Introduction
Due to the position of the pelvis, the early
symptoms of ovarian cancer may not be noticed, with 60–70% of the
patients being diagnosed at later stages of the disease.
Chemotherapy is effective in ~80% of patients with ovarian cancer;
however, >60% of the patients relapse, and the 5-year survival
rate is <40% (1). Patients with
ovarian cancer often display large abdominal masses in the later
stages of the disease, which are mostly cystic or solid, and there
are currently no effective treatments available. Adoptive
immunotherapy is aimed at destroying tumor cells and it is based on
a theory that the host immune system may generate an immune
response against cancer cells. Natural killer (NK) cells in the
human immune system play an important role in anticancer treatment.
NK cells perform immunosurveillance mediated by the ‘missing-self’
mechanism, i.e., NK cell inhibitory receptor signaling is decreased
when the expression of the major histocompatibility complex-I
molecules on the target cell is downregulated or missing (2). In addition, the intracellular signaling
pathways in NK cells are activated. Mediated by perforin and
granzyme B, the target cell is lysed. Consequently, donor NK cells
are alloreactive towards recipient cells that lack their inhibitory
receptor ligands. It is advisable that testing for killer cell
inhibitory receptor (KIR) and its ligand, human leukocyte antigen
class I, be performed prior to NK cell cultivation.
The aim of the present study was to report the
results of six infusions of immune cell therapy in a 60-year-old
patient with a sizeable ovarian carcinoma.
Case report
Patient history
A 60-year-old woman was diagnosed with ovarian
carcinoma at the Guangdong General Hospital (Guangzhou, Guangdong)
in March, 2015. The patient had massive ascites and was unable to
eat or walk. The expected survival was ≤1 month. To improve the
quality of life, the patient received allogenic NK cell
immunotherapy.
Immunotherapy
Clinical-grade NK cells were cultured using
clinical-grade reagents and under good manufacturing practice
conditions. The human high activity NK cell in vitro
preparation kit was used (Hank Bioengineering Co. Ltd, Shenzhen,
China) that contained chimeric active cellular factors on K562 cell
membranes (3), plasma treatment
fluid, lymphocyte culture fluid additives, serum-free medium
additives and cell infusion additives. This kit is intended for
expanding and activating NK cells in peripheral blood mononuclear
cells in vitro to prepare NK cells of higher quantity,
purity and activity, namely highly activated NK (HANK) cells
(4). Blood samples from the patient
and donors were analyzed using the TIANamp Blood DNA kit (Tiangen
Biotech Co., Ltd., Beijing, China) and KIR/HLA-C allotypes
Genotyping Low Resolution kit (Tianjin Super Biotechnology
Developing Co., Ltd., Tianjin, China). Approximately 8–10 billion
HANK cells may be harvested after culture from 80 ml of peripheral
blood using NK cell serum-free medium and culture bags (Tianjin
Haoyang Biological Manufacture Co., Ltd, Tianjin, China). Cell
counting and quality control inspection are commonly performed on
day 12 of culture, and the quality indicators include ≥8 billion
total cells with ≥90% living cells, ≥85% CD3-/CD56+ cells (3), ≤1 EU/ml endotoxin, ≥80% cell killing
activity against K562 target cells (3), and bacteria-, fungi- and
mycoplasma-negative culture. After a 14-day culture, the HANK cells
were divided into three parts and infused intravenously on days
15–17.
Detection of tumor markers
The level of carbohydrate antigen 125 (CA125,
reference range <30 U/ml) expression was determined by
radioimmunoassay. The tests were performed according to the
protocols in the instruction manuals.
Discussion
In this study, we evaluated the efficacy and safety
of allogenic NK cell immunotherapy in a patient with ovarian
cancer. Polymerase chain reaction testing using sequence-specific
primer by the abovementioned KIR-HLA genotyping kit revealed that
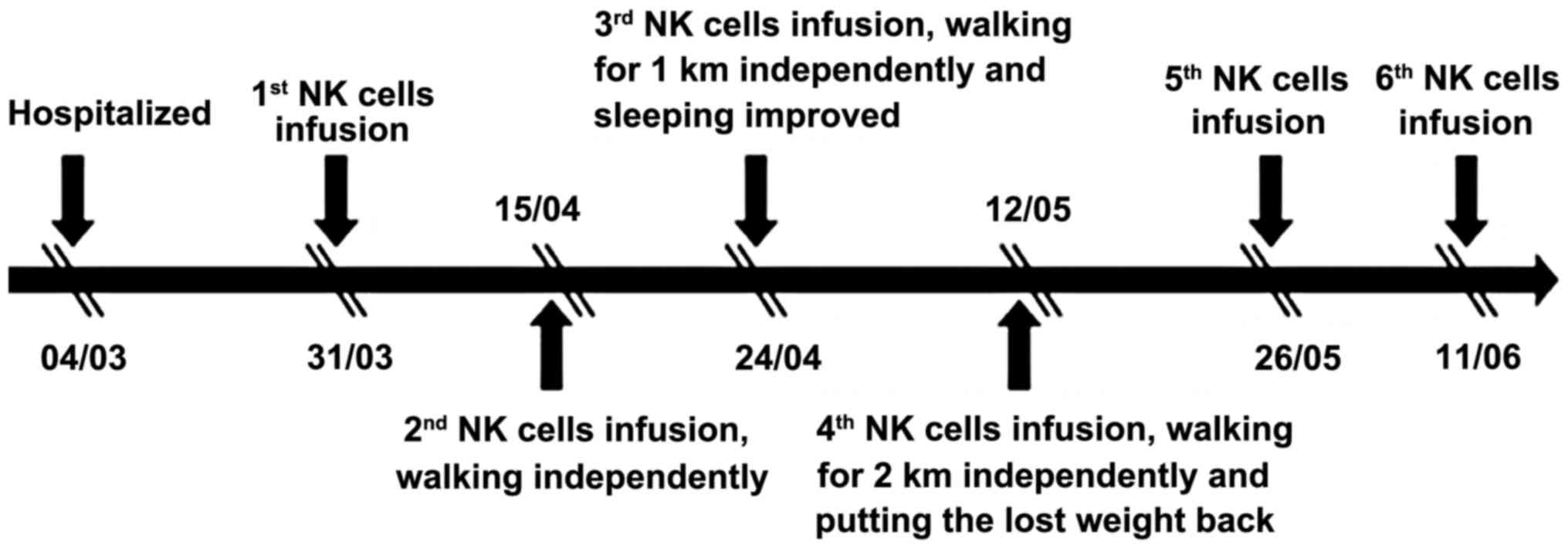
the patient's KIRs were mismatched with her own HLA. The patient
was treated with one infusion every 2 weeks over 3 months (between
March, 31 and June, 11) and achieved a definitive improvement
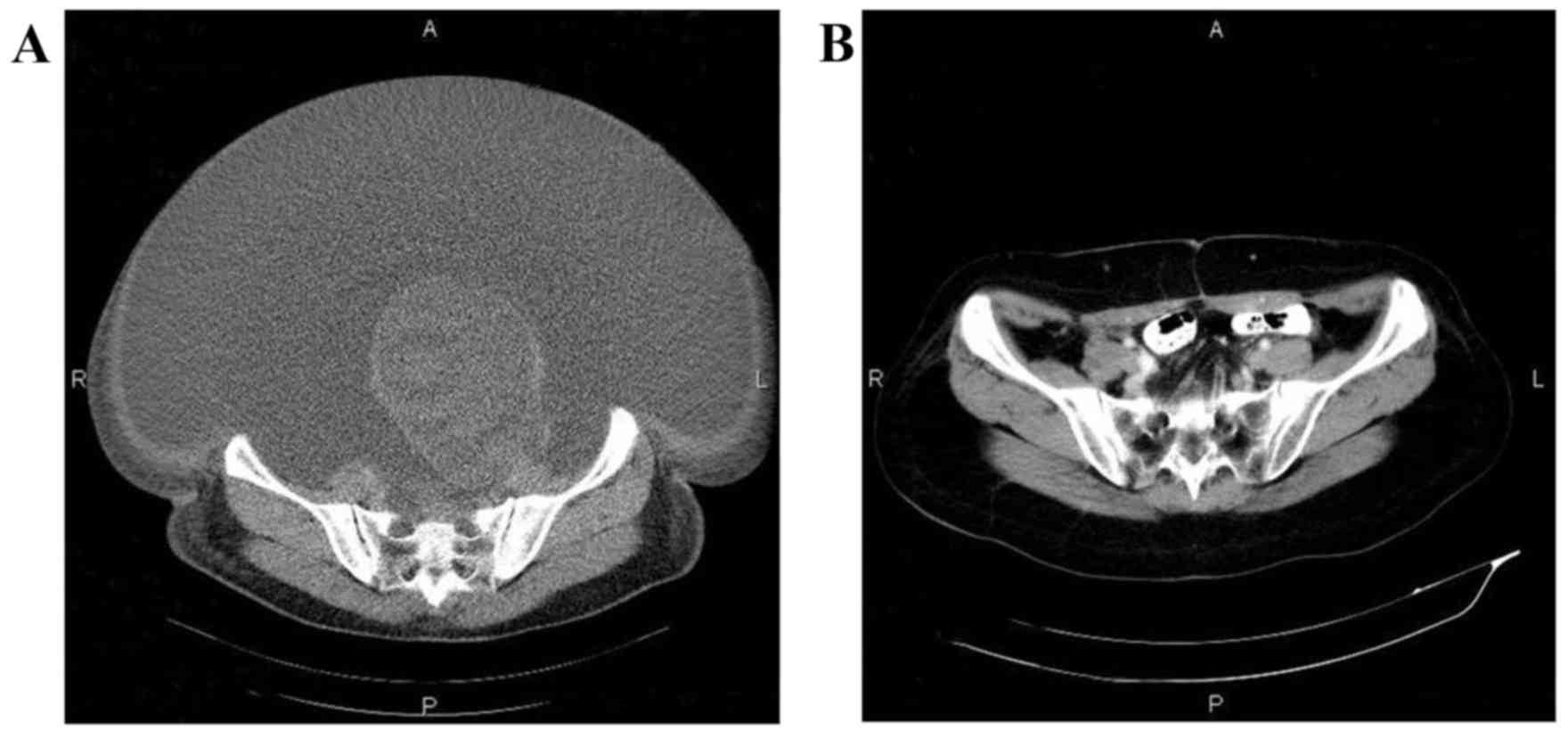
(Fig. 1). Computed tomography scans
indicated that the abdominal mases were markedly reduced following
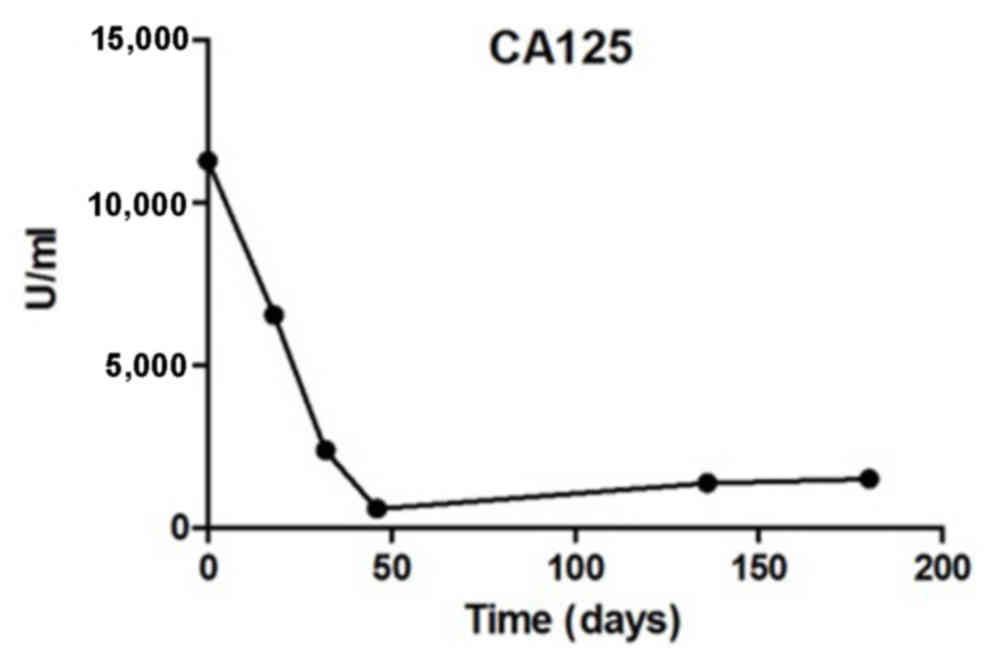
NK cell infusion (Fig. 2). The
expression levels of the ovarian cancer marker CA125 were measured
after each HANK cell infusion (Fig.
3) and were found to have decreased from 11,270 to 580 U/ml
after four infusions. The symptom of ascites was also alleviated
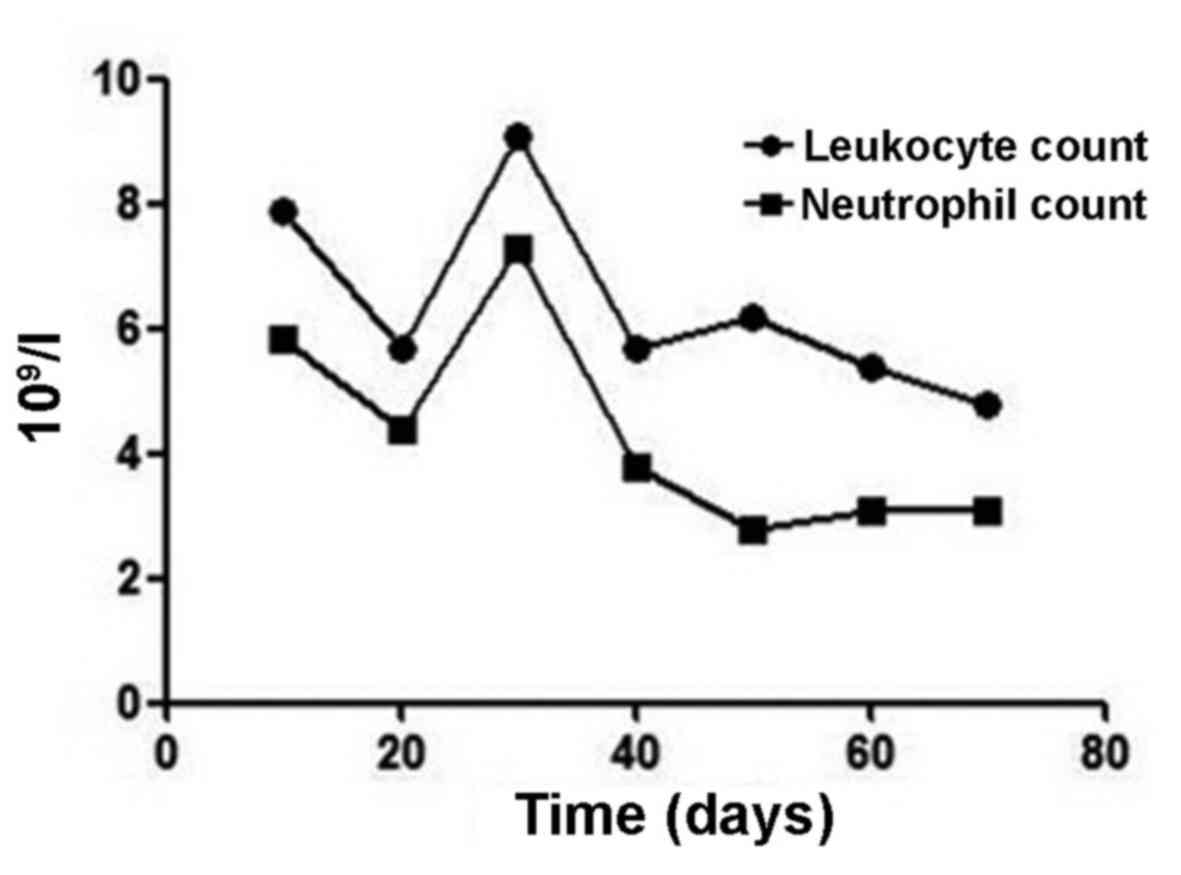
during the immunotherapy. The number of overall leukocytes and
neutrophils also improved with HANK cell infusion (Fig. 4).
In 1985, Rosenberg et al from the US National
Cancer Institute were the first to apply lymphokine-activated
killer cells to the treatment of melanoma (5). An increasing number of studies support
the hypothesis that immunotherapy is one of the best cancer
therapies in the clinical setting. NK lymphocytes are an important
part of the innate immune system, as they are able to destroy tumor
cells and target cells without antigens or sensitization. At the
same time, NK cells secrete numerous cytokines, such as interferon
(IFN)-γ and tumor necrosis factor (TNF)-α.
The pathogenesis of ovarian cancer has not been
fully elucidated. The majority of the patients are already at an
advanced stage of the disease when they receive treatment, and
advanced disease is the leading cause of death in patients with
gynecological tumors. Therefore, a more effective treatment is
urgently required. With the development of tumor immunology and
molecular biology, the use of tumor immunotherapy has increased
significantly in clinical practice. Allogenic NK cell immunotherapy
involves the intravenous infusion of immune cells that have been
expanded and activated ex vivo, treating tumors by directly killing
the tumor cells or stimulating the patient's immune response.
Immunosuppression is observed in patients with
ovarian cancer. The prognosis is closely associated with the
patient's immune status, and ovarian cancer may significantly
reduce the number of B cells, CD4+ T cells and
follicular dendritic cells (6). A
study including 176 patients with advanced ovarian cancer found
T-lymphocyte invasion of the tumor in 50% of the patients, and the
number of T cells in the tumor was strongly associated with
prolonged disease remission and improved overall survival rate
(7). In a study of 117 epithelial
ovarian cancer cases, T-lymphocyte immunohistochemical analysis
revealed high numbers of intraepithelial CD8+ T cells in patients
with long-term survival (8). Liu
et al reported the curative effect of cytokine-induced
killer cell treatment after surgery and chemotherapy for epithelial
ovarian cancer. Compared with the control group, patients treated
with immunotherapy exhibited a longer progression-free survival
(9). These results encourage more
attempts focused on immune anticancer therapy.
NK cells are large granular lymphocytes of the
innate immune system responsible for elimination of infected cells.
Based on the balanced recognition of membrane molecules by
activating and inhibitory receptors expressed on the NK cell, NK
cell-mediated cytotoxicity is directed towards target cells
(10). The mechanism underlying
destruction is multimodal and includes: Release of granzymes and
perforin; apoptosis of target cells by the expression of the Fas
ligand and TNF-related apoptosis-inducing ligand mediated by NK
cells (11); promoting immune
response by secreting cytokines such as IFN-γ, TNF-α and
granulocyte-macrophage colony-stimulating factor (12). The level of NK cell response depends
on the balance between signals from activating and inhibitory
receptors (13).
Antibody-dependent cell-mediated cytotoxicity is an
important antitumor mechanism of the immune system. Mediated by
tumor-specific monoclonal antibodies (mAbs), the Fc regions of the
mAbs bind to the antigens on the tumor cell surface, creating
multiple interactions of Fc-Fc receptors. Through the
immunoreceptor tyrosine-based activation motif, cytotoxicity and
the destruction of the tumor cell are triggered by downstream
signaling (14,15). It was demonstrated that overall and
disease-free survival may be prolonged by the combination of the
tumor-targeted mAb rituximab and NK cells for the treatment of
non-Hodgkin lymphoma (16).
Over the past decade, adoptive transfer of allogenic
NK cells has shown promise as an immunotherapy method. Taking
advantage of alloreactivity by the ‘missing-self’ concept, a number
of studies have demonstrated that infusion of haploidentical NK
cells to exploit KIR/HLA alloactivity is safe and may achieve a
better clinical effect in acute myelocytic leukemia (AML) patients
(17–19). Among 19 AML patients, 5 achieved
complete remission via subcutaneous interleukin-2 following
haploidentical NK cell infusion. Without eliciting
graft-versus-host disease, infusion of KIR-HLA mismatched donor NK
cells may have enhanced the antitumor effect in the 5 AML patients
(17). NK cell-based immunotherapies
are also a promising treatment for solid tumors. In a phase II
trial, patients with non-small-cell lung cancer received infusions
of allogenic, in vitro activated NK cells, combined with
chemotherapy, and the treatment was found to be safe and clinically
effective (20). In addition, a
phase II study of allogenic HANK cell therapy administered to 20
patients (14 with ovarian cancer and 6 with breast cancer)
demonstrated that adoptive transfer of haploidentical NK cells
following chemotherapy with lymphocyte depletion was clinically
effective (21).
To the best of our knowledge, the treatment of
ovarian cancer in the present report marks the first application of
HANK cells to allogenic immunotherapy at the Fuda Cancer Hospital.
Compared with traditional T-cell therapy, HANK cells exhibit the
following characteristics (4): i)
High activity. It is worth mentioning that the expression level of
the activating receptor, which increased from the almost
undetectable 0.31% to 65% after expansion, was enhanced by
≥200-fold. ii) High quantity. The total number of CD56+ cells was
increased ~100-fold. Ten billion NK cells rapidly proliferated in 2
weeks. iii) High purity. The purity of NK cells may reach 80%, or
even ≥96%.
Our patient received six intravenous infusions of
allogenic HANK cells between March, 2015 and June, 2015, but
discontinued treatment due to financial difficulties in October,
2015; she succumbed to the disease in March, 2016 following
relapse.
In conclusion, in the context of immune therapy,
HANK cells may be beneficial for cancer patients by enhancing their
cytotoxic lymphocytes. Allogenic HANK cell therapy was found to
achieve long-term partial response and to remarkably improve the
quality of life, and may be recommended for patients who have no
other treatment options. Although allogenic HANK cell therapy shows
promise as a cancer treatment, more studies are warranted to obtain
more clinical data.
Acknowledgements
The present study was supported by the International
Scientific Fund of Fuda Cancer Hospital, Guangzhou
(Y2016-ZD-001).
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
zum B, üschenfelde CM, Hermann C, Schmidt
B, Peschel C and Bernhard H: Antihuman epidermal growth factor
receptor 2 (HER2) monoclonal antibody trastuzumab enhances
cytolytic activity of class I-restricted HER2-specific T
lymphocytes against HER2-overexpressing tumor cells. Cancer Res.
62:2244–2247. 2002.PubMed/NCBI
|
|
3
|
Imai C, Iwamoto S and Campana D: Genetic
modification of primary natural killer cells overcomes inhibitory
signals and induces specific killing of leukemic cells. Blood.
106:376–383. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang M, Daniel S, Huang Y, Chancey C,
Huang Q, Lei YF, Grinev A, Mostowski H, Rios M and Dayton A:
Anti-West Nile virus activity of in vitro expanded human primary
natural killer cells. BMC Immunol. 11:32010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rosenberg SA, Lotze MT, Muul LM, Leitman
S, Chang AE, Ettinghausen SE, Matory YL, Skibber JM, Shiloni E,
Vetto JT, et al: Observations on the systemic administration of
autologous lymphokine-activated killer cells and recombinant
interleukin-2 to patients with metastatic cancer. N Engl J Med.
313:1485–1492. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hoechst B, Ormandy LA, Ballmaier M, Lehner
F, Krüger C, Manns MP, Greten TF and Korangy F: A new population of
myeloid-derived suppressor cells in hepatocellular carcinoma
patients induces CD4(+)CD25(+)Foxp3(+) T cells. Gastroenterology.
135:234–243. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang L, Conejo-Garcia JR, Katsaros D,
Gimotty PA, Massobrio M, Regnani G, Makrigiannakis A, Gray H,
Schlienger K, Liebman MN, et al: Intratumoral T cells, recurrence,
and survival in epithelial ovarian cancer. N Engl J Med.
348:203–213. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sato E, Olson SH, Ahn J, Bundy B,
Nishikawa H, Qian F, Jungbluth AA, Frosina D, Gnjatic S, Ambrosone
C, et al: Intraepithelial CD8+ tumor-infiltrating
lymphocytes and a high CD8+/regulatory T cell ratio are
associated with favorable prognosis in ovarian cancer. Proc Natl
Acad Sci USA. 102:pp. 18538–18543. 2005; View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liu J, Li H, Cao S, Zhang X, Yu J, Qi J,
An X, Yu W, Ren X and Hao X: Maintenance therapy with autologous
cytokine-induced killer cells in patients with advanced epithelial
ovarian cancer after first-line treatment. J Immunother.
37:115–122. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Orange JS: Formation and function of the
lytic NK-cell immunological synapse. Nat Rev Immunol. 8:713–725.
2008. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zompi S and Colucci F: Anatomy of a
murder-signal transduction pathways leading to activation of
natural killer cells. Immunol Lett. 97:31–39. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Biron CA, Nguyen KB, Pien GC, Cousens LP
and Salazar-Mather TP: Natural killer cells in antiviral defense:
Function and regulation by innate cytokines. Annu Rev Immunol.
17:189–220. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Moretta L, Bottino C, Pende D, Vitale M,
Mingari MC and Moretta A: Human natural killer cells: Molecular
mechanisms controlling NK cell activation and tumor cell lysis.
Immunol Lett. 100:7–13. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ravetch JV and Bolland S: IgG Fc
receptors. Annu Rev Immunol. 19:275–290. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Farag SS, VanDeusen JB, Fehniger TA and
Caligiuri MA: Biology and clinical impact of human natural killer
cells. Int J Hematol. 78:7–17. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Alderson KL and Sondel PM: Clinical cancer
therapy by NK cells via antibody-dependent cell-mediated
cytotoxicity. J Biomed Biotechnol. 2011:3791232011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Miller JS, Soignier Y,
Panoskaltsis-Mortari A, McNearney SA, Yun GH, Fautsch SK, McKenna
D, Le C, Defor TE, Burns LJ, et al: Successful adoptive transfer
and in vivo expansion of human haploidentical NK cells in patients
with cancer. Blood. 105:3051–3057. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rubnitz JE, Inaba H, Ribeiro RC, Pounds S,
Rooney B, Bell T, Pui CH and Leung W: NKAML: A pilot study to
determine the safety and feasibility of haploidentical natural
killer cell transplantation in childhood acute myeloid leukemia. J
Clin Oncol. 28:955–959. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Curti A, Ruggeri L, D'Addio A, Bontadini
A, Dan E, Motta MR, Trabanelli S, Giudice V, Urbani E, Martinelli
G, et al: Successful transfer of alloreactive haploidentical KIR
ligand-mismatched natural killer cells after infusion in elderly
high risk acute myeloid leukemia patients. Blood. 118:3273–3279.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Iliopoulou EG, Kountourakis P, Karamouzis
MV, Doufexis D, Ardavanis A, Baxevanis CN, Rigatos G, Papamichail M
and Perez SA: A phase I trial of adoptive transfer of allogeneic
natural killer cells in patients with advanced non-small cell lung
cancer. Cancer Immunol Immunother. 59:1781–1789. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Geller MA, Cooley S, Judson PL, Ghebre R,
Carson LF, Argenta PA, Jonson AL, Panoskaltsis-Mortari A,
Curtsinger J, McKenna D, et al: A phase II study of allogeneic
natural killer cell therapy to treat patients with recurrent
ovarian and breast cancer. Cytotherapy. 13:98–107. 2011. View Article : Google Scholar : PubMed/NCBI
|