poorly differentiated adenocarcinoma in the uterine cavity
(Fig. 2). Physical examination in
our hospital revealed a soft abdomen, a minor ulcer-like lesion in
the anterior cervical lip with a diameter of 0.5 cm, and an
enlarged uterus, similar to the 11th gestational week. Pelvic
examination revealed a movable cervix with a grossly smooth
appearance, well-supported smooth vagina, free parametrium and
movable uterosacral ligaments. Magnetic resonance imaging of the
pelvic cavity revealed an abnormal signal in the anterior lip of
the cervix and a 5×4×1-cm thickening of the endometrium in the
uterine cavity involving the upper part of the corpus. The
preoperative serum tumor marker levels were as follows:
Carbohydrate antigen (CA) 125, 15.35 U/ml (normal range, 0–35
U/ml), CA 19–9, 5.16 ng/ml (normal range, 0–40 ng/ml) and
carcinoembryonic antigen, 1.48 ng/ml (normal range, ≤5 ng/ml). The
patient had never participated in a cervical screening procedure,
and the human papillomavirus (HPV) test results revealed infection
by type 18.
As the cervical cancer was at clinical stage Ib1 and
the endometrial cancer was at stage Ia according to the
International Federation of Gynecology and Obstetrics (FIGO)
classification, the patient underwent abdominal staging surgery,
including radical hysterectomy, bilateral salpingo-oophorectomy,
pelvic and para-aortic lymphadenectomy. Macroscopically, the uterus
was enlarged, measuring 12×8×6 cm3, with a minor
ulcer-like lesion in the anterior lip of the cervix measuring 0.5
cm in greatest diameter. The adnexa and parametrium were
unremarkable. A fungating tumor, sized 5×4.5×1 cm3, was
identified in the uterine cavity, with superficial invasion of the
myometrium. Hematoxylin and eosin-stained sections revealed poorly
differentiated endometrial adenocarcinoma with superficial
myometrial invasion (<50%) in the corpus uteri. No residual
carcinoma cells were found in the resection margin of the vagina,
and lymph node mapping revealed no metastasis. There was chronic
cervicitis with local squamous metaplasia of the cervix and
Naboth's cysts, bilateral hydrosalpinx and Graafian follicles in
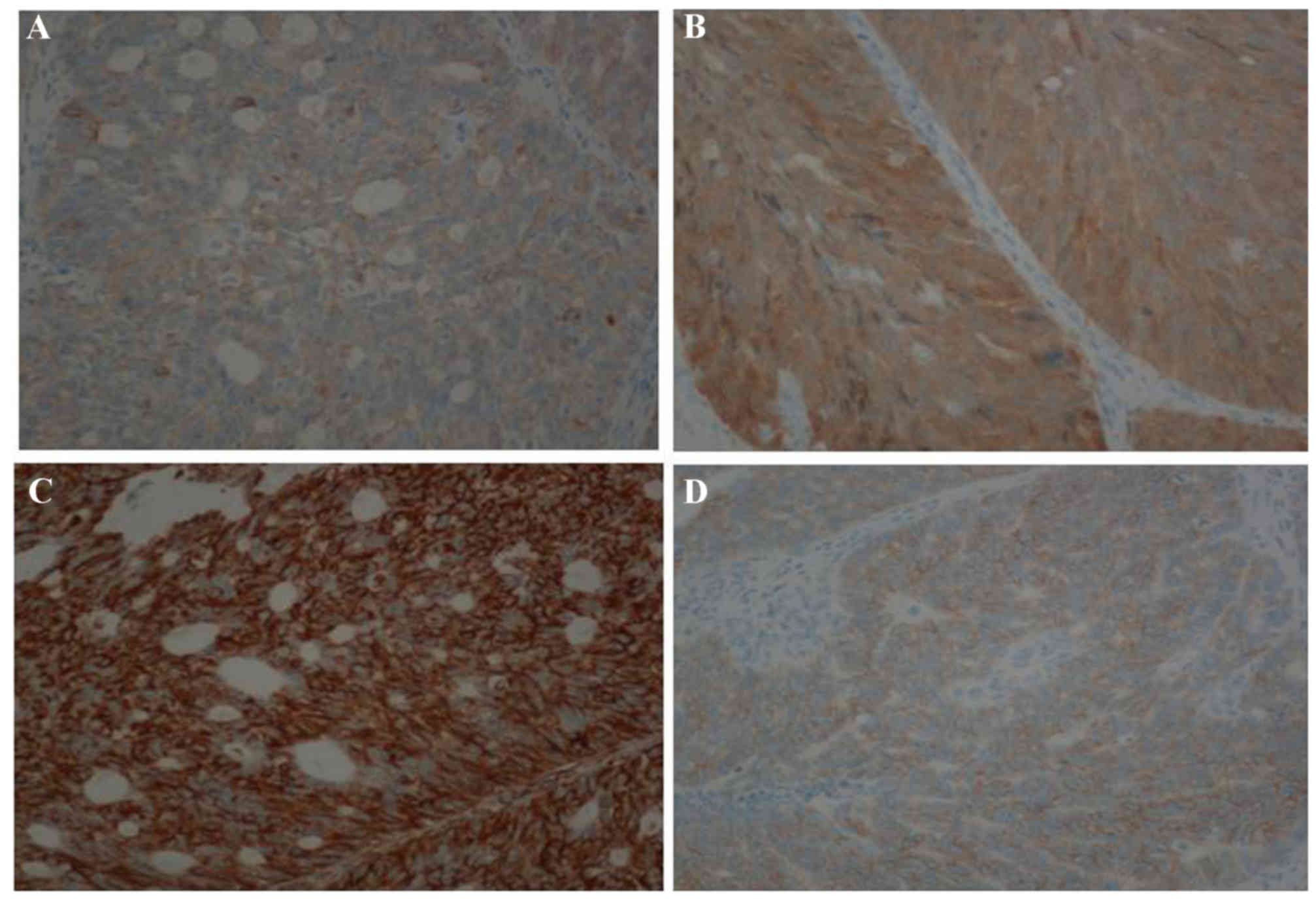
the bilateral ovaries. The results of the immunohistochemical
examination of the carcinomas of the cervix and endometrium were as
follows: Creatine kinase+ (Fig. 3A), P16+ (Fig. 3B), vimentin+ (Fig. 3C), human epidermal growth factor
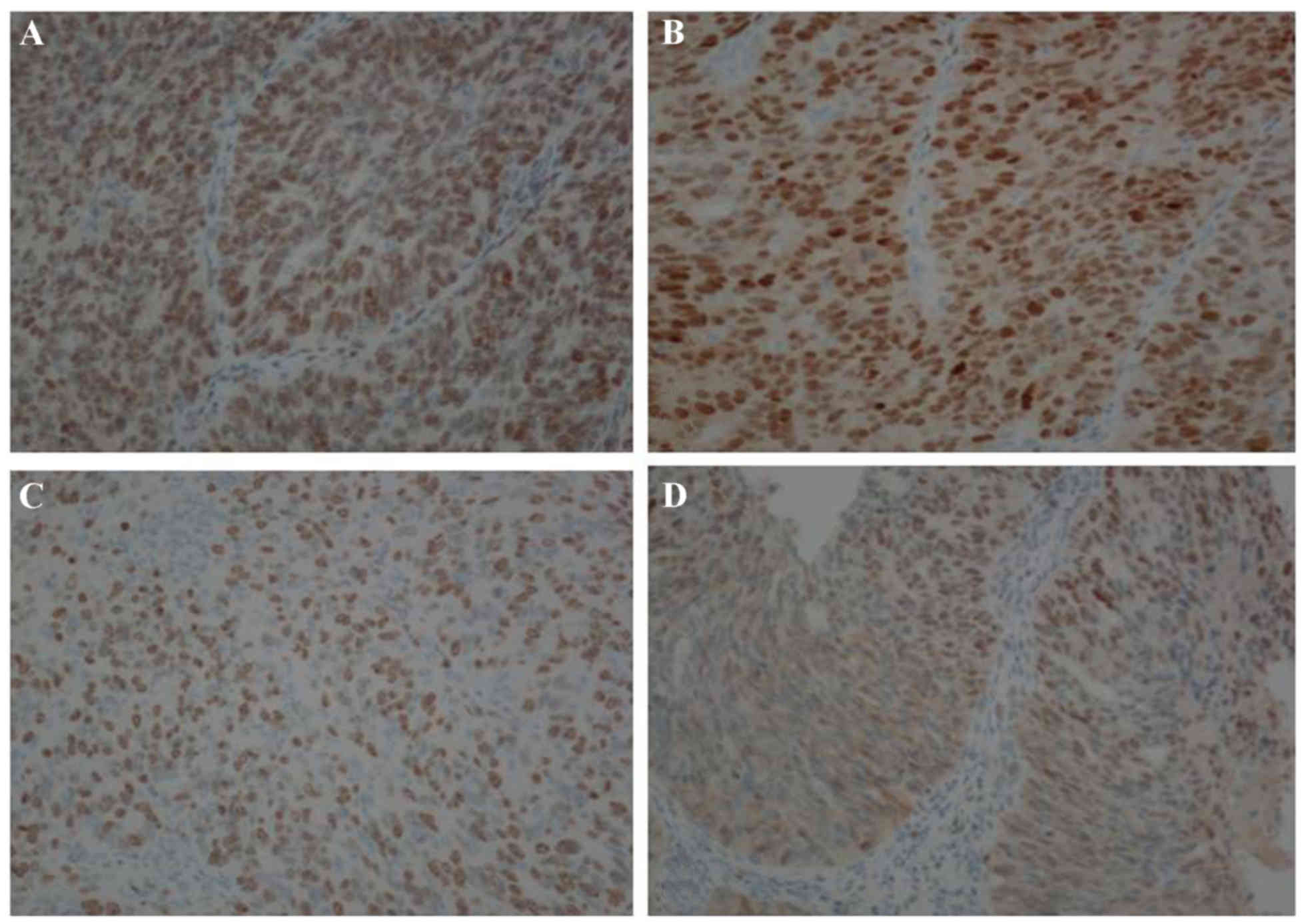
receptor-2+ (2+) (Fig. 3D), estrogen receptor+
(2+, 90%) (Fig. 4A),
progesterone receptor+ (3+, 80%) (Fig. 4B), Ki-67+ (80%) (Fig. 4C), P53+ (80%) (Fig. 4D), cytokeratin (CK)5/6−,
P63−, P40− and CK14−. The patient
was thoroughly evaluated and the FIGO stages were cervical cancer
stage Ib1 and endometrial cancer stage Ia, without lymph node
metastases. The patient is currently followed up every 3 months.
The date of the last follow-up was May 24, 2016 and no recurrence
was observed.
Discussion
Synchronous tumors are defined as two or more tumors
occurring in a patient simultaneously. In 1879, Billroth and
Hackley were the first to report the development of different
primary malignant tumors in the same patient (4). Multiple primary cancers are an
infrequent finding. The etiology and pathogenesis of synchronous
cancers remain unclear. When similar tissues of the female genital
tract are subjected to carcinogen exposure during
fetal/embryological development, synchronous tumors may develop
(5). In gynecological oncology,
endometrial cancers with simultaneous ovarian cancers are the most
common, whereas, to the best of our knowledge, only 9 cases of
carcinoma of the cervix with carcinoma of the endometrium have been
reported to date (3,6–10); the
tumors comprised different histopathological subtypes, whereas in
only two cases (~22%) the types were the same as in the present
case.
Unlike the single aggressive ovarian cancers that
usually remain asymptomatic until they reach an advanced stage,
endometrial and cervical cancers usually produce earlier symptoms,
such as abnormal vaginal bleeding. Therefore, the disease was stage
I at diagnosis in the present case. The diagnosis of synchronous
cancers generally relies on postoperative pathological examination,
as the same pathological patterns may be considered as metastatic
carcinoma. In the present case, the diagnosis of synchronous
cancers was made prior to surgery, as the cancers were of different
pathological type. In order to improve the accuracy of diagnosis of
synchronous cervical and endometrial cancers, when contact bleeding
is observed, the cervix and endometrium should be more closely
inspected. Fractional curettage may be performed if necessary. When
the diagnosis of endometrial cancer is confirmed, a Pap smear or
ThinPrep cytological test should be performed to exclude cervical
cancer. Biopsy is of the same diagnostic value as curettage in
patients with endometrial cancer, particularly those with cancer of
the cervical canal. Stage should be thoroughly evaluated pre- and
postoperatively. Staging should be performed in combination with
clinicopathological diagnosis in order to determine the treatment
strategy. At present, none of the available staging systems is
considered to be suitable and a new system of staging and treatment
determination must be established. According to the results of
diagnostic dilatation and curettage and colposcopic biopsy, some of
the cases may be diagnosed preoperatively and the precise extent of
the resection may be determined.
Radical hysterectomy is the recommended treatment
for stage Ib1 cervical cancer. During the operation, resection of
the sacral and main ligaments and vaginal and pelvic
lymphadenectomy are crucial. For stage Ia poorly differentiated
endometrial adenocarcinoma, hysterectomy may be sufficient,
provided bilateral adnexectomy, pelvic and para-aortic
lymphadenectomy are performed. For our patient, these two types of
operations had to be combined. Radical hysterectomy with bilateral
adnexectomy, pelvic and para-aortic lymphadenectomy were performed.
Adjuvant concurrent chemoradiotherapy was deemed necessary based on
postoperative FIGO staging. The treatment strategies for
synchronous cancers depend on the established strategy for each
individual cancer and, occasionally, both tumors may be treated
simultaneously.
The prognosis of patients with synchronous primary
cervical and endometrial cancers is associated with disease stage
at the time of diagnosis. In general, synchronous cancers are often
considered worse when compared with malignancies of a metachronous
nature, but are associated with significantly higher survival rates
compared with metastatic cases (5,7,10). In every follow-up visit, an HPV text
of the vaginal stump or surgical scar should be performed. As
endometrial cancer may metastasize to the lungs, a chest X-ray is
also reasonable when necessary. Standard therapy including surgery
and/or radiation therapy is strongly recommended. In conclusion,
the occurrence of synchronous primary gynecological cancers is an
uncommon occurrence deserving further investigation.
This case report has been approved by the
Institutional Review Board of the First Affiliated Hospital of
Xi'an Jiaotong University. Written informed consent was obtained
from the patient for publication of the details of this case and
any accompanying images.
References
|
1
|
Eifel P, Hendrickson M, Ross J, Ballon S,
Martinez A and Kempson R: Simultaneous presentation of carcinoma
involving the ovary and the uterine corpus. Cancer. 50:163–170.
1982. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sun HD, Lai CR, Yen MS and Wang PH:
Synchronous occurrence of primary neoplasms of the uterus with
mucinous carcinoma of the cervix and endometrioid carcinoma of the
endometrium. Taiwan J Obstet Gynecol. 50:377–378. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hascalik S, Celik O, Erdem G, Usta U,
Alkan A, Karakas HM and Mizrak B: Synchronous endometrial and
cervical tumors in a 26-year-old nullipara: Diagnostic modalities
updated. Gynecol Obstet Invest. 60:171–176. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Billroth T and Hackley CE: General
surgical pathology and therapeutics. D. Appleton and company; New
York: 1879
|
|
5
|
Eisner RF, Nieberg RK and Berek JS:
Synchronous primary neoplasms of the female reproductive tract.
Gynecol Oncol. 33:335–339. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lin CK, Yu MH, Chu TW and Lai HC:
Synchronous occurrence of primary neoplasms in the uterus with
squamous cell carcinoma of the cervix and adenocarcinoma of the
endometrium. Taiwan J Obstet Gynecol. 45:336–339. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Takeda T, Sagae S, Koizumi M, Terasawa K,
Ishioka S, Takashima S and Kudo R: Multiple primary malignancies in
patients with gynecologic cancer. Int J Gynecol Cancer. 5:34–39.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Benito V, Beltrán L, Andújar M, Lubrano A
and Falcón O: Synchronous primary carcinoma of the cervix and
endometrium with early lymph node recurrence. Int J Gynaecol
Obstet. 103:181–182. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tong SY, Lee YS, Park JS, Bae SN, Lee JM
and Namkoong SE: Clinical analysis of synchronous primary neoplasms
of the female reproductive tract. Eur J Obstet Gynecol Reprod Biol.
136:78–82. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ayhan A, Yalçin OT, Tuncer ZS, Gürgan T
and Küçükali T: Synchronous primary malignancies of the female
genital tract. Eur J Obstet Gynecol Reprod Biol. 45:63–66. 1992.
View Article : Google Scholar : PubMed/NCBI
|