Introduction
Thyroid carcinoma is the most common endocrine
malignancy. The majority of cases are of papillary thyroid
carcinoma (PTC), which often has a good prognosis (1). Distant metastases derived from PTC
occur in ~4% of the patients (2).
The most common sites are the lungs and bones; however, renal
metastasis is rare, with fewer than 30 cases reported in the
literature (3), and it is easily
misdiagnosed. The present study reports a case of PTC with initial
presentation of renal metastasis, which was initially
misdiagnosed.
Case report
A 53-year-old man was admitted to the Department of
Urology Surgery in Sun Yat-sen University Cancer Center during July
2011 with a complaint of discomfort on the left side of the waist.
An occupying lesion in the left kidney was identified by performing
computed tomography (CT). The patient had no medical history of
renal disease, thyroid disease, neck irradiation, dysphagia or
dyspnea. A physical examination at the time of presentation
revealed no clear symptoms.
The CT analysis demonstrated a roughly spherical
mass ~5 cm in diameter in the left kidney, and an uneven
enhancement in the enhanced scanning images, which was originally
considered to be primary renal cell carcinoma, as well as irregular
nodular shadows in the left adrenal area and multiple pulmonary
nodules. The clinical diagnosis was of primary renal cell carcinoma
accompanied by adrenal and bilateral pulmonary metastases;
subsequently, the patient was admitted for surgery and underwent a
nephrectomy for a renal mass on July 8, 2011.
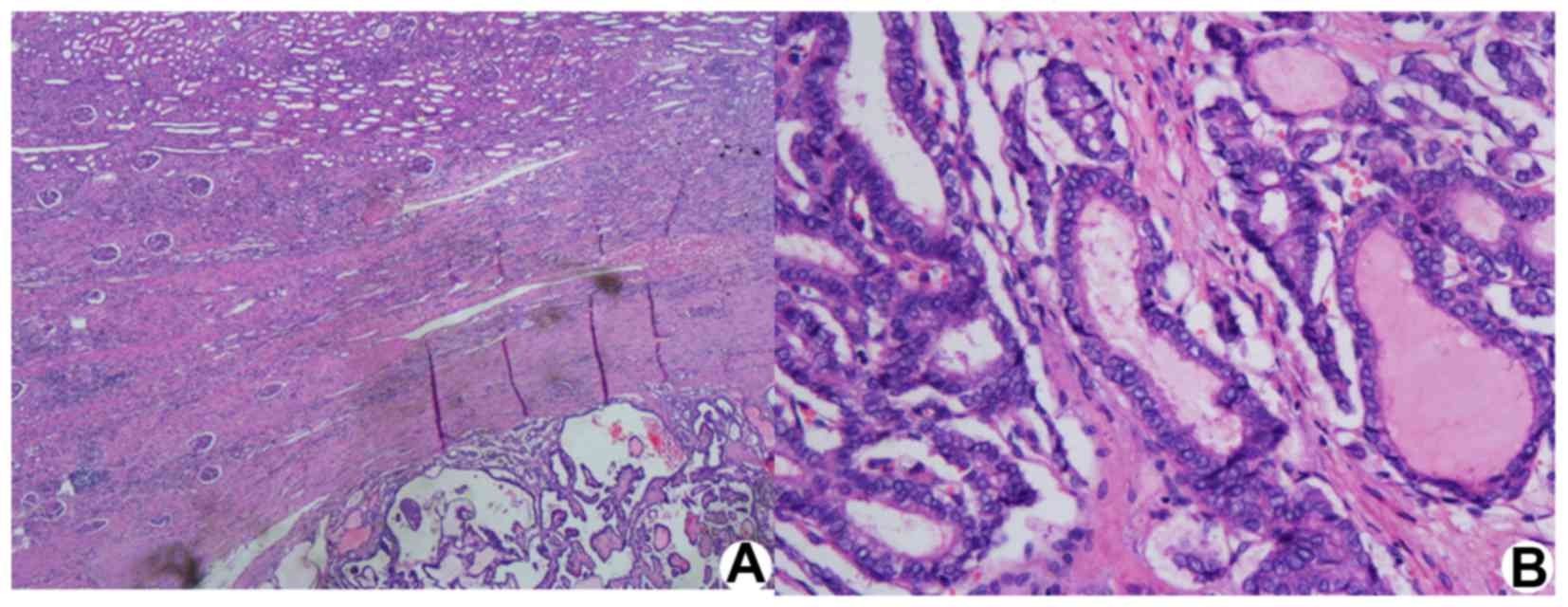
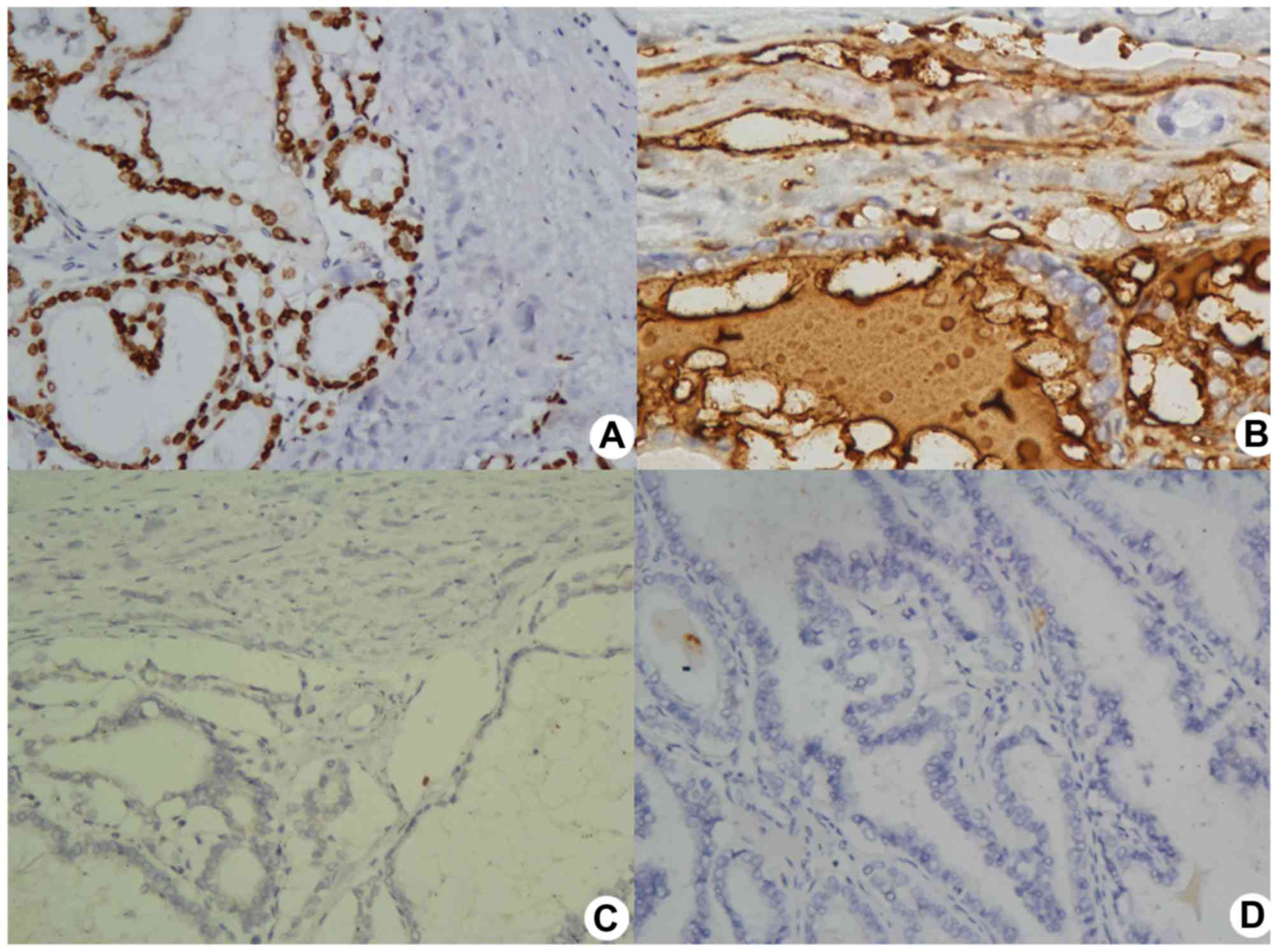
Histologically, a pathological examination of the
left kidney tumor revealed a metastatic follicular variant of PTC.
The diagnosis was confirmed by positive immunoperoxidase staining
for thyroglobulin, cytokeratin 19, thyroid transcription factor-1
and vimentin, whereas negative staining of CD10 and thrombopoietin
within the tumor cells (Figs. 1 and
2), and the left adrenal schwannoma,
were also noted.
A further examination of the thyroid was performed
on August 3, 2011. Ultrasonography and CT revealed multiple lesions
in both sides of the thyroid accompanied by multiple lesions of the
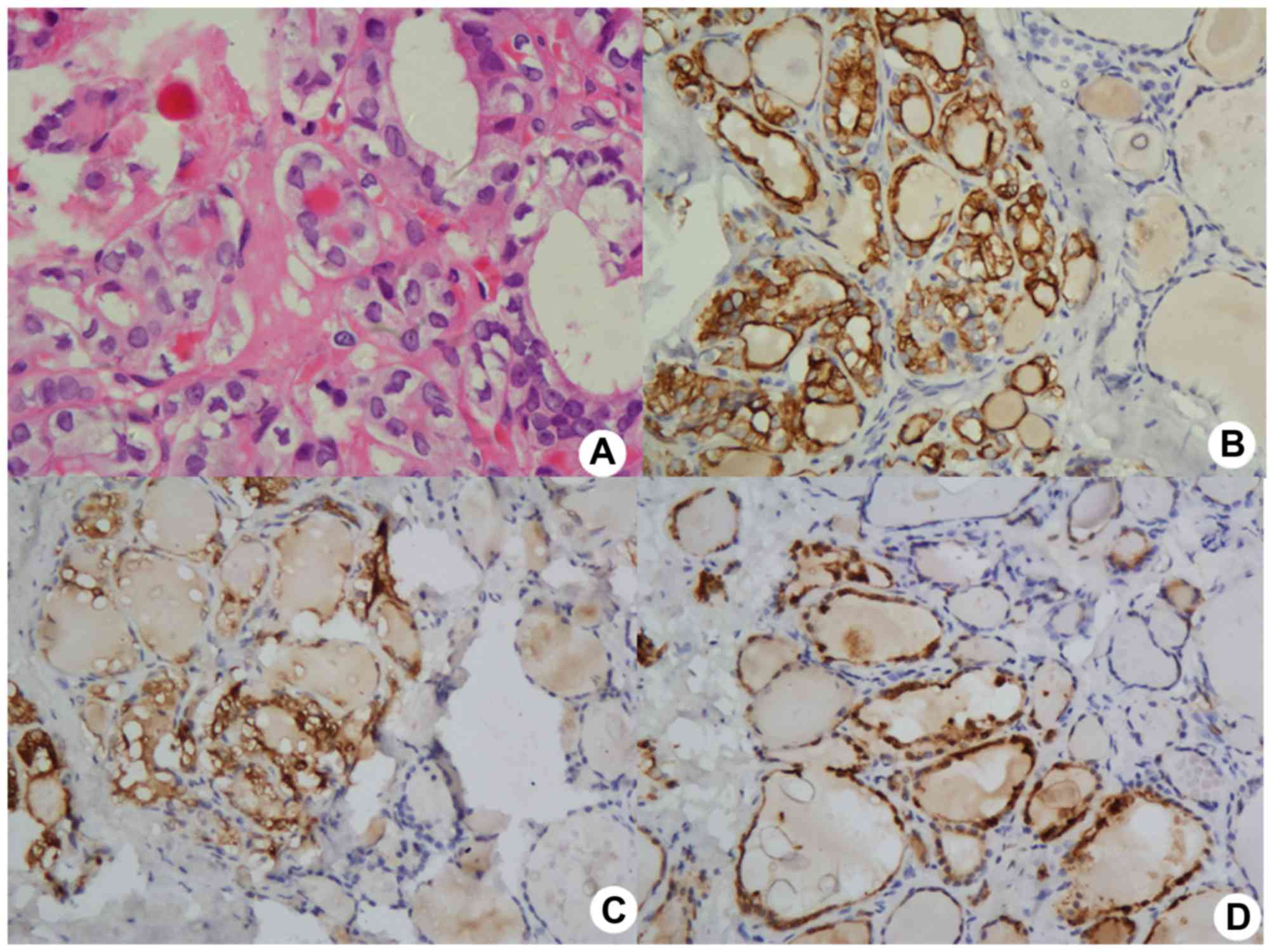
bilateral neck lymph nodes. Total thyroidectomy and bilateral
radical neck dissection were performed, and the postoperative
pathological results confirmed the follicular variant of PTC in the
both sides of the thyroid, with widespread bilateral neck lymph
node metastasis, as revealed by the strong positive
immunoperoxidase staining of cytokeratin-19, galectin-3 and
melanocytes (Fig. 3). The patient
underwent radiometabolic treatment with 100 mCi Iodine-131 twice in
October 2011 and April 2012, respectively; however, the patient
subsequently failed to present at our hospital regularly. On August
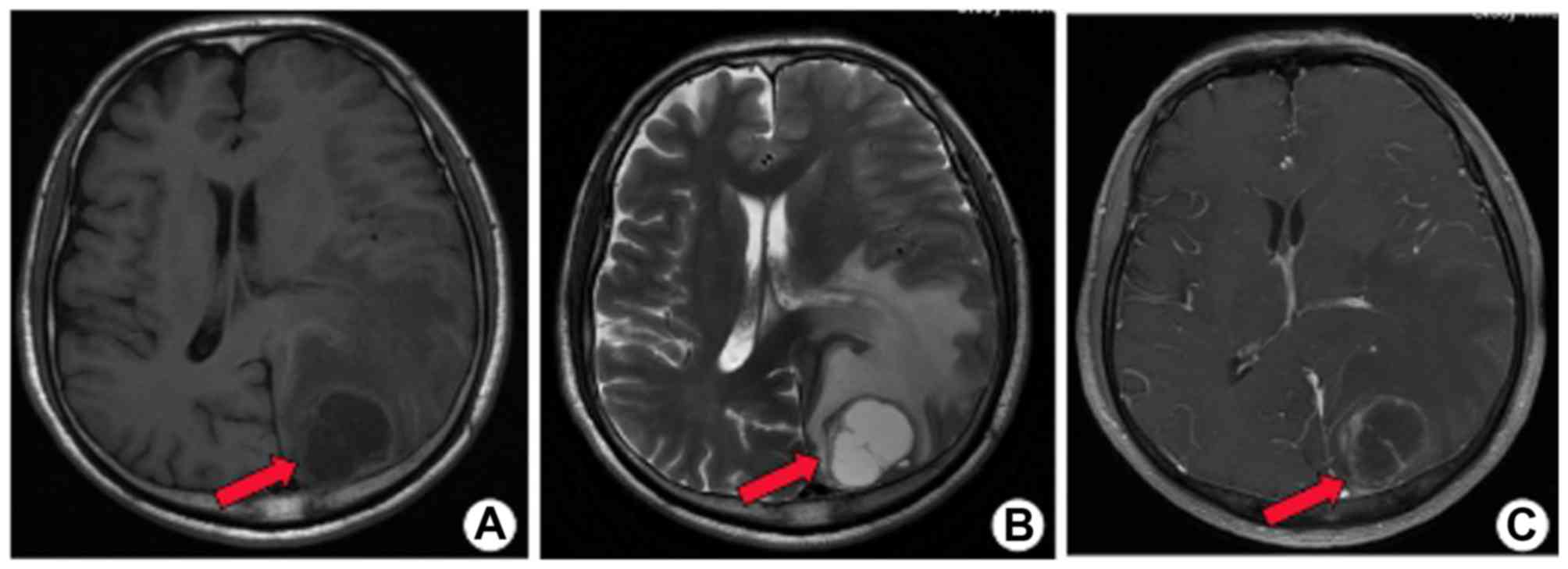
21, 2015, the patient attended the hospital to be treated for
dyspnea and right-sided hemiparesis. Imaging studies, including CT
and magnetic resonance imaging, revealed the presence of multiple
nodule metastases in the bilateral pulmonary, bilateral hilar and
mediastinal regions, and, of greatest concern, left temporal lobe
metastasis (Fig. 4).
Discussion
Thyroid cancer is one of the fastest growing
malignant tumors in the world, and PTC is the most common
pathological type of tumor, accounting for ~70% of cases of thyroid
carcinoma, the most common types of which are typical, follicular
type and columnar type PTC (4). PTC
originates from thyroid follicular epithelial cells, and metastasis
occurs most easily to cervical lymph nodes in the neck, which
accounts for ~30–90% of all cases (5). A few cases of PTC that occur are of
distant metastasis (ranging from 3.5–3.8%) (6), and the most common site is the lungs,
followed by the bones; however, renal metastasis occurs only
rarely, and it is easily misdiagnosed (7). Distant metastases are often associated
with a poor prognosis, and the 10-year survival rate is <50%
(8). Cervical neoplasms (primary
tumors or metastasis lymph nodes) are presented frequently as a
chief complaint of patients with PTC.
It is rare for patients with PTC to show kidney
metastatic lesions at their initial presentation, and the total
number of cases reported in the literature is fewer than 30. The
majority of these cases were of female patients (~80%), and the
cases were concerned with unilateral metastasis. Furthermore, the
majority of the cases were of thyroid follicular carcinoma, which
accounted for >50% of the total, whereas PTC accounted for not
more than 13% (3,9,10).
Kidney metastases of thyroid carcinoma often occur several years
after resection of the thyroid lesions (11,12);
initial symptoms with kidney metastasis are rare, and so these
cases may easily be misdiagnosed as renal cell carcinoma. The
present case was a male patient, whose main complaint was of kidney
syndrome, which was misdiagnosed as renal cell cancer, and it was
subsequently disclosed to have originated from thyroid carcinoma.
The details of the present case differed from those previously
reported in the literature (13).
Surgery is the first-choice option for PTC, although invasive PTC
with distant metastases may result in a limitation of the range of
treatment options available, with the notable exception of lung
metastases, which are sensitive to Iodine-131 treatment. The
pathological diagnosis of the present case was confirmed as renal
metastases of the follicular variant of PTC following surgery.
Further therapy confirmed the diagnosis as the follicular variant
of PTC, accompanied by widespread bilateral cervical lymph node
metastasis. A preoperative diagnosis of the follicular variant of
PTC is often quite difficult to make, and is often controversial
(14).
The prognosis of the follicular variant of PTC is
less favorable compared with that of typical PTC, particularly for
invasive lesions of the infiltrating type, or with multiple nodules
(15). In the present case, the
initial diagnosis in July 2011 was of PTC with bilateral neck,
bilateral lung and left kidney metastases. Following surgical and
radiation therapy, at present, the patient appears to have adrenal
gland and brain metastases, which indicate that the condition
belongs to the invasive subtype of PTC, and therefore the clinical
prognosis for the patient is poor.
In conclusion, renal metastases from PTC with
initial renal syndrome occur rarely, and this makes the condition
difficult to diagnose and manage. This has been reported in the
present case study, and our hope is that this will be helpful for
the diagnosis and treatment of renal metastasis from PTC in the
future.
References
|
1
|
Mazzaferri EL and Kloos RT: Clinical
review 128: Current approaches to primary therapy for papillary and
follicular thyroid cancer. J Clin Endocrinol Metab. 86:1447–1463.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shaha AR, Shah JP and Loree TR:
Differentiated thyroid cancer presen-ting initially with distant
metastasis. Am J Surg. 174:474–476. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Varinot J, Ménégaux F, Bitker MO and
Compérat E: Renal metastasis from thyroid carcinoma: A case report.
Anal Quant Cytopathol Histpathol. 36:46–50. 2014.PubMed/NCBI
|
|
4
|
Lloyd RV, Buehler D and Khanafshar E:
Papillary thyroid carcinoma variants. Head Neck Pathol. 5:51–56.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Isaacs JD, McMullen TP, Sidhu SB, Sywak
MS, Robinson BG and Delbridge LW: Predictive value of the Delphian
and level VI nodes in papillary thyroid cancer. Anz J Surg.
80:834–838. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Benbassat CA, Mechlis-Frish S and Hirsch
D: Clinicopathological characteristics and long-term outcome in
patients with distant metastases from differentiated thyroid
cancer. World J Surg. 30:1088–1095. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mazzaferri EL and Massoll N: Management of
papillary and follicular (differentiated) thyroid cancer: New
para-digms using recombinant human thyrotropin. Endocr Relat
Cancer. 9:227–247. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Elisei R, Molinaro E, Agate L, Bottici V,
Masserini L, Ceccarelli C, Lippi F, Grasso L, Basolo F, Bevilacqua
G, et al: Are the clinical and pathological features of
differentiated thyroid carcinoma really changed over the last 35
years? Study on 4187 patients from a single Italian institution to
answer this question. J Clin Endocrinol Metab. 95:1516–1527. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ruggiero FP, Frauenhoffer EE and Stack BC
Jr: Papillary thyroid cancer with an initial presentation of
abdominal and flank pain. Am J Otolaryngol. 26:142–145. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Song HJ, Xue YL, Xu YH, Qiu ZL and Luo QY:
Rare metastases of differentiated thyroid carcinoma: Pictorial
review. Endocr Relat Cancer. 18:R165–R174. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Malhotra G, Upadhye TS, Sridhar E, Asopa
RV, Garde PS, Gawde S and Rangarajan V: Unusual case of adrenal and
renal metastases from papillary carcinoma of thyroid. Clin Nucl
Med. 35:731–736. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Farina E, Monari F, Tallini G, Repaci A,
Mazzarotto R, Giunchi F, Panzacchi R, Cammelli S, Padula GD,
Deodato F, et al: Unusual thyroid carcinoma metastases: A case
series and literature review. Endocri Pathol. 27:55–64. 2016.
View Article : Google Scholar
|
|
13
|
Wallander M, Layfield LJ, Jarboe E,
Emerson L, Liu T, Thaker H, Holden J and Tripp S: Follicular
variant of papillary carcinoma: Reproducibility of histologic
diagnosis and utility of HBME-1 immunohistochemistry and BRAF
mutational analysis as diagnostic adjuncts. Appl Immunohistochem
Mol Morphol. 18:231–235. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lloyd RV, Erickson LA, Casey MB, Lam KY,
Lohse CM, Asa SL, Chan JK, DeLellis RA, Harach HR, Kakudo K, et al:
Observer variation in the diagnosis of follicular variant of
papillary thyroid carcinoma. Am J Surg Pathol. 28:1336–1340. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
DeLellis RA, Lloyd RV, Heitz PU and Eng C:
Pathology and genetics of tumours of endocrine organsKleihues P and
Sobrin LH: World health organization. Classification of Tumours
Lyon: IARC Press; 2004
|